
Abstract
Background:
The use of double-bundle and selective-bundle anterior cruciate ligament (ACL) reconstruction is increasing. Few studies have been conducted to determine the diagnostic efficacy of additional oblique views of knee magnetic resonance imaging (MRI) for grading ACL graft injury for double-bundle and selective-bundle ACL reconstructions.
Purpose:
To evaluate the diagnostic value of combining oblique coronal and sagittal imaging with orthogonal views for diagnosis of ACL graft failure after double-bundle or selective-bundle ACL reconstruction.
Material and Methods:
This retrospective study included 64 patients who underwent double-bundle or selective-bundle ACL reconstruction surgery and received oblique coronal and oblique sagittal MRI of the knee. Subjective scoring of the images was performed by two radiologists who assessed the possibility of ACL graft failure based on full length view, full width view, and margin sharpness according to a 4-point scale. Diagnostic performance for ACL graft failure based on orthogonal views alone, ACL views alone, and orthogonal views with additional ACL views was evaluated by calculating the sensitivity, specificity, and accuracy.
Results:
The full length scores and total scores on ACL views were significantly higher than those of orthogonal views. The specificities and accuracies of diagnoses were highest for a combination of orthogonal, ACL sagittal, and ACL coronal views.
Conclusion:
After double-bundle or selective-bundle ACL reconstruction, oblique sagittal and coronal images of the ACL provide better anatomic evaluation of the ACL than orthogonal views and specificity and accuracy of diagnoses were improved when oblique views were combined.
Introduction
The anterior cruciate ligament (ACL) is composed of two bundles, the anteromedial bundle and posterolateral bundle, which have distinct and complementary roles in stabilization (1). The aim of ACL reconstruction is reproduction of the stability of the native ACL. The use of double-bundle and selective-bundle ACL reconstruction is increasing because it reproduces native ACL anatomy and improves the ACL reconstruction outcome compared with traditional ACL reconstruction by the single anteromedial bundle technique. Several studies have shown the superiority of double-bundle ACL reconstruction in restoring intact knee kinematics, including rotations and translations (2,3). Regarding the imaging modality, several studies have shown that additional oblique magnetic resonance imaging (MRI) is helpful in the diagnosis of ACL tears and single-bundle reconstructed ACL graft injury (4,5). However, as far as we know, few studies have been conducted to determine the diagnostic efficacy of additional oblique views of knee MRI for grading ACL graft injury for double-bundle and selective-bundle ACL reconstructions.
The purpose of this study was to evaluate the diagnostic usefulness of combining oblique coronal and sagittal imaging (ACL views) with orthogonal views for evaluation of ACL graft failure after double-bundle and selective-bundle reconstruction procedures.
Material and Methods
Case selection and clinical diagnosis
This study was approved by our Institutional Ethics Review Board, and the requirement for informed consent was waived due to the retrospective study design. We retrospectively evaluated 64 patients who underwent double-bundle or selective-bundle ACL reconstruction surgery and knee MRI approximately 5 months after surgery between September 2010 and March 2012. The study sample included 12 women and 52 men (mean age, 31 ± 11 years; range, 16–57 years). One experienced orthopedic surgeon performed all operative treatments through double-bundle reconstruction or selective-bundle reconstruction. The mean follow-up time between the ACL reconstruction and the most recent follow-up in the outpatient department or the most recent postoperative MR examination was 279 ± 110 days. In the outpatient department, the same surgeon evaluated graft failures clinically using the pivot test and Lachman test. The result of the Lachman test was considered positive if anterior subluxation of the tibia from the femur could be elicited with knee joint flexion. Clinical findings such as response to physical therapy and course of clinical symptoms were also included in the final diagnostic analysis. Fifteen of 64 patients (23.4%) underwent second-look arthroscopy. The arthroscopic records revealed five cases with intact ACL graft, six with partially torn ACL grafts, and four with completely torn ACL graft. In clinical examinations, graft failure was diagnosed in three patients without arthroscopy. Therefore, 13 patients were ultimately diagnosed with graft failures.
MR parameters
Imaging parameters for the MR sequences.
