
Abstract
The novel coronavirus disease 2019 (COVID-19) pandemic has rapidly wrought havoc on the world, exposing the gaps in public health systems of countries that were previously considered most prepared for infectious disease outbreaks. Notably, despite being ranked highest on the Global Health Security Index, the United States has been severely hit with nearly two million confirmed cases and one hundred thousand deaths by the end of May 2020. In addition to the public health fragmentation from the federal to the state level and lagging regulations, early reports highlight substantial socioeconomic disparities and health system barriers contributing to the spread and impact of the pandemic in the United States. In this review, we explore the impact of COVID-19 on public health systems by assessing systems through the lens of the Centers for Disease Control and Prevention’s Ten Essential Public Health Services. Building on prepandemic and COVID-19 observations and lessons, we propose recommendations moving forward to prepare for future waves and other disease outbreaks.
Introduction
The novel coronavirus disease 2019 (COVID-19) and SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), the virus causing COVID-19, have led to an unprecedented impact on the modern world. As of mid-May 2020, nearly five million people have been confirmed with COVID-19 worldwide, already causing tens of thousands of deaths (Dong et al., 2020). On March 11, 2020, the World Health Organization (WHO) officially called the SARS-CoV-2 outbreak a global pandemic, with most of the world following with national lockdowns or shelter-in-place policies. The outbreak in the United States far exceeds the original outbreak in China and makes it—together with Western Europe—the new epicenter of the pandemic (Dong et al., 2020).
Prior to the COVID-19 pandemic, the United States was considered to have one of the most robust public health systems in the world, especially strong in terms of emergency preparedness. The Global Health Security Index ranked the United States as the most prepared country in the world to handle infectious disease outbreaks (Cameron et al., n.d.). Ironically, the pandemic is wreaking most havoc in the presumably most prepared country in the world. The inability of the U.S. public health system to do a better in preventing and mitigating the national COVID outbreak may indicate that technological advancements in the U.S. health care system were mistaken for basic and essential public health and emergency preparedness. It is clear that, although the United States spends nearly four trillion dollars each year on health—more than any country in the world—investments in public health have remained substantially less. Public health spending in the United States is less than 3% of total health spending, at only US$274 per capita per year (Christopher et al., 2019; Himmelstein & Woolhandler, 2016). This is especially surprising given public health’s potentially high return on investment as high as 14-to-1 in high-income countries (Himmelstein & Woolhandler, 2016).
In the United States, public health is mainly a function of the state and local governments, with the federal government playing a role through creating guidelines and regulating interstate commerce which impacts public health goods and services such as testing kits and pharmaceuticals. The main federal public health institutions include the Department of Health and Human Services, the Centers for Disease Control and Prevention (CDC), and the Food and Drug Administration (FDA).
Here, we evaluate the impact of the COVID-19 pandemic on public health systems, with a particular focus on the U.S. public health system, using the CDC’s Ten Essential Public Health Services (Table 1) (“Public Health System and the 10 Essential Public Health Services,” 2019).
