
Abstract
Background
Parotid tumor is an uncommon neoplasm. Only a few studies describing the sonographic features of pleomorphic adenomas and Warthin’s tumors have been published, and most of those reports are based on a relatively small number of cases.
Purpose
To define the sonographic characteristics of pleomorphic adenoma and Warthin’s tumor in the parotid gland.
Material and Methods
We retrospectively evaluated the sonographic features of 77 pleomorphic adenomas in 70 patients and 93 Warthin’s tumors in 61 patients. The features included tumor size, shape, border, echogenicity, and homogeneity, the presence of a cystic area, acoustic enhancement, and the grade and distribution of vascularization.
Results
Lobulated lesions were observed in 49 pleomorphic adenomas and 36 Warthin’s tumors. The lobulated shape was observed more frequently in pleomorphic adenomas than in Warthin’s tumors (P = 0.005). Cystic areas within lesions were detected in 16 (16/77, 20.8%) pleomorphic adenomas and 42 (42/93, 45.2%) Warthin’s tumors (P = 0.001). Of the pleomorphic adenomas, 77.9% had grade 0 or grade 1 vascularity, while 73.1% of Warthin’s tumors had grade 2 or grade 3 vascularity (P = 0.000). Flow was peripheral in 53.2% of pleomorphic adenomas. The frequencies of central perfusion and mixed perfusion in Warthin’s tumors were equal (47.3% vs. 47.3%, respectively). The differences in the vessel distribution between these two diseases was significant (P = 0.000).
Conclusion
Ultrasound imaging characteristics, including multiple occurrences, shape, intrinsic cystic change, and the grade and distribution of tumor vessels, can be used to differentiate pleomorphic adenomas from Warthin’s tumors.
Introduction
Parotid tumors are uncommon neoplasms that account for approximately 3% of all head and neck tumors (1). The majority of parotid tumors are benign, of which 85–90% are pleomorphic adenomas (2). Warthin’s tumors are the second most common benign tumors of the parotid gland, accounting for 6–10% of parotid tumors (3). Pleomorphic adenomas are associated with a 2–25% risk of malignant degeneration over time (4). The recurrence rates of pleomorphic adenoma were higher in patients who were treated by enucleation than in patients treated with parotidectomy, as well as in patients who had capsular rupture at surgery (5). For this reason, a partial parotidectomy is suitable for pleomorphic adenomas. In contrast, enucleation is sufficient for Warthin’s tumors because Warthin’s tumors usually do not recur (6). Therefore, it is important to make more exact differential diagnoses, not just differentiating malignant from benign lesions (7).
Ultrasonography (US) is frequently used as an initial diagnostic imaging modality for assessing parotid gland disease (8). US can determine the location, measure the size, and evaluate the perfusion patterns of the tumor in most cases, because most lesions are located superficially and, thus, are easily accessible. US may also provide some useful information on the differentiation of malignant from benign diseases, guide the biopsy of the suspected malignancy, and help determine the need for computed tomography (CT) or magnetic resonance imaging (MRI) in malignant or large masses (8).
To our knowledge, however, only a few studies have described the sonographic features of pleomorphic adenomas and Warthin’s tumors. Additionally, previous reports included relatively small numbers of cases (19–69 pleomorphic adenomas; mean, 36; 10–54 Warthin’s tumors; mean, 31) (4,9,10). Thus, the purpose of the current study was to further define the US features of pleomorphic adenomas and Warthin’s tumors and distinguish between the two types of parotid tumors in a larger case series.
Material and Methods
Between April 2005 and October 2012, US examinations were performed in 860 patients suspected of parotid lesions in our hospital. Of these patients, 131 were enrolled in the present study, including 70 cases (77 lesions) of pleomorphic adenomas and 61 cases (93 foci) of Warthin’s tumors, which were proven histopathologically after surgical excision; the other patients were excluded because they had no lesions on ultrasound images or lesions from other histological types.
The 70 patients with pleomorphic adenomas (34 men and 36 women) had a mean age of 43.4 years (range, 21–73 years); 66 of them had solitary lesions in the gland, three had multifocal lesions, and one had recurrent lesions.
The 61 patients with Warthin’s tumors (59 men and 2 women) had a mean age of 60 years (range, 31–81 years); 40 of them had solitary entities in the gland, and 21 showed multiple lesions (11 cases with unilateral multifocal masses, 6 cases with bilateral solitary masses, and 4 cases with a combination of bilateral masses and unilateral multifocal masses).
