
Abstract
Background
Assessment of breast lesions with magnetic resonance imaging (MRI) provides a means for lesion detection and diagnosis. Proton (hydrogen-1) magnetic resonance spectroscopy (1H-MRS) has been proposed as a useful diagnostic technique in providing metabolic information of suspicious breast lesions.
Purpose
To determine the clinical significance of in-vivo single voxel 1H-MRS at 3T in the assessment of benign and malignant breast lesions in combination with dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI).
Material and Methods
Twenty-four women with known breast abnormalities from conventional imaging (mammography, ultrasonography) underwent DCE-MRI at a 3T MR scanner and 26 breast lesions were detected. Breast lesions were assessed according BI-RADS classification. Single voxel 1H-MRS was performed after gadolinium administration and choline peak was qualitatively evaluated. All lesions were confirmed histologically from the surgically excised specimens. Sensitivity, specificity, and accuracy of the 1H-MRS, of the BI-RADS classification and of their combination (DCE-MRI + 1H-MRS) were calculated.
Results
Fifteen out of 26 lesions proved to be malignant and 11 proved to be benign. In our study 1H-MRS showed sensitivity 80%, specificity 81.8%, and accuracy 80.7%. DCE-MRI showed sensitivity 100%, specificity 63.6%, and accuracy 84.6%. The combination of DCE-MRI and 1H-MRS provided higher accuracy (96.4%), as well as higher specificity 81.8% compared to BI-RADS classification.
Conclusion
The combined use of 1H-MRS and DCE-MRI found to have improved diagnostic performance in the assessment of equivocal breast lesions. 1H-MRS can be used as a useful adjunct during lesion characterization in clinical routine in cases classified as BI-RADS 3 and 4.
Keywords
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) has become an established modality for detection and diagnosis of breast lesions. In many studies, it has been demonstrated that DCE-MRI can be used to detect otherwise occult breast cancers in the same or the contralateral breast and that it plays an increasingly important role in the screening of women who are at high risk for breast cancer (1–4). It evaluates the morphologic features and the kinetic parameters of a lesion in order to detect characteristics of tumor microvasculature. The diagnosis and further assessment of the lesion is based on the fourth edition of the Breast Imaging Reporting and Data System (BI-RADS) which is used as a lexicon for the morphological and kinetic analysis of breast lesions (5). The sensitivity of DCE-MRI in the detection of breast cancer is almost 100%, and the method plays an important role in breast cancer staging (6). However, the specificity of breast MRI is greatly variable ranging from 37% to 97%, resulting in false-positive rates and unnecessary biopsies (2, 7–9). Therefore additional methods are necessary to improve the specificity and the positive predictive value of MRI and thus patient management and outcome.
Proton (hydrogen-1) magnetic resonance spectroscopy (1H-MRS) has been demonstrated as a useful diagnostic technique in providing metabolic information of suspicious breast lesions (10–16). The diagnostic value of 1H-MRS is typically based on the detection of choline-containing compounds such as phosphocholine and glycerophosphocholine. Choline complexes are believed to be precursors of the phospholipids that compose cell membranes. Therefore, elevations of choline signals are thought to reflect increased membrane synthesis and hence are considered a marker of active tumor (17).
Previous 1H-MRS studies performed on 1.5T MR scanners have reported reasonable levels of specificity for breast lesion characterization (10, 11, 14, 16, 18–20) proving that this technique may become a valuable adjunct to DCE-MRI in the clinical evaluation of breast masses. Nevertheless, although MR scanners of higher magnetic fields are increasingly used in clinical practice, few studies have reported 1H-MRS performance on 3T and above concerning breast lesion characterization (20, 21). It has been shown that signal to noise ratio as well as spatial and spectral resolutions have been remarkably improved in higher fields compared to 1.5T (22). Hence, as 1H-MRS is continuously being incorporated to the clinical routine; it would be of interest to evaluate the performance of the technique in high magnetic fields.
The purpose of the current study is to prospectively evaluate the diagnostic performance of 1H-MRS at 3T in patients with suspicious lesions at MRI by using histologic findings as the reference standard, to compare 1H-MRS results with the BI-RADS classification of the lesions and to assess the clinical significance of the combination of 1H-MRS and BI-RADS classification.
Material and Methods
Study population
In this prospective study, 24 women were included ranging in age from 33 to 75 years (Mean ± S.D., 53 ± 12 years), who underwent breast MRI from February 2010 to April 2010 because of suspicious mammographic or ultrasonographic abnormalities. Inclusion criteria were consecutive patients in whom the bilateral breast MRI shown one or more contrast-enhancing masses measuring at least 10 mm in the largest diameter and at least 7 mm in the other two dimensions. Exclusion criteria were previous or current neoadjuvant chemotherapy or radiation therapy, previous needle biopsy or other interventional or surgical procedures in the 2 months preceding the breast examination, the presence of metallic clips from previous surgery or needle biopsy in the breast, and general contraindications to MRI or to the administration of gadolinium-based contrast agents. None of the patients was a lactating mother.
Examinations were always scheduled during the second week of the menstrual cycle for premenopausal women. None of the enrolled postmenopausal women was under treatment with hormone replacement therapy.
Twenty-six breast lesions were detected on the dynamic contrast-enhanced imaging. All lesions were confirmed histologically either from the surgically excised specimens or ultrasound-guided core biopsy. Written informed consent was obtained from all patients.
