
Abstract
Several imaging options are available today to diagnose endometriosis. Currently, the two techniques most used are sonography and magnetic resonance imaging (MRI). Three-dimensional (3D) sonography has proved to be particularly sensitive in the diagnosis of endometriosis. In recent years, MRI has emerged as a high reproducible method to explore endometriosis; moreover, its capability to evaluate tissue signal is an extremely powerful system in the differential diagnosis with other pathologies and for the identification of malignant degeneration. The purpose of this paper is to present the state-of-the-art of MRI of endometriosis by performing a review of the literature and showing the epidemiology, pathogenesis, and classification of endometriosis. In this work, the technique that should be used, MR findings of endometriosis and the principles of differential diagnosis are explained.
Introduction
Endometriosis is an inflammatory disease characterized by the presence of functional endometrium-like tissue in ectopic locations outside the uterine cavity, primarily on the pelvic peritoneum and ovaries (1,2). In some locations, endometrial tissue is associated with the presence of fibrous tissue (3). Its prevalence is up to 10% in women between 15–40 years and its incidence in relatives of affected women is up to seven times that in women without a family history (4,5). The etiology and pathogenesis of endometriosis are still unclear and are probably multifactorial and the mechanism of its development is unclear (1).
Clinical features and therapy
The main clinical features of endometriosis are chronic pelvic pain, dyspareunia, and infertility (1). Therefore, this disease has a negative impact on everyday life and sexual life (6). Symptoms of endometriosis usually appear after menarche and vanish after menopause and occasionally, a recto-vaginal nodule remains symptomatic in a postmenopausal woman and this fact suggests that its persistence is independent of ovarian estrogen secretion (7).
The inflammation involved in endometriosis can stimulate nerve endings in the pelvis and thereby cause pain, impair the function of uterine tubes, decrease receptivity of the endometrium, and hinder development of the oocyte and embryo (8). Endometriosis can also cause infertility by physically blocking the fallopian tubes (1). The treatment of infertility caused by endometriosis is surgical removal of endometriotic tissue or assisted reproductive technology, whereas the usual treatment of pain is a combination of medical suppression of ovulation and surgery. Usually, peritoneal endometriosis is asymptomatic whereas deep pelvic endometriosis is frequently associated with infertility, dyspareunia, pelvic pain, dysmenorrhea, and urinary tract symptoms. Unusual findings such as pneumothorax and epistaxis may be seen when endometriotic implants occur in atypical locations outside the pelvis (9).
Malignant transformation of endometriosis
Although endometriosis is usually a benign pathology, this condition is sometimes associated with malignant ovarian neoplasm, (endometrioid and clear cell adenocarcinomas); malignant transformation is a documented but uncommon (<1%) complication of endometriosis (10). The prevalence of malignancy in ovarian endometriosis is 0.6–1.0% (10) whereas the prevalence of endometriosis in patients affected by ovarian cancer is in the range of 4–15% (11). The highest prevalence is found in Japan (11).
Malignant transformation affects women years younger than those affected by de novo ovarian cancer and 75% of malignant transformations arise from the ovary (12). Twenty-five percent of malignant transformations arise from extra-ovarian lesions (endometrioid tumors and sarcomas). The most common histopathologic subtypes arising in ovarian endometriomas are the clear cell and endometrioid carcinoma whereas extra-ovarian lesions are commonly sarcomas or endometrioid. The reason why endometriosis, that is usually a benign process, may shift to malignant transformation is not clear: it has been hypothesized that estrogen might play a role in the development of malignancy by some authors (13).
Magnetic resonance imaging technique
The magnetic resonance imaging (MRI) examinations can be performed at different times during the menstrual cycle since there is no evidence that MRI performed during the menstrual period has greater diagnostic accuracy (9). Usually, patients had been fasting for 6 hours and were asked to perform an intestinal toilette (water enema) before examination (14). Patient preparation required a moderately filled bladder; this is required to change the angle of uterine anteversion, leading to better evaluation of the pelvic structures. Moreover, a moderately filled bladder displaces the bowel superiorly, by reducing the artefacts from bowel motion (14).