The US examinations were performed using color Doppler imaging devices (Logiq 9; GE HealthCare, Milwaukee, WI, USA; Philips IU22, Philips Medical System, Bothell, WA, USA). The probe frequency was in the range of 7–12 MHz. All patients were scanned by three radiologists (HTJ, JPL, and HLH) with >8 years of experience in the diagnostic ultrasound of the head and neck.
B-mode US evaluation of the lesions included the largest diameter (cm), shape (oval, lobulated, or irregular), border characteristics (>90% of the border is clear, well-defined, 50–90%, predominantly well-defined, or <50%, ill-defined), echogenicity (hypoechoic, isoechoic, or hyperechoic compared with the normal parts of the gland), homogeneity (homogeneous or heterogeneous), the presence of cystic areas (yes or no), and distal acoustic enhancement (yes or no). If multiple cystic changes in the lesions were observed, then the largest cystic area was regarded as the object of observation. On color Doppler imaging, tumor vascularization was graded on a 4-point system: grade 0, no visible tumor vessels; grade 1, consistent detection of one or two separate vessels; grade 2, consistent detection of three to five separate vessels; and grade 3, more than five separate visible vessels (11). The vessel distribution was classified as peripheral, central, or mixed.
All images were reviewed by two experienced radiologists (XYR and QZ) who were not aware of the pathologic diagnoses. They analyzed the features of images together to establish a consensus and to minimize inter-observer variability.
The differences between pleomorphic adenomas and Warthin’s tumors were compared using Student's t-test or a chi-square test. The significance level was set at a P value <0.05.
Results
The US appearance (i.e. the size and morphological features of US images) of 77 pleomorphic adenomas and 93 Warthin’s tumors were analyzed.
The largest diameters of the pleomorphic adenomas and Warthin’s tumors were 2.3 ± 0.8 cm (range, 0.4–4.7 cm) and 2.7 ± 1.3 cm (range, 0.4–6.7 cm), respectively. The difference in size between the two tumor types was not significant (P = 0.075).
US features of pleomorphic adenomas and Warthin’s tumors of the parotid gland.
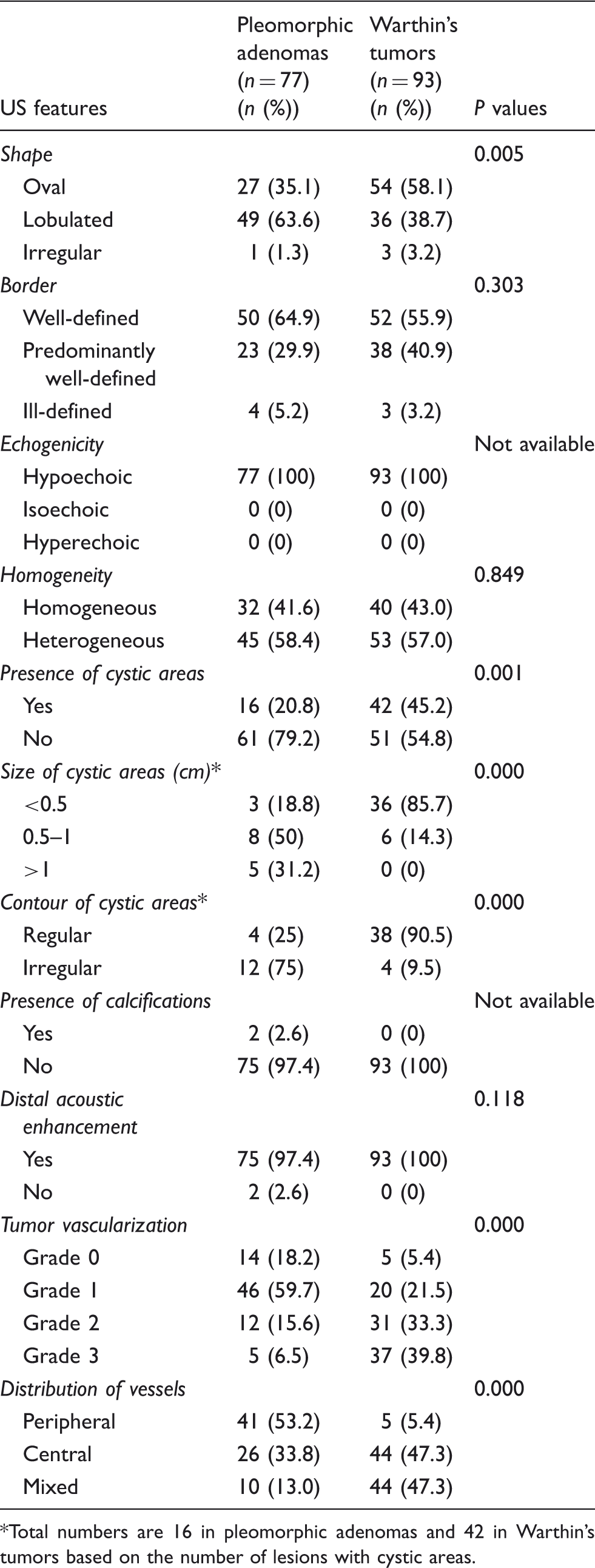
Total numbers are 16 in pleomorphic adenomas and 42 in Warthin’s tumors based on the number of lesions with cystic areas.