MRI acquisition and postprocessing
All MR examinations were performed on a 3T MR scanner (Signa HDx GE Healthcare, Milwaukee, WI, USA), using a dedicated bilateral phased array breast coil (four-element two-channel coil, one channel per breast). All women were in the prone position and, immediately before the examination and during patient positioning, each patient was carefully instructed to breath normally and not to move during the entire examination.
Bilateral breast imaging was performed with the following protocol: (i) axial T2-weighted fast spin echo (FSE) sequence (T2-FSE, TR/TE, 3600/100 msec; slice thickness, 4 mm; spacing, 0 mm); (ii) axial diffusion-weighted echo-planar imaging (DWI) sequence (DW-EPI, TR/TE, 6000/63.7 msec; slice thickness, 4 mm; spacing, 0 mm); and (iii) axial short TI inversion recovery sequence (STIR) (TR/TE, 3875/90 msec; slice thickness, 4 mm; spacing, 0 mm). A three-dimensional (3D) fat-suppressed (FS) T1-weighted vibrant dynamic sequence (flip angle, 10°, 1 mm3 isotropic voxel, one unenhanced and five contrast-enhanced acquisitions) was taken once before and five times after the dynamic intravenous (IV) injection of 0.1 mmol/kg of gadopentate dimeglumine during 10 s approximately and followed by a 20-mL flush of saline solution.
Postprocessing consisted of image subtraction for all the dynamic phases (enhanced minus unenhanced images) and kinetic analysis of the lesions and signal-intensity curves were taken according to Kuhl (23). Lesion diameter was measured on the second phase, on axial images and, when needed, on coronal and sagittal reconstructions. Morphologic and dynamic lesion assessment was done according to the MRI lexicon of BI-RADS (5). Breast lesions classified in BI-RADS categories as follow: BI-RADS 2, benign lesion; BI-RADS 3, probably benign lesion (6-month follow-up is recommended); BI-RADS 4, probably malignant lesion (biopsy is recommended); BI-RADS 5, malignant lesion (surgical excision is recommended). Breast lesions classified as BI-RADS 2 were considered benign and those classified as BI-RADS 3, 4, and 5 lesions were considered positive for malignancy.
Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of DCE-MRI were calculated based on the final histopathology reports, or 2-year follow-up.
All MRI scans were interpreted by two experienced radiologists, with 12 and 8 years experience in breast imaging, respectively.
Proton 1H-MRS acquisition and postprocessing
For 1H-MRS performance single-voxel water and fat-suppressed point resolved spectroscopy (PRESS) was acquired 15 min after contrast administration. This delay time has already been mentioned in previous 1H-MRS studies of the breast, even after a double dose (0.2 mmol/kg) of a 0.5-M gadolinium chelate (18). In addition, there has already been discussed the relatively low effect of the extracellular gadolinium chelate in comparison with measurement errors and variability of intracellular choline levels (24).
Before 1H-MRS was performed the channel contralateral to the lesion was automatically switched off. Automated parameter optimization consisted of frequency and receiver gain adjustment and gradient tuning. To ensure MR signal quality, a shimming adjustment was also performed in order to reach a full width at half maximum (FWHM) of the unsuppressed water peak lower than 30 Hz. In two cases where the value of FWHM was >30 Hz the voxel was re-adjusted within the lesion in order to avoid areas of obvious signal inhomogeneities and voxel contamination from normal breast parenchyma.
1H-MRS sequence was acquired with the following technical parameters: TR/TE, 2000/155 msec; number of excitations (NEX), 56 for voxel size 3.375 cm3; and NEX, 32 for voxel size > 3.375 cm3; flip angle, 90°; 512 measurements. The spectra acquisition time was approximately 10 min including the shimming procedure. This relatively long TE (155 milliseconds) was chosen to increase the visibility of the choline resonance because of the longer T2 of choline (>350 milliseconds) in comparison with that of lipids (∼100 milliseconds) (25). The voxel of interest (VOI) was positioned by an experienced radiologist and an MR physicist in breast MRI and 1H-MRS. The positioning of the VOI was performed on axial FS T1-weighted vibrant dynamic images together with sagittal and coronal reconstructions of the T1 images. Voxel size was chosen not <1 cm3 and not > 8 cm3 and it was carefully adjusted to the lesion. The VOI position and size were chosen to encompass each enhancing lesion, limiting as much as possible the inclusion of non-enhancing gland parenchyma or surrounding fat.
Moreover, a strong lipid and water spectral suppression was applied using a frequency-selective inversion pulse surrounded by a spoiler gradient pulse of opposite sign, which also incorporates a motion correction.
A second MR physicist and an experienced radiologist qualitatively assessed the presence of choline in a blinded review of the water suppressed spectra. A copy of the spectra from all patients was given to each reader without any other information regarding MR images or voxel placement. Consequently, the readers were asked to evaluate the spectra for choline presence at 3.2 ppm, by responding yes or no.
In order to assess the diagnostic value of 1H-MRS, sensitivity, specificity, accuracy, PPV, and NPV values were calculated, as well as the statistical significance of the method. Also, 1H-MRS results were correlated with the BI-RADS classification of the lesions by multivariate analysis.
Statistical analysis
Descriptive statistics consisted of means and standard deviations (SDs) for patient demographics. Mann-Whitney U test was employed to determine whether Cho peak presence and BI-RADS classification are associated to lesion's malignancy separately. Receiver-operating characteristic (ROC) curve analysis based on logistic regression models was performed to compare the diagnostic performance of the multivariate models to that of BI-RADS classification and Cho presence. Data were analyzed in SPSS 16.0 (SPSS, Chicago, IL, USA) Statistical significance was set at P = 0.05.
