
Abstract
Background
Computed tomography urography (CTU) is used widely in the work-up of patients with symptoms of urinary tract lesions. Preoperative knowledge of whether a tumor is invasive or non-invasive is important for the choice of surgery. So far there are no studies about the distinction of invasive and non-invasive tumors in ureter and renal pelvis based on the enhancement measured with Hounsfield Units.
Purpose
To examine the value of CTU using split-bolus technique to distinguish non-invasive from invasive urothelial carcinomas in the upper urinary tract.
Material and Methods
Patients who underwent nephroureterectomy between 2006 and 2011 and who had split-bolus CTU prior to surgery were included. The images were available electronically. The attenuation values before and after administration of iodine-based contrast media were measured. The radiology, patient, and pathology records were reviewed.
Results
Of the 158 patients who underwent unilateral nephroureterectomy 69 fulfilled the inclusion criteria. Histopathological examination revealed 31 patients with non-invasive and 38 with invasive urothelial carcinoma. Neither absolute attenuation nor change in attenuation values obtained at CTU could distinguish between invasive and non-invasive lesions. No patients had a CTU within the last year before the examination that resulted in surgery.
Conclusion
A split-bolus CTU cannot distinguish between invasive and non-invasive urothelial tumors in the upper urinary tract, but the examination is useful to diagnose a tumor in the renal pelvis and the ureter.
Introduction
Computed tomography urography (CTU) is used widely in the diagnostic evaluation of the urinary tract in the work-up of patients with symptoms indicating presence of urinary disease (1). It has been discussed whether CTU could replace intravenous urography in the diagnosis of pelvic and ureteral tumors (2,3), but their occurrence is infrequent compared to cancers originating from the bladder wall and the renal parenchyma. To our knowledge the use of attenuation values to distinguish between invasive and non-invasive tumors of urothelium in the ureters and the renal pelvis has never been studied.
There is an ongoing discussion on the best method to conduct CTU (1). We prefer the split-bolus method. Urothelial tumors in the ureter and pelvis (Fig. 1) are rare, but a correct preoperative diagnosis of the invasiveness is important for the prognosis and the choice of surgery (local excision versus nephroureterectomy) in selected high-risk patients. Obtaining a biopsy from a suspected tumor in the upper urinary tract is difficult as it requires ureteroscopy with precise biopsy targets and the pathologic results are often unclear particularly in terms of invasion mainly due to the small sample size and superficial biopsy (4). Therefore we found it important to study whether a simple measurement on the images from a low radiation and low contrast CTU could help with the diagnostic issues about invasiveness as it helpful to distinguish between clear renal cell carcinoma (RCC) and papillary RCC (5).
An example of an urothelial cell tumor in the right pelvis.
Material and Methods
Patients
All patients undergoing nephroureterectomy at the Department of Urology, Copenhagen University Hospital Herlev from 2006 through June 2011 fulfilling the following criteria were included in the study: (i) the patient had undergone split-bolus CTU prior to surgery; (ii) the CTU was available in electronic format (PACS); (iii) histopathological examination of the removed tissue had been performed.
The patient records of the included patients were reviewed with regard to patient sex, age, medical status, concurrent diseases, previous surgery, and symptoms leading to the CTU. It was noted if a patient underwent CTU within the 12 months before the examination that led to surgery.
Histopathology
The pathological specimens were reviewed by an uropathologist for the diagnosis including grading and pT-staging. The tumors were graded according to the WHO 2004 classification (6) and staged according to the UICCC TNM system (7). Tumors with stage T1 or more were classified as invasive and pTa staged tumors as non-invasive tumors. The terms “benign” and “malignant” are no longer used regarding urothelial tumors but have been substituted by the terms “non-invasive” and “invasive” according to WHO (6,7). The term “invasive” is thereby not used in the radiological sense where it describes the invasiveness of the tumor, but in accordance to the pathological classification as mentioned above.
CT urography
The CTUs were all performed on a 16 MDCT scanner (Philips Medical Systems, Best, The Netherlands) using our standard protocol. Breath-hold was used to obtain the CT images. The unenhanced series used the following parameters: 120 kVp, 40–100 mAs (depending on patient size), pitch 0.938, section thickness 16 × 1.5 mm reconstructed to 3 mm, increment 1.5 mm. In the contrast series the mAs was 150; otherwise the parameters were identical in the two runs.