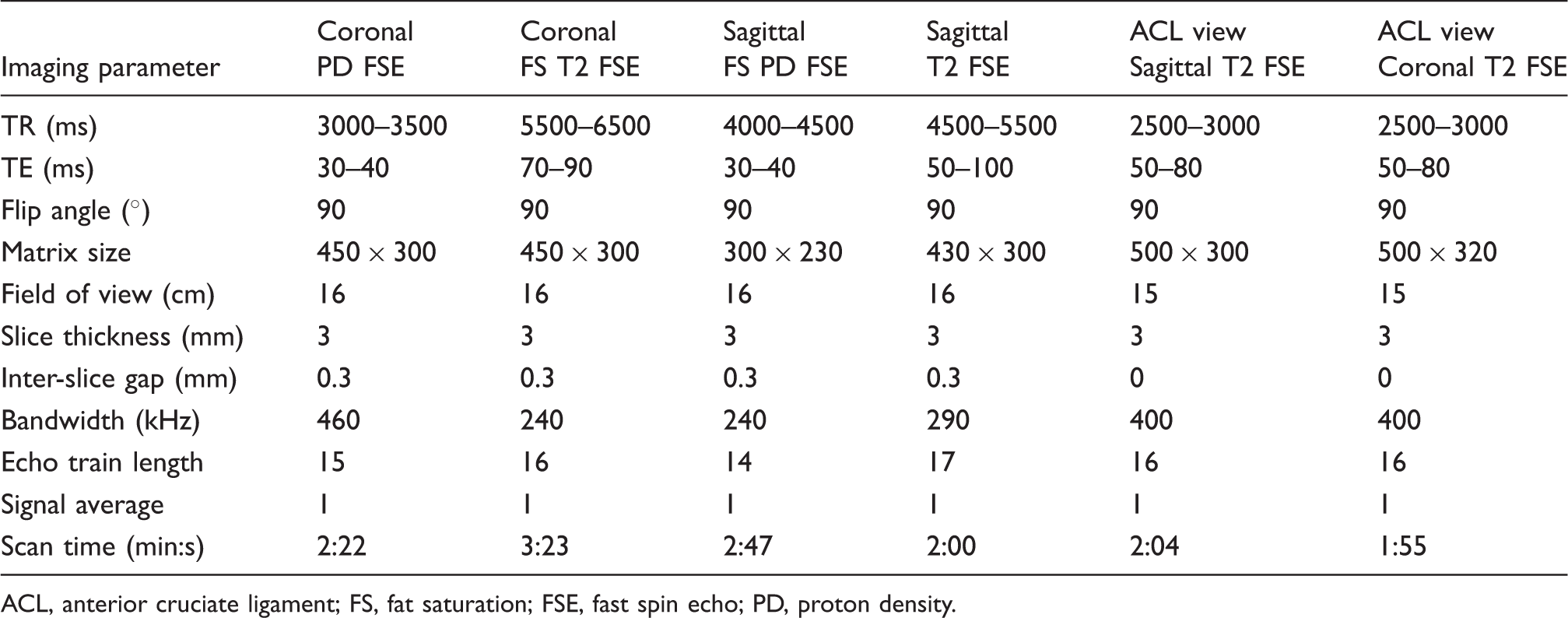
ACL, anterior cruciate ligament; FS, fat saturation; FSE, fast spin echo; PD, proton density.
Image analysis
MRI was performed at least 5 months (mean interval, 213 ± 72 days) after surgery, based on the normal ligamentization phase that occurs in immature grafts. The knee MR images were interpreted separately by two fellowship-trained musculoskeletal radiologists who were unaware of the radiologic reports or clinical history.
First, anatomic identification of ACL pathology on orthogonal MRI sequences (coronal T2-weighted [T2W] images and coronal and sagittal proton density images) and the ACL views was evaluated. Subjective scoring of the images was performed using abilities of discrimination through the entire length (full length), the entire width (full width), and margin sharpness according to a 4-point scale (0, poor; 1, fair; 2, good; 3, excellent). The entire length score implied whether the observer can perform longitudinal evaluation of the graft from femoral end to tibial end completely. The entire width score implied whether the observer can perform transverse evaluation of the graft from medial edge to lateral edge.