The Effects of the COVID-19 Pandemic on the U.S. Public Health System and Recommendations for the Recovery, Using the Centers for Disease Control and Prevention’s (CDC) Ten Essential Public Health Services.
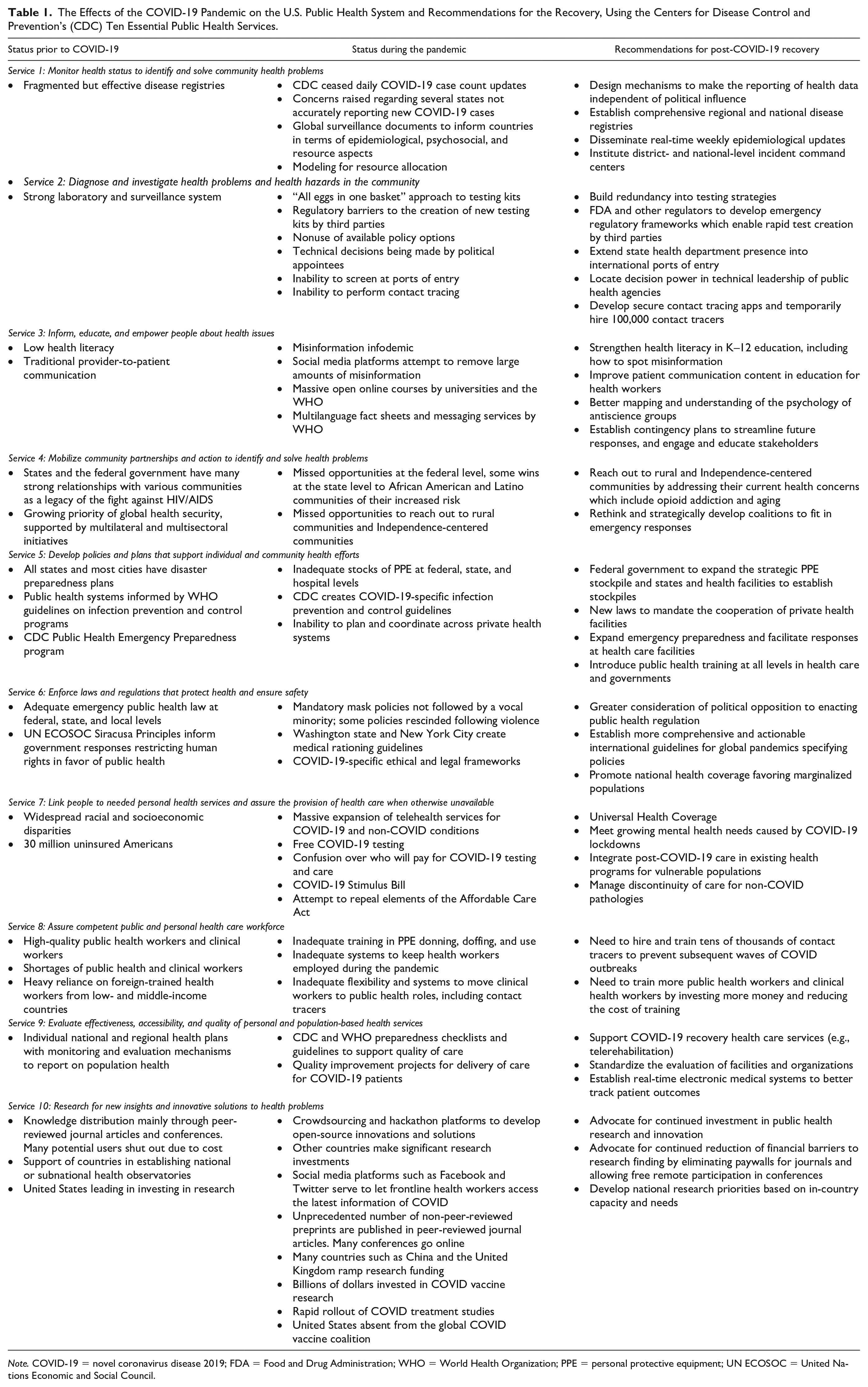
Note. COVID-19 = novel coronavirus disease 2019; FDA = Food and Drug Administration; WHO = World Health Organization; PPE = personal protective equipment; UN ECOSOC = United Nations Economic and Social Council.
Essential Public Health Services
Service 1: Monitor Health Status to Identify and Solve Community Health Problems
Prior to COVID-19, fragmented but effective disease registries had been leveraged to address local health needs. Around the world, these have demonstrated the potential to improve health care delivery adapted to local contexts and, importantly, propelled by the effective use of community health workers surveilling households and local communities. Amid the pandemic, the CDC discontinued reporting new case numbers, despite it constituting one of the most important pieces of data to assess the size of an outbreak and the effects of mitigation measures. In this data vacuum, many different organizations and initiatives have made an attempt to comprehensively map the number of confirmed cases, deaths, and recovered cases. The Johns Hopkins University Center for Systems Science and Engineering has established a transparent dashboard visualizing data on the national and subregional levels on a continuous basis. The WHO put out global surveillance documents and situation dashboards to inform countries in terms of epidemiological, psychosocial, and resource aspects. The Institute for Health Metrics and Evaluation, notably responsible for tracking the Global Burden of Disease study, has further enabled models to project resource allocations and morbidity and mortality projects for the United States and all individual states, depending on different public health measures taken. Controversies occurred over states such as Virginia combining data on positive antibody tests with data on positive RNA tests. In addition, the states of Georgia and Florida received criticism for taking steps which were perceived as suppressing data on positive cases.
In the post-COVID-19 rebuild, the need for more comprehensive regional and national disease registries, especially for infectious diseases, has become apparent. There is an urgency for real-time updates, similar to the CDC’s Morbidity and Mortality Weekly Report in the United States, which may better and more promptly inform policymakers and state leaders to take appropriate action. It has become clear that data must be protected from political influence and that, when the availability and interpretation of data are affected by politics, public health leaders must bring it to the public’s attention. Furthermore, district- and national-level incident command centers ought to be set up, staffed by public health professionals, to more effectively and rapidly deploy resources for the isolation of confirmed cases and the mitigation of outbreaks. (Sellers et al., 2019). Lessons from the SARS and Ebola outbreaks, now visibly effective in keeping the spread of SARS-CoV-2 at a minimum in East Asia and much of West and Central Africa, must be integrated into conventional public health measures. This will include the introduction of vigilant contact tracing approaches in case of emerging or reemerging infectious diseases. It is estimated that approximately 100,000 public health workers and an investment of US$3.6 billion is necessary to establish a comprehensive contact tracing workforce; digital contact tracing may substantially reduce costs and be equally, if not more, effective but brings privacy concerns and perceived infringement on individuals’ freedom with it. Google and Apple are now collaborating to enable such digital contact tracing through Bluetooth-enabled smartphone applications, pending higher-level decisions (Scott, 2020).