Results
Twenty-six enhanced lesions were detected on DCE-MRI and 1H-MRS was performed. Twenty-five (25) out of 26 lesions were mass lesions and one was a non-mass lesion. The median lesion size at DCE-MRI was 2.5 cm (range, 0.8–9 cm).
From the 26 lesions 15 proved to be malignant and 11 proved to be benign. Among the 15 malignant lesions, 11 were invasive ductal carcinomas, three were invasive lobular carcinomas, and one was malignant phylloides tumor. Among the 11 benign lesions, nine were fibroadenomas and two consisted of fibrocystic changes.
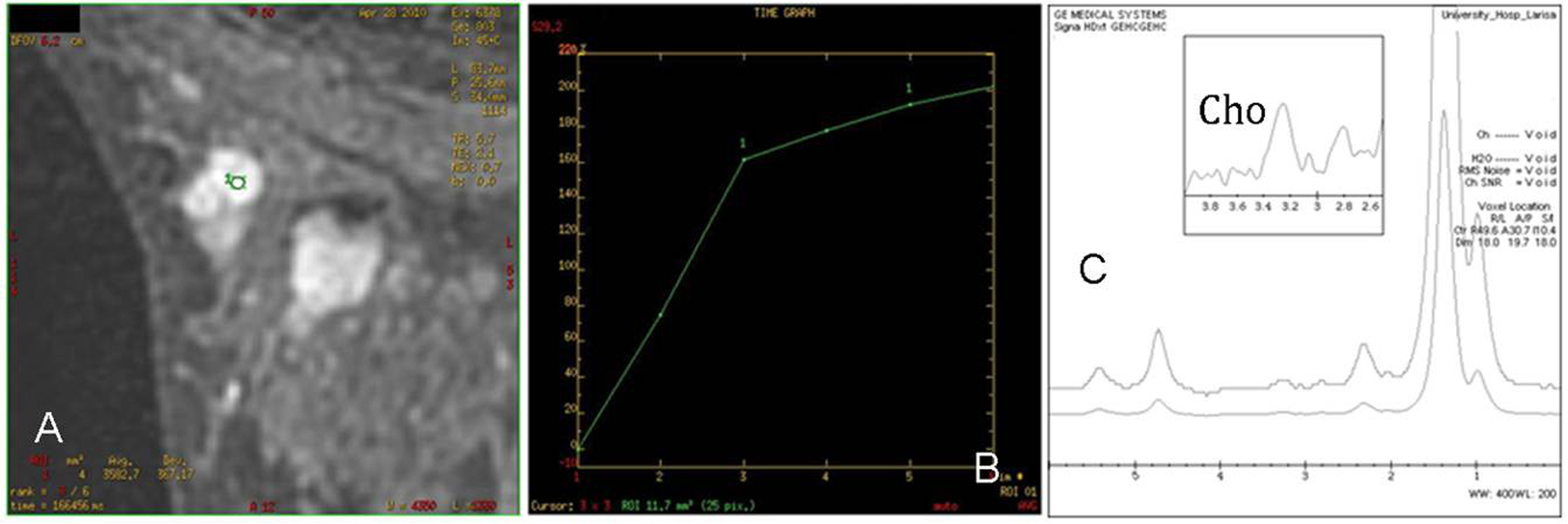
1H-MRS significantly differentiated malignant from benign breast lesions (P = 0.006). Specifically, 1H-MRS was positive for choline detection at 14 lesions and negative at 12 lesions. From the 14 Cho-positive lesions, 12 were malignant (Fig. 1) and 2 were benign (Fig. 2). From these 12 malignant lesions, eight were invasive ductal carcinomas, three were invasive lobular carcinomas, and one was malignant phylloides tumor. Their diameters were in the range of 1.7–9 cm. The benign lesions were two fibroadenomas in a 35-year-old woman.