Forty-nine of 77 pleomorphic adenomas (63.6%) and 36 of 93 Warthin’s tumors (38.7%) presented as lobulated lesions. Twenty-seven pleomorphic adenomas (35.1%) and 54 Warthin’s tumors (58.1%) were oval. The lobulated shape was more frequent in pleomorphic adenomas than in Warthin’s tumors (P = 0.005; Fig. 1).
Grayscale ultrasound demonstrated a lobulated mass (arrows) with the homogeneous hypoechoic feature of pleomorphic adenoma.
Fifty pleomorphic adenomas (64.9%) and 52 Warthin’s tumors (55.9%) were well defined. Boundaries were predominantly well defined in 23 pleomorphic adenomas (29.9%) and 38 Warthin’s tumors (40.9%). Four pleomorphic adenomas (5.2%) and the remaining three Warthin’s tumors (3.2%) were poorly defined. No significant difference was observed in borders between the two types of tumors (P = 0.303).
All the lesions were hypoechoic (100%) compared with the normal parenchyma of the parotid gland on grayscale images. Calcifications were observed in two pleomorphic adenomas (2.6%). We did not find calcifications in any of the Warthin’s tumors. Forty-five pleomorphic adenomas (58.4%) and 53 Warthin’s tumors (57.0%) had a heterogeneous echo texture. Thirty-two of 77 (41.6%) pleomorphic adenomas and 40 of 93 (43.0%) Warthin’s tumors had a homogeneous echo structure. The difference in homogeneity between pleomorphic adenomas and Warthin’s tumors was not significant (P = 0.849). On grayscale images, cystic areas within lesions were detected in 16 of 77 (20.8%) pleomorphic adenomas and 42 of 93 (45.2%) Warthin’s tumors (P = 0.001; Figs. 2 and 3). The largest dimensions of the cystic areas in pleomorphic adenomas and Warthin’s tumors were 0.25–2.2 cm (mean, 1.11 ± 0.55 cm) and 0.20–0.80 cm (mean, 0.41 ± 0.17 cm), respectively. Thirty-six of 42 (85.7%) cystic areas in Warthin’s tumors were <0.5 cm, while three of 16 (18.8%) cystic changes in pleomorphic adenomas were <0.5 cm (P = 0.000). Most cystic areas (90.5%, 38/42) in Warthin’s tumors had regular contours, whereas 75% (12/16) of pleomorphic adenomas exhibited irregular contours (P = 0.000).
