
Abstract
Background
Idiopathic osteosclerosis is a localized growth of compact bone with an unknown cause. This asymptomatic lesion is an insignificant finding and as such requires no treatment. It should be distinguished from other types of osteosclerosis created by inflammatory processes and systemic diseases.
Purpose
To determine the prevalence and distribution of idiopathic osteosclerosis in the jawbones in Iran and to compare this prevalence and distribution with other populations.
Material and Methods
This cross-sectional descriptive study was performed in the Dental School of Shahid Beheshti University of Medical Sciences, Tehran, between 2010 and 2011. Data were collected from the files of patients who underwent panoramic radiography for dental treatment. Location, shape, and relation between idiopathic osteosclerosis and the tooth as well as the resorption of the tooth involved were evaluated. Lesion distribution regarding age, gender, localization, shape, dental relationship, and root resorption was assessed using the chi-squared test.
Results
In total, 787 panoramic radiographs of 456 women and 331 men were assessed. Idiopathic osteosclerosis was detected in 75 (9.5%) patients. The prevalence of idiopathic osteosclerosis was significantly higher in the women (11.8% vs. 6.3%; P <0.01). The mean age of the patients with idiopathic osteosclerosis was 31.9 ± 17.9 years and 30.8 ± 13.3 years in the patients without idiopathic osteosclerosis. The distribution of idiopathic osteosclerosis in the mandible (97.3%), mostly in the premolar region, was significantly higher than that in the maxilla (2.7%).
Conclusion
Our results showed high frequencies of idiopathic osteosclerosis in Iran in comparison to some other countries.
Introduction
Idiopathic osteosclerosis is a localized growth of the compact bone that develops within cancellous bone with an unknown cause. This asymptomatic lesion is an insignificant finding and as such requires no treatment; therefore, it should be distinguished from other types of osteosclerosis created by inflammatory processes and systemic diseases (1,2). Idiopathic osteosclerosis has also been described as bone scar, bone island, bone whorl, enostosis, and focal periapical osteopetrosis (1–3). Idiopathic osteosclerotic lesions in the jaws are more common in the mandible than in the maxilla and are often seen in the premolar-molar area. Idiopathic osteosclerosis can be detected incidentally during routine radiographic examination of the jawbones and appears as a well-defined radiopacity abutting directly against the normal bone with no radiolucency or capsule. Usually the internal structure of idiopathic osteosclerosis is homogenous without any characteristic pattern. In rare instances, however, it is located periapical to the tooth and can cause external root resorption, although the tooth is still vital and the resorption process is self-limiting (4,5).
The prevalence of radiopaque lesions has been reported in the range of 3.3–31% (6–8). Given the different range of the prevalence of idiopathic osteosclerosis and lack of research in Middle Eastern populations, we performed this study to determine the prevalence and distribution of idiopathic osteosclerosis in the jawbones with respect to age, gender, localization, shape, dental relationship, and root resorption in Iran with comparison to other populations.
Material and Methods
Study population
This cross-sectional descriptive study was performed in the Dental School of Shahid Beheshti University of Medical Sciences, Tehran, Iran in 2010 and 2011. Data were collected from the files of patients who underwent panoramic radiography for dental treatment. Demographic data, including age and gender, were also recorded. The panoramic radiographs were observed initially by a trained senior dental student before subsequent review by a head and neck radiologist. In case of disagreement between the first two observers as to the outcome of an examination, another oral and maxillofacial radiologist was consulted.
Radiologic criteria for diagnosis of jawbone idiopathic osteosclerosis
The idiopathic osteosclerosis of jawbones was defined based on radiological criteria (3,9,10). The inclusion criteria comprised well-defined, round, ovoid or irregular, and radiodense lesions associated with normal bone with no surrounding radiolucency and with uniform internal radiopaque patterns. The exclusion criteria comprised lesions with the following characteristics:
Association with chronic inflammation defined as condensing osteitis; Mixed radiopaque and radiolucent lesions such as diffuse sclerosing osteomyelitis; Other benign fibro-osseous lesions such as periapical cemento-osseous dysplasia and focal cemento-osseous dysplasia; Increased lamina dura thickness around teeth showing marked malposition or serving as abutment for fixed bridges or partial dentures; Identifiable remnants of deciduous or permanent teeth; Radiopacities recognized as tori or exostosis; Solitary radiopacities seen in edentulous regions (since these might have been excessively ossified surgical sites); Patients with Gardner's syndrome, familial polyposis of the colon, and other diseases with bone metabolic disturbance (according to patient file data).