The patients were instructed not to void within 2 h before the examination. No oral contrast medium was administered. Immediately after the non-contrast series 25 mL of Iomeprol 400 mgI/mL (Iomeron®, Bracco, Milan, Italy) were given intravenously by hand injection. Ten minutes later, using a stop watch, 50 mL of the agent was administered intravenously followed by 20 mL normal saline using an injection pump (Medrad, Warrendale, PA, USA). Fifty seconds after the start of the injection the second CT run was done. Axial and coronal reconstructions (3/3 mm) were performed and forwarded to the PACS system.
Image analysis
The CT images were evaluated independently by two radiologists who only had access to the indication on the request for the examination. All other information related to the examination was erased. The attenuation before and after contrast medium administration was measured (Hounsfield Units [HU]) using the PACS (iSite, Phillips Medical Systems, Best, The Netherlands).
A round region of interest (ROI) was placed in the middle of three subsequent image slices in the center of the lesion where there were no visible opacified urine and a clear distance to normal tissue to avoid partial volume artifacts and the possibility of pseudoenhancement (Fig. 2). In masses with calcifications, vessels, or cysts the ROI was placed outsides of these and in the most homogenous area of the lesion. The size of the ROI was 0.35–1.5 cm2. Tumors being so small in size that a ROI in this range could not be placed as the above mentioned criteria were excluded. The size and placements of the ROI were consistent in the two runs. The size and site of the lesions were measured.
Example on placement of the region of interest (ROI) and the measurement of HU before (left) and after (right) contrast medium administration.
Statistical analysis
Statistical analyses were performed using the statistical software “R”.
Results
Of the 158 patients, who underwent nephroureterectomy over the 6.5 years, 69 patients fulfilled the inclusion criteria. The most frequent cause of exclusion was absence of an electronic version of the CTU (51 patients) and no split-bolus CTU prior to surgery (18 patients). The remaining 20 patients were excluded because of misclassified tumor, e.g. bladder tumor without ureteral involvement (2 patients), renal cell carcinoma (3 patients), or sarcomatoid carcinoma (1 patient). Thirteen had no enhanced CT mainly due to GFR below 45 mL/min/1.73 m2; some of these patients had enhanced MRI. One patient was excluded as a consensus decision by the two readers because the tumor was too small to be measured.
Thirty-one patients with a median age of 71 years (range, 41–87 years) had a non-invasive tumor and 38 patients with a median age of 77 years (range, 50–88 years) had an invasive tumor. Among the 89 excluded patients 34 patients who has a non-invasive tumor were 47–90 years old (median age 74) and the 55 with an invasive tumor were 45–89 years old (median age, 73 years).
None of the 69 patients had undergone a CTU 1 year prior to the diagnostic CTU that led to nephroureterectomy.
Localization and symptoms
Of the 69 tumors 78.3% were located in the renal pelvis, 2.9% in the upper third of the ureter, 5.8% in the mid third, and 13% in the lower third of the ureter. Of the invasive tumors 86.8% were found in the renal pelvis, whereas this was only the case for 67.7% of the non-invasive tumors.
In 48 of 69 patients (69.6%) macroscopic hematuria was the cause for the referral to the CTU that showed the lesion in the renal pelvis or ureter. Other reasons for referral were known bladder tumor (8 patients), pain (4 patients), microscopic hematuria (4 patients), and other reasons including findings on imaging for non-urologic disease (4 patients). In one patient the reasons for referral could not be found in the records.
The distribution of symptoms leading to CTU.