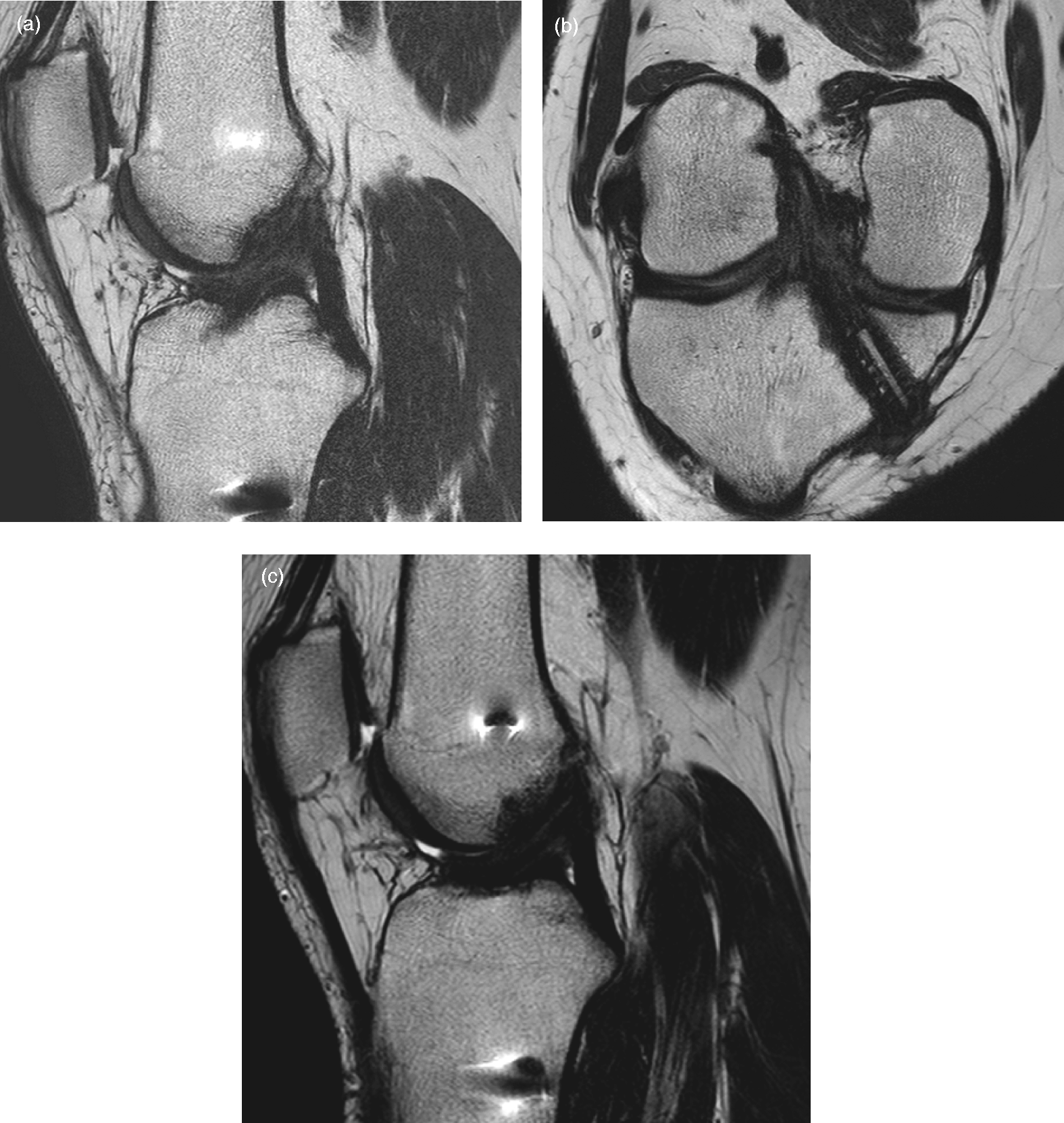
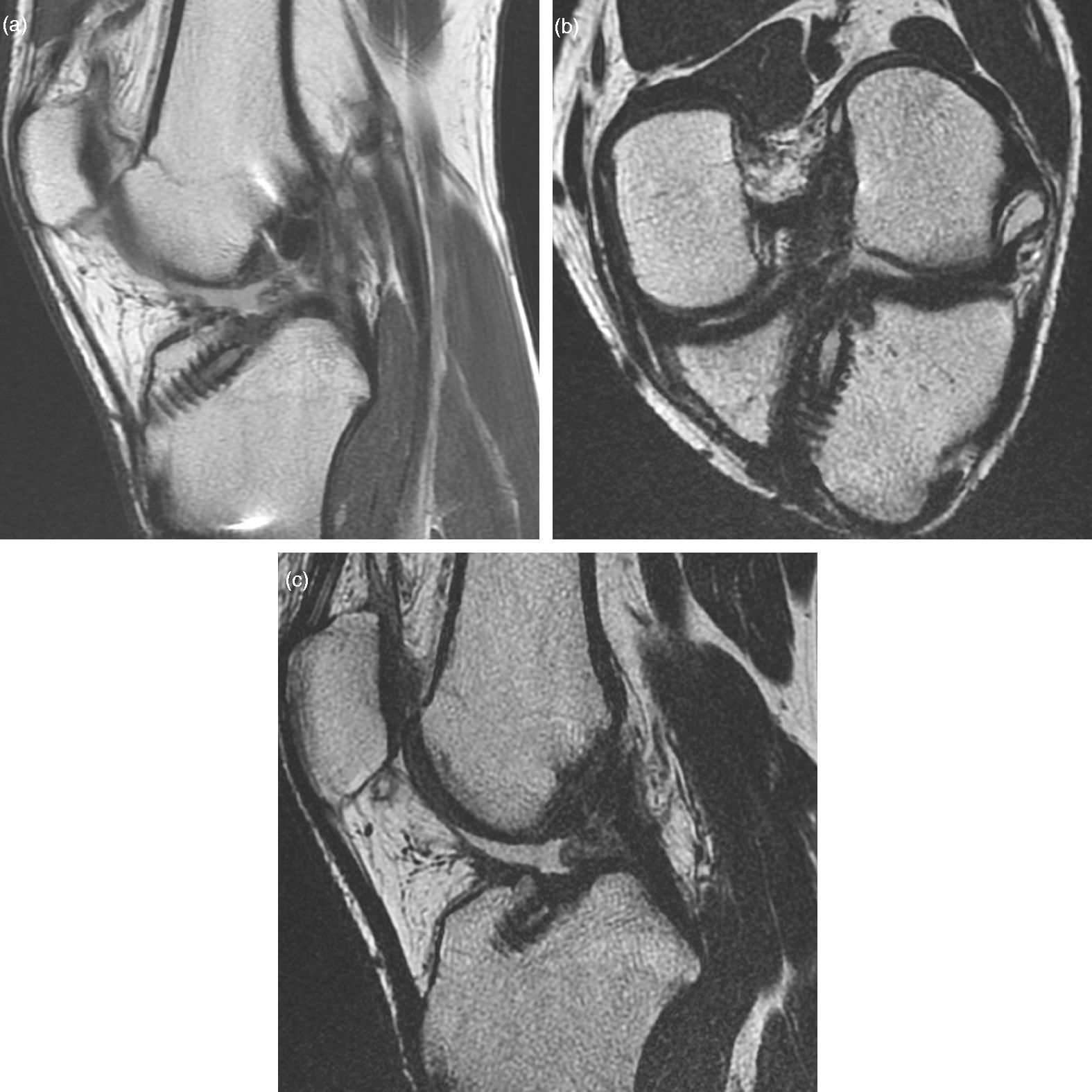
Second, diagnostic accuracy of the orthogonal MRI sequences and orthogonal MR images with additional ACL views was evaluated. The reconstructed ACL was considered intact if two bundles of low signal intensity were observed (Figs. 1 and 2). The reconstructed ACL was considered to have a partial graft tear if there was a focal area of increased signal intensity in the intact graft fibers on T2W or proton density images. The reconstructed ACL was considered to have a complete graft tear if MRI findings included an absence of intact graft fibers and a fluid-filled defect (Figs. 3–5). Partial tears and complete tears in MRI were regarded as graft failure.
Postoperative MRI of a 40-year-old man performed 6 months after arthroscopic selective bundle ACL reconstruction of the left knee due to ACL tear. (a) Oblique sagittal T2W image (TR/TE, 2500/70) of the ACL was obtained in the plane parallel to the medial border of the lateral femoral condyle on an orthogonal coronal image using 2-mm slice thickness. This image shows the full length of the reconstructed ACL. (b) Oblique coronal T2W MR image (TR/TE, 2800/70) of the ACL obtained in the plane parallel to the course of the femoral intercondylar roof based on the conventional sagittal image. This image shows the full length of the reconstructed ACL. (c) Orthogonal T2W sagittal image (TR/TE, 5500/60) of the ACL does not show the entire reconstructed ACL compared with the oblique sagittal image. Second-look arthroscopy revealed no graft failure. Postoperative MRI of a 27-year-old woman performed 9 months after double-bundle ACL reconstruction of the right knee due to ACL tear. (a) Oblique sagittal T2W MR image (TR/TE, 2500/80) of the ACL shows intact bundles. (b) Oblique coronal T2W MR image (TR/TE, 2800/60) of the ACL shows intact bundles. (c) Orthogonal coronal proton density MR image (TR/TE, 3000/40) of the ACL shows two intact bundles. Second look arthroscopy revealed graft failure. Postoperative MRI of a 36-year-old man performed 8 months after arthroscopic selective bundle ACL reconstruction of the right knee due to ACL tear. (a) Orthogonal sagittal T2W MR image (TR/TE, 5500/70) shows high signal intensity lesion in the reconstructed ACL, implying graft failure. (b) Oblique coronal T2W MR image (TR/TE, 2500/60) of the ACL shows intact bundles with low signal intensity. (c) Oblique sagittal T2W MR image (TR/TE, 2600/50) of the ACL also shows intact bundles of low signal intensity. Arthroscopy did not show graft failure. Postoperative MRI of a 23-year-old man performed 7 months after selective bundle ACL reconstruction of the right knee due to ACL tear. (a) Oblique sagittal T2W MR image (TR/TE, 2800/70) of the ACL shows high signal intensity in the reconstructed ACL, suggesting graft failure. (b) Oblique coronal T2W MR image (TR/TE, 2800/70) of the ACL also shows high signal intensity in the reconstructed ACL. (c) Orthogonal sagittal T2W MR image (TR/TE, 4400/30) of the ACL shows two intact bundles with low signal intensity. Second look arthroscopy showed graft failure. Postoperative MRI of a 16-year-old man performed 10 months after double-bundle ACL reconstruction of the left knee due to ACL tear. (a) Orthogonal sagittal proton density MR image (TR/TE, 4400/40) of the ACL shows a disrupted reconstructed ACL. (b) Oblique coronal T2W MR image (TR/TE, 2800/70) of the ACL shows disruption of reconstructed ACL. (c) Oblique sagittal T2W MR image (TR/TE, 2600/70) of the ACL shows disrupted reconstructed ACL. Following second-look arthroscopy, complete tear of the reconstructed ACL was diagnosed.


