
Abstract
This study uses the constellation approach of transition theory as a theoretical framework to depict the ways in which facilitators and barriers in police system's structure, culture, and practice interact to shape police response to persons with mental illnesses (PWMIs). The study utilizes the framework method to analyze 57 in-depth interviews with police officers in Texas. Using a hybrid approach of inductive and deductive thematic analysis, we develop a matrix of four quadrants characterizing the constellation of mental health service provision by police: (1) structural barriers (deficits in resources, unsuccessful collaboration, lack of training), (2) structural facilitators (crisis intervention teams, informal cross-disciplinary collaborations, technology), (3) cultural barriers (role conflict, perceived inability to help, stigma), and (4) cultural facilitators (the police mission ‘to serve and protect’, improving police public image, managerial support). The study ends with recommendations for the scaling up of police mental health service provision to PWMIs.
Keywords
Introduction
Mental illnesses represent one of the top causes of disability in the U.S., with nearly one in five adults (21%, 52.9 million) suffering from some type of diagnosable mental disorder (National Institute of Mental Health, 2022). In the face of these mounting numbers, especially during the COVID-19 pandemic (e.g., Lee et al., 2021), police have become a pivotal player in providing mental health services to individuals experiencing mental health emergencies (Watson et al., 2021).
The central role of police in servicing people with mental illnesses (hereafter, PWMIs) is not new and has been historically controversial (Cotton & Coleman, 2010). Early works by Buss (1995) and Fogarty (1989) have noted how deinstitutionalization laws and policies in the early 1960s created challenges in balancing the law enforcement and the social service functions of policing. In the last decade, twenty-first Century Policing reforms, such as developing procedural justice training and implementing specialized mental health response teams, have anchored police as the primary non-medical resource for mental health services in communities (Hirschi, 2022).
The notion that mental health response is a core police duty (Sced, 2006) is unsurprising. After all, police officers are street level Bureaucrats (SLBs) who stand at the frontlines of public service (Lipsky, 1971), and as such, although not mental health experts, they are also the frontline response to PWMIs (Alpert, 2015). According to Livingston (2016), police are involved in the care of one-third of people with mental illnesses in the United States.
With that said, perhaps more than any other group of SLBs, police officers possess a wide discretional freedom (Bittner, 1970) to make decisions that impact the delivery of public policies to the citizenry (Lipsky, 1971). In the case of mental health calls, police interactions with PWMIs are complex in nature, and the decisions that officers make, sometimes in split seconds, can have a long-term impact on PWMIs’ lives (Lockwood et al., 2021).
For example, scholars found that PWMIs’ encounters with police increase their likelihood of being arrested and entangled in the legal system, even if they are not committing a crime (e.g., Watson et al., 2021). Others have found that such encounters have more potential to become violent and end in tragic injuries or deaths (e.g., Reuland et al., 2009). The statistics here are outdated and inconsistent, but the most recent available data suggests that 25% of all fatal police shootings in the U.S. involve PWMIs (Kindy & Elliott, 2015).
Recently, publicized and controversial police use-of-force incidents involving PWMIs have placed a heightened focus on police response to mental health calls, questioning officers’ ability to handle situations involving such individuals (Tully & Smith, 2015) and calling for a reform in police service provisions (Watson et al., 2021). As the responsibility for mental health concerns continues to shift towards law enforcement, it becomes crucial to study the system of police response to PWMIs and the factors that facilitate or inhibit its success.
In this study, we use transition theory, specifically the constellation approach described by van Raak (2010, 2016), as a theoretical framework to depict the interplay between structure, culture, and practice in police service provision to PWMIs. Specifically, we ask:
What factors hamper police service provision to PWMIs in terms of the dominant structure and culture of the policing system? What factors facilitate police service provision to PWMIs in terms of the dominant structure and culture of the policing system? Can identifying these barriers and facilitators provide a basis for developing effective strategies to scale up police service provision to PWMIs?
Identifying these factors is essential for facilitating a transition in the police service provision system. It would give police leaders and policymakers a better understanding of which barriers must be addressed and which pathways should be further explored.
Literature Review
Theoretical Framework: Understanding Constellations in Transition Theory
Transition theory emerged to explain why organizational changes occur and what processes drive them. Rotmans et al. (2001) define a transition as: “a gradual, continuous process of change where the structural character of a society (or a complex sub-system of society) transforms” (p.16). They posit that transitions result from complicated and persistent problems deeply rooted in societal systems (Rotmans et al., 2001). More specifically, the theory offers a theoretical framework from which transitions in complex systems are analyzed through fundamental changes in that system's dominant structure, culture, and practices (Loorbach & Rotmans, 2010).
According to transition theory, each societal system is made of a multitude of nested, competing, and complementing constellations (van Raak, 2016) that define and fulfill their role in the larger system (Wiertsema et al., 2021). Within a constellation, three elements: structure, culture, and practice (hereafter, SCP), continuously interact in a process that ultimately leads to a change in the system. Structure refers to institutional, physical, economic, and other arrangements that influence members’ behavior within a constellation (Pellekooren et al., 2022). Examples of structures include but are not limited to rules, regulations, and law (i.e., institutional), infrastructure, technologies, and resources (i.e., physical), finance, consumption, and production (i.e., economic) (Heemskerk, 2020).
Culture pertains to members’ shared norms, values, and perceptions within a constellation that shape actors’ perspectives on the structures and practices of the system (van der Ham et al., 2013). Finally, practice relates to the activities undertaken within a constellation, such as the daily routines and practices of the members involved in the system (Pellekooren et al., 2022; van der Ham et al., 2013). Simply stated, while structure emphasizes the ways actors organize the things they do, culture focuses on the ways actors think about the things they do and practice on what actors actually do (Motiwala & Ezezika, 2021).
In the “structure, culture, and practice triplet” (Loorbach & Rotmans, 2010), all three elements interact with and adapt to each other (Pellekooren et al., 2022) in a way that hampers and/or facilitates a change in the constellation(s). This may eventually lead to a long-term, fundamental transition within the entire system (Loorbach & Rotmans, 2010). The driving force behind these changes is usually the “actors” in the constellation and their collective sense of urgency for change (Wiertsema et al., 2021). According to Rotmans et al. (2001), these complex societal problems cannot be solved in the short term, and the changes needed to resolve them require long-term processes that last at least one generation.
Transition theory, specifically the SCP model within it, has been widely applied to a wide range of societal systems, such as agriculture, economics, and especially healthcare systems, to show how these elements operate within a constellation to induce system-wide change in organizations and improve overall service delivery. For example, Ebuenyi et al. (2020) explored barriers and pathways to the inclusion of persons with mental disabilities in educational programs. They found that barriers related to underlying structure and culture issues significantly impede the practices of inclusion of persons with mental or intellectual impairments into educational programs.