Enhancement
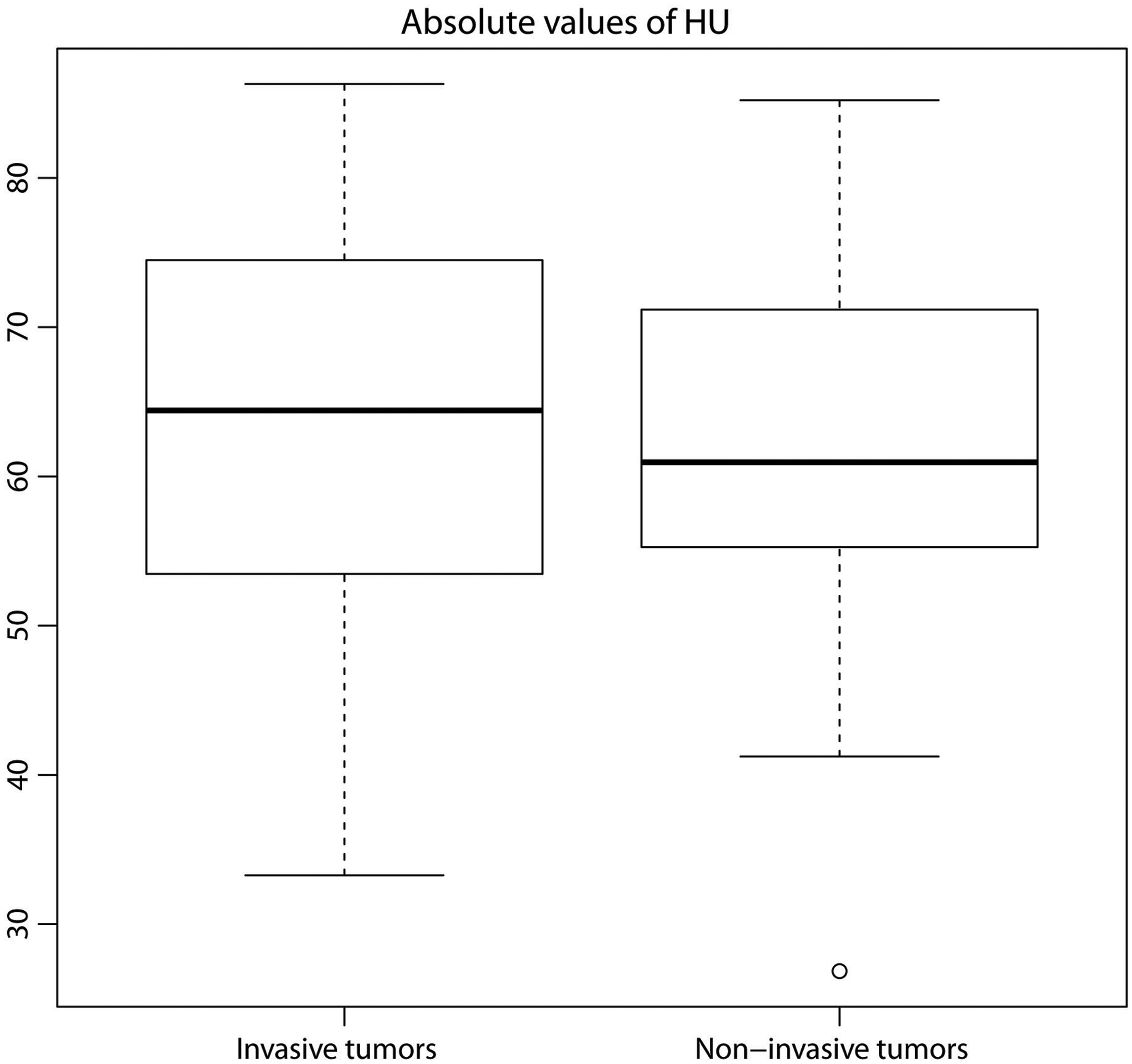
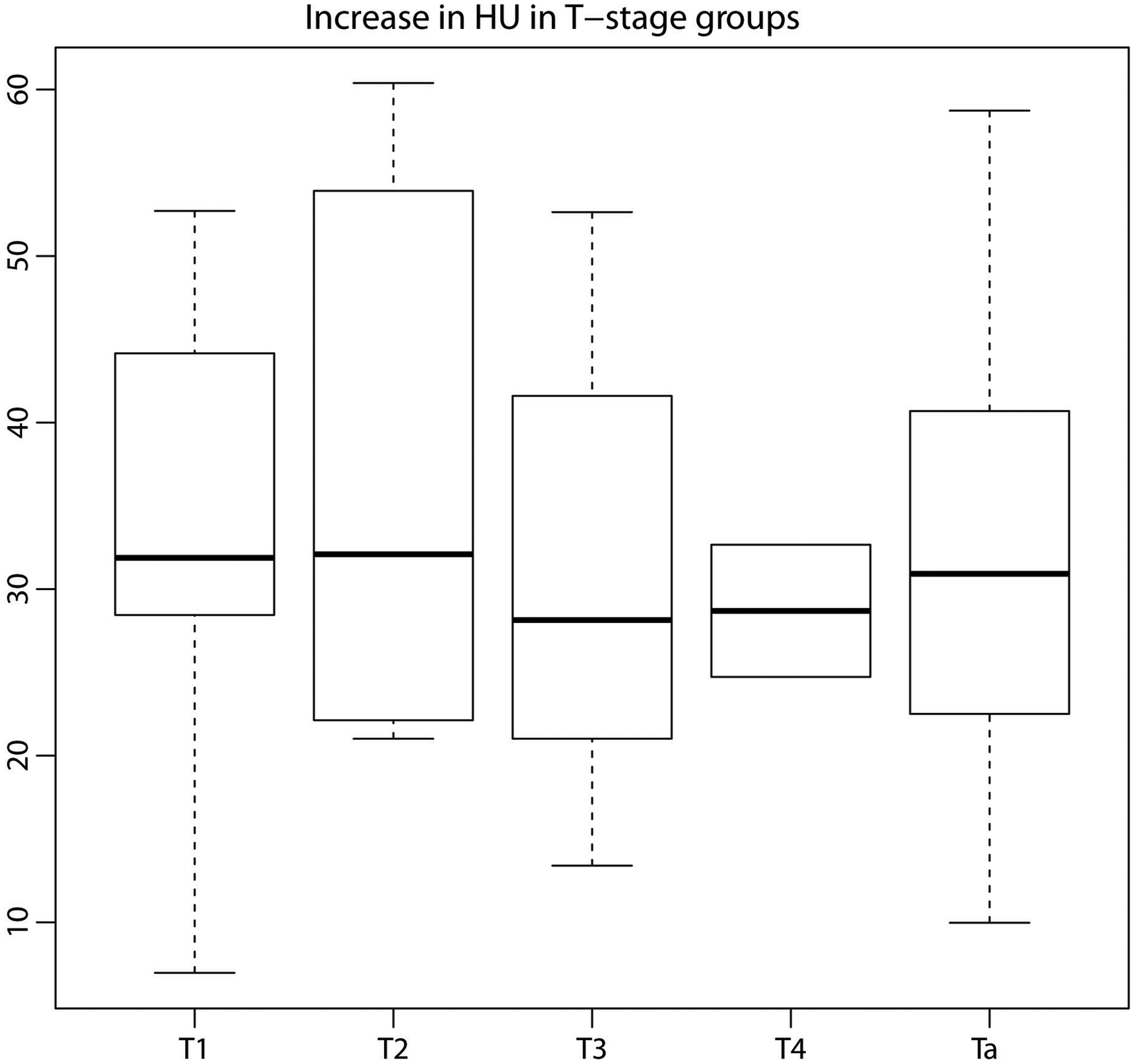
There was no statistically significant difference regarding: (i) the increase in HU; or (ii) the absolute HU on the enhanced run between the non-invasive or invasive tumor (Figs. 3 and 4). A lesion enhanced on average 32.32 HU (SD ± 12.71). Even when the T stages were taken into consideration there was no difference (Fig. 5).