A 71-year-old man with a pleomorphic adenoma in the right parotid gland. Grayscale ultrasound showed an oval-shaped mass (thin arrows) with an anechoic (cystic) area (thick arrows). A 70-year-old man with a Warthin’s tumor in the right parotid gland. Grayscale ultrasound showed an oval-shaped mass (arrows) with multiple anechoic (cystic) areas (stars).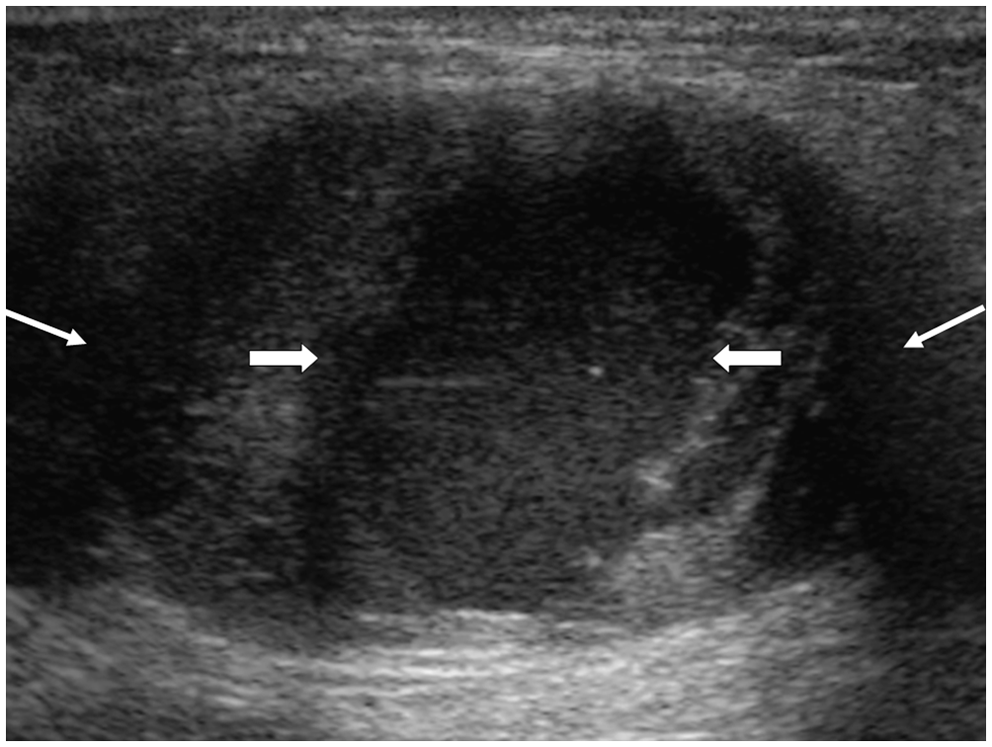

Seventy-five of 77 (97.4%) pleomorphic adenomas and all Warthin’s tumors presented with distal acoustic enhancement. The difference between the two groups in the presence of distal acoustic enhancement was not significant (P = 0.118).
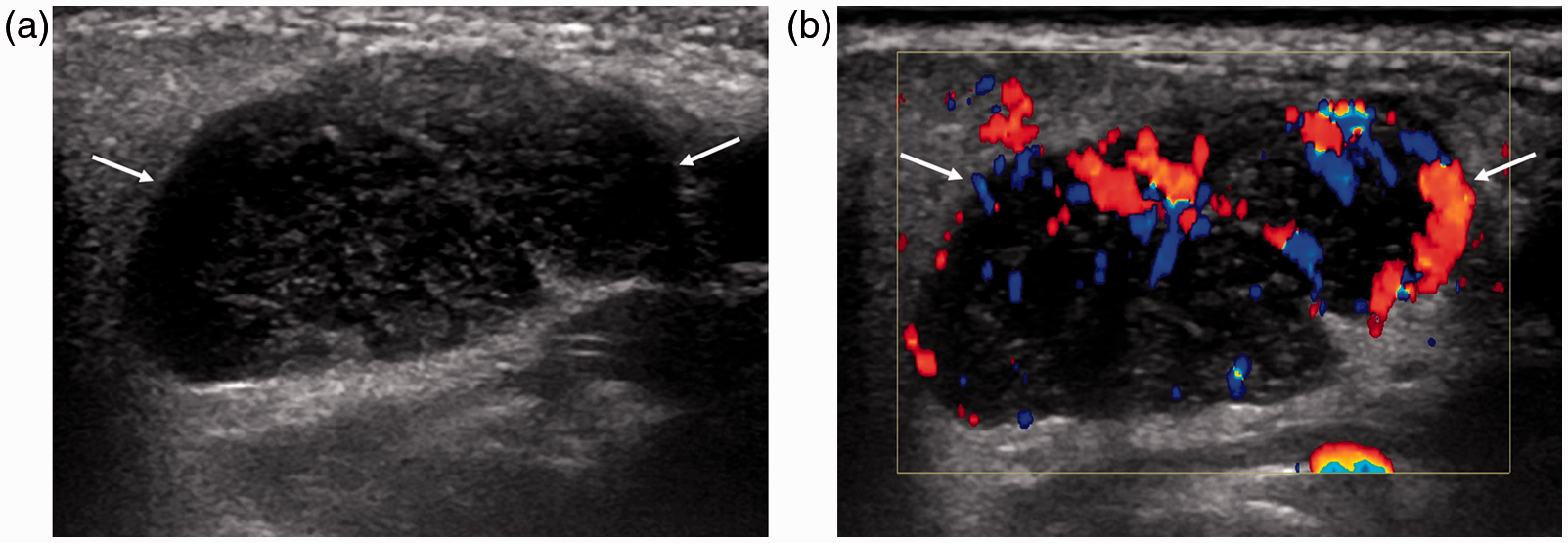
Most masses (77.9%) in pleomorphic adenomas had a vascularity of grade 0 or 1 (Fig. 4). In contrast, most masses (73.1%) in Warthin’s tumors had a vascularity of grade 2 or 3 (Fig. 5). Only five of 77 (6.5%) pleomorphic adenomas had grade 3 vascularity, and only five of 93 (5.4%) Warthin’s tumors had grade 0 vascularity. The difference in the grading of tumor vascularization between these two diseases was significant (P = 0.000).