Similarly, van der Ham et al. (2013) differentiated between factors in the dominant SCP of a mental healthcare system that hamper or facilitate the integration of service user knowledge. Some of the significant hampering factors they identified include, at the structural level – the lack of mental health policy, legislation, and resources, and, at the cultural level – stigma and power differences between service providers and users. In terms of facilitating factors, they found that establishing inter-sectoral collaborations and adopting right-based approaches can enhance service user knowledge integration.
Moreover, studying the interface of organizational structure, culture, and practice in end-of-life care to people with intellectual disabilities, Grindrod & Rumbold (2017) reported the most significant relationship to be between culture and practice. They found that staff attitudes and beliefs towards persons with intellectual disabilities repeatedly informed the end-of-life care options (i.e., practices) that staff members offered to clients, despite the organizational governing policies (i.e., structure). They used their findings to develop an integrated service model to improve end-of-life capacity and capability for disabled clients. Wiertsema et al. (2021) also used SCP analysis to evaluate the barriers and facilitators associated with implementing an advanced rehabilitation model for trauma patients. They found that the structural level, specifically the communication structure, was a powerful facilitator in the successful implementation process of the model.
The “SCP Triplet” of Police Service Provision to PWMIs: A Constellation Perspective
Police systems, like other public bodies, can also be characterized in terms of multiple constellations of SCPs through which actors interact. Police officers are the key actors in the constellation whose actions influence and are influenced by every aspect of the structure, culture, and practices of the societal system (i.e., police) (Loorbach & Rotmans, 2010). These SCPs encompass the response models and daily routines in the provision of mental health services to PWMIs and are presented in Figure 1.

The interplay of structure, culture, and practice in the constellation of police service provision to PWMIs. Framework adapted from van Raak (2016).
Structural factors in the constellation of police service provision to PWMIs include but are not limited to federal and state mental health legislation, departmental policies and procedures regarding PWMIs, and any formal resource that either limits or facilitates the response of police officers to PWMIs. A few examples of structural issues are – departmental policies and procedures on taking custody and transporting PWMIs; state and federal laws governing incarceration (i.e., jail diversion strategies) or the sharing of medical information of PWMIs; and specific mental health training programs for police officers. The latter is of particular importance in the context of this study.
The literature points to training as a structural pathway as well as a barrier. On the one hand, studies have addressed lack of, or insufficient, training for police officers as a significant barrier to effective policing. For example, Fry et al. (2002) found that perceptions of inadequate training made officers feel unprepared, unconfident, and incompetent in their dealings with PWMIs. In addition, studies have found that a lack of mental health training can lead to officers’ negative attitudes and stigmatization towards PWMIs (e.g., Sheehan et al., 2016).
On the other hand, studies have recognized the facilitating impact of quality training. For example, Skogan (2022) argued that adopting clear and relevant training in problem-solving skills for officers (among other factors) has increased the quality of police operations. Similarly, Fry et al. (2002) found that incorporating communication skills training improved police response in mental health-related calls.
Cultural factors in the constellation include organizational and individual norms, values, and beliefs that shape the provision of policing services. Specific to mental illness, culture reflects the shared perceptions officers hold towards PWMIs and the in-place police structures and practices to respond to them.
For example, culture may involve mental illness stigma in policing (e.g., Edwards & Kotera, 2021), biased attitudes towards PWMIs that may lead to discrimination and fair treatment (e.g., Sheehan et al., 2016), and a negative opinion of police's function as a mental health service provider (e.g., Bailey et al., 2018). Together, these views create a strong occupational police culture that impacts how actors (i.e., officers) think and act.
In fact, such a view on the “sharedness” of police culture has been recently demonstrated in the final report to the president (President's Task Force on 21st Century Policing, 2015), which portrays police officers as a homogenous group confronting similar occupational pressures (Ingram et al., 2018).
However, it is important to note here that despite the consensus in the literature regarding the monolithic nature of police culture (e.g., Sierra-Arévalo, 2019), a (somewhat) competing school of thought points to its deep fragmentation, challenging the assumptions of a single uniform police culture (e.g., Cohen, 2018; Ingram et al., 2018; Paoline, 2003, 2004; Paoline & Terrill, 2005; Paoline et al., 2000). For example, Cohen (2018) found that fragmentation in police culture in terms of agency type, rank, and leadership style can either enhance or constrain police interagency collaboration.
Moreover, Paoline's (2004) extensive work on the relationship between police culture and officers’ behavior yielded a characterization of seven analytically distinct groups of officers, suggesting that police officers can be significantly different in how they manage aspects of their job. According to Paoline et al. (2000), the variation in police cultural orientations can diminish (and even dissolve) the occupational attitudes that are viewed as “collective” elements of police culture and, therefore, can cause a wide variation in the ways police cultures shape police practices (also: Ingram et al., 2013, 2018).
Lastly, factors related to practice in the constellation of police service provision to PWMIs reflect the actions undertaken by police officers – meaning, their actual behavior and performance at work (Pellekooren et al., 2022; van der Ham et al., 2013). This mainly refers to the officer-PWMI interaction but also to the interactions between officers and other players in the constellation. For example, power differentials between officers and their supervisors can impede service provision (Grindrod & Rumbold, 2017). Another example is cross-disciplinary collaboration practices between law enforcement and other professions during mental health-related calls that may inhibit or promote service provision to PWMIs.
Contemporary research on multidisciplinary collaboration regarding PWMIs has mainly focused on the development of crisis intervention teams (CIT) and other co-responder mental health teams models (e.g., mobile CITs, early response teams, crisis outreach, and support teams) (Bailey et al., 2018). On the positive side, research findings demonstrate that such collaborations promote interprofessional information sharing (Bailey et al., 2018) and increase the likelihood of diverting PWMIs from the criminal justice system to the care of the mental health and social services systems (Bailey et al., 2018).
On the negative side, studies point to uncertainty and ambiguity of role expectations and responsibilities as significant challenges in multidisciplinary response teams. Morabito et al. (2018) explain that paramedics and police officers have different views on PWMIs and best practices for mental health response. When responding to mental health calls, each professional group brings its backgrounds, priorities, and skill sets that may conflict with those of the other group (also Bailey et al., 2018).
The interplay between structure, culture, and practice is complex as they dynamically influence one another (Ebuenyi et al., 2020). Within a constellation, structure and culture serve as both enhancers and inhibitors of police officers’ practices involving PWMIs. For example, a change in structure, such as new legislation, will change how officers practice their work. Moreover, such change might influence a cultural shift in the way officers perceive PWMIs.