A 49-year-old patient with invasive ductal carcinoma in the left breast. (a) T1-weighted vibrant dynamic sequence shows the malignant lesion. (b) A Cho peak at 3.22 ppm is clearly visible A 35-year-old patient with fibroadenoma of the left breast. (a) T1-weighted vibrant dynamic sequence shows the benign lesion. (b) The lesion exhibited a type I curve indicative of benignity. (c) A Choline (Cho) peak at 3.22 ppm is clearly visible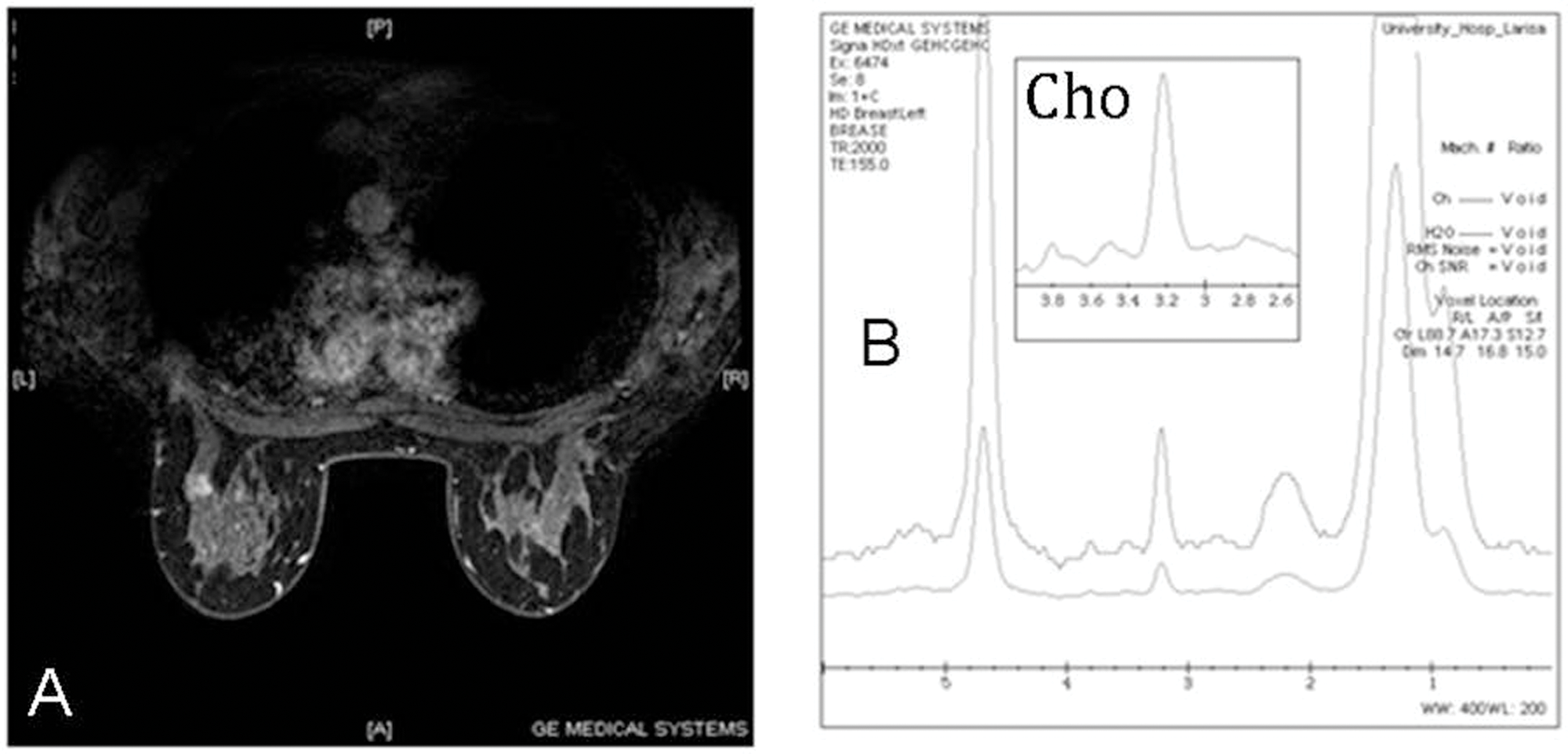
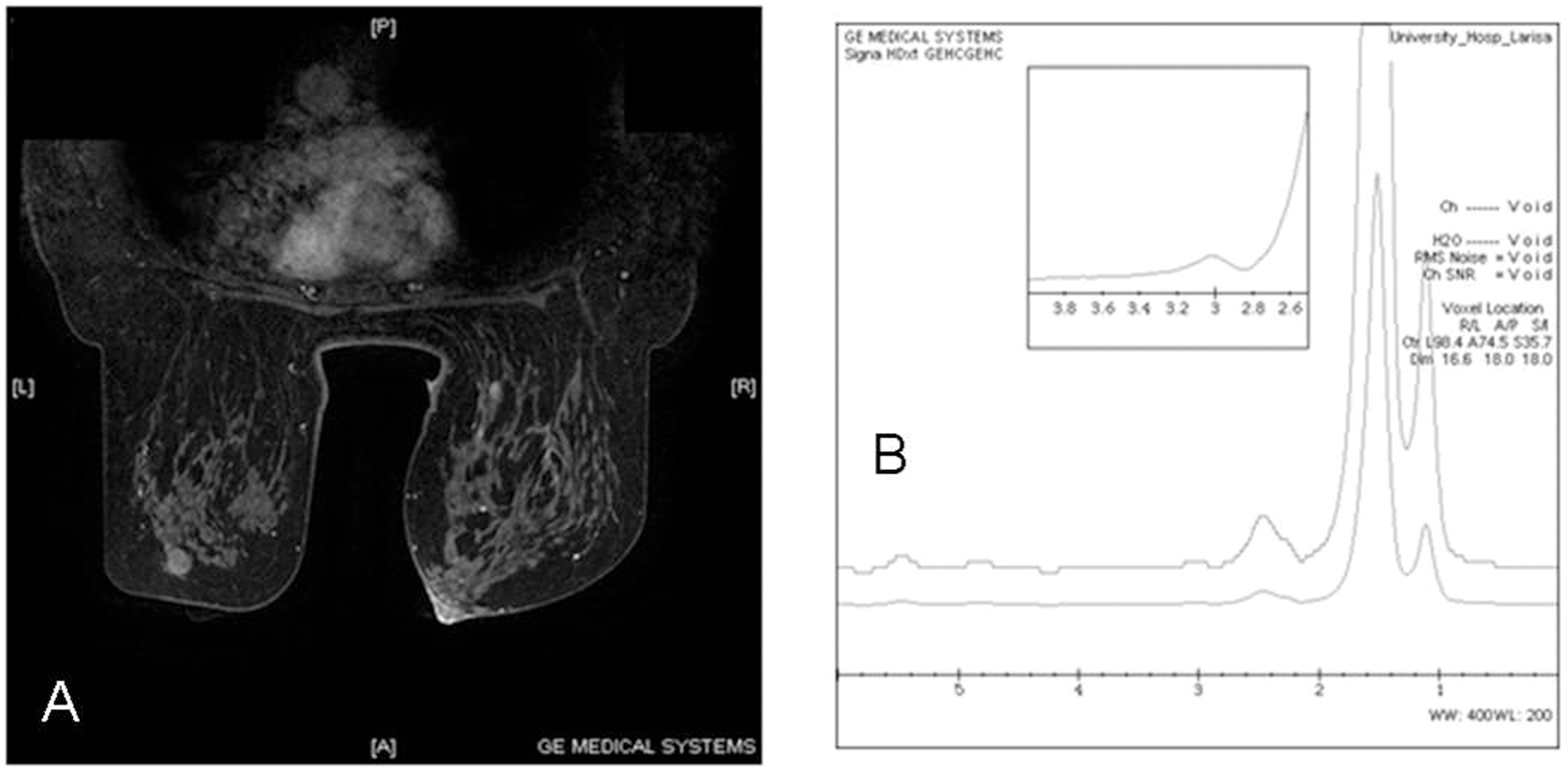
From the 12 Cho-negative lesions three were malignant (false-negative) (Fig. 3) and nine were benign lesions (true-negative) (Fig. 4). All three lesions proved to be invasive ductal carcinomas with their maximum dimension to be > 1.5 cm (1.5–3.2 cm). The nine true-negative cases included seven fibroadenomas and two fibrocystic changes. The aforementioned 1H-MRS results are summarized in Table 1.
A 67-year-old patient with invasive lobular carcinoma in the left breast. A. T1-weighted vibrant dynamic sequence shows the malignant lesion. (b) The lesion exhibited a type III curve indicative of malignancy. (c) MRS measurements show no Cho peak at 3.22 ppm A 