
Abstract
Background
Renal arteriovenous malformations (AVMs) are rare vascular malformations that cause hematuria. Treatment for renal AVMs has evolved from open nephrectomy to transcatheter arterial embolization (TAE).
Purpose
To retrospectively evaluate efficacy and adverse events of TAE for renal AVMs.
Material and Methods
We examined 12 patients (three men, nine women; mean age, 56 years) with renal AVM with gross hematuria, who underwent 14 sessions of treatment, using various embolization materials (liquid embolization agents, gelatin sponge, and coils). Among the 12 patients, 10 had cirsoid AVMs, eight of which were high-flow lesions. The remaining two patients had aneurismal AVMs. We assessed technical and clinical success, and also complications. All patients were followed for 7–92 months (mean, 48 months).
Results
Technical success was obtained in all patients. Primary clinical success was obtained in all patients; however, recurrence was observed in two patients who were treated with coils alone. A second session of TAE led to the sustained relief of symptoms. Clinical success rate was significant better (P = 0.045) when coils combined with other agents or liquid agents were used, than when only coils were used. No major complications occurred in any of patients; post-embolization syndrome and deterioration of renal function were not observed.
Conclusion
TAE treatment was safe, effective, and provided a good outcome, except when only coils were used as the embolization agent.
Introduction
Renal arteriovenous malformations (AVMs) are rare vascular disorders, which may require treatment as they are frequently associated with gross hematuria (1). Other symptoms include flank pain, hypertension, and high-output heart failure. Renal AVMs are classified as congenital, idiopathic, and acquired. A cirsoid tangle of vessels is commonly observed in congenital lesions, while cavernous communication between arteries and veins, and aneurysmal change are observed in the idiopathic type (2); arteriovenous fistula is observed in acquired lesions. Gross hematuria is most commonly associated with the congenital type (2).
Treatment for renal AVMs has evolved from partial or total nephrectomy to transcatheter embolization (1,3). The development of microcatheter systems enabled the selective embolization of renal AVMs with preservation of the renal parenchyma. As the result, the frequency of post-embolization syndrome, which consists of fever, loin pain, nausea, and vomiting, has been significantly reduced (4).
Contemporary embolization techniques aim to permanently occlude the multiple small channels between arteries and veins, which form the nidus of the AVM. Several embolization agents used in the past, such as gelatin sponge particles, stainless steel or platinum microcoils, or polyvinyl alcohol are not adequate for the procedure because of high recanalization rate and subsequent recurrence of hematuria. Recently, absolute alcohol (3) or n-butyl 2-cyanoacrylate (NBCA) mixed with lipiodol (5) has provided good outcomes, in terms of safety, efficacy, and duration of results. However, there is a potential risk of severe complications, such as renal infarction and pulmonary embolism (3). Most of the studies performed on renal AVM are case reports and describes complications or outcomes of TAE performed on only a few cases. We retrospectively investigated the clinical outcomes and complications of TAE for renal AVMs using various embolization materials and techniques, which were performed in our facility over the past 10 years.
Material and Methods
Patients
Patients’ characterization and embolization technique.