At the same time, officers’ perceptions of PWMIs (i.e., the culture) shape, and are shaped by, policies and regulations (i.e., the structure) concerning PWMIs which, in turn, guide the practices utilized by agencies (Kett, 2012). Lastly, even the practices of police influence both the structure and the culture of the constellation, and while all three elements depend on one another in a recursive relationship, they can also become competing autonomies in the face of a change (Octarra, 2018).
Today, police agencies in the U.S. face a growing demand for social intervention by police due to the scarcity of mental healthcare services in communities (Johansen et al., 2018). Therefore, a complex transition is needed in the police system's dominant structure, culture, and practices to accomplish an effective and sustainable reform of, or an institutional change in, police service delivery (Greig-Midlane, 2019b). The difference between the two, according to McMahon and Ericson (1984), is that reform is a new policy that attempts to change or redirect an existing policy, whereas institutional change results from adapting to the policy reform (Greig-Midlane, 2019b).
Nonetheless, a meaningful discussion about police reform must involve the application of the SCP model assumptions to policing systems. However, a search for empirical studies on the topic revealed a gap in the literature. While the SCP model has been extensively applied to several societal systems, mainly in health care, when it comes to police as a societal system, research utilizing the SCP framework is almost nonexistent.
A thorough review of the literature yielded two studies that explicitly used the SCP model in the context of police organizations. Greig-Midlane's (2019a, 2019b) works explored how institutional changes in the austerity era influenced reform and implementation of community policing in England. He found that while socio-economic and political changes have triggered various changes in police reform, some other features of policing culture have stayed relatively stable. Greig-Midlane's (2019a) analysis reveals a discursive struggle between reform and changes in the institutional structure, culture, and practice of neighborhood policing delivery.
The current study addresses this gap in the literature by exploring the constellation of police service provision to PWMIs through the lens of transition theory. We aim to identify barriers and facilitators in the organizational structure and culture of the police system and how they influence the practices that shape the delivery of services to PWMIs.
Methodology
Data Sources and Collection
The total sample for this study consisted of 57 law enforcement officers in Texas (n = 57). The choice of Texas as a focal state for this study makes sense because the Texas police system is one of the most fragmented police systems in the United States. Therefore, it serves as a good proxy for the overall high level of fragmentation in the U.S. American criminal justice system in general (Cohen, 2018).
We collected the data between November 2021 and July 2022 through semi-structured interviews, each lasting between 45 and 60 min. The interviews were conducted, recorded, and transcribed using Zoom. Immediately after each interview, the transcript was checked against the recording for accuracy. Transcription conventions outlined in Braun et al. (2016) were used in cases where the texts were unclear and to mark paralinguistic features of the interview that might be relevant for the analysis but were not said explicitly by the interviewees.
The interview questions were developed with the help of an experienced law enforcement professional, then pilot tested with two police officers. In the interviews, we focused on officers’ perceptions of PWMIs and the barriers and facilitators they experience when providing service during mental health-related calls.
The study employed a snowball sampling, in which police officers who volunteered to participate in the study also helped recruit future participants. Snowball sampling is one of the most commonly used strategies for sampling hard-to-reach populations (Rao et al., 2017), and policing scholars commonly agree that law enforcement officers are considered as such (i.e., Cohen & Cohen, 2021; Paoline, 2003). In the context of police, hard-to-reach population (also: “hard to track” and “hidden population”) means that officers are unlikely to participate in an interview with a non-police “outsider” unless the individual is vetted by “one of their own” (Cohen, 2018).
We realize that snowball sampling is not ideal and has limitations. Primarily, while it is an efficient method for gaining access to hidden populations (Rabe-Hemp, 2008), it is not beneficial in providing a representative sample. A possible limitation here is that the findings of this study, which was carried out in a single state in the U.S. (i.e., Texas), may be limited in terms of generalizability to a Metroplex environment in the South-Central region of the United States.
Moreover, the nonrandom nature of the data collection exposes our findings to a selection bias. Specifically, given our previous discussion of the multiple police subcultures in modern police organizations, our study is open to the criticism that police officers who volunteered to participate belong to the same police subculture or “personality” and are, therefore, biased from the outset.
However, Rao et al. (2017) explain that the composition of the final sample in snowball sampling is primarily influenced by the initial nonrandom choice of participants (i.e., the “first seed”). In this study, the “first seed” was recruited from a police training academy that provides training services to police officers from all over Texas. Overall, our results are based on 57 interviews collected from 22 different police agencies across Texas. Therefore, there are no data to suggest that the 57 participants in this study belong to the same police subculture.
In addition, our uniquely large number of interviews allowed us to achieve an appropriate theoretical saturation, a widely accepted measure in qualitative research to alleviate subjectivity (Braun & Clarke, 2006).
Despite these limitations, our study's findings are compelling. Exploring officers’ experiences with PWMIs through in-depth interviews provides a unique insight into the drivers and barriers of a pervasive societal concern that affects millions of citizens in the United States. The survey instrument alone could not have provided such a level of understanding (Rabe-Hemp, 2008). As Cohen and Arieli (2011) argue, the use of snowball sampling sometimes makes the difference between conducting a study and not conducting it at all.
Participants’ Demographics
Our interview sample consisted of 45 men and 12 women, which reflects the male-dominated nature of policing (Gaub & Holtfreter, 2022). Their age ranged from 25 to 58 years, with an average of 41.7 years. Regarding race, 86% were White (including White Hispanic), 8.7% were Black, and 5.3% were Asian. Participants’ highest completed level of education varied between high school (9.8%), some college (12.2%), undergraduate degree (47%), and master's degree (31%). As for their tenure in law enforcement, participants ranged from 3.5 to 34 years of seniority, with an average of 16.5 years. In addition, 18% of our interviewees hold executive-level ranks, 30% hold mid-level management ranks, and 52% are at the police officer rank.
Data Analysis Procedures
The data analysis for this study was based on the framework method, a common content analysis analytic approach in social policy research (Gale et al., 2013). A key feature of this method is that it enables a matrix-based presentation of qualitative data. The framework method was developed in the 1980s and is widely used in qualitative health research scholarship (e.g., Wiertsema et al., 2021) but only rarely in the public administration literature (e.g., Cluley et al., 2021).
Our approach to the coding process combined deductive and inductive analyses. The first step of the analysis started with open coding. Following Braun and Clarke's (2006) thematic analysis framework, we inductively analyzed the transcribed interviews using NVivo 12 software. The goal was to generally understand the system that constructed police response to mental health-related calls and to code every theme that might be relevant to it freely, without a priori expectations. This process yielded a list of initial codes, which were grouped into conceptual sub-themes in an iterative process until overarching themes emerged.