53-year-old patient with fibroadenoma of the left breast. (a) T1-weighted vibrant dynamic sequence shows the benign lesion. (b) MRS measurements show no Cho peak at 3.22 ppm Correlation of 1H-MRS findings with histology and BI-RADS classification of breast lesions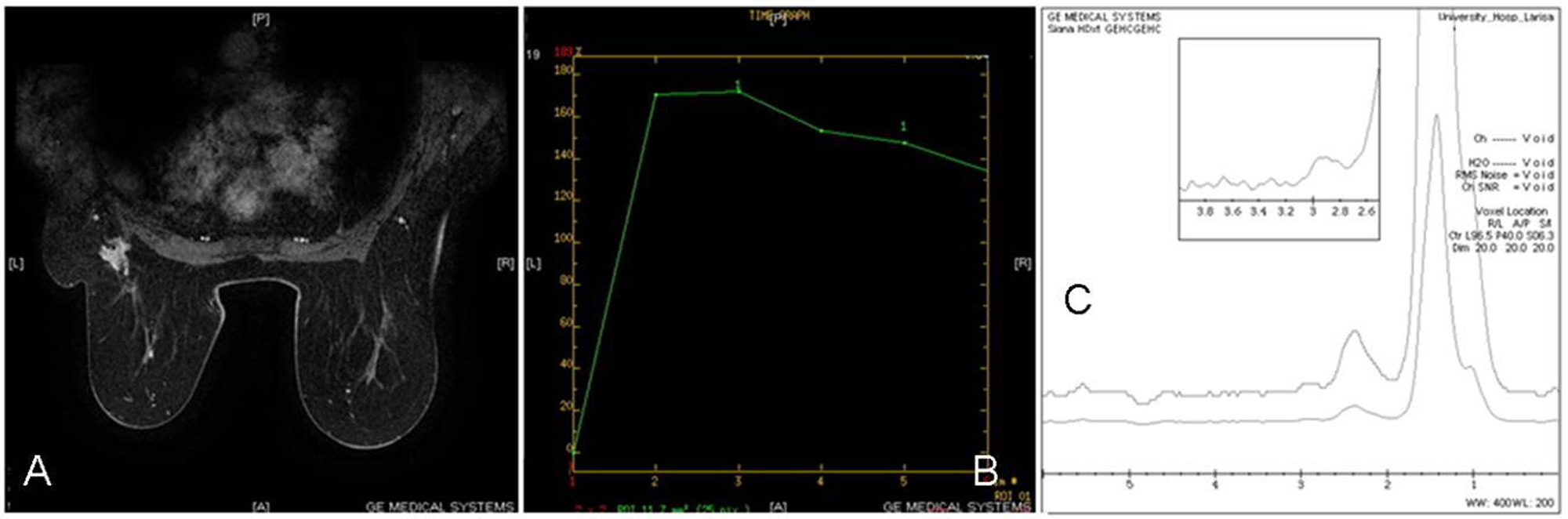
Patient demographics, voxel size, 1H-MRS choline presence and histology results
1H-MRS – BI-RADS correlation
The 26 breast lesions detected on the DCE-MRI were classified as follows: seven lesions as BI-RADS 2 (26.92%), two lesions as BI-RADS 3 (5.55%), nine lesions as BI-RADS 4 (34.61%), and eight lesions as BI-RADS 5 (30.76%). All seven BI-RADS category 2 lesions and all two BI-RADS category 3 lesions proved to be benign, either histologically or by follow-up. Of the nine lesions assigned BI-RADS 4, seven were proved to be malignant and two to be benign by histology. Also, all eight lesions assigned BI-RADS 5 histologically proved to be malignant by histology. DCE-MRI had a sensitivity of 100%, specificity of 63.6%, PPV of 78.9%, NPV of 100%, and accuracy of 84.6%. BI-RADS classification significantly differentiated malignant from benign breast lesions (P < 0.005).