Service 2: Diagnose and Investigate Health Problems and Health Hazards in the Community
Before the pandemic, the U.S. public system had a strong public laboratory system and a strong system of screening for and reporting infectious diseases, especially influenza and other respiratory infections, tuberculosis, and sexually transmitted infections, including HIV. Baseline disease surveillance was conducted to identify and explore potential health threats in communities. For example, for the flu and flu-like symptoms, the United States participated in the WHO Global Influenza Surveillance and Response System surveilled and responded to seasonal, pandemic, and zoonotic influenza, alerting the global health community in case of worrisome deviations of endemic and expected epidemiological spread (“Global Influenza Surveillance and Response System [GISRS],” n.d.). The United States also participates in other global surveillance systems such as HealthMap which serves as early warning systems curated on a real-time basis.
During the COVID response, it is this “diagnose and investigate” function that encountered the greatest challenges. Rather than using the WHO COVID-19 test which had been developed by a prominent German lab, the United States chose to develop its own test, which it often does for new diseases. However, this “all eggs in one basket” approach backfired when there was a manufacturing flaw in the CDC’s testing kits and weeks of potential testing were lost. The diagnosis and investigation function was also compromised by rigid FDA rules that barred state labs and private labs from developing their own kits. In fact, much of what is known about the early stages of the Washington state outbreak is known because a research science developed and used a COVID-19 test against the FDA policy. In addition, the Defense Production Act (DPA), one of the most powerful tools to increase access to products and services in emergencies, has, as of the publication of this article, not been used to increase access to testing kits. This is despite the fact that the DPA is employed on a regular basis for the U.S. military.
A major challenge during the outbreak was the inability to access timely, accurate data. The CDC had trouble getting data from states and from private testing labs and stopped updating its website daily. This led to the states, epidemiologists, physicians, and the general public turning to nongovernment sites such as the aforementioned Johns Hopkins ArcGIS Coronavirus Dashboard (“COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU),” n.d.).
Another flaw that was revealed was the lack of coordination between state departments of public health and the international ports of entry in states (international airports, ports, and land border crossings). After the CDC issued guidance that travelers coming from certain high-risk areas should be identified and screened for fever and COVID symptoms, tested, and quarantined, there were multiple reports of this not being done. In addition, there were reports of gross crowding of air passengers with little or no separation of symptomatic and asymptomatic travelers.
Standard public health measures to contain infectious disease outbreaks include contact tracing. However, the COVID pandemic rapidly overwhelmed the contact tracing capacity of the CDC and state and local departments of health. Neither the CDC nor state governments released contact tracing smartphone applications for the public. However, several other organizations did, most notably MIT’s SafePaths, and Google announced that it was working on an app.
After the pandemic, it will be necessary to develop efficient mechanisms and detection tools to more rapidly and accurately identify cases of COVID-19 and other infectious diseases. The low sensitivity of contemporary SARS-CoV-2 testing kits illustrates that many positive cases may falsely be assured not to have COVID-19, which complicates effective disease containment. In addition, laboratories nationwide should be equipped with the minimum requirements to be able to quickly scale-up testing. Furthermore, actionable protocols to screen incoming travelers at all land, sea, and air borders are necessary to mitigate a likely inevitable second wave of COVID-19. This will be complemented with experiences from contemporary social distancing and shelter-in-place policies, as well as informed by findings from lockdowns on the city, state, regional, and national levels in different parts of the world.
Furthermore, some of the broader challenges revealed by the pandemic should be addressed during the recovery. The United States should adopt a policy of “testing redundancy” for new diseases to ensure that no similar delay in testing ever happens again. In addition, the FDA should develop a set of emergency regulations that can be triggered automatically if the WHO declares a Public Health Emergency of International Concern (PHEIC) or can be activated by FDA technical leadership. Where possible, decision authority should be migrated from CDC and FDA political leadership (“Plum book” positions) to technical leadership. This approach does not infringe on political appointees’ ability to lead as they retain the power to block action, but it will then be on the record as an active blocking of the decisions of the technical leadership rather than the passive failure to act. State departments of health need to establish their presence in international ports of entry to ensure compliance with the screening of travelers. In addition, as part of regular infectious disease surveillance, international travelers should be periodically screened for fever and other infectious disease symptoms.