Statistical analysis
Anatomic identification on orthogonal and ACL views, as graded by the two radiologists, was compared. To determine the statistical significance of the anatomic identification scoring, Wilcoxon signed-rank tests were used. Inter-observer agreement was analyzed using an intra-class correlation coefficient (ICC). ICC interpretation was as follows: values <0.40 indicate poor agreement; values of 0.40–0.75 indicate fair-to-good agreement; and values >0.75 indicate excellent agreement (6). Inter-observer agreement of diagnostic performance was analyzed using kappa statistics. The kappa value was interpreted as follows: poor, k <0.1; slight, 0.1 ≤ k ≤ 0.2; fair, 0.2 < k ≤ 0.4; moderate, 0.4 < k ≤ 0.6; substantial, 0.6 < k ≤ 0.8; and almost perfect agreement, 0.8 < k ≤ 1 (7). Diagnostic performance of the orthogonal views, ACL views, and orthogonal images with additional ACL views was evaluated using the sensitivity, specificity, and accuracy for diagnosing an ACL graft failure. Arthroscopically and clinically confirmed (positive on pivot test and Lachman test and aggravating clinical course despite of the non-surgical therapy) graft failures were used as the reference standard and the values were statistically analyzed using the McNemar test. Statistical analyses were performed using PASW software version 18.0 (IBM, Armonk, NY, USA), and P values ≤0.05 were considered to be statistically significant.
Results
Intra-class correlation coefficients of anatomic identification scores.

*Full length = abilities of discrimination through entire length.
†Full width = abilities of discrimination through entire width.
‡Orthogonal view = coronal and sagittal images.
Mean scores for anatomic identification of reconstructed ACL on ACL views and orthogonal views.
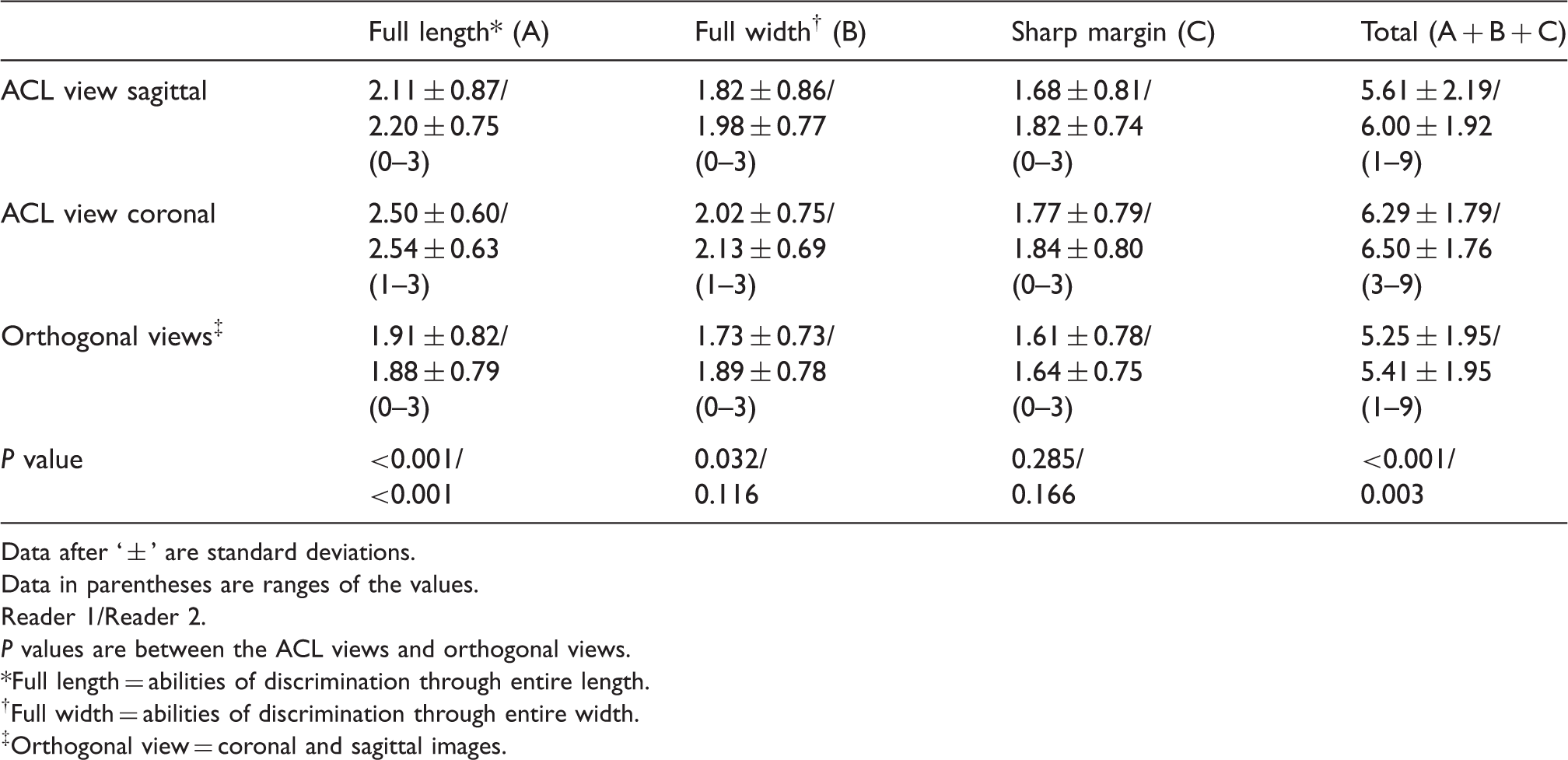
Data after ‘ ± ’ are standard deviations.