Next, we used van Raaks’ (2010, 2016) constellation approach to construct the analytical framework that guided our deductive analysis. In this step, codes were categorized first as either facilitators or barriers to the provision of service to PWMIs, and then as either structural or cultural level factors. We found that practices developed as a result or the cause of barriers and facilitators, and therefore they were analyzed within the categories of structure and culture and not separately.
The final framework consisted of 12 themes, clustered into four categories of facilitators and barriers at the structural and cultural levels. To ensure the rigor and credibility of the findings, a law enforcement expert, who served as an advisor throughout this project, helped review and refine the thematic map and the generated matrix. This validation method is commonly used in qualitative methods (Brough et al., 2016).
Results and Analysis
Barriers and Facilitators of Police Service Provision for PWMIs: A Constellation of Evidence
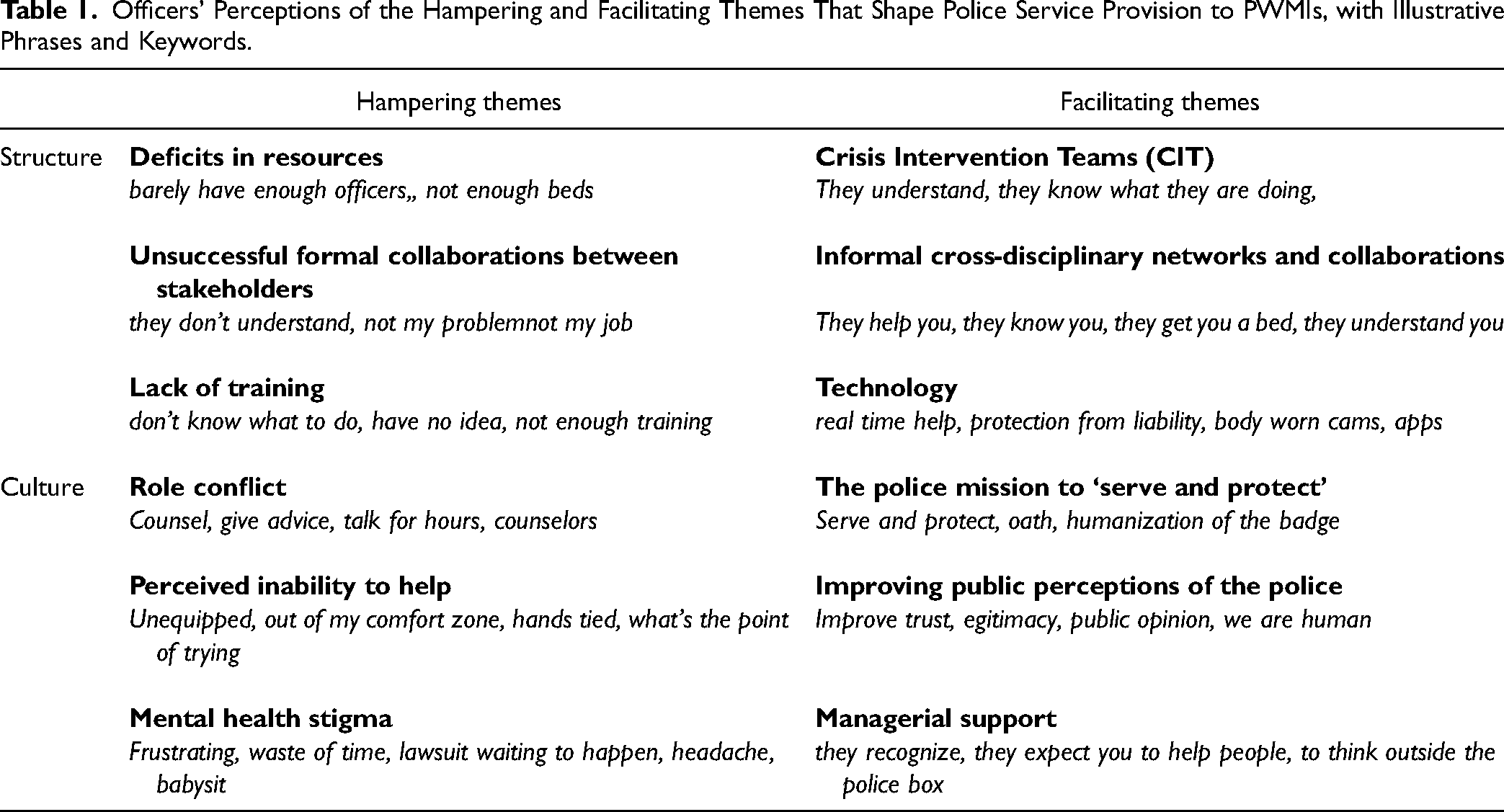
To answer our first two research questions, we explored themes of police structure and culture in the provision of services to PWMIs. In each category, themes are discussed as either barriers or facilitators in the constellation. Grouping our themes based on their function allows for an in-depth understanding of which factors in the constellation inhibit service provision for PWMIs and must be addressed and resolved, and which factors enhance service provision and should be further explored and developed (see Table 1).
Officers’ Perceptions of the Hampering and Facilitating Themes That Shape Police Service Provision to PWMIs, with Illustrative Phrases and Keywords.
Structure-Level Analysis
Hampering Themes
At the structural level, three overarching themes: deficits in resources, unsuccessful formal collaborations between stakeholders, and limited training, emerged as structural barriers to the provision of police services. The first barrier at the structural level relates to deficits in resources related to mental health. Two different structural aspects were mentioned by participants for this barrier: lack of internal resources and lack of external resources. Firstly, the lack of internal resources pertains to resources provided by the police departments themselves. Here, the main concern was inadequate staffing. “It's not realistic to think that we're going to have enough [officers]; we barely have enough officers to answer the regular calls, much less to go to every person experiencing a mental health issue” (interviewee #6).
Secondly, lack of external resources refers to resources provided by entities outside the police department, such as hospitals, community day programs, and other social services frequently utilized by PWMIs. The most critical barrier here was the perceived dysfunctionality of the U.S. mental health care system. The limited, or the lack thereof, availability of mental health care facilities, specifically, the unavailability of hospital beds, was unanimously pointed to as the biggest challenge to providing services to PWMIs. The following illustrates one of many stories we heard from our interviewees on their experiences with trying to locate a hospital that will accept a PWMI: “So we [officer and partner] spent the next five hours calling mental hospitals, one after the other, to check if there is a bed for her [PWMI]. I swear, we were turned down by at least ten hospitals until one said ‘ok,’ and we took her there” (interviewee #14).
In addition, officers also pointed to the lack of availability of mental health professionals, such as doctors and counselors, as a significant issue affecting their mental health care provision. “We use them [counselors] as a resource … they help us take care of the person … but come on, this is a Monday-Friday, eight to five job … it is not like we can call them at two in the morning … it's not enough” (interviewee #35).