To improve contact tracing, the Johns Hopkins Center for Health Security recommends that 100,000 employed or volunteer contact tracers be hired. It is important that this cohort of contact tracers be reflective of each state’s communities with special emphasis on mobilizing tracers from hard-hit minority and rural communities. In addition, contact tracing apps need to be developed that people can download onto their phones, securely record their movements, and selectively share with public health authorities only if they test COVID positive. Nevertheless, such interventions have to balance population health with the individual right to privacy. Organizations trusted by different communities should be encouraged to create tracing apps. For example, organizations trusted by rural communities, African American communities, and Latino communities should be encouraged to create contact tracing apps for their communities.
Service 3: Inform, Educate, and Empower People About Health Issues
Before the COVID pandemic, the United States struggled with low health literacy, especially among poor, minority, and rural communities. One in three Americans did not have sufficient health literacy compared with one in 10 Europeans (Baker et al., 2002; Sørensen et al., 2012). In addition, a growing antivaccination movement had led to multiple measles and whooping cough outbreaks in the United States.
There currently is a misinformation infodemic which combines both science and political disinformation and is unlike any seen in previous epidemics is its speed and scope. The misinformation is being combated aggressively by health care and public health professionals alike. Innovative communication projects attempt to reach indigenous populations and rural communities living in the last mile in sub-Saharan Africa, efforts supported by the Africa CDC and the Co-Creation Hub.
Now, several frontline initiatives and online crowdsourcing have enabled and empowered individuals to be educated on COVID-19, its health implications, and infection prevention and control. In addition to official information by public health authorities such as the CDC, open-access training modules have been rolled out by, for example, the WHO, Johns Hopkins University, and the London School of Hygiene and Tropical Medicine, accessed by millions of individuals to date. Moreover, the WHO and universities—spearheaded by students—have rolled out messaging services to correctly inform the public in dozens of languages, amid the contemporary infodemic and growing spread of misinformation. Social media platforms such as Facebook and Twitter tried to remove misinformation and to provide trusted channels of correct information.
Beyond the pandemic, contingency plans are necessary to streamline future responses and educate stakeholders on measures and actions to take. These can, and should, entail opportunities for community engagement and civil society participation through health education and promotion mechanisms. Content on how to combat misinformation should be integrated into health workers’ education. In addition, health content in public K–12 education should be increased and include how to access the validity of medical claims.
Service 4: Mobilize Community Partnerships and Action to Identify and Solve Health Problems
Previously, the U.S. federal government and state governments had formed partnerships with at-risk communities. In addition, partnerships were built with the private sector at the national and global levels. Growing public–private partnerships have enabled increasing support of the public health and public health care sector, especially in low- and middle-income countries, strengthening countries’ and regions’ health care systems. Multilateral and multisectoral initiatives were proposed to optimize global health security; here, the GAVI Alliance, as a partnership of public, private, and nongovernmental organizations, has become an important stakeholder in supporting countries’ global health security, particularly through deploying new preventive vaccines.
During the outbreak, the United States focused mainly on hospital-based care and did not activate its partnerships with community groups and other constituencies. Some states were able to work with Latino and African American groups to inform them of their greater risk. However, there were missed opportunities for community partnership at the state and federal levels. Public–private partnerships were also not sufficiently engaged, as exemplified by the lack of engagement of the private sector to produce adequate amounts of personal protective equipment (PPE) and testing kits. Because the federal government declined to partner with states on a variety of elements of the response, states partnered together to purchase PPE and coordinate the reopenings of their economies.
After COVID-19, coalitions need to be rethought and strategically developed to fill necessary roles in emergency responses. A global response will always be hindered by the weakest link in a chain, requiring holistic and collaborative approaches to strengthen every partner involved. Stakeholders should hereby also focus their efforts on rebuilding health systems in countries and areas that may be most heavily hit by the current pandemic, which notably includes low- and middle-income countries where fragile health systems are commonly in place. Although lessons were drawn from previous outbreaks and endemic infectious diseases, critical care capacity is severely lacking in the majority of low- and middle-income countries, putting unprecedented strain on these systems and risking an inability to adequately manage a rapid surge in cases—complicated by the population-level difficulty to stop work and shelter-in-place (Ma & Vervoort, 2020).
Service 5: Develop Policies and Plans That Support Individual and Community Health Efforts
Prior to the pandemic, all U.S. states and most U.S. large to midsized cities had disaster preparedness plans and many states had run outbreak simulations. Countries had put public health systems in places informed by WHO guidelines on infection prevention and control programs. These guidelines ensured appropriate baseline necessities to respond to outbreaks on the national level and at the facility level. Along these lines, in the United States, the CDC had developed a Public Health Emergency Response Guide to inform states, cities, and tribes, as well as funded health departments through its Public Health Emergency Preparedness program (CDC, 2011).