The five out of seven BI-RADS 2 lesions were choline-negative (true-negative). The two BI-RADS 2 lesions that were choline-positive (false-positive) were fibroadenomas in a 35-year-old woman. All BI-RADS 3 lesions were choline-negative (true-negative).
The two histological benign BI-RADS 4 lesions were choline-negative (true-negative). The six out of seven (6/7) histological malignant BI-RADS 4 lesions were choline-positive (true-positive) and 1/7 malignant BI-RADS 4 lesion was choline-negative (false-negative).
Of the eight BI-RADS 5 lesions six were choline-positive (true-positive) and two were choline-negative (false-negative). All the previous results are demonstrated in Table 1.
ROC analysis of 1H-MRS, BI-RADS classification, and 1H-MRS + BI-RADS
ROC curve analysis based on logistic regression models, showed that Cho presence alone produced a moderate discrimination of malignancy with an AUC of 0.807. On the other hand, BI-RADS classification produced an AUC of 0.846. Furthermore, the combination of DCE-MRI (BI-RADS) and 1H-MRS (Cho presence) provided even higher accuracy (AUC = 0.964), as well as higher specificity (81.8% versus 63.6% for BI-RADS) for the discrimination between malignant and benign breast lesions (Fig. 5) over BI-RADS classification or Cho presence alone (Table 3).
ROC curve for differentiating malignant from benign breast lesions using Cho presence (a), BI-RADS classification (b), and the combination of both (c) as discriminators Sensitivity, specificity, accuracy of 1H-MRS, and BI-RADS classification respectively, and their combination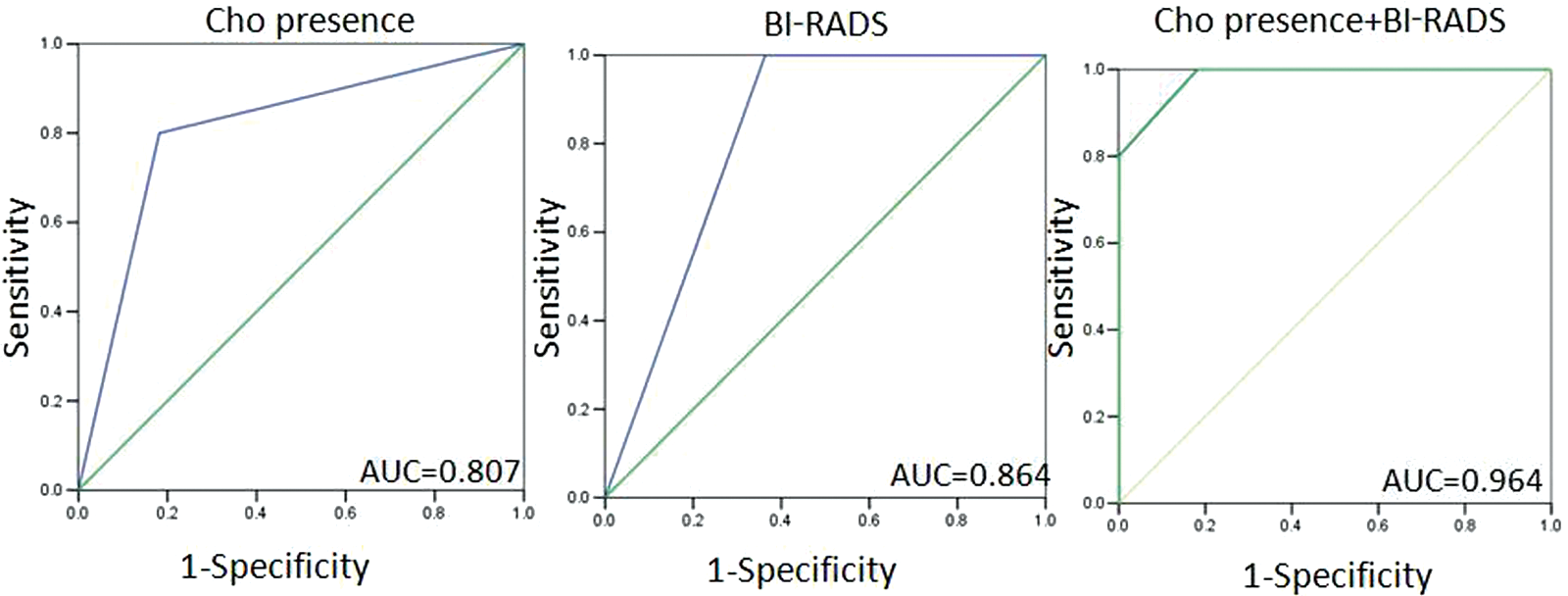
Discussion
Currently conventional breast MRI and DCE-MRI are not routine screening methods for breast disease; however, it serves an important role in identifying lesions in women with a high risk for developing breast cancer (4). Although the available dynamic morphological and kinetic features used for MRI interpretation reach high levels of sensitivity, they still exhibit relatively low specificity which remains a drawback in the differential diagnosis especially in small breast lesions (1–4, 6–9). For that purpose a shift towards molecular MRI promises to provide an insight into the underlying metabolic characteristics of breast tumors and thus improve MRI specificity. In-vivo 1H-MRS is a non-invasive method for characterizing the cellular biochemistry which underlies breast pathologies, by monitoring the choline concentration. As choline complexes are believed to be precursors of the phospholipids that compose cell membranes, increases in choline signals are thought to reflect increased membrane synthesis. It can be considered as a bridge between metabolism and the anatomic and physiological studies available from MRI. 1H-MRS of the breast is proposed to be used as an adjunct to the MRI examination for the improvement of specificity. 1H-MRS can provide a qualitative and/or a quantitative analysis of a number of metabolites within the tissue under study (25). For a meaningful 1H-MRS procedure several parameters should be properly adjusted before the spectroscopic examination, as they strongly affect tCho visibility within the spectrum. The two parameters which hold particular importance for high quality spectra include shimming and voxel localization performance (26, 27).