Data in parentheses are ranges of the values.
Reader 1/Reader 2.
P values are between the ACL views and orthogonal views.
*Full length = abilities of discrimination through entire length.
†Full width = abilities of discrimination through entire width.
‡Orthogonal view = coronal and sagittal images.
Inter-observer agreement for diagnostic performance.
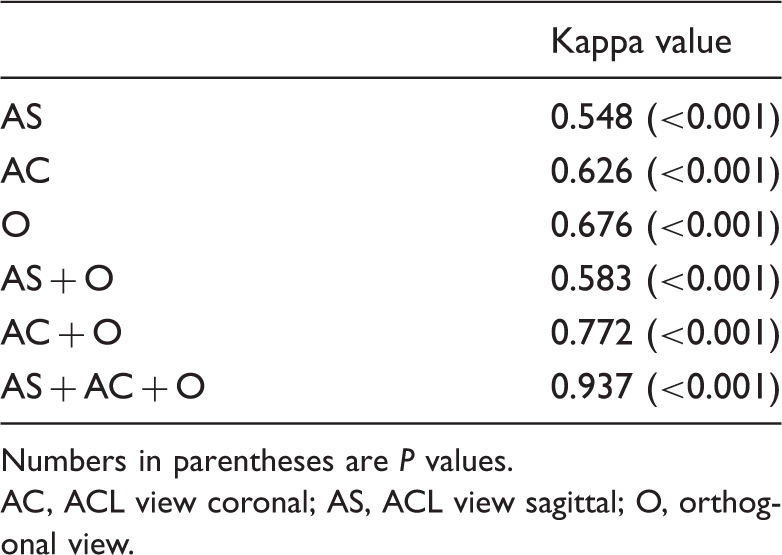
Numbers in parentheses are P values.
AC, ACL view coronal; AS, ACL view sagittal; O, orthogonal view.
Sensitivity, specificity, and accuracy of ACL views and orthogonal views in diagnosing ACL graft failure.
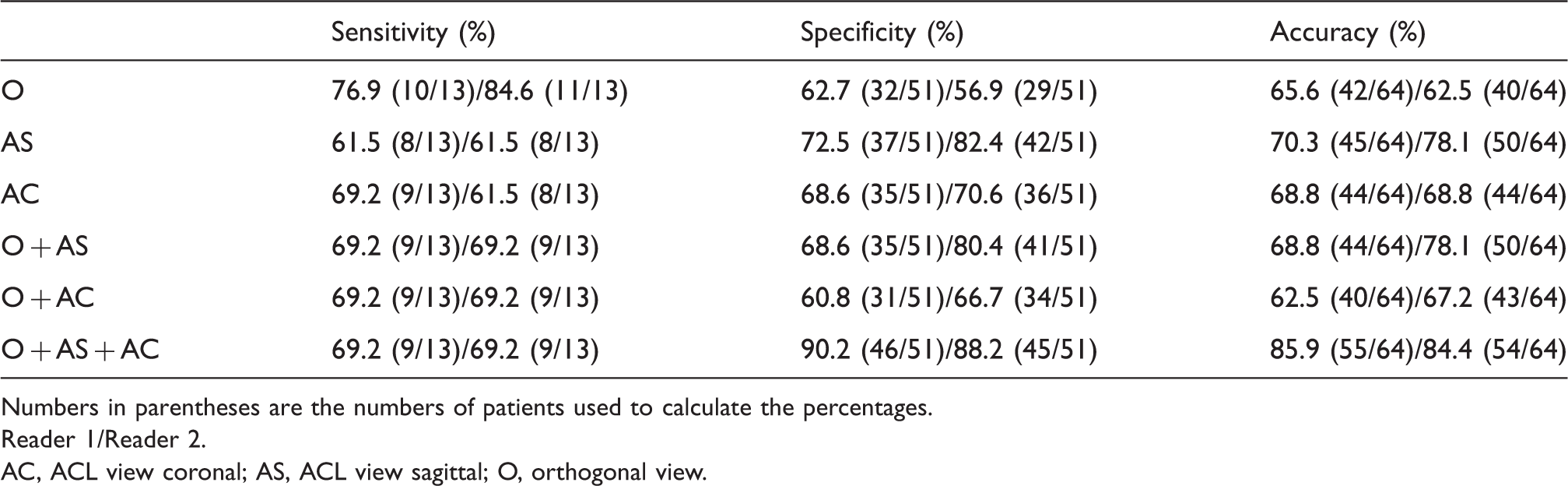
Numbers in parentheses are the numbers of patients used to calculate the percentages.
