
Abstract
Background.
Adherence to statins for the primary prevention of cardiovascular disease (CVD) is low but may be improved through shared decision making (SDM). CVD risk estimation is fundamental to SDM at statin initiation, and the absence of a CVD risk score may indicate that SDM has not taken place. This study explores statin initiation decisions by investigating whether CVD risk is associated with adherence to statins and CVD outcomes.
Design.
A cohort of statin-naïve patients aged 40 to 84 y initiated on statins for primary prevention between 2017 and 2020 was identified and categorized by the presence or absence of a CVD risk score at statin initiation. Multivariable modeling determined the association between CVD risk score and statin adherence and persistence. A secondary analysis investigated the relationship with CVD outcomes and death.
Results.
A total of 255,730 patients were included with a mean follow-up of 4.6 y. The presence of a CVD risk score (67.7% of patients) was associated with a 7% increase in adherence and an 8% reduction in discontinuations as well as a 15% reduction in CVD and all-cause mortality.
Conclusion.
The presence of a CVD risk score is associated with improvements in both adherence and persistence, which could indicate that the quality of initiation consultations, and a focus on SDM, improves the utility of statins. In addition, CVD risk scoring is associated with a large decrease in CVD/death, which cannot fully be explained by improvements in statin adherence and persistence, an important finding necessitating further investigation.
Implications.
Efforts to improve the integration of CVD risk scores and SDM in statin initiation consultations may significantly improve statin utilization and CVD outcomes.
Highlights
We present a comprehensive assessment of the adherence to and persistence with statins for the primary prevention of CVD, which, for the first time, is linked to the presence or absence of CVD risk scoring.
CVD risk scoring is associated with improvements in both adherence and persistence as well as significant reductions in CVD and all-cause mortality.
There should be renewed focus on the content of statin initiation consultations ensuring that CVD risk is communicated using a shared decision-making approach.
Further consideration should be given to the important discrepancy in CVD and death seen when CVD risk scoring is, and is not, used in practice.
This is a visual representation of the abstract.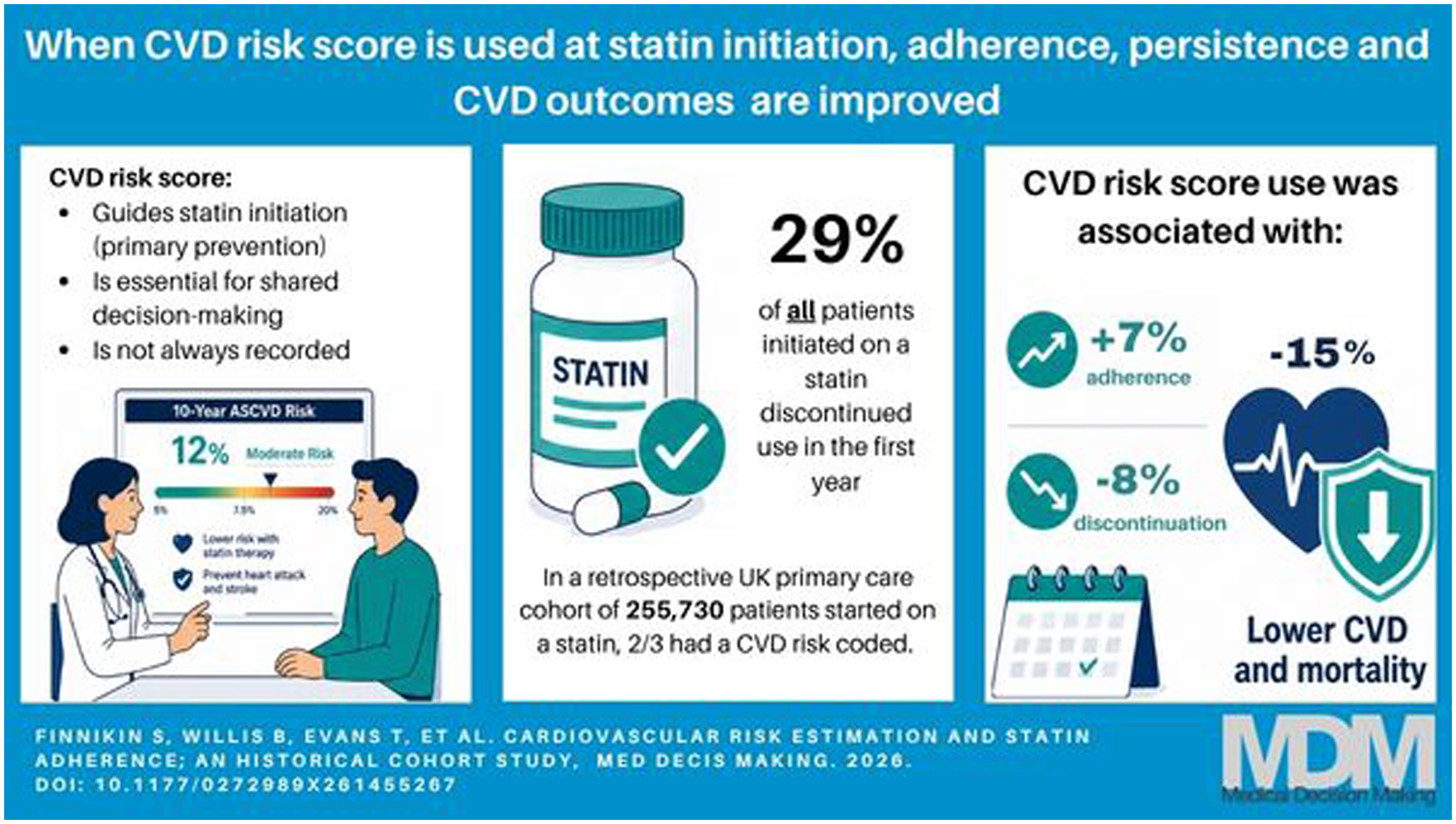
Keywords
The optimal use of lipid-lowering therapies (LLTs) is one of the cornerstones of cardiovascular disease (CVD) prevention strategies worldwide, and as a result, statins (the most used class of LLT) are one of the most commonly prescribed medications. 1 However, adherence to statins is known to be low, with roughly half of people being nonadherent after a year.2–4 Poor adherence to statins used for primary prevention is associated with an increased risk of cardiovascular events. 5 It has been proposed that shared decision making (SDM) at statin initiation could improve adherence, although evidence from interventions designed to improve SDM is mixed.6–9
Statins for the primary prevention of CVD are usually recommended to patients based on an estimate of their overall risk of CVD.10–12 This strategy is adopted because the benefit a patient may gain from a statin is proportional to their CVD risk, whereas the disadvantages and costs of the medication are, essentially, unrelated to the underlying CVD risk. Therefore, at low CVD risk, prescribing statins may not be cost-effective and/or the net benefit may not be sufficient at an individual level based on the patient’s preferences and values. 13 Thus, CVD risk estimation is a necessary component of the offer and acceptance of a statin and should be discussed with patients using an SDM approach. SDM is the accepted and preferred approach to medical decision making, consisting of a thorough discussion of the options available to a patient (including doing nothing), along with their risks and benefits, before agreeing on the option that is right for the individual. 14 It follows that CVD risk estimation is a necessary component of statin initiation decisions, as a fully informed discussion about the benefits and risks of statins is not possible without this information.