For the evaluation of deep endometriosis it was suggested (15) to introduce intra-vaginal aqueous gel (50 mL) to distend the vaginal cavity and better explore the vaginal fornices and the retrocervical area. In the presence of symptoms that may be related to rectal involvement, such as constipation, hematochezia, or painful defecation endorectal gel may also be useful to distend the rectal\sigmoid bowel wall.
When beginning the MRI, an antispasmodic agent (i.e. 20 mg of hyoscine butylbromide – Buscopan; Boehringer Ingelheim, Ingelheim am Rhein, Germany) should be administered intravenously to reduce motion artifacts caused by intestinal peristalsis.
A phased array surface coil is used for imaging of the pelvis. The typical imaging protocol (9,14,16) includes three T2-weighted (T2W) sequences in different slice orientations (sagittal, coronal, and axial planes), followed by three T1-weighted (T1W) sequences in an identical imaging plane (TR 500 ms, TE 14 ms) without fat suppression and fat-suppressed T1W before and after intravenous injection of contrast media (16). The field of view can be smaller than 32 cm in order to obtain a better spatial resolution (17). Use of contrast-enhanced imaging is primarily required to identify solid enhancing nodules within endometriotic cysts when malignant transformation is suspected. In cases of suspected ureteral involvement, MR urographic techniques can be used. Recently, some authors have suggested that diffusion-weighted imaging (DWI) may play a significant role in the diagnosis of endometriosis, in particular for the deep infiltrating one (18). It is easy to overlook even moderate sized soft tissue masses in the pelvis for inexperienced readers as demonstrated by Siegelmans (19) and the DWI may help in this.
MRI findings according to the different locations of endometriosis
Diagnostic performance, strength point, limitations and pitfalls of MR in the evaluation of endometrioma, deep infiltrating endometriosis (DIE), and malignant transformation.
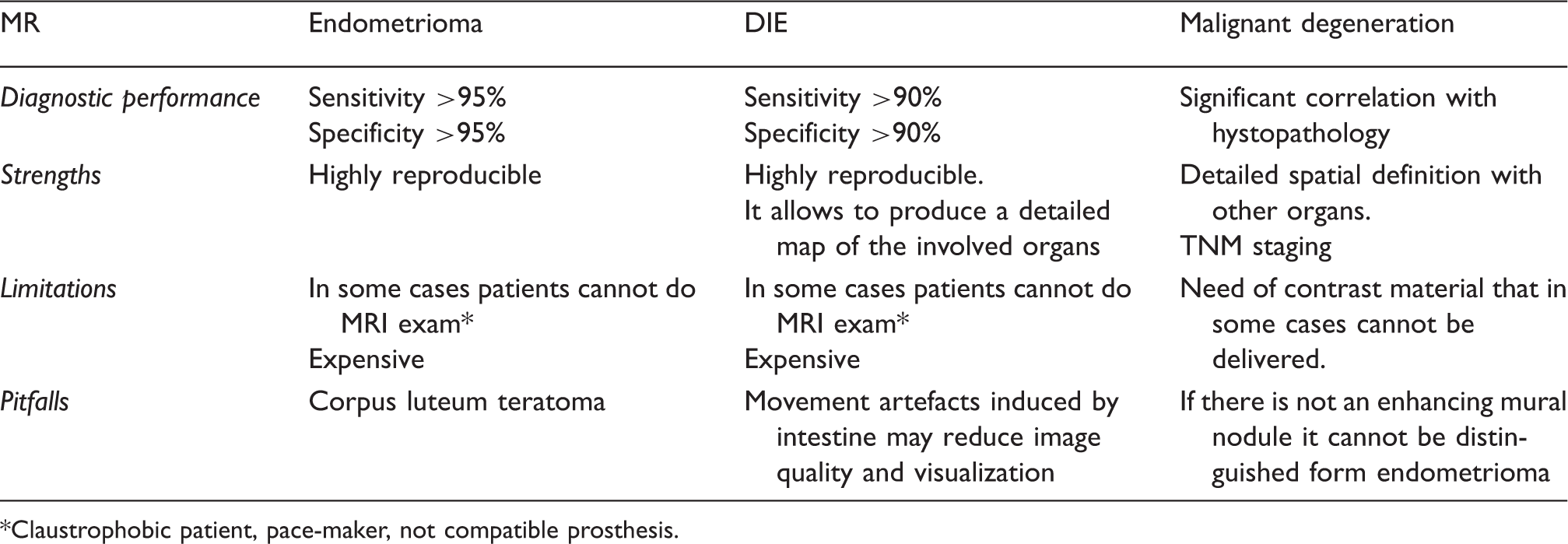
Claustrophobic patient, pace-maker, not compatible prosthesis.