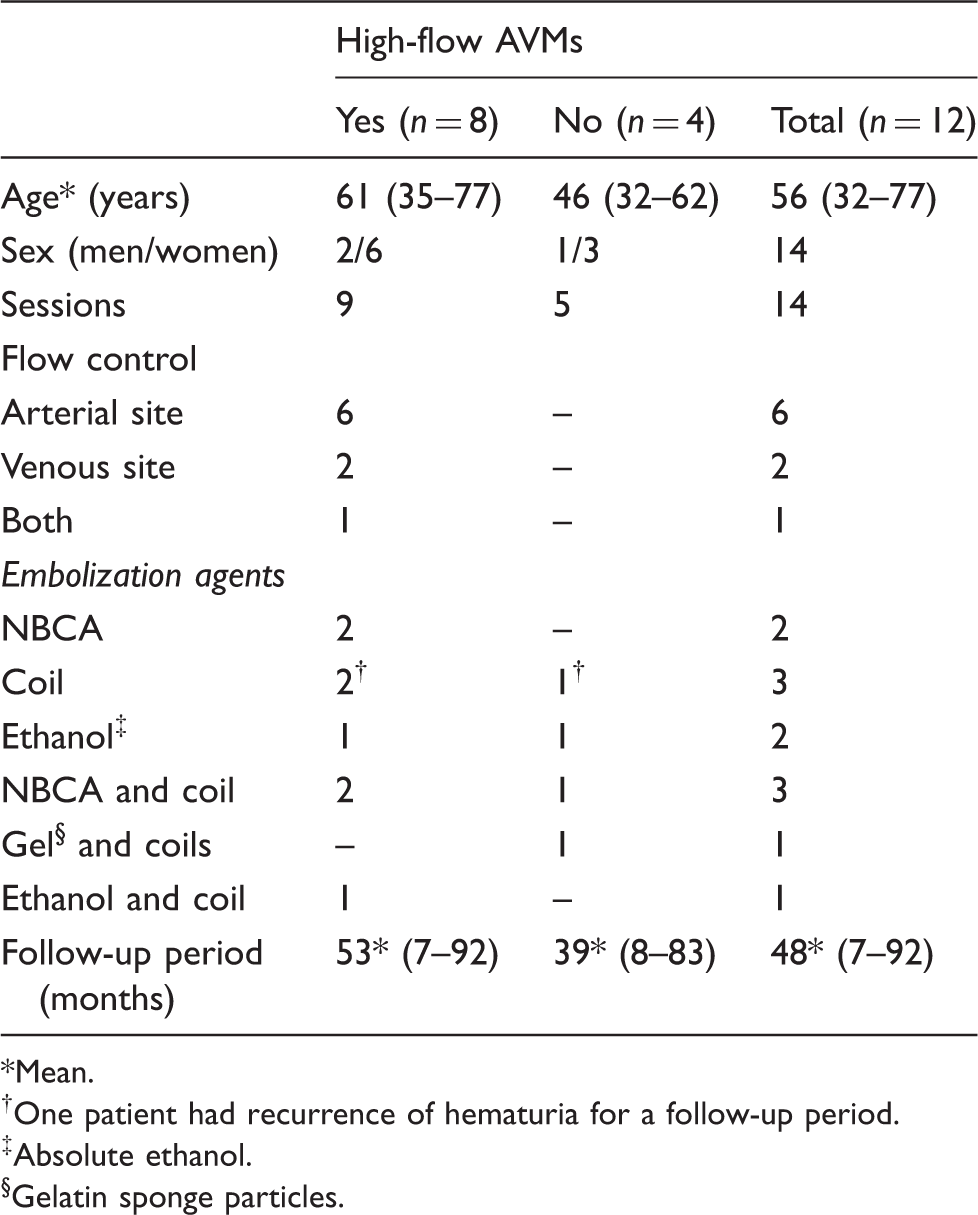
Mean.
One patient had recurrence of hematuria for a follow-up period.
Absolute ethanol.
Gelatin sponge particles.
Embolization technique
Angiography. The Seldinger technique was used to unilaterally place a 5-French sheath (Medikit, Tokyo, Japan) into the femoral artery. A 5-French pigtail catheter (Medikit) was advanced into the abdominal aorta at the T12 level, and abdominal aortography was performed to identify the number of renal arteries and the location of the renal AVM. Next, renal arteriography and selective arteriography of feeding arteries supplying the AVM were conducted to confirm the velocity of arterial inflow and venous return.