In the United Kingdom, QRISK is used for CVD risk estimation. 15 Several iterations of this algorithm have been used, with QRISK3 being the most current one used in practice. Previous studies using UK primary care data have shown that many patients are initiated on statins without a QRISK score recorded in the patient’s record. 16 Moreover, when QRISK is not recorded, the principal predictor of the decision to initiate statins is the total cholesterol level, whereas, when it is recorded, the CVD risk estimate is the principal predictor. 17 The presence or absence of a record of a QRISK score is therefore an indicator of different decision-making processes. If a QRISK score is not coded in the patients record when statins are initiated, the evidence suggests CVD risk estimates are not discussed at the time of statin initiation, and SDM is less likely to have taken place. Conversely, a QRISK score coded at the time of statin initiation indicates that the necessary information required for SDM was available to the clinician during the consultation. Thus, it is reasonable to hypothesize that there is an association between the coding of a CVD risk estimate and SDM when statins are initiated for the primary prevention of CVD.
It has been argued that adherence to medications could be improved through better SDM at initiation,18–22 and there is evidence that some facets of the initiation consultation, or the clinician doing the initiation, are associated with adherence.23,24 Establishing a link between SDM and adherence is, however, not straightforward, largely because it is difficult to measure SDM in practice. 25 Several barriers to effective SDM exist in practice, including a lack of training and time, poor communications skills, and cultural perceptions. 26 Not having access to accurate information about risks and benefits would also make SDM difficult, and thus the absence of a coded QRISK score would be a further barrier in the specific SDM scenario. Having established that the presence or absence of a QRISK score is associated with a different initiation decision process and that CVD risk estimation is necessary for SDM, there is an opportunity to explore the link between SDM and adherence in a new way.
The objective of this study is to investigate whether the recording of a QRISK score at the point of statin initiation is associated with adherence to, and persistence with, statins and CVD outcomes to explore whether this component of medical decision making influences behaviors and outcomes.
Methods
This cohort study used CPRD Aurum (version 2023.12.001), and the study design and data extraction were facilitated using Dexter software.27,28 All statin-naïve patients aged 40 to 84 y (inclusive) initiated on statins for primary prevention between 2017 and 2020 were included. To include only patients in whom a QRISK calculation was appropriate, patients were excluded if they had existing CVD (or a CVD event within 60 d of statin initiation to account for any coding delay), type 1 diabetes mellitus, chronic kidney disease stages 3 to 5, or familial hypercholesterolemia (either coded or presumed due to total cholesterol being ≥9.0 mmol/L). The population was split into 2 cohorts: those with a coded QRISK score and those without. A QRISK score coded within the 60 d prior to statin initiation was regarded as being associated with the statin initiation. This time period was chosen because it was considered clinically plausible that a CVD risk estimation within 60 d is likely to have been calculated because of a risk factor update (e.g., new lipid profile result) and resulted in the statin initiation consultation. This QRISK would therefore be logically linked to the initiation decision.
The index date was the date of the first statin prescription. Patients were eligible for inclusion from the earliest of the following dates: study start date, registration date plus 1 y, and age 40 y, and until the earliest of the following dates: age 85 y, study end date, CVD diagnosis, or other excluding diagnosis. Patients were excluded if they left the database within 2 y of the index date as a minimum of 2-y follow-up was required. Patients were followed up until the earliest of the following dates: study end period, exit from the database, a new CVD diagnosis, or death.
Baseline characteristics and variables that may be associated with adherence 29 that were available in the dataset were identified along with coded QRISK scores (latest recorded in the period 60 d prior to initiation up until statin initiation) and statin type and dose. Relevant comorbidities were hypertension, atrial fibrillation, type 2 diabetes mellitus, inflammatory arthritis, and severe enduring mental illness. These were chosen as relevant confounders as they are common comorbidities in CVD and/or associated with cardiovascular outcomes. These were combined into a single ordinal variable. Both QRISK2 and QRISK3 scores were extracted and treated in the same way and therefore not referred to separately in this article. All subsequent statin and other LLT prescriptions (ezetimibe, bempedoic acid, and fibrates) following initiation were identified (type, quantity, and duration of prescription in days) along with the total number of consultations between index and exit dates. Lipid profiles and new CVD diagnoses were the other outcome variables. A composite outcome of CVD diagnosis and all-cause mortality was created as a secondary outcome. This composite was chosen to increase the power given the low anticipated event rate in this primary prevention population. It was not possible to categorize the cause of death from the available data, so CV deaths could not be isolated.
A post hoc QRISK score was calculated using the available variables for all participants.
Statistics
The primary outcome of adherence was measured using the medication possession ratio (MPR).30,31 The quantity of drug prescribed, rather than the “days” prescribed, was used for the prescription duration as it was felt that this would provide more accurate data. Statins (and other LLTs) are prescribed as a once-daily dosing regimen, but the number of “days” entered by the clinician can be inconsistent with this. To check this assumption, a sensitivity analysis was undertaken including only patients for whom the number of days is equal to the quantity of drug prescribed. Patients were excluded from adherence analysis if they were issued only 1 prescription of a statin (but they will be included in the persistence analysis). Patients were classified as being adherent if their MPR was greater than 0.8 in a 12-mo period, as this threshold is consistently used for research purposes. 32 Adherence (MPR) was calculated for each completed 12-mo period of follow-up to assess for trends.
For persistence, patients were identified as having discontinued statin therapy if there was no new prescription 180 d after the expected end of their supply. There is no consensus on the permissible gap 32 in persistence research, but 180 d is commensurate with other research 4 and considered clinically appropriate by the authors with experience of English prescribing practices. Persistence was defined as the time between initiation and the final prescription plus the duration of the last prescription. 32 A sensitivity analysis was performed including all oral LLTs prescribed following statin initiation. The post hoc QRISK calculation was compared with the coded QRISK score (where available) using the concordance correlation coefficient.
Patients who restarted their medication after a period of discontinuation >180 d were identified, but prescriptions after a period of discontinuation were not included in the adherence and persistence analysis based on the assumption that further discussion about the medication may have influenced the decision to recommence, so the link with the initiation consultation is less robust.
Linear regression and multivariable logistic regression modeling were used to establish the effect of variables on adherence in the first 12 mo (as measured by the MPR) with the presence or absence of QRISK score being the main variable of interest and practice ID as a random effect (this is a change from protocol, as prescriber-level data were not available). Collinearity was assessed using the variance inflation factor. Mediator analysis was undertaken using Med4Way 33 to establish whether the association between QRISK coding and CVD outcomes and death was mediated by adherence and persistence.
Two time-to-event analyses using Cox regression for the outcomes of statin discontinuation and CVD outcomes and death were performed. In both cases, QRISK coding was the main predictor variable. Statistical significance for all models was adjusted for multiple testing using the Bonferroni technique. 34
Because prescribing data are electronic and recorded automatically, it was assumed that the absence of a prescription means that none was issued. If the QRISK score was missing, it was presumed to be absent. Previous research has shown that when QRISK2 is not recorded, it does not seem to influence prescribing decisions, which provides validity to this assumption. 17 Categories for missing data were used for categorical variables. All analysis was performed using StataSE V18.