Moreover, officers discussed how the unavailability and inaccessibility of mental health resources negatively influenced the ways in which they treated mental health patients. As this quote illustrates: “Unfortunately, because we don't have the staffing or funding we need … we can't provide a ‘softer’ approach to mental health; it has to be the strong and quick approach” (interviewee #4).
The “soft approach” the officer refers to pertains to conversing with the individuals and generally doing what counselors would do in these situations. The “strong and quick approach” pertains to arresting the individual or transporting them to a mental hospital.
The second theme addresses the unsuccessful (or lack of) collaboration between the police and other stakeholders in the mental healthcare system. In unsuccessful (formal) collaborations, officers felt that mental health professionals did not understand police officers’ job and their primary role as public safety – and not mental healthcare – providers.
For example, they reported that the medical staff expected them to sit in the hospital for hours, waiting for the PWMI they brought in to be treated. They also described having to deal with lengthy and cumbersome paperwork and inefficient hospital policies, such as rigid admission criteria. These factors, combined with the lack of resources mentioned above, contributed to officers’ negative perceptions of mental health service professionals and the creation of a strong sense of an “us versus them” approach. As one officer stated: “They don’t understand us, they don’t understand our job … they see us coming, and all they see is more work for them … well, I’m sorry, you think I like it? I’m not your problem here … this is not even my problem; it is the system's fault, not mine” (Interviewee #11).
Historical context is needed here to fully understand this quote, specifically the “fault” reference. One of the main criticisms raised by police is that they have become society's “fallback” plan. Meaning, when gaps in society's services occur (or when they fail) – they are the first to be blamed, especially when it comes to mental health care (also Wood et al., 2008). As exemplified in this quote: “We get dumped on with all kinds of mental issues, are we counselors now? Just because you can call us 24/7, and we will be there to fix it, does not mean we are equipped to deal with these types of problems … but then when something goes wrong, you [public] have someone to blame … easy” (Interviewee #31).
In some cases, officers felt that health professionals are failing not only the police but also PWMIs, their families, and even society. The following quote was given about a juvenile with mental illness: “He was homicidal, threatening to kill another student, and they [hospital] were going to let him go because they had no bed … there are so many kids in mental health crisis who don’t get the help they need … well, now my next call would be about this kid ‘offing’ himself or one of his classmates, and then who's fault is this? They let him go!” (Interviewee #27).
Lastly, the third barrier is officers’ limited training. Concerns over limited or inadequate training in mental health care were mentioned consistently during the interviews. One officer pointed out that cops are ill-equipped to deal with PWMIs: “Their [officers’] level of education on the topic is just not enough for them to make the right judgment or take the right action” (Interviewee #28).
Another elaborated: “Most times they [officers] have no idea what to do … so they'll just take the person to [mental hospital] and be done with it” (Interviewee #6).
Interestingly, officers strongly agreed that police had made good progress regarding mental health training and that there is a heightened awareness of its importance. However, although they felt that mental health training is much more available to officers today than before, it is “still not enough.” In essence, the overtone message of this structural barrier is that police officers are just not meant to provide mental health care because they are not part of the medical profession. As one officer explained: “Even though we do a lot of training … there is still so much unknown when it comes to mental health. We are not doctors or counselors … honestly, I don't know if it's even a question of more training, I don't know if there's even right amount of training you can give officers to make them mental health care experts … it is just not our field” (Interviewee #35).
Facilitating Themes
The structural-level facilitating themes of service provision to PWMIs include CIT, cross-disciplinary networks and collaborations, and technology. First, as previously explained, CIT is an innovative police-based response that represents a paradigm shift from the traditional policing model to one that includes a social service component (Morabito et al., 2013). Some models of CIT include certified police officers who received specialized training in mental illnesses, while others include mental health professionals as part of the team.
Our participants were strikingly unanimous in the view that CIT is a critical facilitator in the provision of service to PWMIs. They believed it increased their mental health knowledge and skills, making their interaction with PWMIs safer and less problematic. In addition, they felt that CIT decreased the time spent on mental health-related calls and their overall workloads.
A repeated theme here was that with CIT, PWMIs are treated by people “who actually know what they are doing.” Contrary to their perceptions of the unsuccessful formal collaborations with other mental health providers mentioned earlier in this analysis, when it came to CIT, officers viewed their working relationship with these professionals as functional and invaluable to PWMIs’ outcomes. One officer described how CIT advances the provision of services to PWMIs: “They [CIT] show up … wearing just a polo T-shirt … in unmarked car, so it's a very soft approach …. we work well together [officers and mental health professionals] because we meet weekly and talk about how to make it better and more efficient to them [PWMIs] … it's a big step … having somebody on the scene that can actually understand these people and help officers get these calls right” (Interviewee #37).
It is important to note that while all officers viewed CIT as a vital facilitator of police response to PWMIs, not all had access to it. For example, officers working for smaller departments with less access to mental health resources believed that CIT is one of the most critical resources they are missing to improve their service delivery to PWMIs. For example, this officer stated: “They [bigger agencies] have the luxury of having these specialized teams on the streets … they can afford having teams that only deal with mental health crises, and it's a big help, you know, we don’t have that” (interviewee #4).
Second, police officers stated that their informal collaborations with stakeholders, such as advocacy groups and faith-based and community organizations, played an important role in police service provision to PWMIs. Specifically, they felt that such informal ties have made them more efficient in locating resources and services for PWMIs. An officer working in the ER as a secondary employment provided insight into how such informal relationships develop: “I developed close relationships with them [hospital medical staff] … they help me whenever I’m dealing with people in mental health crises. Those informal relationships bridge the gap between us [law enforcement and mental health professionals] … now that they know us, they become part of us” (interviewee #43).
Another officer said that it is an advantage to make informal connections because: “When they know you, they get you the [hospital] bed that you can’t get, they have more influence … those relationships, man, they are everything” (interviewee #37).
Moreover, officers attributed their successful outcomes, for example, providing PWMIs with the appropriate intervention rather than sending them to jail, to the informal networks they have established with mental health service providers: “We have fantastic relationships with them [advocacy group], we can call them at any time, even after midnight, and they’ll come … He [volunteer] came in, talked to her [PWMI], he convinced her to get help, and I didn’t need to take her to jail … he literally saved the day for us all” (interviewee #36).
Lastly, the role of technology in facilitating police service provision also came up as a leading theme in the interviews. For example, officers believed body-worn cameras are a positive technological advancement in policing that protects them from liability, especially when responding to mental health calls. One officer described their experience testifying in a case that involved a PWMI: “They pulled the video footage of my body cam …. it just proved how bipolar she was … thank God it was there … all recorded … so there was no question of whether or not I behaved appropriately” (Interviewee #13).