Changes of embolization agents used
From April 2001 to Jun 2003, gelatin sponge particles or coils, including detachable coils, were routinely used for TAE of AVMs, regardless of arterial inflow velocity. From July 2003 to March 2006, absolute ethanol had been primarily used, and since April 2006 NBCA began to be used. Changes in the embolization agents were approved by the Ethics Committee of our institution.
Embolization strategy
Super-selective embolization was performed using the coaxial catheter system. Flow control was applied for high-flow lesions to avoid the migration of embolization agents to systemic circulation. Draining vein (mainly the renal vein), or the renal artery, or both were occluded using balloon catheter to prevent migration of the embolization agents
Embolization techniques and materials
Coils
The afferent arteries of the renal AVMs or the arteries supplying the target area were selected with a microcatheter and embolization was performed with platinum microcoils, including detachable coils.
Combination of gelatin sponge particles and coils
First, the afferent arteries of the renal AVMs were selected using a microcatheter and were embolized with gelatin sponge particles. Thereafter, platinum microcoils, including detachable coils, were placed in the arteries supplying the target area.
Absolute ethanol
Alcohol ablation was performed using an emulsion of absolute ethanol and iodized oil (Lipiodol Ultra-Fluid; Guerbet, Aulnay Sous-Bois, France) (emulsion ratio 2:1), with a maximum ethanol dose of 0.4 mL/kg body weight (7,8). The emulsion was slowly injected via the afferent arteries. Flow control using a balloon catheter, with a 6-French shaft and a 20-mm-diameter balloon (Terumo-Clinical Supply, Tokyo, Japan), was performed in high-flow lesions. The balloon catheter was placed either in the feeding artery or the draining vein, or both, to occlude these vessels. Manual aspiration of blood was also performed simultaneously with ethanol injection via the balloon catheter placed in the draining vein. Blood loss during the procedure was minimal (10–30 mL).
NBCA
NBCA mixed with lipiodol was administered, with the ratio of 1:3. The ratio was sometimes modified, depending on the distance between the nidus and the microcatheter tip, and the velocity of venous return. Prior to the injection of NBCA mixture, a manual test injection with contrast media was routinely performed, to evaluate the velocity of flow thorough the AVM and venous return, and also the reflux of media into non-target areas. When the venous return was too fast, the renal artery was occluded by a balloon catheter to control arterial flow. When reflux of the contrast media into non-target areas was identified, blood flow was controlled by adjusting the expansion of the balloon (Fig. 1). The lumen of the microcatheter was filled with glucose solution before the administration of NBCA mixture to prevent the contact with blood, which can induce conjugation of the agent. NBCA mixture was immediately injected in the same manner as the test injection and the microcatheter was quickly removed after injection.
Flow control accomplished by adjusting the expansion of the balloon. Before administration of n-butyl 2-cyanoacrylate diluted in Lipiodol, several test injections were performed under different flow conditions, achieved by adjusting the expansion of the balloon, to confirm the absence of reflux of the contrast media into non-target areas. (a) Complete balloon occlusion of the renal artery (white arrow) led to reflux of contrast media into the non-target areas (black arrows). (b) Contrast media flows into the nidus without reflux, under incomplete balloon occlusion (arrow).
Assessment of embolization procedure efficacy
All clinical and laboratory data were obtained from the medical records. Results of treatment were classified according to the nidus volume reduction in post-treatment angiography; excellent for 100% reduction, acceptable for 80–100% reduction, and insufficient for <80% reduction. Technical success was defined as either excellent or acceptable embolization. Clinical success was defined as the cessation of hematuria within the 30 days after the procedure according to the record (9). For statistical analysis, SPSS ver. 18 (SPSS Japan, Tokyo, Japan) was used; differences at P < 0.05 were considered statistically significant.
Adverse events
In accordance with the criteria of the Society of Interventional Radiology (9), major complications were defined as those necessitating further treatment, and minor complications were those that resolved spontaneously or with conservative treatment.