The study protocol 35 (23_003321) was approved by CPRD, who hold ethical approval (21/EM/026) for use of data without individual patient consent. This study received no external funding. Amendments from the published protocol included the use of post hoc QRISK estimation and consulting rate in modeling and the examination of smoking cessation and blood pressure changes over the study period. These changes were approved by CPRD.
Results
The cohort comprised 255,730 patients from 1,771 practices (see the strobe diagram in Figure 1). The characteristics of the included patients are shown in Table 1, split by the presence or absence of a QRISK score (within 60 d of statin initiation). Two-thirds of patients had a QRISK score coded (173,051, 67.7%; 95% confidence interval [CI]: 67.5%–67.8%), and the groups were statistically different by all measures apart from the incidence of raised liver transaminases and the combined variable of CVD diagnoses or death (P value for significance adjusted to 0.0036 by Bonferroni correction). Notably, those patients with a QRISK score, when compared to those without, were more likely to be male (54.3% v. 49.2%), older (mean age 63.3% v. 59.6%), from areas of lower deprivation (16.7% in the first index of multiple deprivation quintile [least deprived] compared with 10.3% in the fifth [most deprived] quintile), and have White ethnicity (85.1% v. 79.1%). When the QRISK score was recorded, it was coded on the day of statin initiation in 52.4% of cases (n = 90,648) with the next most common intervals between QRISK coding and initiation being 1 d (3.6%) and 7 d (3.2%). Those with a QRISK score coded had a higher mean post hoc calculated QRISK (14.0% v. 10.9%, P < 0.001) and a higher proportion of 10-y estimates ≥10% (68.8% compared with 31.2% in the uncoded group). However, these findings should be interpreted with caution as the post hoc QRISK calculation correlated poorly with the coded QRISK (correlation coefficient 0.624, 95% CI 0.622–0.627) due to the missing variables in the dataset.
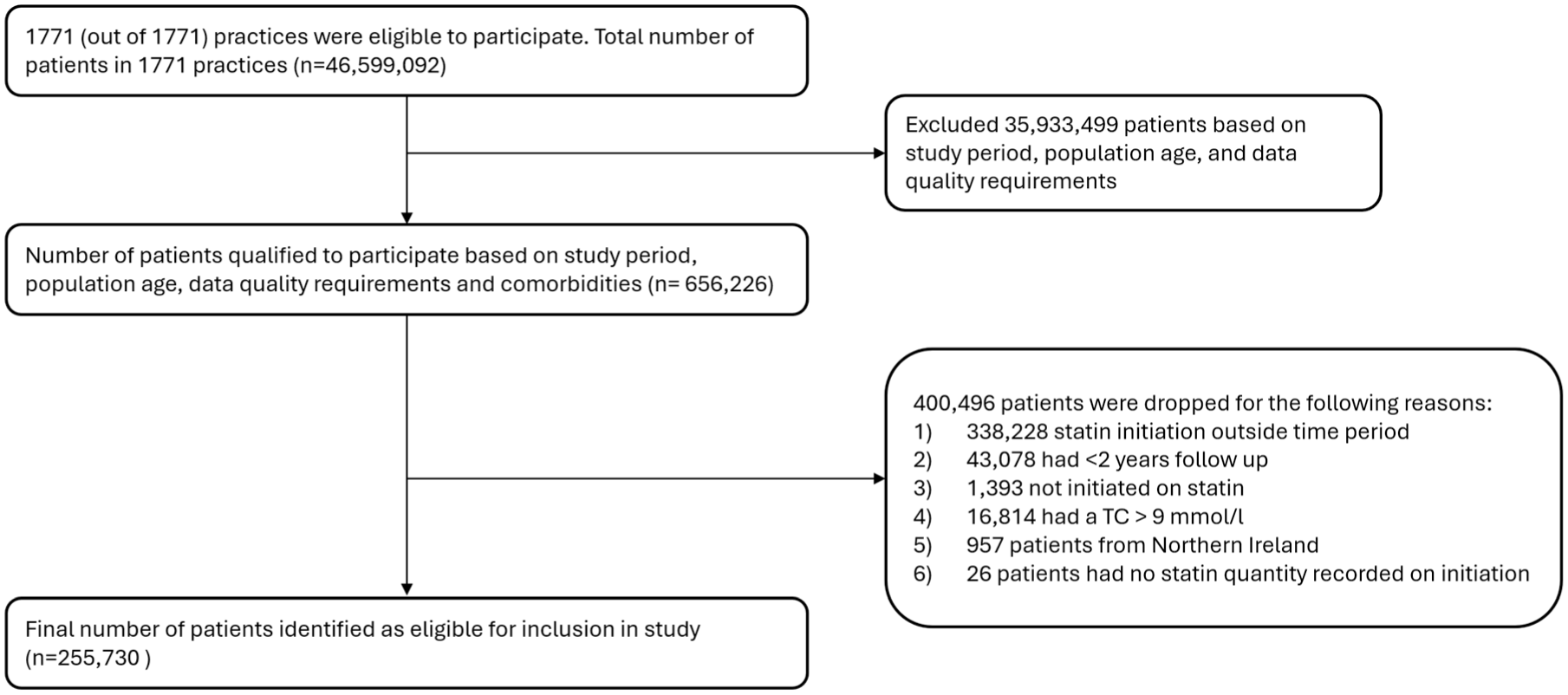
STROBE diagram.
Cohort Characteristics.