Signal intensity resume for the analysis of endometriosis at various MRI weightings.
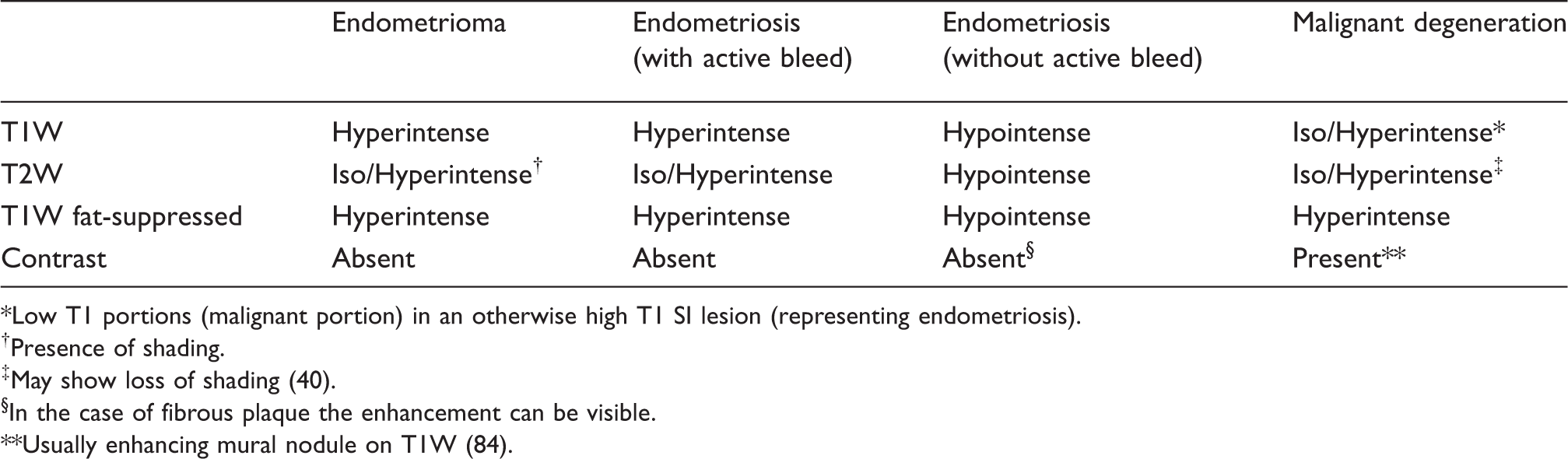
Low T1 portions (malignant portion) in an otherwise high T1 SI lesion (representing endometriosis).
Presence of shading.
May show loss of shading (40).
In the case of fibrous plaque the enhancement can be visible.
Usually enhancing mural nodule on T1W (84).
In recent years, several papers have described the MR findings according to the different locations of endometriosis (17,21–28).
Ovaries
The ovaries are the most common site for endometrial involvement and may be affected in two ways: (i) the endometriomas or chocolate cysts that are associated with ovarian enlargement, and which are caused by repeated episodes of hemorrhage, may replace completely normal ovarian tissue; and (ii) small nodular implants which may cause paraovarian scarring and adhesions (29). In MRI an endometrioma appears as a homogeneously hyperintense mass on T1W MR images; on T2W MR images, it appears as a low-signal-intensity mass with areas of high signal intensity (Fig. 1) (30).