Additionally, officers noted that mobile app-based information on mental health care is on the rise, significantly improving police service provision. Such apps gave officers comprehensive and reliable information on various social services available around their geographic location. For example, a commonly reported benefit was being able to quickly query about open homeless shelters in the area. Others have mentioned being able to connect with local volunteers from advocacy groups in real time; such volunteers would arrive at the scene and take care of the PWMI, relieving the officers of their other duties. One caveat to these helpful tools – that can also be related to the limited training theme – was mentioned by this executive: “The problem is that most officers in the street do not even know about this app, or what other resources they have at their disposal when it comes to mental health … they need to be educated about these things” (Interviewee #13).
Culture-Level Analysis
Hampering Themes
At the cultural level, three hampering themes explained the limitations in police service provision to PWMIs: role conflict, perceived inability to help, and the impact of mental health stigma. First, role conflict was one of the strongest themes in the interviews. Officers repetitively described the conflict between their criminal justice and social service roles when responding to mental health-related calls. High role conflict was detected mainly when the nature of the call was non-criminal, and the proper intervention required the officer to assume the role of a counselor and help individuals with mental recovery. The following quotes, made by two officers, illustrate the counseling aspect of the police officer's job: “We counsel, oh my gosh, who would have thought we would be doing so much counseling in this job?” (Interviewee #37).
“Sometimes you just sit there, talking with somebody, listening … for hours … giving advice, convincing them to get help … what else can I do? I’m not gonna take him to jail; he's not dangerous to anyone; he just needs someone to talk to” (Interviewee #17).
The literature commonly recognizes role conflict as a significant stressor (Balenovich et al., 2008) that develops due to competing expectations between the different roles a person is expected to undertake but cannot fulfill (Cain, 1968). In the case of police officers, the role conflict was perceived highly negatively as officers rejected their assumed role as social service providers. They argued that counseling and other mental health services (e.g., transporting PWMIs to mental hospitals) are not (and should not be) part of their job. The following officers asked: “Are we police officers or are we counselors? Because let me tell you, I don't know counselors that work 24/7 … and if we are [counselors], then we are the worst paid counselors in the world” (Interviewee #18).
A related theme, perceptions of inability to help, emerged as another significant barrier to police service provision to PWMIs. Interestingly, perceived inability to help is a well-researched phenomenon in the social welfare literature that is hardly mentioned in policing research. Nevertheless, our data revealed a robust sense of inability to help PWMIs through statements such as “feeling unequipped,” “out of my comfort zone,” and “working with my hands tied.” Notably, these sentiments were strongly reflected in stories involving juveniles with mental illnesses. For example, one officer gave the following example about dealing with a juvenile in a mental health crisis: “This young adult runs around naked in the neighborhood scaring people … there's not much I can do … I'm not a psychiatrist … I can detain him and now burden his already struggling parents with all this bureaucracy … you want to help so bad, but there's nothing you can do but stand there and watch them cry … it's very frustrating” (Interviewee #11).
Moreover, the belief that PWMIs are not improving by their service (or the lack thereof) contributed to officers’ already intense feelings of organizational burnout and cynicism that highly characterize the police occupational culture (Murad et al., 2021; Vinzant, 1998). This sentiment is well illustrated in the following quote: “I can spend hours trying to convince them to get counseling, go into detox, do something … but if no one follows up with them, tomorrow I will be at the same address, answering another call. Only maybe this time, someone got hurt … makes you wonder what's even the point of trying?” (Interviewee #5).
Lastly, we identified the negative stigma associated with mental health-related calls as another inhibitor to PWMIs’ police response. Such calls were described by officers as “frustrating,” “waste of time,” and “a lawsuit waiting to happen.” One participant explained how the fear of liability influences officers’ perceptions of PWMIs: “If I say, ‘okay, this person is not a criminal,’ ‘doesn't belong in jail,’ ‘I'm not going to arrest him, I'll just let him be.’ What if the next day, he either commits suicide or some act of violence against someone? Now because you left him there … now you are liable … man, no officer wants to deal with that … I don't need this headache” (Interviewee #51).
Moreover, the gravity of the time invested in mental health assistance calls also seems to shape officers’ perspective on PWMIs, as illustrated in the following quote: “When you get the [mental health] call – you know it – you're done for the night … you're going to get stuck babysitting someone until a bed opens up … you [researcher] need to understand, this weights on the officer … now that officer can't complete their nightly checks, their reports … they can't get their real job done. No wonder everyone is dreading these calls” (Interviewee #48).
Variations of the verb-stem “babysit” came up repeatedly throughout the interviews, echoing the sentiment of the previously mentioned themes – role conflict and inability to help. However, it also (negatively) compared PWMIs to incapable children needing a non-complex service – babysitting – a service that does not belong to the “real work” of police.
This finding aligns with Hackman and Oldham's (1976) classic job characteristics theory, which argues that when employees do not feel task significance (i.e., that their work is not making a difference in someone else's life), they are more likely to develop negative job attitudes. Similarly, the stigma associated with the tasks of mental health assistance calls (i.e., transporting, counseling, and babysitting) diminished officers’ task significance and negatively affected PWMIs. As explained in the following quotes: “Sometimes it makes you want to look the other way … you're thinking, oh shit, it's a mental call, let me take that burglary call instead because I don't want to sit in the hospital for five hours” (Interviewee #27).
“I'll be honest, it can affect officer's decision making about the person … they might try and find a reason to say, ‘I can't help you' just so they don't get stuck with it for their entire shift” (Interviewee #36).
Facilitating Themes
Three facilitating themes were identified as culture-related factors that serve as pathways to enhance police service provision to PWMIs: the police mission ‘to serve and protect,' improving public perceptions of the police, and officers’ perceptions of management support. First, police culture is deeply entrenched in the ethos and values derived from the duty to serve and protect. When asked about their motivation to help PWMIs, officers immediately avowed their oath “to serve and protect” the public. Rutgers (2010) describes the “oath of office” as the ultimate mean to establish the public servant's moral commitment to the citizenry. In policing, the oath officers take when they are sworn-in also qualifies their testimony to count as evidence in the courtroom (Rutgers, 2010); hence, it bears more than a symbolic meaning.
Here, again, officers described a clash between two competing beliefs. The belief that providing mental health care is not their job, and the belief that they carry the duty to serve and protect all members of society. Interestingly, the definition of what it means “to serve and protect” expanded beyond the traditional law enforcement role of “catching bad people” – to encompass social service role themes such as “caring for humans” and “being fair and respectful to people.” One officer explained the meaning of the ‘serve and protect' oath in the following way: “We took an oath to serve and protect the community, it means that everything that goes on in our community is part of our job … if someone is not right in their mind – it is our job to protect their well-being as well” (Interviewee #36).