Elevated levels of the choline signal have been reported in many studies of excised human breast tumors, cultured human breast cancer cells, and animal models (28). The phosphocholine content in human breast cancer cells was found to be 10-fold higher than that of normal human mammary epithelial cells (29–32). Several studies have been also devoted to the in-vivo spectroscopic detection of choline in breast lesions achieving reasonable levels of specificities (33–36). Nevertheless, most of the previous studies have been performed on 1.5T MR scanners and only few investigators have reported 1H-MRS performance on higher magnetic fields (3T and above) concerning breast lesion characterization (20, 21, 26, 37, 38). With the advent of 3T MR scanners into clinical practice it would be challenging to report 1H-MRS performance, as improvements in the signal-to-noise ratio using higher field magnets (27) may increase the detection of composite choline compounds and therefore may increase the specificity in the detection of smaller breast cancers.
In this study the initial results regarding the utility of 1H-MRS in distinguishing benign from malignant breast lesions at 3T are demonstrated. Also, a correlation between 1H-MRS findings and BI-RADS classification of the lesions is performed and the diagnostic accuracy of the combination of 1H-MRS + BI-RADS classification is assessed. The diagnostic sensitivity, specificity, and PPV of 1H-MRS were 80%, 81.8%, and 85.7%, respectively, which compared favorably with the results of previous investigators (10, 11, 14, 16, 18–20). Taking into account that DCE-MRI shows a wide range of specificities (37–97%) (2, 7–9), 1H-MRS is a method which may shift that range towards higher values. According to the literature, MRI has an NPV of 97% (39–41), so a malignant lesion can be safely excluded. In this study the NPV of MRI is 100%. The most equivocal breast lesions are those classified as BI-RADS 3, with a possibility of malignancy <2% (42) and, second, those classified as BI-RADS 4, with a possibility of malignancy ranging between 2–95% (42).
In the literature, there is a wide range of cancer yield for BI-RADS 3 lesions (43). The diagnostic work-up of BI-RADS 3 lesions usually is a 6-month follow-up, but in many cases a biopsy can be performed. The diagnostic work-up of BI-RADS 4 lesions is biopsy. In both cases there is a significant number of benign disease after biopsy (39).
Comparing the results of 1H-MRS and BI-RADS classification, all BI-RADS 3 lesions, which proved to be benign in our study, were true choline-negative. These cases can be excluded from further invasive diagnostic work-up and 6-month follow-up can be suggested to them. In our small sample the two BI-RADS 4 lesions that were choline-negative, proved to be benign at biopsy. In contrast, six out of seven BI-RADS 4 lesions (85.7%) that were choline-positive proved to be malignant at biopsy. More studies need to be performed to confirm this trend to avoid biopsy in cases with equivocal morphological and kinetic findings assigned as BI-RADS 4 and 1H-MRS negative results. In these cases close follow-up can be recommended.
In our study one BI-RADS 4 lesion and two out of eight BI-RADS 5 lesions, which were proved to be malignant by histology, were false choline-negative. In these three cases the morphological and kinetic features of the lesions were typical of malignancy so that the complementary use of 1H-MRS was not necessary for diagnostic purposes. Likewise, the two benign 1H-MRS false-positive lesions exhibited typical benign morphological and kinetic features.
The diagnostic sensitivity, specificity, and accuracy of the combination of 1H-MRS and BI-RADS classification were 100%, 81.8%, and 96.4% respectively, higher than the corresponding values of 1H-MRS and BI-RADS classification alone, as shown in Table 3. Therefore, the aforementioned results suggest that 1H-MRS may be a useful adjunct to breast MRI, especially in equivocal cases classified as BI-RADS 4, by reducing the number of unnecessary biopsies.
In the literature there are a few studies featuring the diagnostic value of combined DCE-MRI and MR spectroscopy in evaluating breast lesions (43–46). In these studies different MRS techniques were performed such as multivoxel MRS (43), chemical shift imaging (CSI) (44), MRS imaging (MRSI) (45), or the single-voxel (SV) technique (46). Their results show that MRS may be a promising technique for the classification of breast lesions at equivocal DCE-MRI findings. All of them were performed in 1.5T MR unit. In our study single voxel (SV) MRS was performed in 3.0T MR unit. In the study of Dorrius (43) only lesions ≥1 cm3 were included and the lesions were located at precontrast sequences. In our study, smaller lesions were evaluated because of the 3.0T MRI system, and more specific location of the lesion was performed as postcontrast sequences were used.