In response to COVID-19, the CDC, as well as other national public health authorities in other countries, put out infection prevention and control guidelines to support individual and community health efforts in the fight against COVID-19 (“Infection Prevention and Control During Health Care When Novel Coronavirus (nCoV) Infection Is Suspected: Interim Guidance,” 2020; “Interim Infection Prevention and Control Recommendations for Patients With Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings,” 2020). These guidelines have been deployed in both community settings as well as health care settings, to protect population health and frontline health care workers. During the outbreak, it was clear that states had difficulties planning across private sector hospitals and getting them to collaborate. For example, it was very difficult for states to get patients or equipment (such as ventilators) transferred from one hospital to another, whereas this was commonplace in Europe.
Once the initial peak has subsided, comprehensive policies are necessary to expand emergency preparedness and facilitate responses at the level of health care facilities, which have been burdened by substantial administrative barriers to responding timely and efficiently. New laws need to be created to mandate the cooperation of private health facilities during health crises. In addition, public health training at all levels—in health care and governments—is critical to ensure that different stakeholders are capable of responding to outbreaks as pertinent to their skills and positions. Through overarching coordination of different actors within federal, provincial, state, city, and local governments during a public health emergency, this will help accelerate decisions and measures taken without delays.
Service 6: Enforce Laws and Regulations That Protect Health and Ensure Safety
Since the WHO’s inception in 1946, individuals’ “right to health” was included in the WHO constitution and later solidified by the United Nations International Covenant on Economic, Social, and Cultural Rights in 1966. In 1984, the United Nations Economic and Social Council adopted the Siracusa Principles which provided authoritative guidance on governmental responses restricting human rights in favor of public health’s interest, provided that these actions are lawful, proportionate, necessary, and of limited duration (Siracusa Principles, 1985).
Now, ethical and legal frameworks have been critical to more promptly respond to the COVID-19 crisis. Governments have the responsibility to balance the best interest of public health with civil liberties; in the United Kingdom, the Public Health (Control of Disease) Act of 1984 enabled that cases, who may pose harm to population health, can be identified, screened, and isolated. Globally, the International Covenant on Civil and Political Rights, as formal international human rights law, legalizes this on a larger scale, if appropriate and proportionate, in line with the Siracusa Principles (“Human Rights Dimensions of COVID-19 Response,” 2020).
The lessons learned from the pandemic will help inform international guidelines during times of global pandemics. Notably, the effectiveness of travel bans, school closures, and other policies will have to be evaluated to ensure more appropriate actions during future pandemics and epidemics in the best interest of public health. For example, although school closures have been instituted in many countries worldwide, including much of the United States, Singapore’s open schools were not initially a cause of rapid disease spread, although it is uncertain whether it contributed to the more recent sudden explosion in domestic COVID-19 cases. In addition, national health coverage policies should create health, social, and economic protections for populations that are marginalized by public health emergencies. This is visibly seen as a result of COVID-19 in the United States, where millions of American have filed for unemployment benefits, health insurance coverage has reduced substantially as a result of losing work, homeless people are not adequately provided with the necessary shelter-in-place opportunities, and American Indian reservations (e.g., Navajo Nation) have been extensively hit by the outbreak.
Service 7: Link People to Needed Personal Health Services and Assure the Provision of Health Care When Otherwise Unavailable
Already prior to COVID-19, health disparities and inequalities were widespread across the world. In the United States, nearly 30 million Americans were uninsured prior to the pandemic, and racial and socioeconomic differences in health outcomes have maintained health and socioeconomic disparities.
Currently, telehealth services have been upregulated to prevent patients from coming to the hospital or doctor’s practice for triaging or continuity of other medical care. Moreover, although COVID-19 testing was initially expensive and not accessible for those without comprehensive health insurance coverage, the Families First Coronavirus Response Act (H.R.6201) in the United States has ensured free testing, limited paid emergency leave and unemployment insurance, and food security initiatives (Benfer & Wiley, 2020). Similarly, the Health Care Priorities For A COVID-19 Stimulus Bill has strengthened Medicaid access and financial risk protection for vulnerable populations, particularly covering necessary medical care for COVID-19 (Forman et al., 2020).
As countries recover from the pandemic, it will be important to incorporate comprehensive post-COVID care in existing health programs that address vulnerable and at-risk populations. Early reports of recovered cases suggest the deleterious effects of the lived infection on the lung function and cardiovascular health. Moreover, the mental health and socioeconomic repercussions of the pandemic, notably among those who lost their jobs or loved ones, and health care workers, will be enormous. In addition, the discontinuity of care for non-COVID pathologies and chronic conditions, as well as threats for other potential infectious disease outbreaks, will put substantial strain on health systems, especially so in countries with market-based (e.g., the United States) or fragile health systems.