Follow-up
Follow-up was performed until death, hospital discharge, or through further outpatient visits to a hospital or a urological clinic, if documented. The follow-up duration ranged from 7 to 92 months (mean, 48 months). Serum creatinine and BUN levels, and eGFR were measured 1–2 days and 6 months after renal embolization.
Results
Fourteen sessions of embolization were performed for 12 patients; two patients received additional treatment for recurrent hematuria (Table 1). Primary embolization was performed with coils in three patients, NBCA in two, absolute ethanol in two, a combination of NBCA and coils in three, a combination of gelatin sponge particles and coils in one, and a combination of absolute ethanol and coils in one. Excellent occlusion (Fig. 2) was accomplished in 10 patients, including six with high-flow lesions, while acceptable occlusion was obtained in the other two patients. Among the patients who obtained excellent occlusion, three patients were treated with NBCA alone, two with absolute ethanol alone, one with coils alone, one with a combination of gelatin sponge particles and coils, two with a combination of NBCA and coils (Fig. 3), and one with a combination of ethanol and coils. Two patients, who obtained acceptable occlusion, were treated with coils alone. Technical success and primary clinical success were obtained in all patients.
A 53-year-old man with cirsoid arteriovenous malformation (AVM). Right renal AVM was suspected, on the basis of enhanced CT results, during the determination of the cause of gross hematuria (a, arrow). Right renal arteriography demonstrated the cirsoid AVM (b). Superselective