Idiopathic osteosclerosis and radiologic investigation
The location, shape, and relation between idiopathic osteosclerosis and the tooth as well as the resorption of the tooth involved were evaluated in patients diagnosed with idiopathic osteosclerosis.
The maxilla was divided into four parts consisting of the anterior, premolar, molar, posterior, and tuberosity. The mandible was divided into four parts consisting of the anterior, premolar, molar, and posterior and ramus. The shape of the lesion was described as round or irregular (Fig. 1). With respect to the relationship between idiopathic osteosclerosis and the tooth, the lesions were divided into two categories: separate from the tooth and along with the tooth, based on the Geist and Katz (10) criteria. A lesion was considered separate when it was clearly discrete from the tooth and lamina dura. The lesions along with the tooth were divided into three subgroups: (i) apical (if the masses were predominantly located around the root apices); (ii) inter-radicular (if the radiopacities were limited between the roots); and (iii) apical and inter-radicular (if the masses were located at the apices and represented significant extension between the roots).
Idiopathic osteosclerosis according to shape: (a) round and (b) irregular.
Statistical analysis
The data obtained from the survey were analyzed using SPSS software (version 15) for Windows (SPSS Inc., Chicago, IL, USA). For this purpose, the absolute frequency (numbers) and relative frequency (percentages) of the relevant variables such as gender, localization, and lesion shape were determined. Lesion distribution in terms of the patients' gender, localization, shape, dental relationship, and root resorption was assessed via the chi-squared test. The patient-related data and lesions are described via appropriate tables. A P value <0.05 was considered statistically significant.
Results
Distribution of patients according to gender and age.
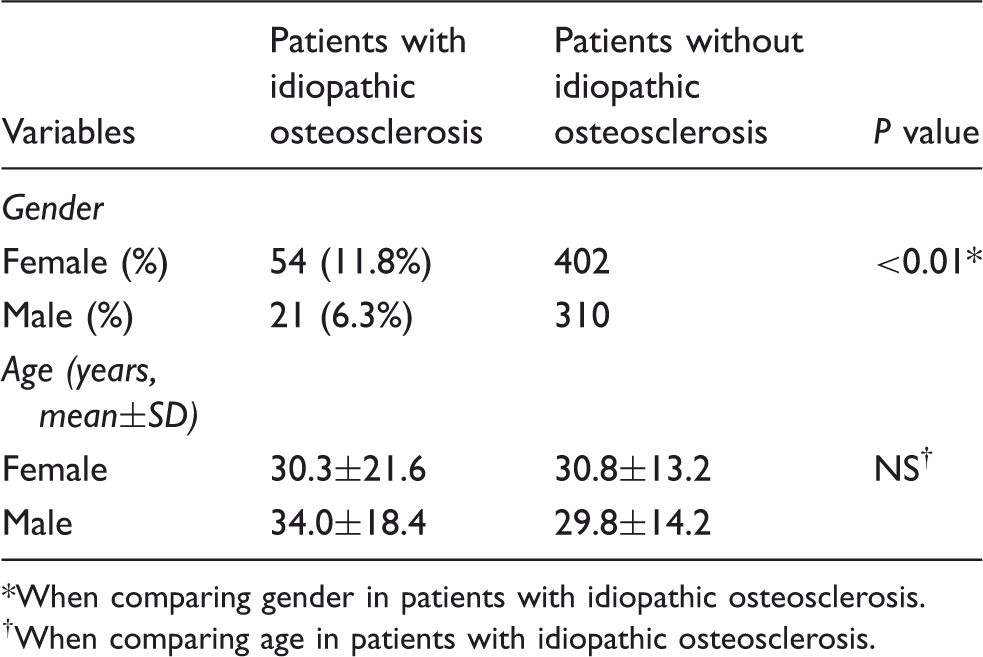
When comparing gender in patients with idiopathic osteosclerosis.
When comparing age in patients with idiopathic osteosclerosis.
The distributions of idiopathic osteosclerosis with respect to location, shape, and relationship to teeth.

Not significant.
Approximately half of the lesions, i.e. 40 (50.6%) lesions, were round in shape, and the other half (39 lesions) were irregular (49.3%).
According to the Geist and Katz (10) classification, 50 (63.3%) masses were separated from the tooth; and among the other 29 (36.7%), 16 (55.17%) lesions were in the apical, eight (27.6%) in the inter-radicular, and five (17.24%) in the apical and inter-radicular regions. Among the 29 mentioned lesions, root resorption was found in two cases.