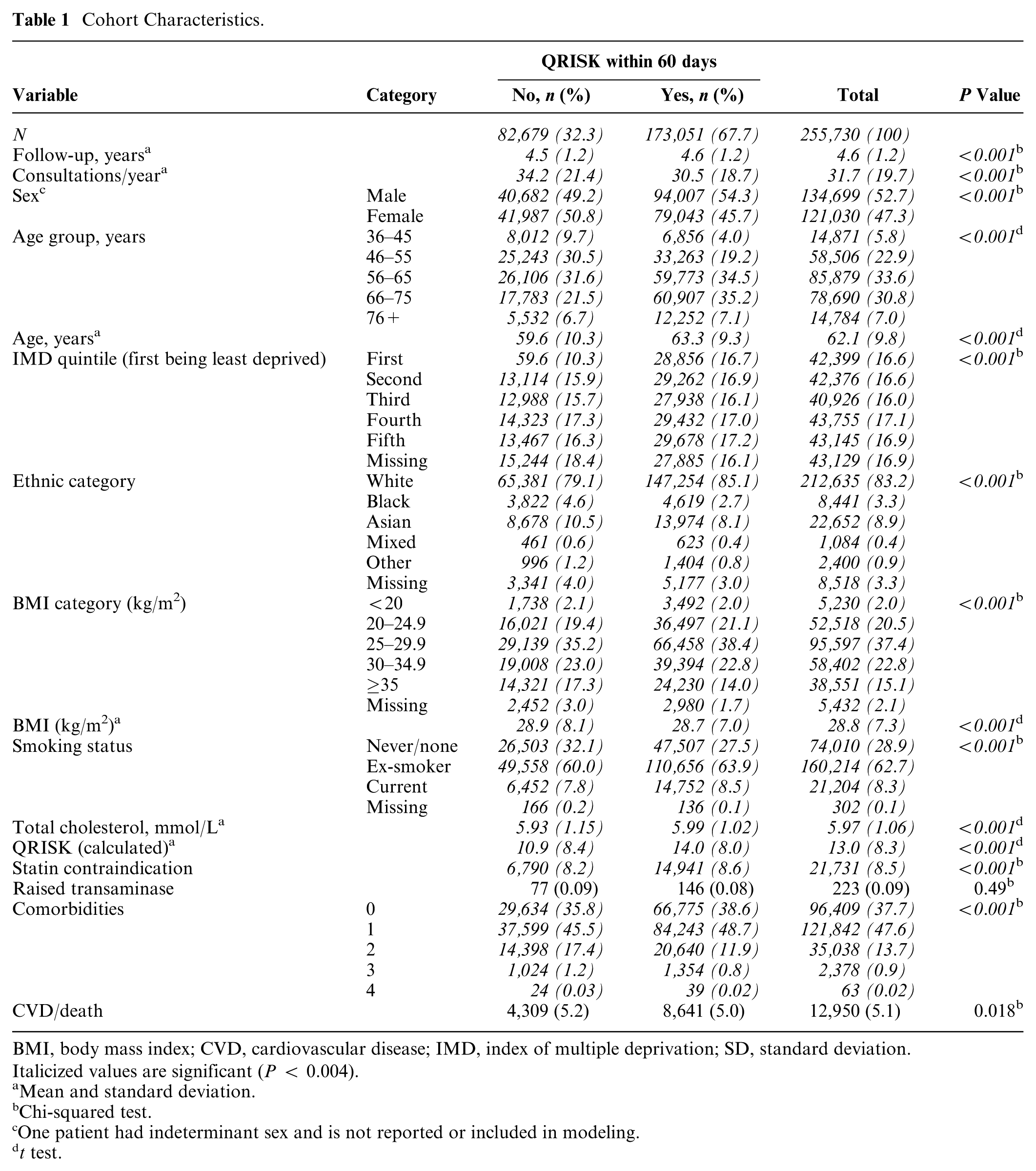
BMI, body mass index; CVD, cardiovascular disease; IMD, index of multiple deprivation; SD, standard deviation.
Italicized values are significant (P < 0.004).
Mean and standard deviation.
Chi-squared test.
One patient had indeterminant sex and is not reported or included in modeling.
t test.
The relationship between QRISK coding and demographic variables is expanded upon through logistic regression in Supplementary Table S1. Atorvastatin was the most common statin prescribed, comprising 93.4% of initial prescriptions and 89.7% of all prescriptions (Supplementary Table S2).
The MPR in the first year of follow-up (excluding people who received only the index prescription) was 82.4% (95% CI 82.3%–82.6%) in patients with a QRISK score compared with 80.9% (95% CI 81.8%–82.1%) in those without a QRISK score (P < 0.001). This is a small improvement in adherence in the population with a QRISK score, but this is an unadjusted figure. Figure 2 shows how the trend in adherence (MPR > 0.8) changed over the duration of observation and is consistently around 3% higher for people with a QRISK score coded compared to those without. Linear regression modeling using the MPR in year 1 as a continuous variable shows that the presence of a QRISK score was associated with increased adherence, alongside increasing age, BMI, baseline total cholesterol, and the number of comorbidities (Table 2). Female sex, increasing deprivation, and non-White ethnicities were negatively associated with the MPR, with very little collinearity between variables (mean variance inflation factor = 1.43). The calculated QRISK score was not significantly associated with the MPR.
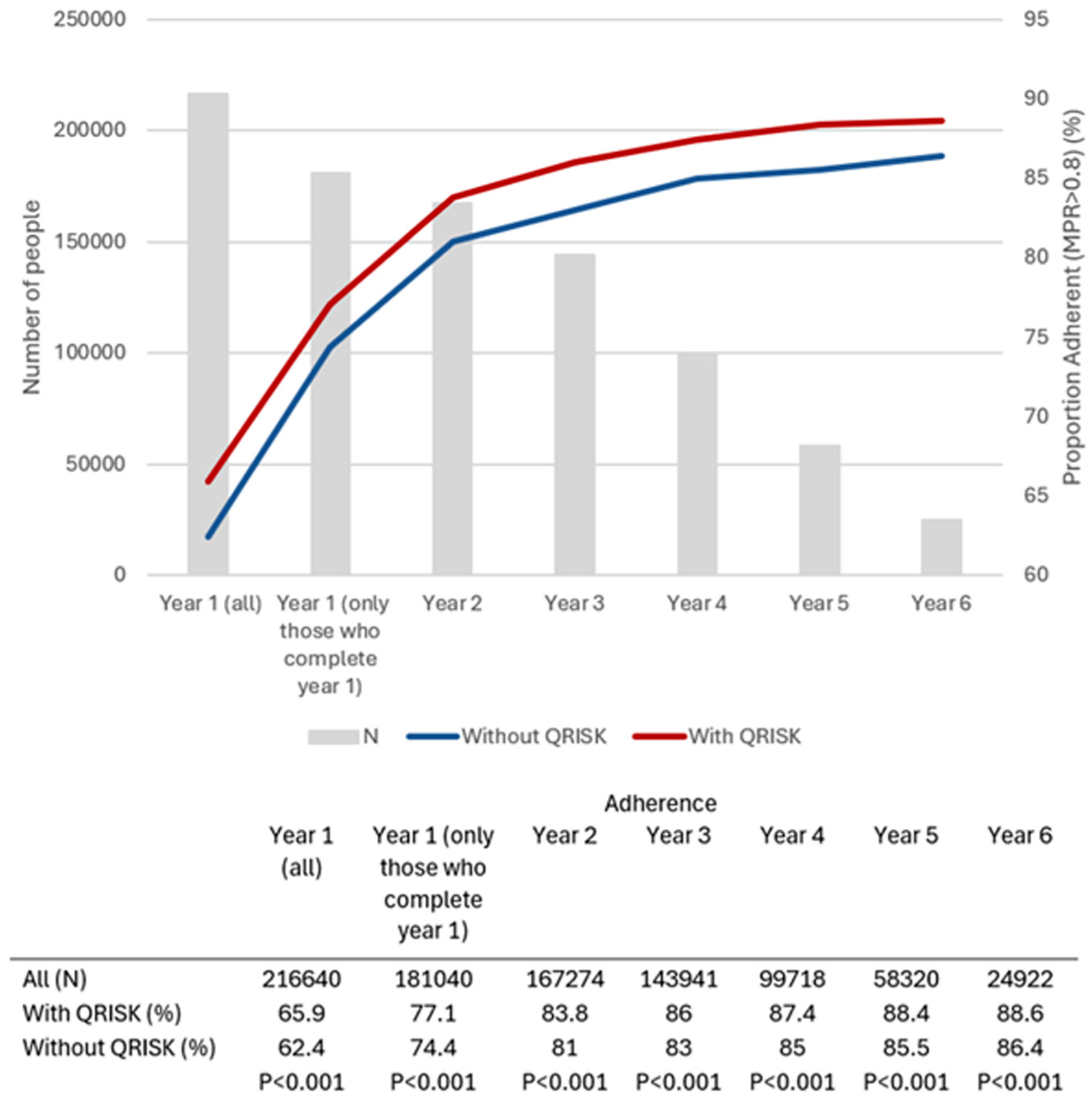
Number of participants per year of follow-up and adherence by QRISK status.