MRI study of a 35-year-old patient. (a) Axial T1W, (b) axial T1W fat-suppressed, (c) axial T2W, and (d) axial T1W fat-suppressed after gadolinium. In (a) and (b) an endometrioma is visible (white arrow). In (c) the shading effect is indicated (open white arrows). In (d) no evidence of enhancement after administration of contrast material is demonstrated.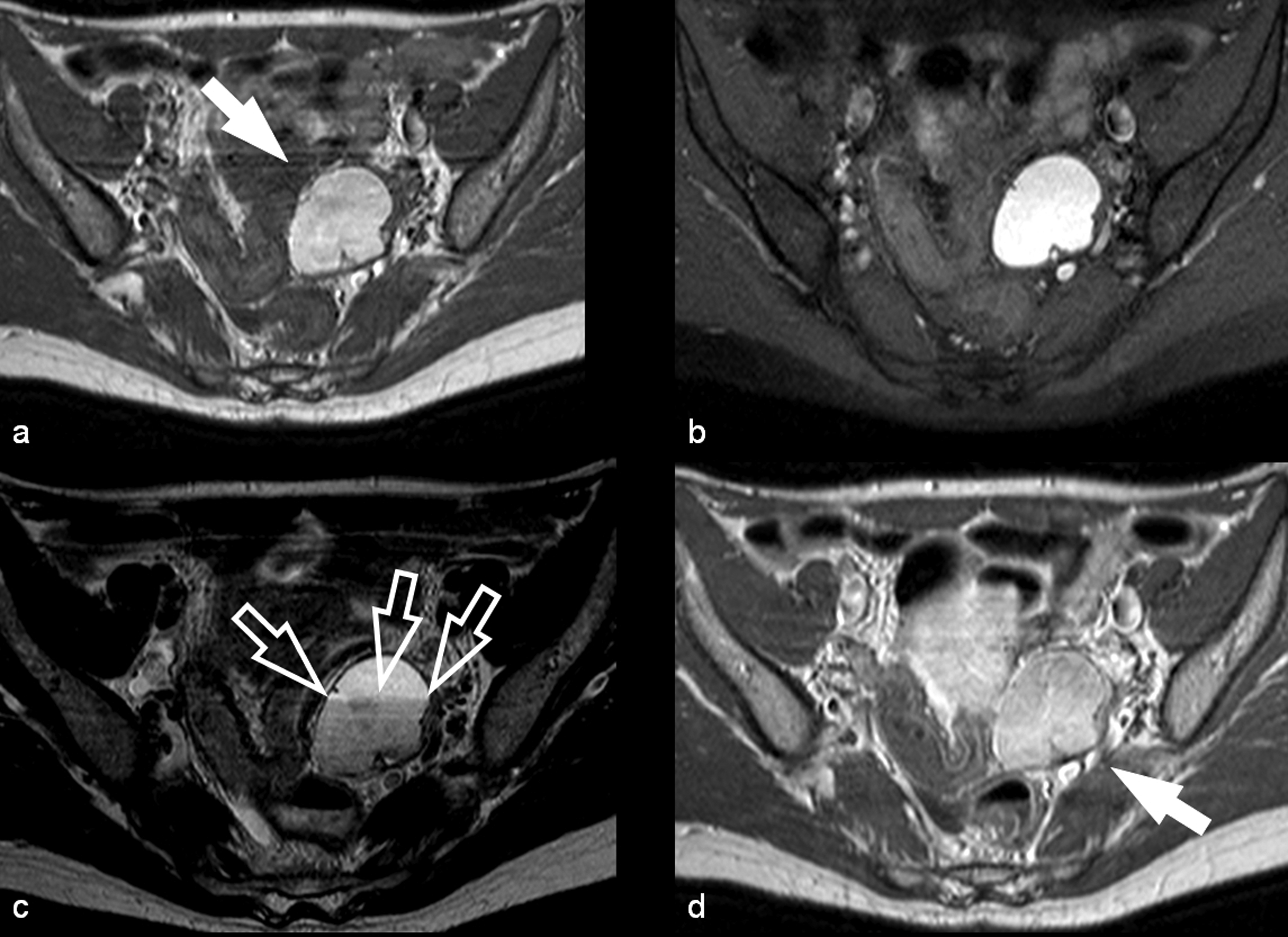
Endometriomas have a wall with a variable appearance (from thin to thick and fibrotic) and they usually contain dark/brown semi-solid material that represents the degenerated blood products (the so called “chocolate cyst”) (30). Because the endometriomas contain blood products of different ages and concentrations, they may show a variable appearance, in fact as free water in the cyst is resorbed, the iron concentration increases along with the viscosity of the contents of the cyst: this condition determines the “shading effect” (Fig. 1). Shading is present when a cyst, hyperintense on a T1W image, shows a gradient from hypointense to hyperintense on a T2W image. Shading can range from faint, dependent layering to complete signal void, according to the concentration of blood products. Togashi et al. (22) found that an extremely sensitive sign for the presence of an endometrioma was the presence of a cyst hyperintense on T1W images and the presence of shading on T2W images. Another criterion is to observe multiple hyperintense cysts on T1W images (and T1W fat-suppressed images) regardless of their signal intensity on T2W images.