A 27-year-old man with a pleomorphic adenoma. Grayscale ultrasound (a) demonstrated an oval-shaped, homogeneous hypoechoic mass (arrowheads). Color Doppler flow imaging (b) showed peripheral vascularity (grade 1). A 59-year-old man with a Warthin’s tumor. Grayscale ultrasound (a) demonstrated an oval-shaped heterogeneous hypoechoic mass (arrows). Color Doppler flow imaging (b) showed mixed vascularity (grade 3).
The flow was peripheral in 53.2% of pleomorphic adenomas. The proportions of pleomorphic adenomas with central and mixed perfusion were 33.8% and 13.0%, respectively. The proportions of Warthin’s tumors with central and mixed perfusion were both 47.3%. Peripheral flow was observed in only 5.4% of Warthin’s tumors. The differences in the distribution of vessels between pleomorphic adenomas and Warthin’s tumors was significant (P = 0.000).
Discussion
This study analyzed the sonographic features of pleomorphic adenomas and Warthin’s tumors of the parotid gland. We found that some characteristics of US imaging, such as multiple occurrences, shape, intrinsic cystic changes, and the grade and distribution of tumor vessels, could be used to distinguish between these two types of tumors.
In the current study, 21 of 61 patients (34.4%) with Warthin’s tumors presented with multifocal or bilateral lesions. In contrast, multifocality was noted in only 4.3% (3/69) of pleomorphic adenomas without bilateral lesions. Warthin’s tumors may be multiple or bilateral in 10–15% of patients, which is more frequent than in patients with pleomorphic adenomas (12). The multiple occurrences of Warthin’s tumors appear to be related to the embryologic origins of these tumors; there is no intra-glandular compartmentalization between the epithelial and lymphoid components during the early morphogenic stages of the parotid gland; Warthin’s tumors arise from heterotopic parotid tissue occurring within parotid lymph nodes (13,14). The majority of Warthin’s tumors are located in the tail of the parotid gland because several lymph nodes are present in the region (14). The histogenesis of pleomorphic adenomas remains unclear. Because of the predominance of multiple occurrences in Warthin’s tumors, multiple occurrences can be used to distinguish them from pleomorphic adenomas. Additionally, Warthin’s tumors were most common in elderly men compared with women and young men, while pleomorphic adenomas had no age or gender predilection in our study.
Zajkowski et al. (9) reported that the majority of pleomorphic adenomas (11 of 20 [55%]) had lobulated shapes. This result is consistent with the findings reported by Shimizu et al. (15), who concluded that lobular shape is the main characteristic feature of pleomorphic adenomas. The presence of lobulations had low sensitivity (42%) but high specificity (92%) for the identification of pleomorphic adenomas (16). Our results confirm that lobular shape was present more frequently in pleomorphic adenomas than in Warthin’s tumors (63.6% vs. 38.7%, respectively).
In our group, 42 of 93 (45.2%) Warthin’s tumors exhibited obvious cystic areas on grayscale images. Cystic areas were more frequently present in Warthin’s tumors than in pleomorphic adenomas (20.8%) (P = 0.001); this result is in agreement with most reports in the literature (4,9). We also found that larger (1.11 ± 0.55 cm) and irregular cystic areas (75%) were frequently observed in pleomorphic adenomas, whereas smaller (0.41 ± 0.17 cm) and regular cysts (90.5%) were usually detected in Warthin’s tumors. Furthermore, pleomorphic adenomas exhibited a maximal diameter of ≥0.5 cm in 81.2% patients, while Warthin’s tumors had a maximal dimension <0.5 cm in 85.7% of cases. These cystic areas might reflect the histopathological patterns of Warthin’s tumors, where an “epithelial layer lines the branching, cystic, or cleft-like spaces”, and might correspond to cystic degeneration or focal necrosis (17). Considering cystic areas as characteristic features of Warthin’s tumors on US images, the sensitivity, specificity, and accuracy of detecting cystic elements in Warthin's tumors were 46.4%, 100%, and 48.3%, respectively (4). The low sensitivity could be due to the small size of those cystic areas, which are typically < 2 mm, so they may not be easily identified by US imaging (15). Cystic changes originating from hemorrhage are often noted in larger pleomorphic adenomas (>3 cm) (18).