embolization with NBCA was performed and the post-embolization arteriography showed that the AVM was completely diminished (c). Enhanced CT, 2 years after the embolization demonstrated no recurrence of AVM (d), and the small high density areas indicated residual Lipiodol (d, arrow). No hematuria was evident over the 71-month follow-up period. A 71-year-old woman with cirsoid and aneurismal arteriovenous malformation (AVM). Renal arteriography demonstrated a cirsoid and aneurismal AVM and early venous return with higher flow arteriovenous connections (a). After embolization of the aneurismal connection with microcoils, including detachable coils, afferent arteries of nidus were embolized with NBCA, diluted in Lipiodol, with flow control achieved by adjusting the expansion of the balloon (b, arrow). Post-embolization renal arteriography showed that only a few afferent arteries of the nidus existed (c, arrow), but malformations were diminished after embolization. Hematuria did not occur over the 19-month follow-up period.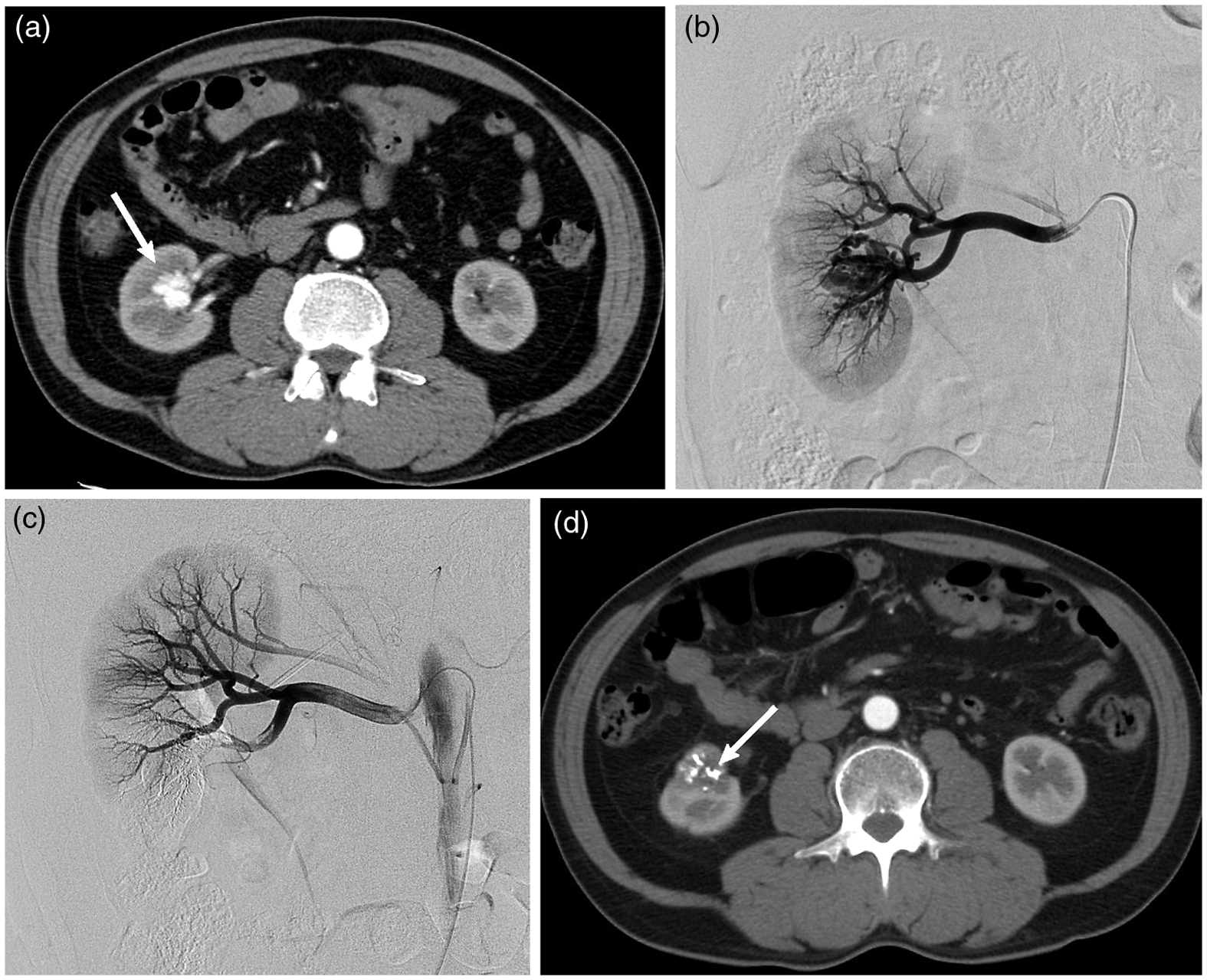

Ten patients, who obtained excellent occlusion, remained free of recurrence for an average of 69.8 months; however, two patients, who obtained acceptable occlusion, developed recurrent hematuria, 14 and 44 months after the initial embolization. A second session of TAE was performed using coils combined with gelatin sponge particles in one patient and NBCA alone in the other patient. They have remained free of hematuria for 39 or 48 months after the retreatment, respectively.
Results of recurrence.
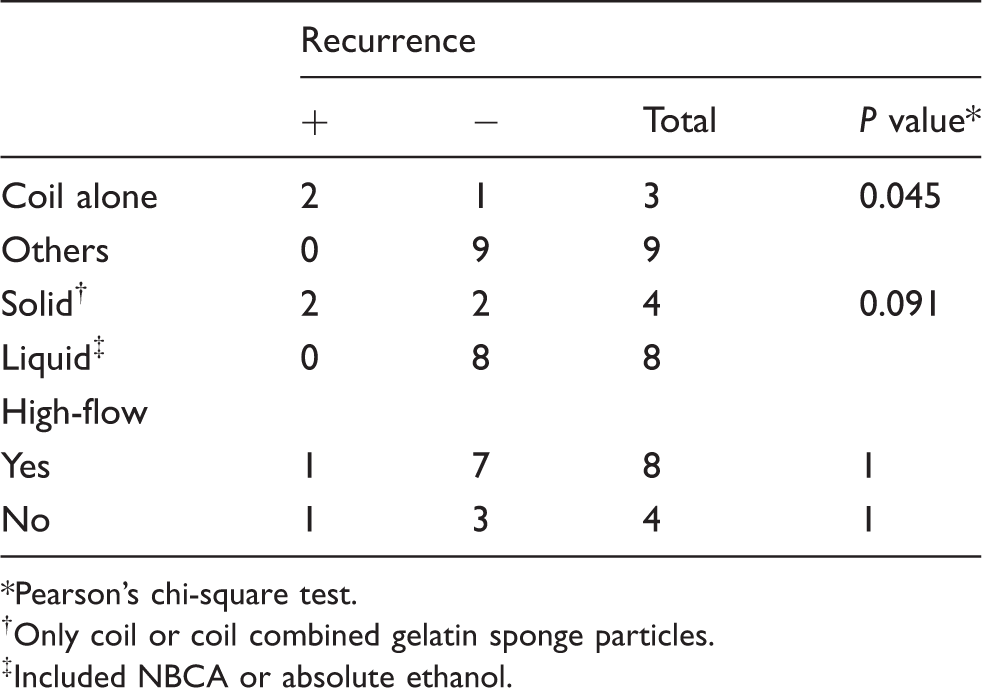
Pearson’s chi-square test.