The other lesions that show high signal intensity on T1W images are hemorrhagic masses, dermoids, and mucinous cystic neoplasms. In the differential diagnosis it is important to remember that hemorrhagic cysts are usually unilocular as opposed to endometriomas, which are usually multilocular and bilateral. Moreover, hemorrhagic cysts do not show shading effect on T2W images and will resolve with time. It is possible to recognize and differentiate dermoids from endometriomas by the presence of chemical shift artifact and signal drop-out on the fat-suppression images whereas the mucinous lesions can have increased signal intensity on T1W images, but the signal is markedly lower than that of fat or blood.
Bladder
MRI represents an important technique to study bladder involvement by endometriosis because this technique may show abnormalities, even in patients with normal cystoscopic results or with no urinary tract symptoms (31). The vesicouterine pouch is a common site of deep infiltrating endometriosis (Fig. 2). The lesions appear as small masses of round or lobulated hypertrophic tissue covered by normal mucosa (30). Usually, the bladder involvement by endometriosis is found on the posterior wall near the dome or in the trigone area. It is quite uncommon for vescical endometriosis to infiltrate the muscular layer and is manifested as a mural mass that projects into the lumen by invading the mucosa (intrinsic involvement) but endometriotic implants are often confined to the serosal surface (extrinsic involvement) (32). The MRI appearance of bladder endometriosis is thickening of the bladder wall with hypointense signal on T2W images. Sometimes, hyperintense foci on T2W images corresponding to the dilated endometrial glands may be found. After contrast material administration, the nodule of endometriosis is more enhanced than the normal bladder detrusor muscle (33). In the detection of endometriosis of the bladder, the performance of MRI is still debated, in fact Chamiè et al. (23) obtained a sensitivity of 23% whereas Bazot et al. (21) obtained a value of 88%.
MRI study of a 29-year-old patient. (a) Sagittal T2W, (b) sagittal T1W, and (c) coronal T2W demonstrate a nodule of endometriosis located in the dome of the bladder (white arrow).
Ureter
Involvement of ureter by endometriosis is quite uncommon and the symptoms can vary according to the type of nodule infiltration. Endometrial tissue can also directly infiltrate the muscularis propria, lamina propria, or ureteral lumen causing symptoms that may be related to the pelvic endometriosis itself (dysmenorrhea, dyspareunia) or secondary to urinary tract involvement (flank pain, obstruction, and in some cases decline of renal function) (34). It is possible to identify two major pathological types of ureteral endometriosis: extrinsic and intrinsic. As with bladder involvement, extrinsic endometriosis is the most common form (80%) of ureteral involvement and it represents endometrial glandular and stromal tissue within the submucosa and adventitia of the ureter that originates from adjacent disease of the ovary, broad ligaments, or utero-sacral ligaments (9). In addition, scar tissue or fibrosis without true endometriotic invasion of the ureter may also be classified as extrinsic disease. In contrast, intrinsic endometriosis (20%) involves the uroepithelial and submucosal layer. At MRI, ureteral endometriosis usually appears as irregular hypointense nodules on T2W images. Extrinsic disease may be hypothesized when the interface of fat between the nodule and ureter is no longer visible. MR urographic techniques can be used to obtain three-dimensional reconstructed images from coronal volumetric excretory phase T1W data.
Urethra
Urethral endometriosis is uncommon; direct implantation of endometrial tissues during procedures (i.e. episiotomy) is hypothesized to be the etiologic mechanism (35). In some cases, endometriosis may be mistaken for a urethral diverticulum and therefore a precise diagnosis is essential to facilitate optimal management. Usually, urethral involvement is observed as a contiguous extension from the bladder and the MRI findings are the same as those described for bladder endometriosis.