Effects on Variables on the MPR in Year 1 (Linear Regression)
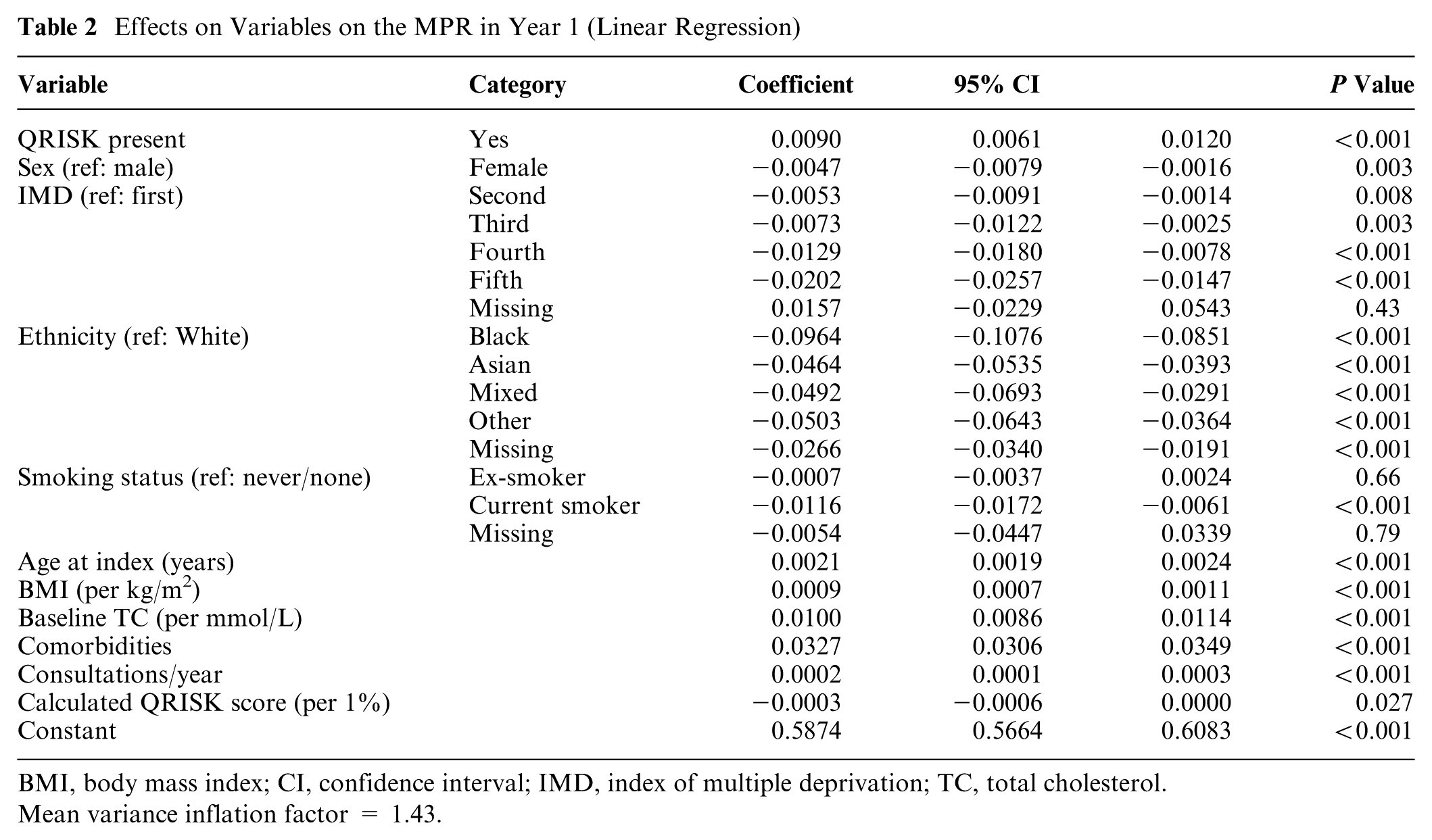
BMI, body mass index; CI, confidence interval; IMD, index of multiple deprivation; TC, total cholesterol.
Mean variance inflation factor = 1.43.
When adherence was modeled as a binary variable (MPR > 0.8) using logistic regression (Supplementary Table S2), the presence of QRISK increased the odds of adherence by 7% (odds ratio [OR] 1.07. 95% CI 1.05-1.10). The presence of comorbidities had the highest contribution to adherence, with a 26% increase in adherence per comorbidity, and all non-White ethnicities had significantly lower adherence, ranging from 61% lower (Black ethnicity) to 37% lower (mixed ethnicity).
Overall, 100,127 (39.2%, 95% CI 39.0%–39.3%) people discontinued their statin for >180 d during the observation period, 75,280 (29.4%, 95% CI 29.3%–29.6%) in the first year. The median time to discontinuation was 110 d (interquartile range [IQR] 56–369.) Of those who discontinued, 51,920 (51.9%) restarted a statin or other LLT with a median discontinuation period of 458 d (IQR 306–864 d). Supplementary Table S3 describes which medications were issued before and after discontinuation, and Supplementary Table S4 shows the number of discontinuations per year split by QRISK status. Figure 3 shows the differential discontinuation of statins for people with or without QRISK in an unadjusted Kaplan–Meier survival analysis. The results of the Cox regression analysis (adjusted for confounders and clustering at practice level) are shown in Table 3. The presence of QRISK coding reduced discontinuation by 8% (hazard ratio [HR] 0.92, 95% CI 0.91–0.94), and the risk of discontinuation was reduced by 10% for each 1-mmol/L increase in total cholesterol and 26% for each additional comorbidity. Non-White ethnicity and higher levels of deprivation were associated with an increased hazard for discontinuation.