Service 8: Assure Competent Public and Personal Health Care Workforce
Prior to the COVID pandemic, the United States had a central-level public health workforce that was considered one of the best in the world, but which had decreased from its peak a few years before. The CDC has more than 10,000 employees, and the Department of Health and Human Services and National Institutes of Health (NIH) also employ thousands of public health professionals. However, in recent years, many positions have been cut or purposely left unfilled to reduce budgets. This includes the elimination of the White House global health security team and the cutting of the CDC global disease outbreak prevention budget by 80%, leading to China being removed from the program (Andrzejewski, 2020). The Association of Schools of Public Health (ASPH) has estimated that there is currently a shortage of more than 250,000 public health workers in the United States, including public health physicians, public health nurses, epidemiologists, health care educators, and administrators. In fact, in 2000, there were 448,000 public health workers in the United States, more than 10% less than that in 1980 when the population was smaller and healthier (“Confronting the Public Health Workforce Crisis,” 2008).
Ensuring adequate numbers of clinical health workers is also a public health responsibility. Although the United States enjoys some of the best physicians, nurses, and other health workers in the world, it suffers from a shortage. The Association of American Medical Colleges (AAMC) estimates that there is currently a shortage of 29,000 to 42,000 physicians and that by 2030 this shortage may expand to 40,000 to 122,000. Because the United States is not self-sufficient in producing enough health workers to meet its needs, it recruits health workers from some of the poorest and sickest countries in the world, causing them even more challenges in caring for the health of their people. In fact, a Gates Foundation study revealed that the number one reason for the loss of African medical school professors was immigration, and the United States was the number one destination.
The 2016 WHO report on a Global Strategy on Human Resources for Health highlighted global gaps in the public and global health workforce, and set concrete goals for countries to coordinate and implement an intersectoral health workforce agenda (“Global Strategy on Human Resources for Health: Workforce 2030,” 2016). Although nearly 20 million health workers were short worldwide, critical shortages were equally seen in filled public health positions in the United States and beyond (Sellers et al., 2019).
In response to the COVID-19 pandemic, which especially places a strain on the emergency and critical care workforce in heavily hit areas, facilities, states, and countries have taken action to rapidly expand the health workforce. For example, Italy, the United Kingdom, and New York State have accelerated the graduation of senior medical students, whereas, in many parts of the world, retired clinicians have been called back to duty to support the growing workforce shortages at the frontlines. Furthermore, especially with critical shortages in PPE, formal recommendations have been put out to protect health care workers (“Coronavirus Disease (COVID-19) Technical Guidance: Infection Prevention and Control/WASH,” n.d.; Haines et al., 2020; “Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19,” 2020). Public health systems everywhere had clearly not planned adequately to protect public health or clinical workers in a pandemic. For example, the U.S. strategic stockpile of PPE was soon exhausted and lack of PPE became a tension point. In addition, most health workers required training in PPE donning, doffing, and use. Tens of thousands of health workers were exposed to and contracted COVID worldwide. The pandemic also revealed a deep flaw in the U.S. health worker employment systems. Due to the canceling of elective surgeries and scans which cross-subsidize much of the rest of health care, health facilities had to lay off tens of thousands of health workers when arguably they were needed the most. The U.S. public health systems did not have the flexibility to pay these workers’ salaries or move them to essential public health rales such as public education and contract tracing. Some states, such as California, did start programs early in the epidemic to train laid-off service workers to be auxiliary health workers.
After the peak of the pandemic, states will need to hire and train tens of thousands of contact tracers. In addition, all primary, secondary, and tertiary care professionals will require foundational training and guidance on pandemic preparedness and ongoing measures for post-COVID-19 recovery. States will need to invest heavily in training and bonding more public health and clinical health workers. This can be accomplished in an era of tight budgets by aligning public secondary and tertiary budgets, which will open jobs in the state. Most states have thousands of open health jobs in the states so public funds should be shifted to those educational programs. Most states have few open jobs in the arts, foreign languages, history, or philosophy, so public funding should be reduced to those programs.
Service 9: Evaluate Effectiveness, Accessibility, and Quality of Personal and Population-Based Health Services
Prior to the pandemic, the United States had excellent quality improvement and evaluation systems in place for health facilities and public health programs. The CDC and WHO have been actively responding to the pandemic by disseminating preparedness checklists and guidelines to improve the safety and delivery of health services in suspected or confirmed COVID-19 patients, as well as mitigating further community spread. Quality improvement measures have gradually been implemented as lessons are drawn from the rapid expansion of the body of COVID-19-related clinical and public health knowledge, and the need to accelerate clinical trials, off-label treatments, and health care innovations. These go alongside the need to critically and wisely allocate resources in an ethical manner, especially when life-saving treatment modalities (e.g., ventilators) become scarce. Opportunities were missed at the state and national levels to pool COVID-19 patient electronic medical record data for quality assurance purposes.