Only coil or coil combined gelatin sponge particles.
Included NBCA or absolute ethanol.
Renal function after embolization.
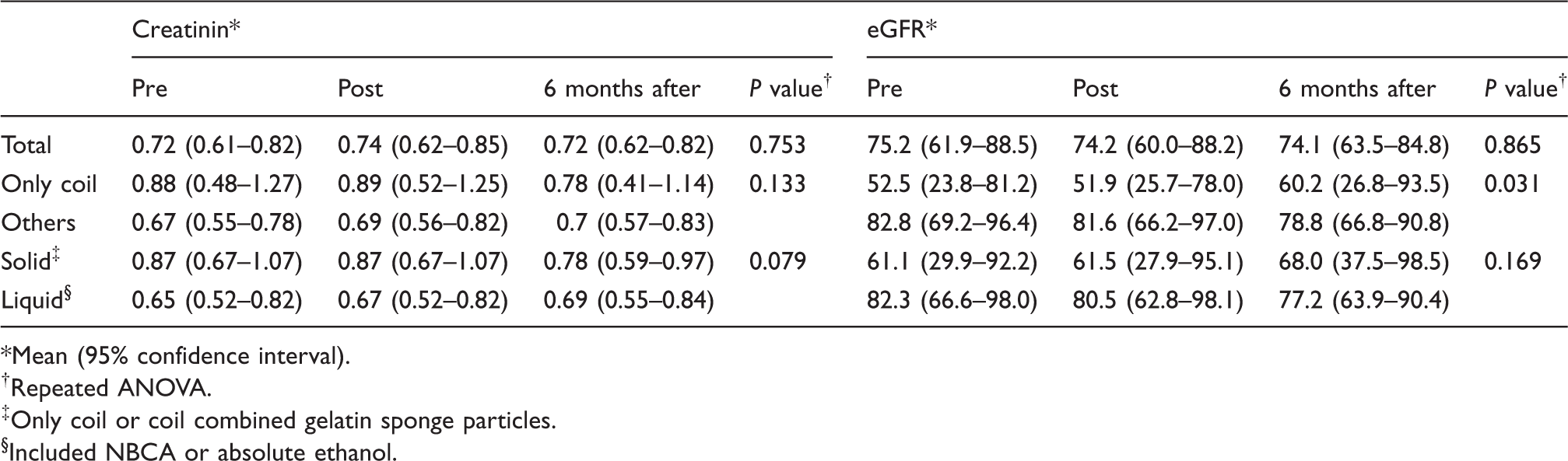
Mean (95% confidence interval).
Repeated ANOVA.
Only coil or coil combined gelatin sponge particles.
Included NBCA or absolute ethanol.
Discussion
The goal of embolization for AVM is permanent occlusion of the nidus, while leaving the draining veins and the parent arteries patent to avoid ischemic complications.