Reader 1/Reader 2.
AC, ACL view coronal; AS, ACL view sagittal; O, orthogonal view.
P values for sensitivity, specificity, and accuracy between the ACL views and the orthogonal views in diagnosing ACL graft failure.
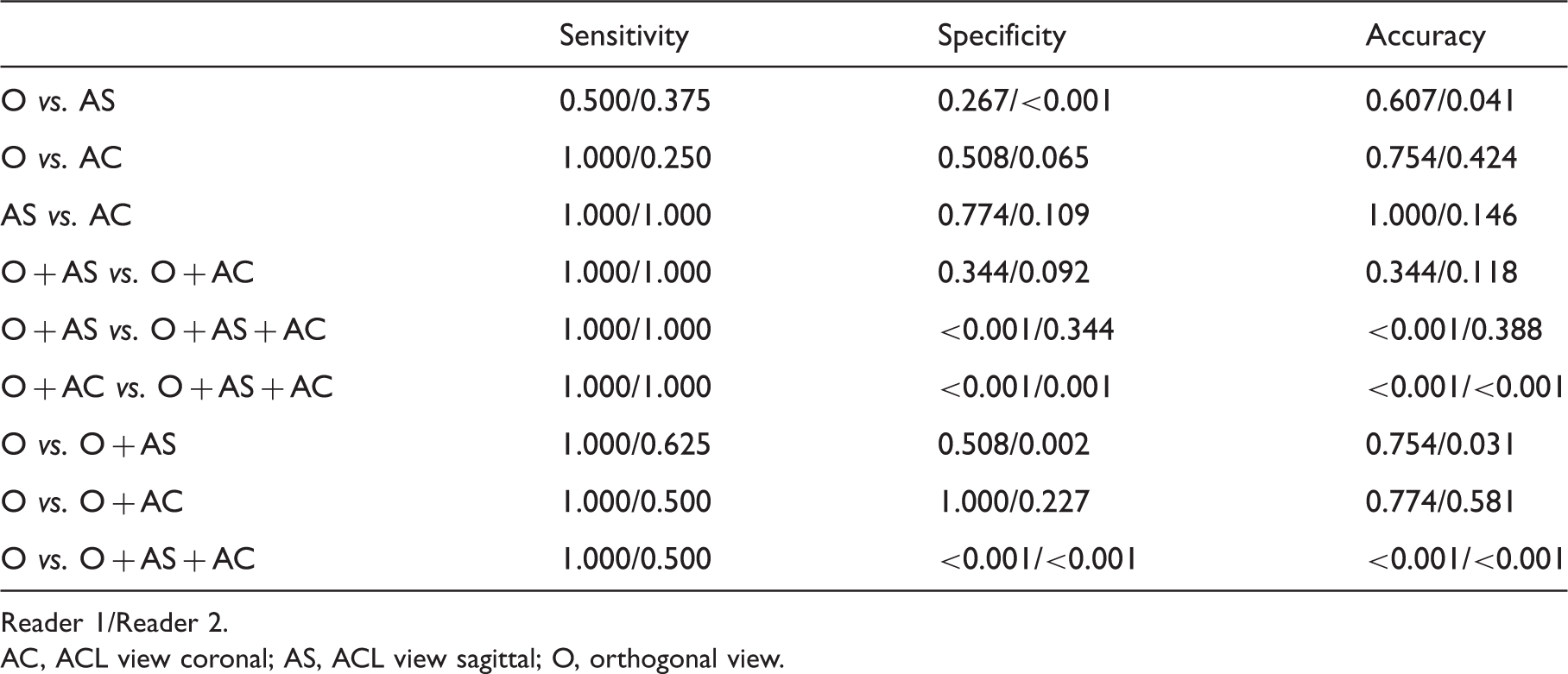
Reader 1/Reader 2.