After the pandemic, it will be vital to ensure that population-based health services are equipped with the knowledge and skills to assist patients in COVID-19 recovery. Standardized mechanisms for conducting evaluations among community health institutions and organizations ought to be developed, and electronic medical systems to be strengthened to better track patient outcomes in real time and to understand gaps in knowledge and skills of health workers. In addition, the expansion of rehabilitation services—in person and through telerehabilitation—is necessary to manage post-ICU and post-comatose COVID-19 survivors as well as those whose non-COVID-19 conditions (e.g., cardiovascular events) have been complicated by COVID-19. Such post-hospital, population-level health services require critical monitoring to ensure its effectiveness and maintain acceptable clinical outcomes and gradually introduce quality improvement interventions as our knowledge on and familiarity with home-based health services increases.
Service 10: Research for New Insights and Innovative Solutions to Health Problems
Prior to the pandemic, lessons and insights were conventionally shared through conferences and peer-reviewed journals. In response to the large infectious disease burden and regular Ebola outbreaks in sub-Saharan Africa, the WHO’s African Health Monitor served as an online data platform for the analysis and synthesis of information to support countries in establishing national or subnational health observatories.
Now, medical journals have struggled to speed up peer review and have published hundreds of non-peer-reviewed “preprints.” Many journals with paywalls made their COVID content freely accessible. Social media, especially Facebook and Twitter, have emerged as the preferred way for health professionals to access the latest learnings and news of COVID-19. Collaboration has occurred faster and on a broader scale than seen previously. Many initiatives, such as the MIT COVID-19 Hackathon, have leveraged crowdsourcing and hackathon platforms to develop new, low-cost technologies such as open-source ventilators and three-dimensional (3D) printed masks, navigate through resource-constrained environments, and safely reuse disposable mask or use other materials off-label. The SARS-CoV-2 genome was mapped and publicly shared in January. The U.S. government, the Coalition for Epidemic Preparedness Innovations (CEPI), the Gates Foundations, and other funders made billions of dollars available for the development of COVID-19 vaccines, treatments, and other innovations. Misinformation is being combated aggressively by health care and public health professionals alike, whereas innovative communication projects attempt to reach indigenous populations and rural communities living in the last mile in sub-Saharan Africa, efforts supported by the Africa CDC and the Co-Creation Hub.
After the pandemic, many innovations such as some of the low-cost ventilators and improved PPE will continue to be used and will be integrated into public health and clinical practice. The public health community can advocate for journals to make all their content freely accessible. Ways can be sought to make the large-scale collaboration sustainable as it enables the leveraging of the resources of more institutions. Drone delivery platforms can be leveraged to reach hard-to-reach communities and populations, which may aid in the delivery of essential medicines, pocket imaging modalities, and other supplies. We propose a “Grand Challenges in Public Health Preparedness,” not only to prevent similar global events in the future, but also to mitigate the impact of more localized infectious disease outbreaks and increasing chronic disease in countries with already fragile health systems. However, most crucially, national research budgets must be aligned with needs-based priorities and in-country capacity, rather than directed by earmarked funding or political agendas. The public health community must advocate for continued high-level funding of public health research and innovations, or risk a dramatic decrease in funding as soon as the COVID-19 pandemic is under control.
Discussion
The world’s response to the COVID-19 pandemic has been widely variable, resulting in differential outcomes in terms of the numbers of confirmed cases per capita and preliminary case fatality rates. In Southeast Asia, lessons from the 2003 SARS outbreak and the 2012 MERS outbreak led to swift and effective actions taken by, for example, Taiwan, Hong Kong, Singapore, and New Zealand, where cases have been kept to a minimum, despite frequent travel to and from China. Similarly, South Korea and Japan, although heavily affected by the early number of positive cases, were quick to flatten the curve of the outbreak. Cultural habits, such as wearing masks in public and more disciplined hygiene measures, have been critical to limit the further spread. In addition, high-risk travelers were promptly detected upon entering the countries, through questioning and temperature measurements at the points of entry.
Meanwhile, the challenges underlying the U.S. response raise four main questions:
How can funding for public health be increased?
How can public health vacancies be filled?
How can public health be made politics-proof?
How can public health measures be implemented in fiercely independent populations?
Public Health Funding
It is estimated that the U.S. public health system is underfunded by US$4.5 billion annually. The best way to increase this funding is through expanding state and local sin taxes beyond tobacco and alcohol to sugary drinks and junk food. For example, a one-cent per ounce tax on sugary drinks would generate US$13 billion in revenue in the United States. As an added bonus, the estimated decrease in sugary drink consumption and associated obesity, diabetes, heart disease, dementia, and cancer would save US$17 billion annually in health care costs. Of note, the state of West Virginia has financed its public medical school for decades through a sugary drink tax. Given that the COVID-19 pandemic and the previous SARS, MERS, and swine flu epidemics were driven by international travel, another option is to raise taxes on international air travel and invest the revenues in outbreak response. A relatively small per-ticket tax would not restrict international travel and would raise hundreds of millions of dollars to help mitigate the public health impacts of such travel.