The increase in HU. The average HU increase was 32.32 (SD ± 12.71). There is no statistical significance between the invasive and the non-invasive group. The absolute values of HU in invasive and non-invasive tumors. No statistical significance was found. The increase in HU related to the pathological T-stage. No statistical significance was found.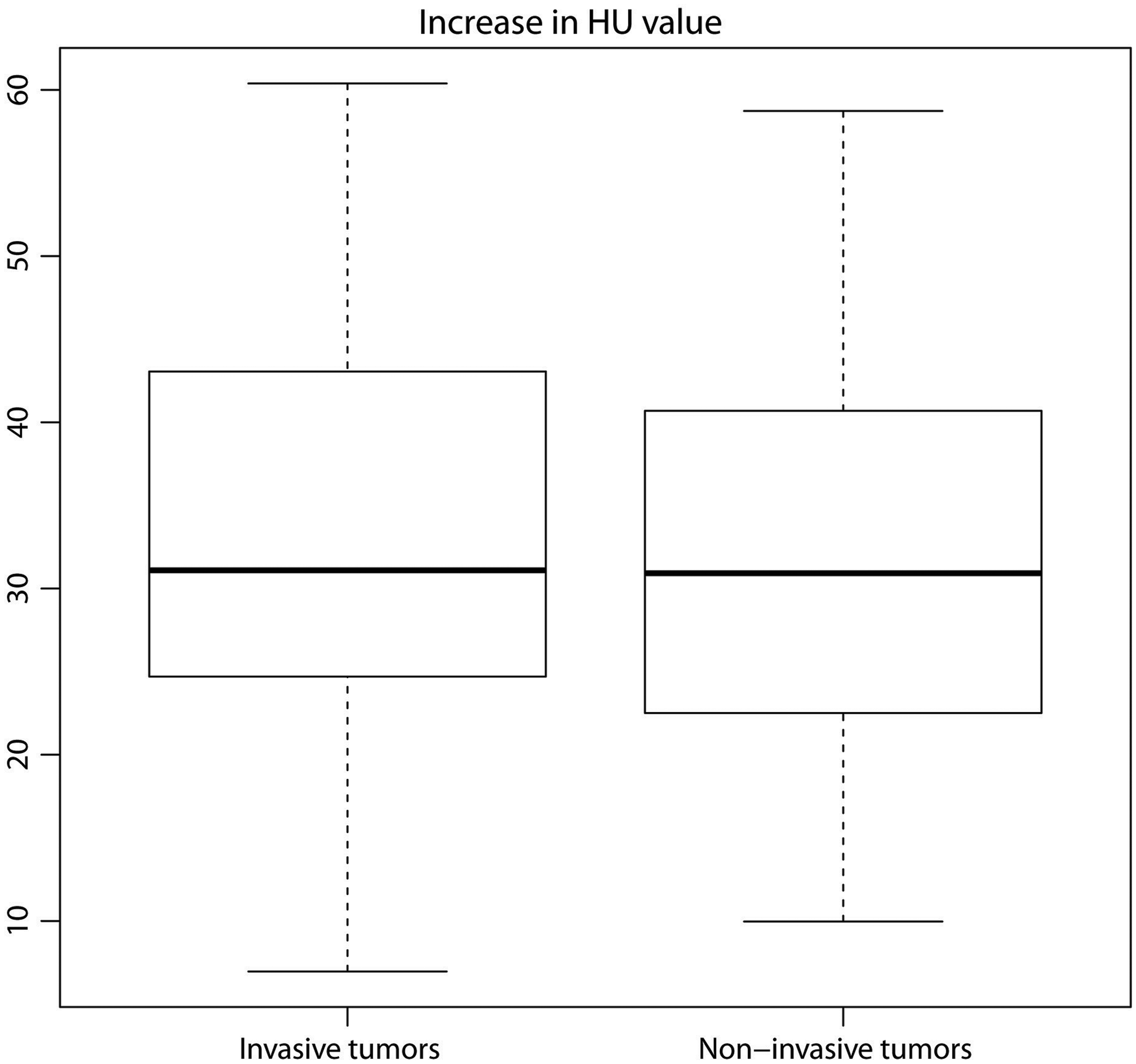
The mean difference and standard deviation of the paired results for the two readers were precontrast mean = 0.13, sd = 10.50 and postcontrast mean =−0.406, sd = 13.05, respectively. Bland-Altman plots showed that the majority of differences in HU were close to these small mean values and well within two standard differences. Thus the readers appear to be in reasonable agreement. A visual inspection of the histogram and normal Q-Q plots of the reader differences confirmed their normal distribution and consequently a Wilcoxon rank sum test was performed on both sets of reading, showing no statistical significant difference (precontrast P = 0.9966, postcontrast P = 0.9864) between the readers' results.
Pathology
T-stage and WHO grading is shown in Fig 6. Urine cytology was performed on 63 of the 69 patients. Tumor cells were found in 18.4% of the patients with an invasive lesion and none of the patients with a non-invasive tumor had tumor cells in their urine. Of the 63 patients, 47 had no tumor cells in their urine, seven had tumor cells, two had atypical cells, six had suspicious cells, and one had inflammatory cells.