AC, ACL view coronal; AS, ACL view sagittal; O, orthogonal view.
Discussion
The ACL is composed of two functionally distinct bundles named according to their tibial insertion, the anteromedial and the posterolateral bundles (8). The complex anatomy of the ACL makes it difficult to see the whole course on an orthogonal view of MRI, therefore, Staeubli et al. (9) recommended using the oblique coronal view of MRI for visualization of the entire anatomic course of the native ACL. For the native ACL, several studies have shown that an additional oblique view improves the diagnostic efficacy of ACL tears with respect to specificity and accuracy (4,10–12). For ACL grafting, Moon et al. (5) have shown that the additional oblique coronal view of the MRI of the knee improves both the diagnostic accuracy and confidence for grading ACL graft injury. However, they enrolled only patients who underwent single-bundle reconstruction and included only an additional oblique coronal view, whereas we added two ACL views, the oblique coronal and oblique sagittal views. Recently, the number of double-bundle and selective-bundle ACL reconstructions being performed has increased compared with traditional single-bundle ACL reconstruction, especially in athletic or young patients, because several studies have reported that double-bundle ACL reconstruction shows improved outcomes and restores intact knee kinetics by reproducing the specific native bundle anatomy (2,3). Several studies have included oblique views of the knee MRI in the evaluation of healthy ACL grafts after double-bundle or selective-bundle ACL reconstructions (13,14). Casagranda et al. (13) added only the oblique coronal view, whereas Kiekara et al. (14) included both oblique sagittal and coronal views for evaluation of reconstructed ACL. The anteromedial and posterolateral bundles are parallel to each other when the knee is full extended, but cross each other when the knee is in 90° of flexion (15). Thus, when the knee joint is flexed, the two bundles make an angle between each other and MRI performed in the neutral position might show differences in the angle between the bundles. This is why additional variant oblique views in MRI are needed to evaluate the two bundles after reconstruction. The ACL graft remodels within between 4 and 8 months after surgery, the so-called “normal ligamentization phase”. During this period, the graft undergoes resynovialization and revascularization, which results in increased signal intensity within the graft (13). Therefore, this study included patients who underwent MRI at least 5 months after surgery to avoid confusion between normal ligamentization and partial tears. Regarding the scores of anatomic identification of the ACL graft with each additional view, although both ACL views showed higher scores than orthogonal views statistical significances were seen only in full length and total scores (Table 3). Moon et al. (5) suggested that oblique coronal views readily show the transverse width of the ACL graft because both the medial and lateral margins of the graft are clearly visualized and ferromagnetic artifacts are reduced by avoiding fixation devices in the plane, whereas artifacts from these devices obscure the femoral and tibial bone tunnel images on the orthogonal view. In our study, the width discriminating abilities of the oblique coronal and sagittal views did not show statistical significance although the full length discriminating abilities were superior to those of the orthogonal view. Moon et al. (5) attributed the superior abilities of full length discrimination of the oblique view to the fact that the oblique coronal angle is similar to the oblique lie of the ACL graft, which is less subject to volume averaging. From the results for sensitivity, specificity, and accuracy, we can assume that combining the additional ACL views with the orthogonal view might be more specific and accurate than the orthogonal view only for the diagnosis of double-bundle ACL graft failure. The sensitivities by using additional views rather decreased slightly. We attribute these to the fact too many images can mask subtle signal change of the ligament. In one case, we could find focal bright signal in the graft on orthogonal images however, as the graft appear intact on both orthogonal views, the final diagnosis of entire images was normal.
Some limitations of our study should be mentioned. First, our study included only a small number of patients with graft failures. Only 13 cases (20.3%) among a total of 64 patients were diagnosed as graft failure. Second, this study lacked surgical confirmation of graft failure. Only 15 (23.4%) patients underwent second-look arthroscopy, and graft failure was confirmed in 10 of these 15 patients. Third, we did not use the exactly same imaging parameters for all planes (different TR/TE, different inter-slice gap), which could influence on the depiction of the graft. Finally, our study lacked objective quantitative analysis of the anatomic identification in reconstructed ACL. Instead, we depended on a subjective scoring system; however, as the ICCs between two readers were very high the scores are presumably quite accurate.
In conclusion, oblique sagittal and coronal views of the ACL provide better anatomic evaluation than orthogonal views in double-bundle or selective-bundle ACL reconstructions and improve the specificity and accuracy for diagnosing double-bundle graft failure when combined with orthogonal views although cannot improve sensitivity. Thus, oblique sagittal and coronal views of the ACL may be helpful in distinguishing equivocal cases of possible double-bundle graft failure.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.