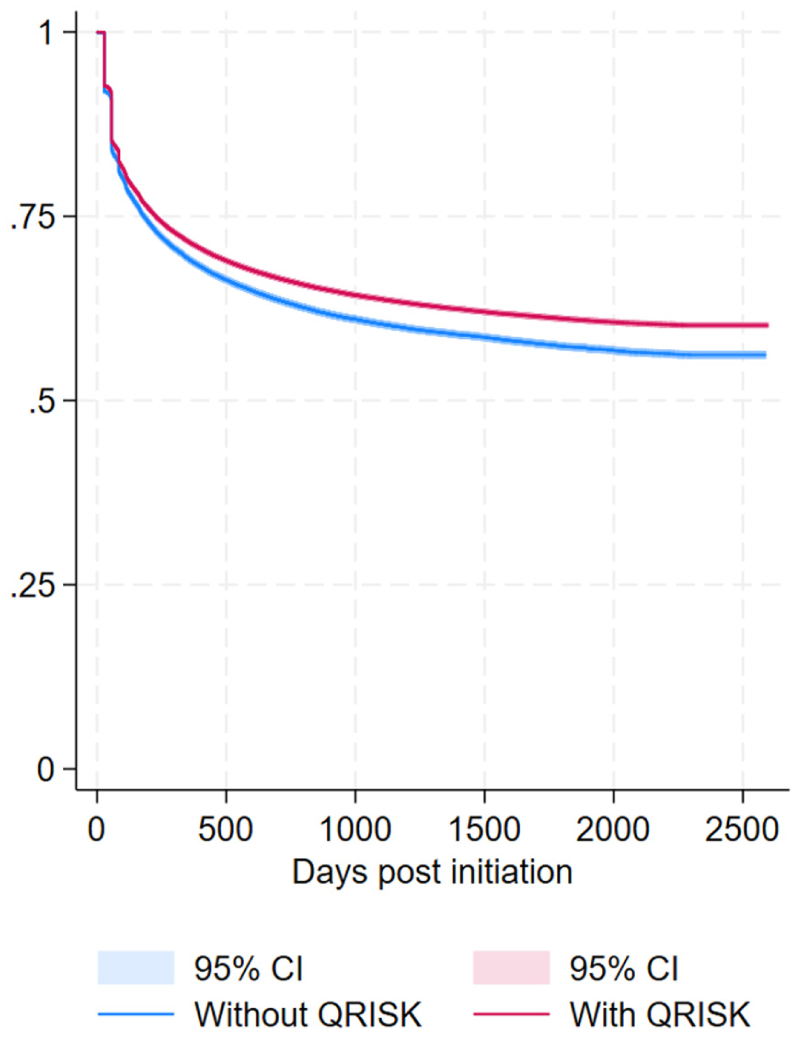
Kaplan–Meier curve showing the cumulative discontinuation rate for patients with and without QRISK (unadjusted).
Adjusted Cox Proportional Hazards Model for Discontinuation
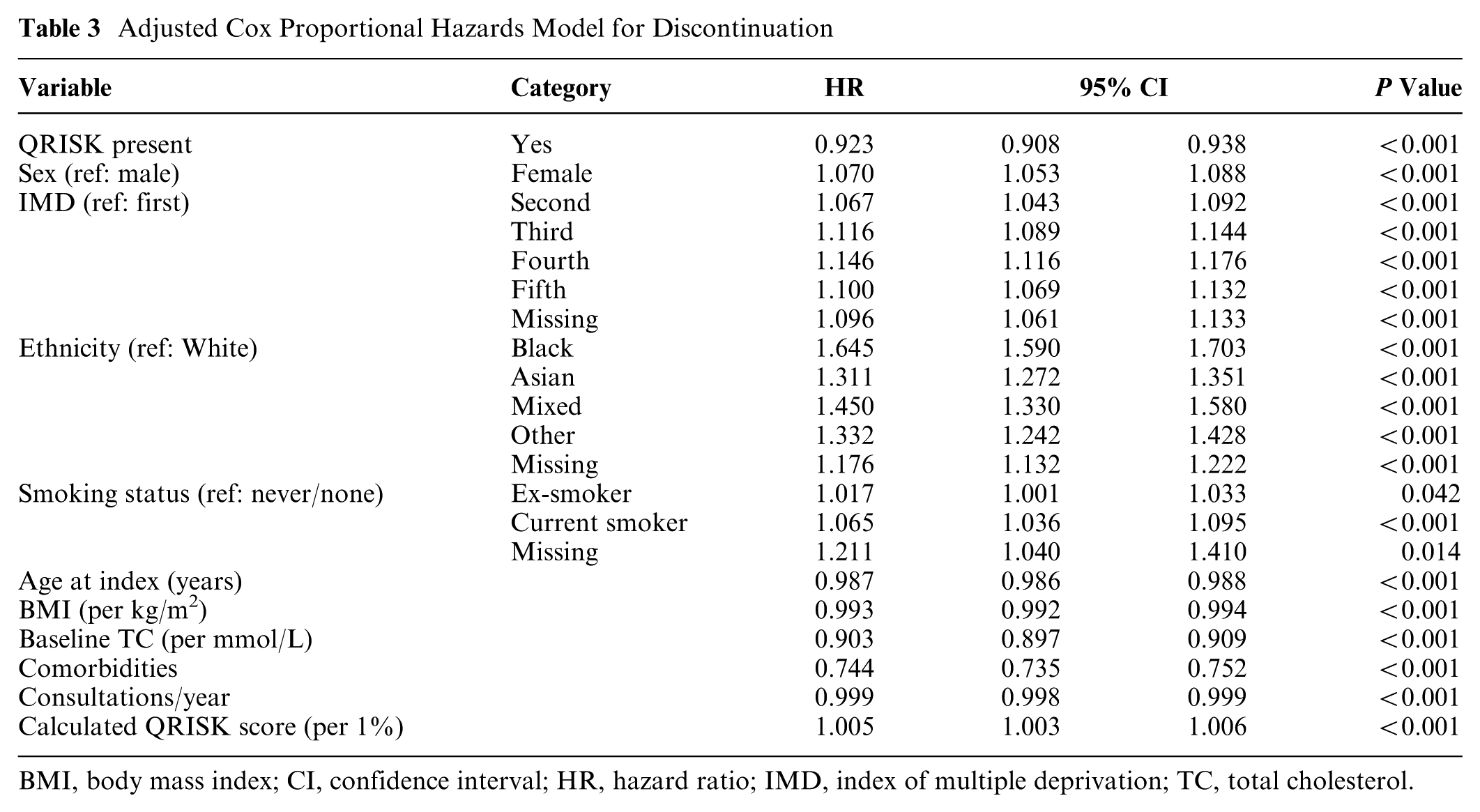
BMI, body mass index; CI, confidence interval; HR, hazard ratio; IMD, index of multiple deprivation; TC, total cholesterol.
A total of 12,950 (5.1%, 95%CI 5.0-5.2%) patients died or had a new diagnosis of CVD during follow-up, with similar proportions in both those with, and those without, a QRISK score. However, when adjusting for confounders in the Cox regression analysis, the presence of a QRISK score was associated with a 15% reduction in the risk of CVD/death (HR 0.85, 95% CI 0.82–0.88) (Table 4). The hazard ratio associated with a QRISK score for CVD events only was 0.89 (95% CI 0.48–0.94) and death only was 0.82 (95% CI 0.78–0.87). Current smoking was associated with the highest risk of CVD/death (2.02, 95% CI 1.89–2.16), and increasing risk was seen with increasing deprivation, but Black and “other” ethnicities had lower HRs when compared with White ethnicity, 0.68 (95% CI 0.6–0.79) and 0.64 (95% CI 0.51–0.81), respectively.