Distribution of patients according to their T-stage and histology grading. Histology grading is an expression of the how well the cells are differentiated. If the cells are poorly differentiated there is a greater risk of development into invasive tumors and is graded “high” (shown in gray). If the cells are highly differentiated the tumor is graded “low” (shown in white).
Discussion
There were no statistical differences in demographic characteristics between the included patients and those who did not fulfill the inclusion criteria. To the best of our knowledge it is the first time the attenuation values have been studied in ureteral and renal pelvis tumors. Studies in other organs have shown promising results. Miyake et al. (8) were able to differentiate breast cancers using attenuation values and showed a significant higher HU values in the malignant tumors. El-Mokadem et al. (5) used attenuation measurements of renal cysts and found higher HU for clear cell RCC than for papillary RCC. Neither the absolute enhancement nor the relative enhancement, when measured 11 min after intravenous injection of 25 mL 400 mgI/mL and 70 s after intravenous administration of 50 mL 400 mgI/mL, could distinguish between invasive and non-invasive pelvic-urothelial tumors or the various pT-stages of the invasive tumors. Thus the attenuation of the tumor at split-bolus CTU cannot be used to characterize urothelial tumors in the upper urinary tract. Our hypothesis was that the invasive tumors, i.e. stage T1 or higher would enhance more than the non-invasive tumors because of the neovascularity that is needed for tumor growth. This was not the case since the attenuation value of the tumor lesion was not different in the non-invasive and the invasive group. Our results indicate that both invasive and non-invasive urothelial tumors are vascularized to the same extent. This favors the use of CTU instead of intravenous urography, as we can move from luminal diagnosis (defect in luminal contrast) to wall diagnosis (enhanced and enlarged wall). We do not need to focus on seeing luminal contrast all the way from the calyces to the vesico-ureteral ostium. This has been the scope of several studies (9–12).
The reasons why neither stage nor grade were related to attenuation are probably that tumors are very heterogeneous with respect to these parameters. For instance, some tumors may be high grade or invasive in only a very small area and yet they are classified as high grade and/or invasive. In some cases, urine cytology can provide the tumor type, mainly in the presence of high grade tumors, but it cannot distinguish between invasive and non-invasive tumors, although high grade tumor cells more often represent invasive tumors. In our study only 28.9% (11/38) of the patients with invasive tumors had had tumor cells or suspicious cells in the urine.
Hematuria, flank pain, and palpable masses are the classic triad of urologic symptoms. The present study shows that the most frequent symptom for referral to a CTU showing a tumor in the ureter or pelvis was hematuria. Macroscopic or microscopic hematuria is the most common symptom of a urothelial tumor in the upper urinary tract as it is present in 70–80% of the patients, whereas flank pain is the second most common symptom; it is found in 20–40% of the patients (13,14). In our study nearly 70% of the patients had macroscopic hematuria at time of referral, and only four patients presented with microscopic hematuria. Only four patients presented with flank pain and in no case a palpable masses were found.
Our aim was to investigate whether a simple additional measurement on the CTU with low radiation dose and low contrast dose could provide information about the nature of the mass in the ureter or kidney pelvis before an operation or biopsy was done. This was not the case and therefore the radiologist should not use the attenuation alone as a factor of invasiveness, i.e. malignancy. The patients still have to undergo risk-filled procedures to distinguish between invasive and non-invasive tumors.
A limitation of this study is the retrospective design and the fact that 51 examinations were not available electronically. However, the demographic data do not indicate that our study population differs from the complete population. Only one CTU technique was used, but it is doubtful whether later runs (after the injection of contrast medium), a single injection and higher doses may cause different results. The number of enrolled patients is small, but the lesion occurs infrequently compared to other tumors in the urinary tract.
Because we used a split-bolus CTU we cannot say if the tumors attenuation would have changed over time with later scans. It would require further studies and is beyond the aim of this study.
In conclusion, split-bolus CTU cannot be used to distinguish between invasive and non-invasive tumors in the upper urinary tract, but can be used for diagnosis of their presence. Positive cytology may help but it is only present in a minority of cases with invasive cancer. Symptoms and signs were neither helpful. Good non-invasive techniques to distinguish between invasive and non-invasive tumors in the upper urinary tract are strongly warranted.
Footnotes
Acknowledgements
The authors want to express their gratitude to Rasmus Hvass Hansen, PhD, for assistance with the statistics.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.