Filling Vacant Public Health Positions
To fill the 20% vacancies in funded public health positions, public health recruiters should leverage the large community of U.S.-based global health practitioners. Due to increases in local public health capacity, many low- and middle-income countries have dramatically decreased child and maternal mortality rates, and are “graduating” from U.S. aid. This is freeing up U.S.-based global health practitioners to be employed to use their valuable skills in the U.S. public health. In addition, U.S. schools of public health should be expanded to produce more needed public health graduates.
Making Public Health Politics-Proof
The U.S. COVID-19 epidemic saw unprecedented politicization of a public health disaster. Prominent people associated with one political party called the outbreak a “hoax” early in the pandemic and claimed another political party was exaggerating the effects of the outbreak for political gain. Public health professionals usually justify public health investments and interventions based on the assumption that human health is a top priority and support their recommendations with epidemiological statistics, human rights, and the prevention of suffering. However, to reach and persuade all audiences, all public health arguments must include economic justifications, including return on investment, costs saved, impact on businesses and the economy, and impact on individual privacy and freedoms. Another suggestion is to strengthen the ability of the states to act collectively when the federal government declines to. This can be achieved by strengthening the public health staffing and capacity of the National Governors Association which includes the governors of all the 55 states, territories, and commonwealths. A robust centralized, yet state-controlled, public health capacity will allow the governors to act collectively to buy equipment and drugs, collect data (such as data on stocks of emerging therapies to inform treatment guidelines), and enforce uniform public health policies.
Public Health in Independence-Oriented Populations
Americans are known for being fiercely independent and often valuing privacy and individual rights over collective rights. Yet, often in public health, especially in disease outbreaks, actions must be taken which temporarily infringe on rights and privacy. As a result, public health communications in the United States must be created to address these concerns. Public health measures must be justified in terms that align with the Independence value set. For example, lockdowns should be supported with the economic argument that one hard lockdown or shelter-in-place will have a lower long-term economic impact than months or years of lower-level interventions, such as social distancing. It is critical to communicate directly with Independence-focused populations and provide public health tools to these populations via trusted sources. An excellent example of communicating with communities that are resisting public health measures is the WHO’s addressing of polio vaccine avoiding in orthodox Muslim communities. The global polio eradication campaign originally struggled with Muslim community resistance in Nigeria and Pakistan to vaccination due to rumors that the vaccine supposedly contained HIV or infertility agents aimed at decreasing Muslim populations. The WHO was able to overcome this through producing the vaccine in Indonesia, a Muslim-majority country, in a process overseen by respected imams. Within most religious, ethnic, political, ideologic, and geographic communities that are resistant to public health interventions, there are trusted leaders and institutions that are willing to share messages of support to public health measures. Similarly, mobile phone–based infectious disease contact tracing apps should be created and disseminated by institutions trusted by these communities. For example, a contact tracing app created by the League of United Latin American Citizens, the largest, oldest, and most active Latino rights organization in the United States, is more likely to be trusted and used by Latinos than one from the federal government. Third, it is vital to recognize that a basic understanding of public health measures is essential to good citizenship and to integrate it into K–12 public education. This would parallel required “citizenship” content in public education as well as public safety education such as school-based active shooter drills and fire drills. Fourth, telemedicine, digital health technologies, and internet-based virtual operations for work and education have become increasingly pervasive in our daily lives in response to social distancing and lockdown measures. This raises the need to invest in more widespread and high-speed connectivity, accessible to all, as well as the availability and distribution of devices to be used for these purposes. Not doing so will further increase already existing large inequalities in the United States and around the world, which is now visibly emphasized. Such measures can support emergency responses by leveraging mobile phone alerts and more efficiently disseminating public health information. This emphasizes the critical role the information technology sector can play in the public health and health care arena.
Finally, the pandemic has exacerbated the need for timely accurate data made available to all. This item is of such importance that it should either be added as an 11th essential public health service or added as an important component of the monitoring, diagnosis, and informing essential services.
Conclusion
The COVID-19 pandemic starkly revealed the cracks in the U.S. public health system. Improvements can be made at the federal, state, and local level across all 10 domains of public health to more efficiently contain current and future infectious outbreaks and rebuild the public health system beyond the COVID-19 pandemic. Such improvements will also help the United States address its growing public health challenges with cancer, aging, dementia, and obesity, and its related diseases of diabetes, heart disease, and kidney disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.