Adjusted Cox Proportional Hazards Model for Combined MACE/Death Outcome and Separate MACE and Death Outcomes
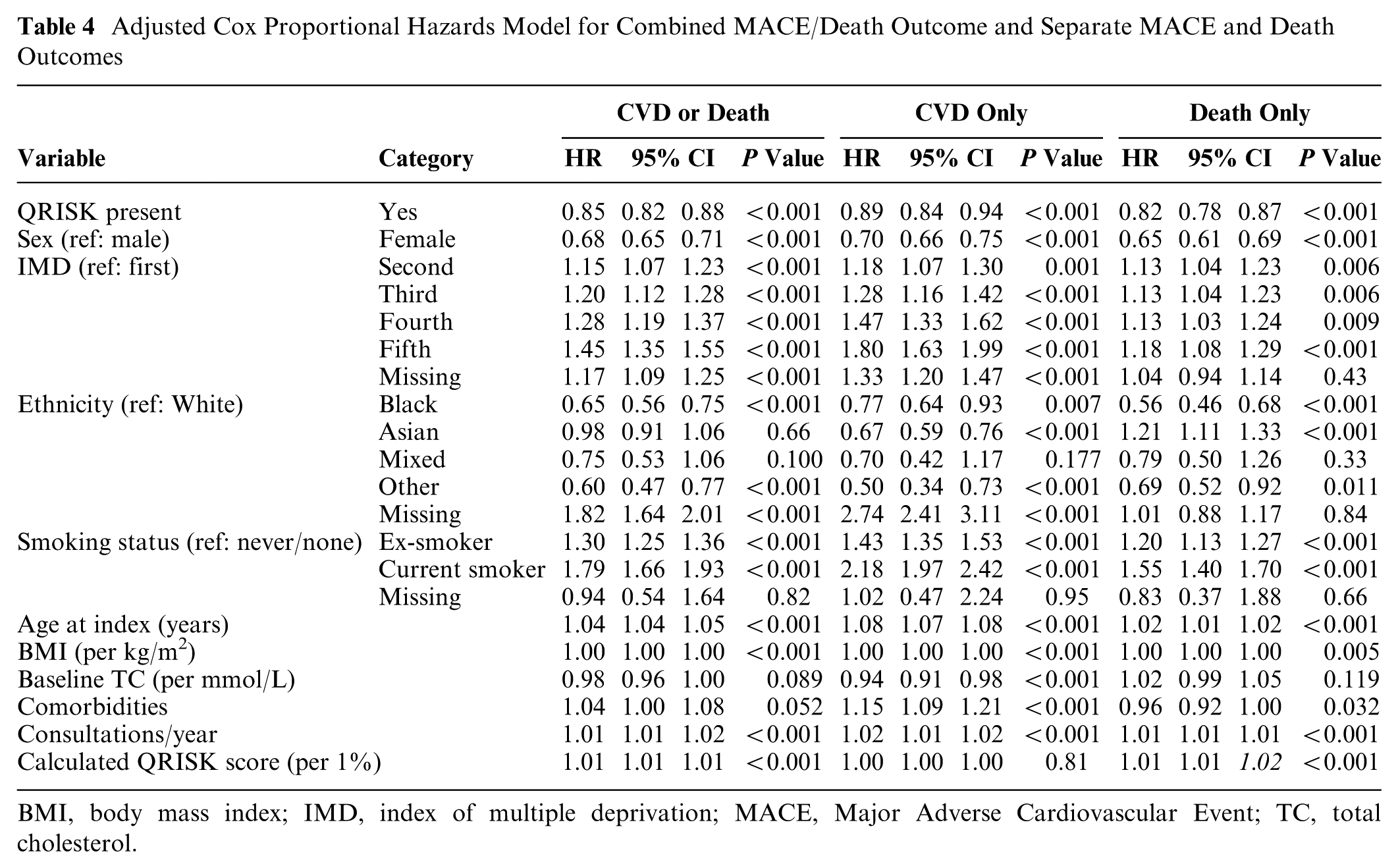
BMI, body mass index; IMD, index of multiple deprivation; MACE, Major Adverse Cardiovascular Event; TC, total cholesterol.
Mediation analysis showed that a small but statistically significant proportion of the reduction in CVD/death observed is mediated through improvement in adherence with little interaction between QRISK and the MPR (Supplementary Table S5). Similarly, mediation analysis looking at time on treatment showed that QRISK scoring led to a longer time on treatment, which reduced the odds of CVD/death; however, most of the direct effect is not explained by treatment duration.
The 2 sensitivity analyses did not reveal any significant differences when adherence and persistence were examined for all LLTs or when only prescriptions where the number of days matched the quantity of tablets (Supplementary Table S6). Finally, an analysis of other CVD risk factors that changed over the study period revealed that smoking cessation was less likely in the coded cohort (39.0% v. 41.1%, P = 0.005), whereas systolic blood pressure reduced more in the coded cohort (−4.0 mm Hg compared with −2.9 mm Hg in the uncoded group, P < 0.001).
Discussion
In this cohort, the presence of QRISK coding around the time of statin initiation is associated with modest but significant improvements in both adherence to, and persistence with, statins. QRISK coding is also associated with a significant (15%) reduction in the composite outcome of subsequent CVD diagnoses or all-cause mortality. It is implausible that this large reduction is fully explained by the combination of improved adherence and persistence, even though these improvements are likely to have an additive effect on CVD outcomes. Indeed, although there are limitations in the post hoc QRISK calculation, the CVD risk of the uncoded cohort is higher than the coded cohort, so one would expect worse outcomes in the coded cohort. This suggests that QRISK coding is associated with other factors that affect CVD risk that are not captured in this study. It could be that when QRISK coding is used, there is a more holistic discussion about CVD risk, which results in improvements in other risk factors. This is plausible since the act of populating the QRISK variables focuses attention (from both the clinician and patient) on these other risk factors. Although the observed changes in smoking habits do not support this hypothesis, a greater reduction in blood pressure was seen in the coded group; this difference may be due to greater health care involvement in the management of blood pressure than in smoking cessation. It is also possible that more effort is made to reduce CVD risk in the coded cohort since their risk is higher; however, a relationship between QRISK coding and adherence/persistence is present when the QRISK score is included in the model, suggesting that the differences seen are not just due to the CVD risk alone. In addition, when statins are started without a QRISK score, clinicians (and patients) are unaware of the degree of risk (clinicians are poor at estimating risk without calculating 36 ), but we can assume they believe the risk is high by virtue of the recommendation to start a statin. Ultimately, it could simply be that QRISK coding is a proxy for a higher standard of clinical care, which permeates the whole of an individual’s primary health care delivery, resulting in better outcomes. Further research is required to explore this important finding further.