In the current study, 1H-MRS was performed using the SV technique. In SV scan techniques, the selected voxels are well-defined with minimal contamination from the surrounding breast parenchyma. Thus, the magnetic field homogeneity across the volume of interest can be readily optimized, leading to improved water and fat suppression, and hence improved spectral resolution (25). On the other hand, SV 1H-MRS has several limitations in terms of breast coverage, since within the time constraints of a clinical examination, only a few breast regions can be sampled. In addition, SV 1H-MRS cannot provide information on the regional distribution of tCho within the breast. Therefore, there has been a shift towards multivoxel technique, since it provides full volumetric coverage of the breast under study, and metabolic information of tCho can be generated. Therefore, multiple lesions can be evaluated simultaneously and lesions boundaries as well as tumor infiltration may be defined. Nevertheless, due to the increasing difficulty of lipid suppression to the breast parenchyma it is more difficult to obtain high filed homogeneity across the entire volume selected, which is necessary for a high quality spectrum (36, 45).
Quantitative spectroscopic analysis can be a substantial improvement over the qualitative detection methods used in breast 1H-MRS. Quantification may be particularly important in the breast because the sensitivity of the 1H-MRS measurement is generally more variable than it is in brain tissue (20). This is due primarily to the highly variable adipose tissue content of the breast and the greater variation of the coil receive efficiency (20). Additionally, quantitative methods extract more information regarding the tissue biological condition and enable more sophisticated statistical analyses (47).
Nevertheless, although absolute quantification of choline concentration may be more desirable in assessing suspicious breast lesions, this method requires additional time to collect data from an internal or external reference, to correct partial volume effects that result from the inclusion of adipose tissue in the prescribed voxel, and to carefully calibrate differences in relaxation times between the tissue choline signal and references (20, 44). Therefore, in such cases 1H-MRS of the breast may not be practical in the clinical setting. On the other hand, a qualitative evaluation of the choline resonance which can be included in a standard imaging routine may provide a substantial and quick answer, which is important if 1H-MRS is to be included in a clinical diagnostic protocol for breast cancer.
From the 15 cancers in our study, 1H-MRS showed false-negative results in three cases of invasive ductal carcinomas. This could be attributed to the recent hemorrhage of the lesions, since blood products can degrade the local field homogeneity or to motion artifacts due to the extended length of the examination (10, 16). Thus, it seems that the sensitivity of breast 1H-MRS is strongly dependent on the nature and content of the tumor. This dependency appears to be mainly based on the technical issues related to the detection of smaller quantities of composite choline.
Another possible cause of this drawback, could be that at least one dimension of these tumors was <1.5 cm, while the minimum voxel dimension used was not <1.5 cm for adequate signal purposes which is sometimes referred to as “voxel bleeding”. Therefore, some amount of the surrounding fat was included inside the voxel and may have contributed to the overall signal, masking the tCho presence in these cases. In fact, such inclusion deteriorates the homogeneity of the main magnetic field (B0) in the region of interest, due to different magnetic permeability of fat and lesion tissue interface, which hampers the shimming procedure (48). In accordance with our observations, at least two previous studies showed that the sensitivity of breast 1H-MRS is strongly dependent on tumor size, and that small malignant lesions (<3.375 cm3) may not reveal a choline signal, resulting in false-negative diagnosis (10, 16). Moreover, as 1H-MRS was performed after contrast enhancement, an under-estimation of the tCho signal in such small breast lesions may have occurred, since gadolinium chelates form ion pairs with tCho dropping its signal height (26, 49). Hence it is evident that 1H-MRS sensitivity is tumor size and contrast enhancement dependent, mainly due to the technical issues related to the detection of smaller quantities of composite Cho.
In our study we included two false-positive cases, which were two fibroadenomas in a young woman (aged 35 years). This has been previously reported (11, 14), although the most common reported false-positive cases are histologically tubular adenomas or fibrocystic changes (11, 14). The reason that some fibroadenomas show choline is unknown and it could refer to the limitations of the method in the diagnosis of benign tumors (28).
It should be mentioned that most of the previous 1.5T studies concerned lesions > 1.5 cm in size (10, 11, 14, 16, 18, 19). In our study, we examined lesions in the range of 0.8–9 cm in DCE-MRI, and it was feasible to detect choline in small (<1 cm) malignancies. Thus, 1H-MRS performance in 3T seems to be superior in characterizing small breast masses due to increased signal-to-noise ratio and spatial resolution compared to 1.5T (27). The improved visibility of small lesions at 3T compared to 1.5T was supported by the study of Matsuoka et al. (37). Consequently, improved mass localization in MRI leads to a better voxel prescription upon the lesion, further aiding 1H-MRS performance.
A limitation of the present protocol is the relative small sample size of the breast lesions from a single center resulting in monocentricity of the study. However, these are the initial results of the combined use of 1H-MRS and MRI at 3T, which indicate the potential advantages in characterizing breast lesions. Another limitation of our study is related to the use of SV 1H-MRS technique in terms of lesion coverage and the results may be affected by tumor heterogeneity.
In conclusion, in our study the combined use of 1H-MRS + DCE-MRI achieved higher accuracy in the assessment of equivocal breast lesions. Also, our study showed that 1H-MRS at 3T achieved good levels of specificity suggesting that this technique can be used as a useful adjunct during lesion characterization in clinical routine in cases with equivocal findings, especially classified as BI-RADS 3 and 4. More large scale studies need to be conducted with more sophisticated equipment of MR units in order to incorporate breast 1H-MRS into clinical practice.