The mean age was 31.9 ± 17.9 years in the patients with idiopathic osteosclerosis and 30.8 ± 7.9 years in the patients without it; the difference did not constitute a statistically significant difference.
Discussion
Different theories have been proposed for the formation of idiopathic osteosclerosis (5,10,11). Some researchers have suggested a reactive origin whose basis is the occurrence of mild inflammation and trauma during the replacement of the deciduous tooth with the permanent tooth (10), whereas others have posited a developmental etiology which primarily takes into account what tends to happen mostly during the first three decades of life (5,11). Geist and Katz (10) presented some radiopacities which could be described as idiopathic osteosclerosis. Miloglu et al. (12) concluded that these radiopacities might be developmental variations of normal bony architecture, unrelated to local stimuli, which could arise at any age and at any location in the jaws. Accordingly, idiopathic osteosclerosis can be deemed a developmental variation.
Summary of 12 reports on frequency and gender distribution of idiopathic osteosclerosis in literature sorted by frequency.

Statically significant
Data are not available.
Summary of 12 reports on distribution of idiopathic osteosclerosis according to most common appearance of the lesions.

Data are not available.
According to our results, the frequency of idiopathic osteosclerosis was significantly higher in women. Indeed, 11.8% of our female patients had idiopathic osteosclerosis, in contrast to 6.3% of their male counterparts (f/m ratio: 1.87; P <0.01). These results are in line with some other previously published studies (4,12); nevertheless, there are also other studies reporting that such differences are not statistically significant (9,13). Also, in the abovementioned local study in Iran (18), the frequency of idiopathic osteosclerosis in women was higher than in men. Although the prevalence of the female sex appears to be more prevalent in the majority of the reports in Table 3, there is no statistically significant difference in the proportion of the two genders with respect to idiopathic osteosclerosis. Therefore, there may be no actual predilection of idiopathic osteosclerosis for women.
We found the highest prevalence of idiopathic osteosclerosis in the third and fourth decades of life. Idiopathic osteosclerosis is an asymptomatic lesion detected during the evaluation of routine radiographs; consequently, the time of its incidence is not clear in a cross-sectional study. Prior longitudinal studies (11,15) have shown that the majority of cases with idiopathic osteosclerosis had no changes during follow-up periods. Geist and Katz (10) proposed response to increased occlusal forces as an etiological factor for the sclerosis of bone. In our study, we found that 63% of the lesions were separate from the tooth. In other words, these lesions were in areas where residual tooth fragments are not found and where the stimulatory effects of excessive occlusion would not be a factor. Miloglu et al. (12) reported that 40% of the idiopathic osteosclerosis lesions in their examination were separate lesions (unrelated to the region), while only 2% of the condensing osteitis lesions were separate from the tooth and the remaining 98% of the condensing osteitis lesions were tooth-associated (apical or apical and inter-radicular positions). These findings support the theory that idiopathic osteosclerosis lesions are developmental variations of normal bone architecture unrelated to a local stimulant such as residual root fragments and excessive occlusal forces and that condensing osteitis lesions could be considered reactive formations allied to teeth with caries, restoration, or pulpitis.
In the differential diagnosis of idiopathic osteosclerosis, root segments should be taken into account. Finding a periodontal ligament around the root segment or detecting a pulp canal can distinguish the root segment from the idiopathic osteosclerosis lesion. Gibilisco et al. (19) concluded that idiopathic osteosclerosis most frequently located in the premolar and molar areas might represent residual roots from deciduous molars, resorbed and replaced by sclerotic bone. In the study by Halse and Molven (11), residual roots, whose periodontal structures disappeared and later presented themselves as idiopathic osteosclerosis, were observed in three patients. Histological examination in the study by Henrikson et al. (20) demonstrated sclerotic bone containing a retained root in only one case. This indicates that although the majority of the cases diagnosed as idiopathic osteosclerosis cannot be explained by this factor, the phenomenon may be occasionally observed.
In the current study, 46.5% of the 77 idiopathic osteosclerosis lesions found in the mandible were located in the premolar, 45.5% in the molar, 3.9% in the anterior, and 3.9% in the ramus and posterior regions. Findings of the other studies have been summarized in Table 4.
First and foremost, among the potential limitations of the present study is selection bias, which is inherent in all retrospective radiographic studies that draw on a large number of radiographs of patients treated in a given facility during a given time period.
In conclusion, the high frequencies of idiopathic osteosclerosis in Iran (a Middle Eastern and Asian country), in comparison to some other countries, suggests a probable role of race difference in the prevalence of this type of lesions.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.