Comparisons with Existing Research
Two-thirds of patient initiated on a statin had a QRISK score coded in their record in the 60 d prior to initiation. This is considerably higher than the 27.1% reported between 2012 and 2015 but consistent with the increasing trend noted at that time 37 and similar to the reported coding rate (within 6 mo of initiation) in 2017 to 2018. 38 QRISK recording was higher in males, older age groups, and people living with lower deprivation. Part of these demographic differences may be explained by the differences in the demographics of people attending the NHS Health Check program, which focuses on CVD risk and sees a higher uptake in low deprivation areas and among older people. 39
The adherence rates observed in the first year (>80%) were higher than observed in most other studies in systematic reviews.3,40 It is worth noting, however, that although an MPR of 0.8 is quite consistently used as a cutoff for adherence, there is variation in how the MPR is calculated between studies, and none of the included studies were UK based. In these reviews, increasing age, male sex, and lower levels of deprivation have previously been found to be associated with improved adherence, and this is consistent with our findings. Two studies, both from the United States, examined ethnicity and adherence and both found that non-White ethnicities had lower rates of adherence. The impact of ethnicity on adherence was notably high, particularly in the Asian, mixed, and other categories. A review into statin nonadherence also found that female sex, non-White ethnicities, and low socioeconomic status were associated with worse adherence. 41 We found a strong association between adherence and increasing comorbidities. In the literature, the association between adherence and comorbidities is complicated by differences between different diagnoses as well as between primary and secondary prevention, but some studies have also found that increasing comorbidities increase adherence, which is in line with our findings. 3 Comorbidities and coprescribing are likely to be associated, and although we did not measure coprescribing, there is similar conflicting evidence on the impact of polypharmacy on adherence in the preventive setting.4,42–45
The existing literature on persistence is highly variable in the definition of persistence, whether reported as a dichotomous or continuous variable, and in the duration of follow-up, meaning there are no direct comparisons with our findings. 40 Of the studies with longer durations of follow-up, there is large variation in persistence, with an Israeli study reporting >75% of patients discontinuing statin therapy by 2 y, 46 an American veteran cohort finding discontinuation rates of about 37% after 675 d, 47 and a Danish cohort (mixed primary and secondary prevention) observing only 16% discontinuation at 3 y. 48 The large impact that comorbidities have on persistence may be a result of increased opportunities to review medication that come with annual reviews of the long-term conditions that we included in our comorbidities list. These reviews, incentivized by the Quality and Outcomes Framework in England, 49 are opportunities to reinforce medicine-taking practices and address concerns. Frequent contact with physicians, particularly when it is the same clinician who initiated the statin, is associated with improved adherence and persistence. 50
Adherence to statins has been looked at as an outcome of interventions designed at improving SDM, and there seems to be a small but consistent effect size, similar to the 8% improvement in adherence seen in our adjusted model. In a primary care cohort, using a decision support tool focusing on CVD risk improved adherence at 12 mo by 5%. 6 Another study using the same intervention in patients with diabetes did not show a significant effect on adherence at 3 mo, although the small size of this study (n = 168) would make it underpowered to detect adherence differences around those we observed. 7 Similarly, a small study in a secondary prevention population showed improvements in adherence in the SDM intervention group of 7% (unadjusted), but this was not statistically significant. 8
Finally, there has been found to be a “clinician component” to statin adherence. An American study showed that when prescriptions are written by a patient’s own primary care provider, adherence rates are higher (OR 1.12), 51 and a questionnaire-based study found that the type and level of information shared during consultations and the quality of consultation positively correlated with statin adherence. 24 A Danish study showed the “health management skills” of a physician (defined as the ability to facilitate adherence with statins) positively affect health outcomes. 23 These results suggest that the interpersonal skills and competencies of the clinician affect subsequent statin adherence. It is likely that the association we have found between QRISK scoring and adherence, persistence, and, ultimately, CVD outcomes and death is, at least in part, a proxy measure for the clinician component statin initiation consultations.
Strengths and Limitations
This study is a comprehensive examination of primary prevention statin adherence and persistence and, for the first time, harnesses the power of a large English primary care dataset to investigate whether some facet of the statin initiation consultation (as measured by QRISK coding) affects subsequent statin use and outcomes. By using electronic prescribing records, we have a complete understanding of prescriptions issued to patients in a dataset that is generalizable to the English population, allowing a high degree of precision in the results. We also considered the potential impact of other LLTs in our analysis given the increasing use of these for people intolerant to statins but found this did not significantly affect the results.
One key limitation of this type of study is that we are using prescriptions issued as a proxy for medications taken. It is acknowledged that, following prescribing, the medication must be dispensed, collected, and, ultimately, taken by the patient, and adherence/persistence could be affected at any point in this chain. Thus, the adherence/persistence levels we observed are the maximum possible levels, with potential for the real numbers to be reduced at several points. Other ways to measure adherence/persistence are possible, including directly observing medicine taking, using electronic pill dispensers, or self-reporting of medicine taking. Each has its limitations, 4 and none would allow the large number of participants and long follow-up we have achieved in this study. Given that statins are long term, repeat prescriptions, it is likely that the link between prescription and medicine taking is stronger than one-off or short-term prescriptions since the patient keeps coming back for a top up of their supply, indicating a likelihood of a reduced stock in the patient’s home, although some patients may stockpile medications.
Some patients restarted LLT after a period of discontinuation. The prescriptions after restarting were not included in the analysis, and this may weaken the association with adherence/persistence and CVD outcomes, as patients may be more adherent on restarting but the link with the initial statin consultation will have been lost.
Finally, we are assuming that when a QRISK score is coded in the record that it is communicated to the patient and used in the initiation consultation through an SDM process. We have shown that more than 50% of the QRISK2 scores coded prior to statin initiation are calculated on the day of initiation, suggesting that this risk score is being used in the consultation. However, it will not always be the that the risk score is used in SDM; the score is necessary but not sufficient for SDM to occur. Thus, the association between QRISK scoring and adherence/persistence and outcomes would be diluted. Importantly, though, the lack of a QRISK score would be a clear impediment to SDM being undertaken. It is also possible that clinicians engage in SDM guided by CVD risk estimates without a coded QRISK score, but, as stated previously, this is not likely to be common given the subsequent observed prescribing patterns. 17 In addition, it is likely that there is residual confounding in this retrospective cohort study, which may explain some of the large differences in CVD outcomes and death that we observed.
Implications
There is a clear indication in our findings that the presence of a QRISK score at the time of statin initiation is associated with improvements in adherence and persistence. We argue that this could be due to a better quality of consultation when a QRISK score is present and a higher likelihood that SDM has taken place. Thus, although there is understandable focus on ensuring the right people are offered a statin, we must also pay attention to how a statin is initiated to ensure that all patients have a high-quality, risk-informed discussion. In addition, the large decrease in the development of CVD or all-cause mortality associated with the presence of QRISK coding cannot be explained by statin adherence/persistence alone and warrants further investigation. It could be that the use of QRISK is a marker of the quality of care that patients are receiving, which could be potentially useful in the quality assurance processes of English primary care.
Supplemental Material
sj-pdf-1-mdm-10.1177_0272989X261455267 – Supplemental material for Cardiovascular Risk Estimation and Statin Adherence: A Historical Cohort Study
Supplemental material, sj-pdf-1-mdm-10.1177_0272989X261455267 for Cardiovascular Risk Estimation and Statin Adherence: A Historical Cohort Study by Samuel Finnikin, Brian Willis, Tim Evans, Brian Finney, Kwan Nok Chris Hui, Rani Khatib and Tom Marshall in Medical Decision Making
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
This work was undertaken at the Department of Applied Health Sciences, College of Medical and Dental Sciences, University of Birmingham.
Ethical Considerations
The protocol for this article (23_003321) was approved by the CPRD review board.
Consent to Participate
Not applicable.
Consent to Publication
Not applicable.
Data Availability
S.F. had full access to the data used in this research. Primary data are not available through the authors due to data-sharing restrictions but are available to researchers through CPRD (subject to approvals). Code lists used in data extraction and processing are available on request from the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.