Vesicouterine pouch
These lesions are usually associated with anteflexion of the uterus and obliteration of the anterior cul-de-sac due to extensive adhesions between the peritoneum of the bladder fold and the uterus. On MRI T2W images, endometriosis of the vesicouterine pouch is manifested as hypointense nodules that typically adhere to the anterior uterine surface, forming an obtuse angle with the vesical wall.
Uterus and vagina
The most common localization of ectopic endometrial tissue within the uterus is the so-called adenomyosis (presence of ectopic endometrial tissue in the myometrium) but this is a different pathology from endometriosis. Whereas it is important to remember that uterine involvement by endometriosis is usually sub-serosal, sometimes it is possible to find nodules of endometriosis in the serosal surface of the uterus. Sometimes, the nodules of endometriosis may affect the vagina and the vaginal fornix. In recent years several papers have been published that demonstrate the good sensitivity and specificity of MRI in detecting nodules affecting the vagina (23,24).
Uterine ligaments
Uterine ligaments can sometimes be affected by endometriosis that usually determines nodularity or thickening of these structures. When the uterine ligaments are involved, thickening of these structures renders the ligaments palpable at physical examination. These nodules are visible as hypo-intensity signal in T2 sequences and after administration of contrast material it is possible to observe a diffuse peritoneal enhancement secondary to the inflammatory reaction incited by microscopic endometrial implants on contrast-enhanced fat-saturated MRI.
Fallopian tubes
Endometriosis of the fallopian tubes is usually a surface phenomenon, with the endometrial glands and stroma being situated in the sub-serosal layer: this condition is strongly associated with infertility. Moreover, an association has been described between the endometriosis in the fallopian tubes and a predisposition to endometrial malignancies such as clear cell carcinoma and endometrioid carcinoma (30). MR usually identifies this condition as a hyper-intense signal in T1W images.