The hypothesis that various tumors of the parotid gland exhibit characteristic vessel patterns remains controversial (19). In the current study, we found a significant difference in vascularization between pleomorphic adenomas and Warthin’s tumors. Our results confirmed that most pleomorphic adenomas and Warthin’s tumors (88.8%, including 63 pleomorphic adenomas and 88 Warthin’s tumors) showed vascularization. The grade of vascularity in Warthin’s tumors was higher than that in pleomorphic adenomas. In our results, central and mixed perfusion occurred more often in Warthin’s tumors than in pleomorphic adenomas (47.3% and 47.3% vs. 33.8% and 13.0%, respectively). These findings are in agreement with the results of Bozzato et al. (20). Specifically, Bozzato et al. reported that pleomorphic adenomas tended to exhibit higher marginal perfusion, while Warthin’s tumors exhibited marked central perfusion. This important information explains why Warthin's tumors show rapid contrast enhancement while pleomorphic adenomas show a gradual increase in enhancement in dynamic CT examinations (21). These features are related to their histopathological features and vascular architecture. Typical histopathological features of pleomorphic adenomas include a large amount of myxoid matrix, rare epithelial components, and low microvessel counts. However, most Warthin’s tumors exhibit a high microvessel count density and high cellularity (22). Unlike the report of Yuan et al. (4), our study showed that the grade of tumor vascularity and the vessel distribution could be used to differentiate pleomorphic adenomas from Warthin’s tumors.
The other sonographic features of boundaries, echo pattern, homogeneity, calcification, and distal acoustic enhancement exhibited no significant differences between pleomorphic adenomas and Warthin’s tumors. Previously, a homogeneous structure was regarded as a characteristic feature of pleomorphic adenomas (7). In a recent study, Yuan et al. (4) reported that most pleomorphic adenomas (78.9%) and Warthin’s tumors (75.8%) had a slightly heterogeneous or heterogeneous echo texture. In our study, both pleomorphic adenomas (58.4%) and Warthin’s tumors (57%) had a heterogeneous echo texture. Higher resolution transducers would likely better depict complex tumor structures and lead them to appear more heterogeneous.
In addition to US, other imaging modalities such as CT and MRI are also commonly used to evaluate masses in parotid glands. Many studies have reported efforts to develop an imaging method that is capable of differentiating benign from malignant lesions. Various imaging techniques exhibit the same ability to perform differential diagnosis (23,24). The accuracy of detecting malignant lesions is 87% for CT, 87–93% for MRI, and 85–93% for US (10,25–27). US has a limited ability to visualize the deep lobe of the parotid gland, which is partially obscured by the body of the mandible bone. When this region must be visualized, CT and MRI are the modalities of choice. Fine needle aspiration cytology (FNAC), which provides a cytological diagnosis, is minimally invasive and easy to perform; however, the most significant problem with FNAC is that the procedure frequently does not obtain enough material, thus precluding evaluation (28). Preoperative biopsy involves significant risk, such as seeding or damaging the facial nerve (29). As an easily available, cost-effective, and non-radioactive imaging technique, US may be the first-step diagnostic method for the evaluation of parotid tumors. Sonoelastography (SE) has recently been applied to major salivary gland masses to differentiate benign from malignant lesions. Yerli et al. showed that pleomorphic adenomas are stiffer than Warthin’s tumors (30). However, recent results showed that SE was of no value in distinguishing pleomorphic adenomas from other parotid masses (31). The predictive value of the modern techniques for the differentiation of parotid lesions must be assessed in a larger series. Thus, the primary diagnostic modality for parotid gland tumors remains B-mode and color Doppler imaging.
This study has several limitations. Being a retrospective study, errors may have been made in the interpretation of previously saved static images, which have less clear margins and vessel contours than real-time scanning. The images were interpreted by two investigators together, preventing the assessment of inter-observer variability; however, this collaboration might be acceptable because inter-observer variability might be very small for individuals with >18 years of experience in head and neck imaging.
In conclusion, features of US imaging, such as multiple occurrences, shape, intrinsic cystic changes, and the grade and distribution of tumor vessels, can be used to differentiate pleomorphic adenomas from Warthin’s tumors.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.