A second emerging theme was public perceptions of the police. Police officers expressed high interest in improving the image of police with the community. One valuable way to facilitate a positive change in police–public relations is through “humanization of the badge,” which, to them, meant providing social welfare-type of services, even those perceived as extending beyond the boundaries of their job, such as the provision of mental healthcare.
Interestingly, officers’ awareness of the current hostile public scrutiny towards police induced a desire to leave PWMIs and their families with a positive impression of police. This desire seemed to counteract previous themes such as officers’ perceptions of role conflict (i.e., “not our job”) and the stigmatization associated with mental health-related calls (i.e., “getting stuck babysitting”). This quote from an officer who helped the family of a PWMI in a crisis to find her medications illustrates this effect: “Is finding her medications part of my job? Probably not … but maybe now they will appreciate the police just a little bit more … because one [officer] did something out of the ordinary for their daughter … who knows, maybe it'll open their mind that we are not that terrible” (Interviewee #1).
Another officer talked about a recent experience he had helping someone going through a mental health emergency: “When we are doing these things [social welfare type of activities], it just shows that officers can have compassion … we're not robots, we are human … maybe she'll change her opinion of the police, I don't know” (Interviewee #47).
Our last facilitating theme, officers’ perceptions of their management, pertained to how the agency's leaders viewed the idea of the provision of mental health services by police. When officers felt their leaders embraced the notion that policing is an extension of society's mental healthcare system, they were more willing to accept it themselves. One officer said: “Our chief says: ‘don’t be cops, be humans … go find opportunities to help someone in the community’ … it means a lot to hear that … it tells you that it is okay to spend time on a call helping someone that is having a mental crisis” (Interviewee #41).
Interviewees also mentioned the practice of recognizing officers for providing services that are not considered traditional police work: “They [command staff] expect you to think outside the law enforcement box … recognition for these kinds of acts is huge in our department” (Interviewee #3).
This finding aligns with the broader literature, which commonly agrees that the degree of organizational and managerial support perceived by employees is positively associated with organizational commitment and involvement (e.g., Dick, 2011).
These last two themes reflect the continuous efforts to reconceptualize policing in the twenty-first century. The police profession is under tremendous pressure to increase its legitimacy and strengthen its relationship with the citizenry. As a result, police tasks are shifting towards more complex, non-routine social intervention activities. This was also evident in the report of the task force on twenty-first Century Policing (2015), which presented recommendations for aligning law enforcement organizations with the expansion in the scope of their responsibilities.
Our findings that police officers and their managers are concerned with improving police public image demonstrate an understanding of this paradigm shift and an acknowledgment of the need for multi-faceted police skills, capacities, and activities.
Towards Scaling Up Police Service Provision to PWMIs: Recommendations for Practice
In this section, we answer our last research question of how identifying barriers and facilitators can provide a basis for developing effective strategies that will enable the scaling up of police service provision to PWMIs. Informed by our research findings, we offer insights into the challenges and pathways for facilitating transition in the PWMI-police service delivery system and recommendations for practice. Figure 2 presents a constellation view summarizing our findings and recommendations.
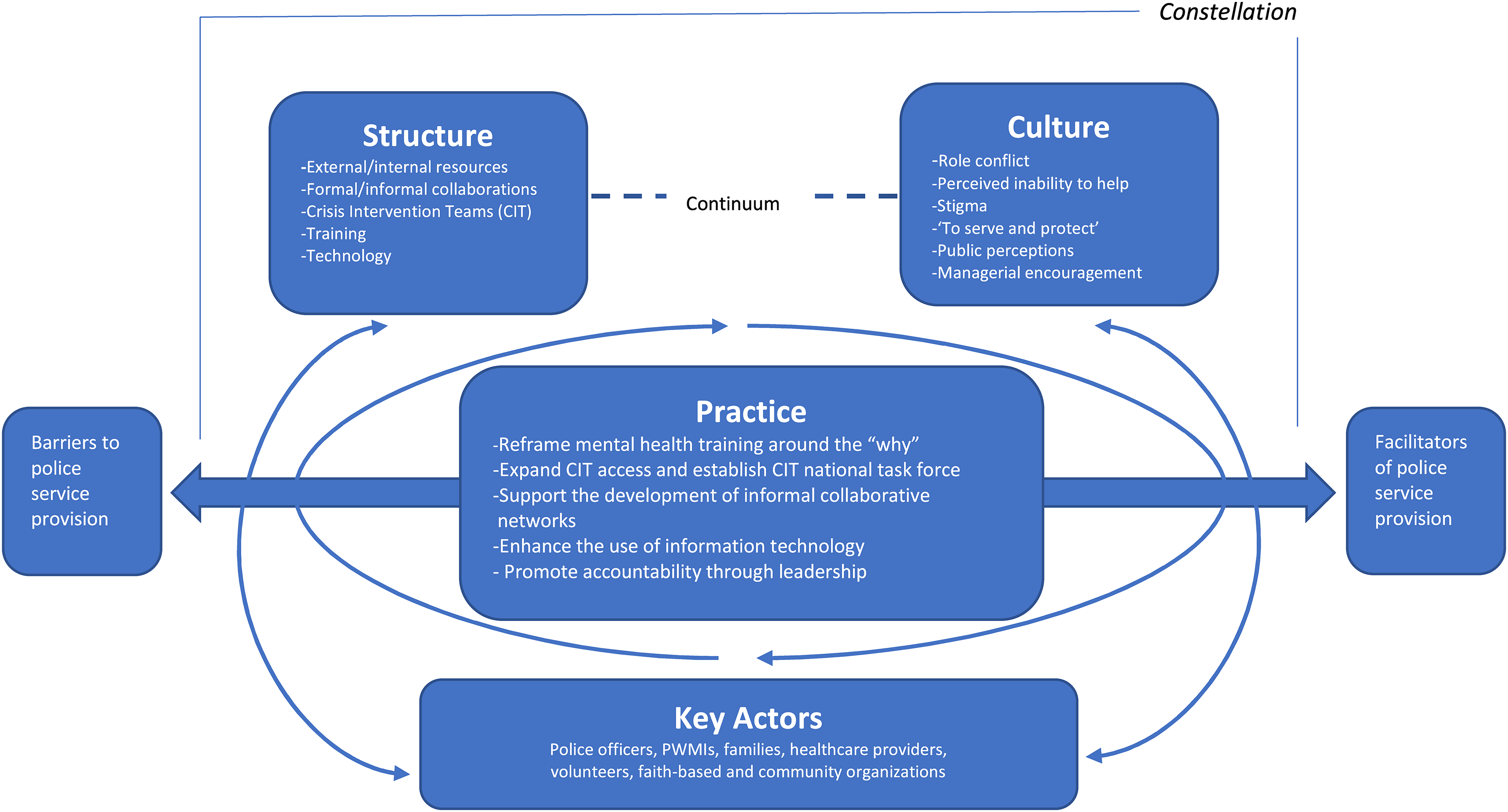
The SCP triplet of police service provision to PWMIs: A constellation of evidence and recommendations. Framework adapted from van Raak (2016).