Rectovaginal pouch
The rectovaginal pouch is frequently affected by endometriosis and uterine retroversion or angular rectal attractions are often associated findings (14,36). In MRI, nodules of endometriosis affecting the rectovaginal pouch usually appear as hypo-intense nodules on both T1W and T2W MRI images with signal intensity close to that of pelvic muscle (Fig. 3) as indicated in Zawin et al. (25) and Caramella et al. (37). Sometimes, foci of endometriosis may also have an abundant glandular component and discrete fibrotic reaction. In such cases, the endometriotic foci are hyper-intense nodules on T1W and fat-saturated T1W MRI images, irrespective of their appearance on T2W MRI images. Moreover, the solid glandular component shows variable enhancement after the intravenous administration of contrast material.
MRI study of a 39-year-old patient. (a) Sagittal T2W, (b) sagittal T1, and (c) sagittal T1W after administration of contrast material. The presence of a nodule in the rectovaginal pouch is visible (white arrow) and this is characterized by (a) hypointense signal in T2W, (b) iso/hypo-intense signal in T1W, and (c) mild enhancement after contrast material.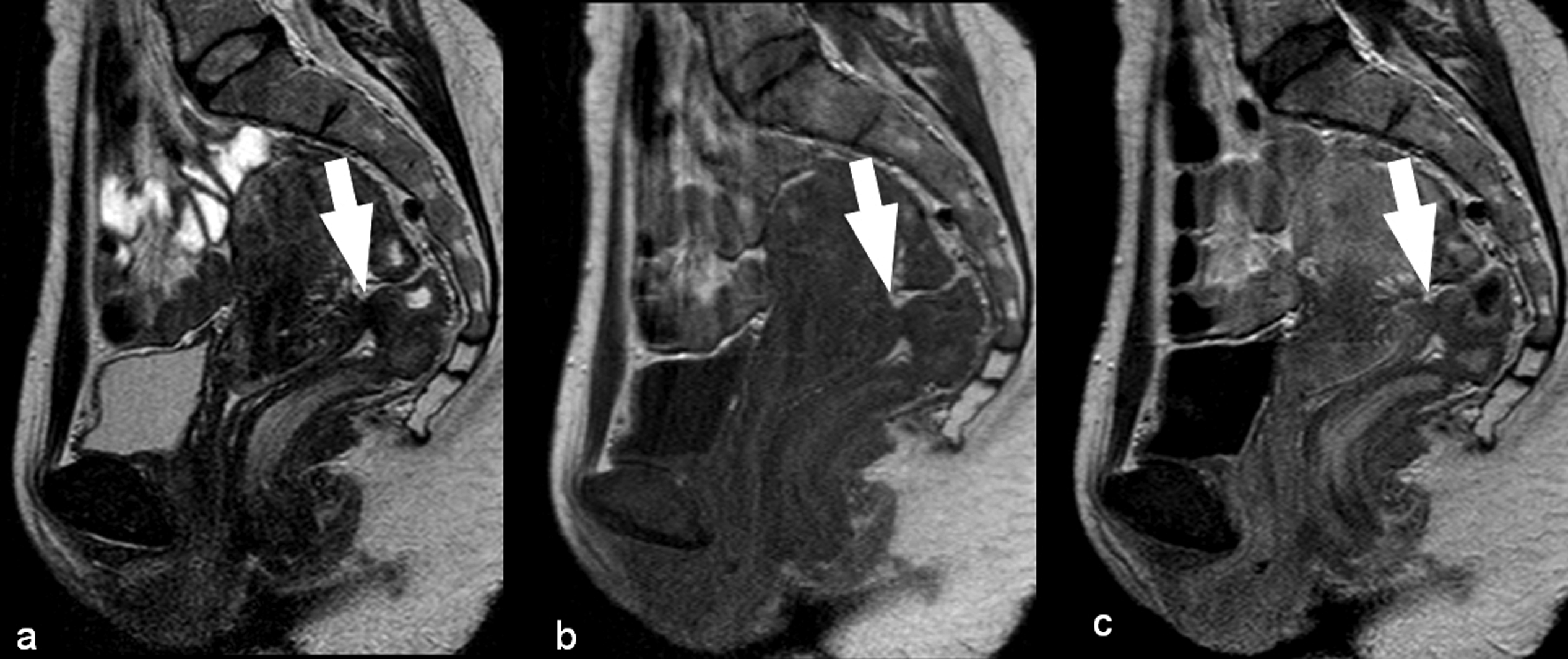
Retrocervical area
The retrocervical area is considered a virtual extraperitoneal space behind the cervix, situated on the same plane as the rectovaginal pouch and above the rectovaginal septum. This area is frequently affected by endometriosis (Fig. 4) and it is usually associated with uterosacral ligament involvement (23) and with the retroversion of the uterus. MRI findings show hypointense thickening and, in some cases, the involvement of the sigmoid bowel. Del Frate et al. (14) identified a condition they called “hourglass-shaped” lesions that are found in 25% of cases and are due to posterior extension of a posterior forniceal lesion toward the anterior rectal muscularis. These lesions are usually larger than 3 cm, with a greater risk of extension to the rectal wall. The authors reported that infiltration of the rectal muscularis is observed in this type of lesion.