Several embolization agents, such as gelatin sponges, coils, or polyvinyl alcohol, have been used for the treatment of renal AVMs. Many authors have reported primary success by using gelatin sponge particles or with coils, but almost 50% of the previous reports have shown late, partial recanalization through the development of collaterals (3,10).
Polyvinyl alcohol has also been used because of its biocompatibility and inertness; however, recanalization of vessels has been reported in patients with facial AVMs (11). Moreover, histological examinations have revealed incomplete occlusion of major target vessels, with particles embedded in the renal arterial walls and residual patency of renal vessels that led to the excessive excretion of renin, resulting in hypertension (3).
Ethanol degenerates blood proteins and injures the vascular endothelium, thereby inducing intense thrombosis (12). This induces complete cellular death by total ischemia, minimizing the risk of vascular recanalization and activation of the renin-angiotensin system (3,13). An NBCA-lipiodol mixture can also be selectively delivered into the AVM nidus (5) and can produce permanent obliteration. The conjugation time can be controlled by altering the lipiodol concentration in the mixture (14,15) to obtain optimal embolization. Moreover, this procedure does not interfere with possible future retreatments. Conventional embolic agents, such as gelatin sponge particles, coils, and polyvinyl alcohol, have been replaced by absolute ethanol or NBCA for these reasons.
In this study, two of the three patients who were treated with only coils had recurrence of hematuria, while 10 other patients treated with other methods did not demonstrate recurrence. Eight patients who were initially treated with liquid embolization agents did not demonstrate recurrence of hematuria for 45 months, on average (range, 7–85 months). These results suggest that embolization using coils alone is not preferable, while the procedure using liquid agents is efficient enough to obtain sustained relief of hematuria.
One of the most severe complications related to the use of liquid embolization agents, is reflux to the normal parenchyma, resulting in renal infarction (3). Rapid injection of ethanol or NBCA increases the risk of reflux, due to the increased vascular resistance of the treatment area (16), so slow injection is recommended according to our experience. The residual flow in vessels should also be frequently checked to prevent the late ablation effect, caused by reflux (12). There is also a potential risk for pulmonary embolism (12) when treating high-flow lesions. Venous flow control techniques (7,8) were applied in this study and successfully prevented migration of liquid agents into systemic circulation. Test injections with contrast media are mandatory to adjust the expansion of the balloon catheter for optimal flow control (Fig. 1). Another complication of using ethanol is the possibility of alcohol intoxication. As Yakes et al. recommended (17), limiting the dose of absolute ethanol to within 0.5–1.0 mL/kg per session is important. We put a safety margin, taking into account individuals who are vulnerable to alcohol, which limited the maximum dose to 0.4 mL/kg. No intoxication was observed in this study.
None of the patients demonstrated post-embolization syndrome, owing to the super-selective embolization (4), and serum creatinine and BUN levels were within normal ranges before and after embolization. The postoperative eGFR values of patients treated with coils alone, were significantly higher than for those of patients treated with other modalities, presumably due to the lower preoperative values in the former group. Decline of eGFR values to abnormal level was not observed in either group.
The major limitation of this study is lack of follow-up angiography, except in four patients, leaving potential recurrence of AVMs unrevealed. Other limitations are the small number of patients, which makes statistical analysis less preferable, and the variability of renal function among patients. However, no exacerbations of renal function were observed, showing the safety of selective renal embolization regardless of the agents used.
In conclusion, TAE for renal AVM is efficient and safe, and the use of liquid embolization agents is especially recommended.
Footnotes
Funding
This study was supported by a grant from the Program for Promotion of Fundamental Studies in Health Sciences of the Organization for Pharmaceuticals and Medical Devices Agency (PMDA) and the Grant-in-Aid for Scientific Research (S and B) from the Ministry of Education, Culture, Sports, Science and Technology, Japan.