It is important to note that, just as with any constellation where elements interact with and affect one another, the recommendations presented here are intertwined and have no clear starting point.
Reframe Mental Health Training (MHT) Around the “why”
A major finding in our study is that officers feel unequipped when responding to PWMIs not only because they lack training, but mostly because they do not perceive the provision of mental health services to be part of the police job. We are less than optimistic that simply increasing the time assigned to MHT would bring a change in that perspective.
Training relevancy is key here (Cohen, 2021). To build an effective and sustainable capacity for mental health response, police MHT should be reframed to emphasize not only “how to respond to PWMIs” but also “why we serve PWMIs.” Our study revealed two strong motivations that facilitate police-PWMIs interaction and can answer “the why” – the desire to serve and protect and the need to improve police public image.
Hence, police should design MHT programs that emphasize these motivations and teach officers how police intervention in mental health issues (and social issues in general) is relevant to their job and can be conducive to their professional motives and goals. In other words, how servicing PWMIs conforms to the ‘to serve and protect’ police mission and can positively change police–community relationships.
Expand CIT Access and Establish CIT National Task Force
Our results support previous findings that officers view CIT as a facilitator of mental health service provision to PWMIs. Interestingly, although CIT is a police innovation with a social service undertone, officers still viewed it as favorable. They firmly believed that CIT increases the safety of those involved in mental health calls and decreases officers’ workload.
However, despite the unanimous support for CIT among officers, our findings revealed a significant discrepancy in the availability of CIT-related resources across police agencies. While some heavily relied on it, others had no access to it at all. This also means that in areas with no access to CIT (mostly rural or small urban settings), PWMIs do not receive mental health care services supported by such teams.
This is a critical gap for policymakers and police leaders to address. If officers believe that CIT improves service provision to PWMI, they should be given more opportunities to practice it. In addition, a national task force should be established to examine how principles of CIT models can be implemented – and mandated – in police agencies in all geographic settings.
Support the Development of Informal Collaborative Networks
Our finding that officers perceive informal partnerships as critical for successful engagement in mental health-related calls contributes to the growing body of evidence on the positive impact of informal collaborations on police job outcomes (e.g., Cohen & Cohen, 2021). If informal collaborative networks are a promising strategy for enhancing service provision to PWMIs, more efforts should be invested in allowing officers to develop them.
Police leaders can improve mental health response by creating opportunities for their officers to form and expand cross-disciplinary partnerships through avenues such as joint training, open forums, and lunch-and-learn programs. Studies show that such cross-disciplinary networks promote openness and trust between mental health professionals and facilitate information exchanges of available mental health resources (e.g., Bailey et al., 2018). Moreover, the development of such networks is specifically significant in the law enforcement profession, which tends to operate in silos and be suspicious of other groups (Shore & Lavoie, 2019).
Enhance the Use of Information Technology
Our results showed that technology should be utilized more effectively as a pathway for service provisions. At the bottom line, officers’ ability to successfully assist PWMIs is a function of their fundamental awareness of the mental health resources available to them (Shore & Lavoie, 2019). They must have access to up-to-date information such as local community mental health treatment options; volunteer groups; and nearby food pantries, homeless shelters, and hospitals with available beds.
This can be achieved by partnering with technology companies in the community to design mobile apps and websites that provide accurate real-time information about such resources. Naturally, the target audience for training on such technology should be officers at the street level, those who come in daily contact with PWMIs, and not only the executive levels (as suggested by our findings).
Promote Accountability Through Leadership
Accountability to PWMIs is at the heart of successful service delivery (Giusti et al., 2004) and is central to the challenge of scaling up police service provision. The high degree of role conflict the officers in our study exhibited (i.e., the role of a law enforcer versus the role of a welfare worker), emerged as a major barrier to service provision to PWMIs that must be overcome - but how?
We do not claim to have the answer for how role conflict in policing can be diminished. And although it may not seem possible to achieve such a drastic change in police culture in the near future, small steps can be taken by police leaders to alleviate it. For example, our findings suggest that when management demonstrated acceptance of the mental health problem as a policing issue – so did their officers.
Creative and forward-thinking leaders can take advantage of this by setting high expectations for service provisions to PWMIs in their agencies, and seizing opportunities to praise, encourage, and support officers who demonstrate it. Moreover, they should promote selection criteria that emphasize service-oriented police officers and support the development of a generation of well-integrated law enforcement professionals who understand the complicated role of the police officer in this postmodern policing era.
Conclusion
This study uses the “structure, culture, and practice triplet” framework of transition theory to depict the factors that facilitate or inhibit police service provision to PWMIs. The reality is that society has come to rely heavily on police to address mental health issues (Watson et al., 2021), and police officers have shifted from being the gatekeepers to the criminal justice system to being (also) the gatekeepers to the social welfare system. Like other scholars (e.g., Shore & Lavoie, 2019), we believe this shift in police role is inevitable.
However, can police transition its service provision system to PWMIs? It might seem easy to answer no. After all, the literature is sprawling with evidence of how police systems have been historically resistant to change (e.g., Skogan, 2008), especially to the “invasion” of the social welfare dimension into their mission (Morabito et al., 2013).
Yet, the wide adoption of the CIT model across police agencies in the U.S. (e.g., Watson et al., 2021) and the quick adaptation in police practices during the COVID pandemic (Cohen & Fortune, 2022) are prime examples of how police are, indeed, capable of accepting change, and areopen to innovation.
Where does such a transition start? System-innovation scholars (e.g., Van Veelen et al., 2018) say, “start where the energy is” (Ebuenyi et al., 2020), that is, with those in the organization willing to think unconventionally, explore new ideas, take risks, and become mental health champions. They must be the driving force to initiate the change in the system. “Change must come from within” may sound like a boilerplate cliché. However, according to transition theory, only when key actors in the constellation develop a collective sense of urgency for change- will a transition in the constellation occur (Wiertsema et al., 2021).
To further our understanding of scaling up police service provision to PWMIs, future research should explore the ways SLBs rationalize mental health-related work practices. For example, how ideas about PWMIs’ deservingness shape SLBs’ service provision decision-making and the role of police subcultures in service delivery. Additionally, research should also focus on how to develop the resources required to support this transition at each level of the constellation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.