MRI study of a 31-year-old patient. (a) Sagittal T1W, (b) sagittal T2W, (c) axial T1W, and (d) axial T2W. The presence of a nodule in the retrocervical area is visible (white arrow) and this is characterized by (b, d) hypointense signal in T2W and (a, c) iso/hypo-intense signal in T1W. Moreover the nodule demonstrates decreased vascularity compared to the normal myometrium.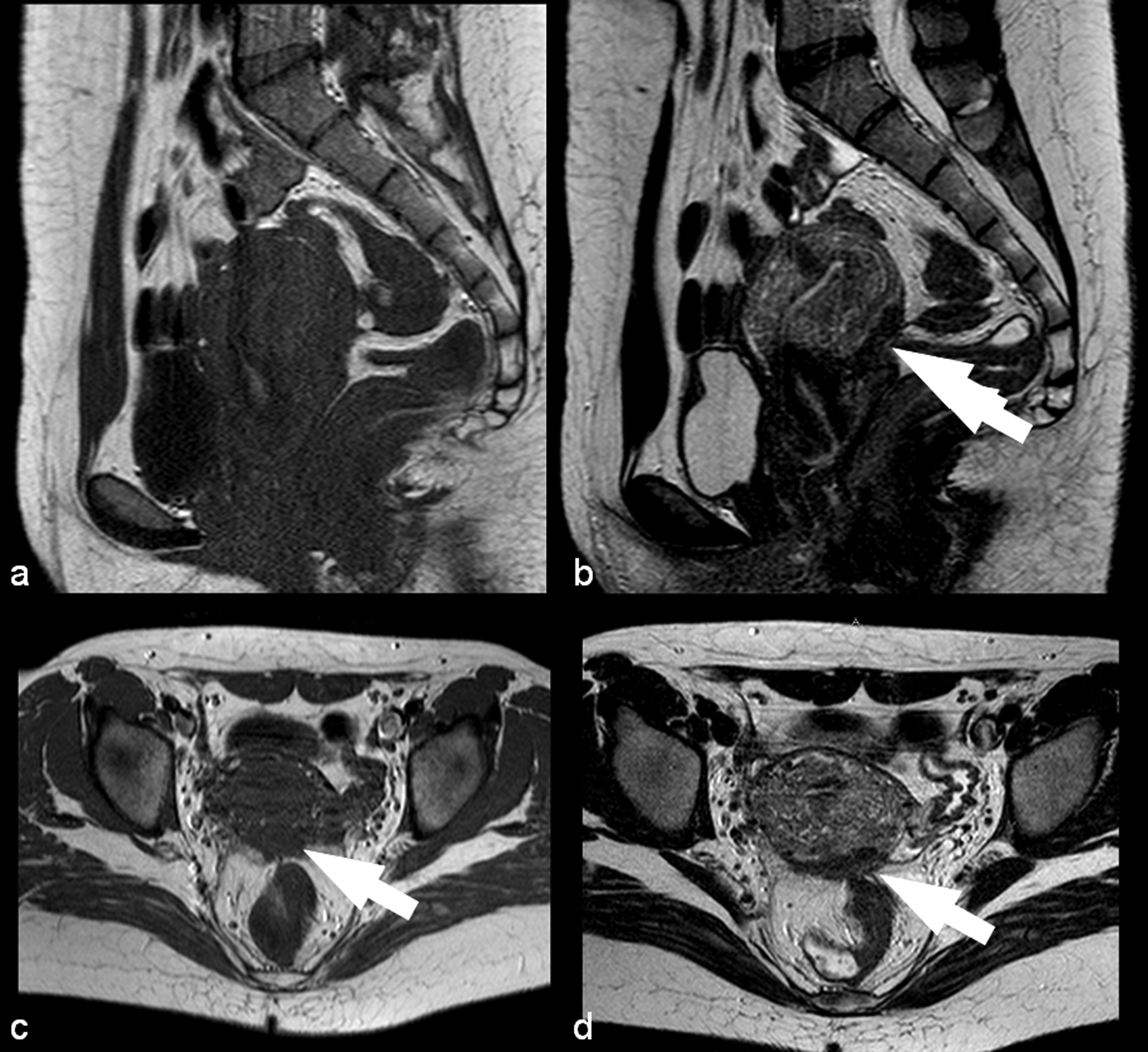
Utero-sacral ligaments
The USLs are visible at MRI as thin, semicircular hypointense cords that originate from the lateral margin of the uterine cervix and the vaginal vault (9). MRI findings of involvement of the uterosacral ligaments are usually monolateral or bilateral hypointense thickening and nodules within these ligaments. In most cases it is not possible to find the nodules in the USLs but only their thickening. The most commonly affected part of USLs affected by endometriosis is the proximal medial portion (Fig. 5) (9). The MRI shows optimal sensitivity in detecting nodules affecting the USL; in particular Bazot et al. showed that by using thin-section oblique axial T2W MR images it is possible to reach 93% sensitivity (17). Saba et al. (27) suggested that the diagnosis of endometriosis of the USL is simple when ligaments are involved together with the torus uterinus, in particular when an arciform pattern or a stellate pattern is formed, whereas, when there is only a thickening or an asymmetric nodular irregularity the involvement of the USL can be difficult (27).
MRI study of a 35-year-old patient where (a) axial T2W and (b) coronal T2W demonstrate the normal morphology (2 mm in the right and left USL) and signal of the USLs (white arrows). MRI study of a 30-year-old patient where (c) axial T2W demonstrated thickened (9 mm in the right USL and 7 mm in the left USL) USLs with the presence of significant contrast enhancement in the (d) axial T1W fat-suppressed image.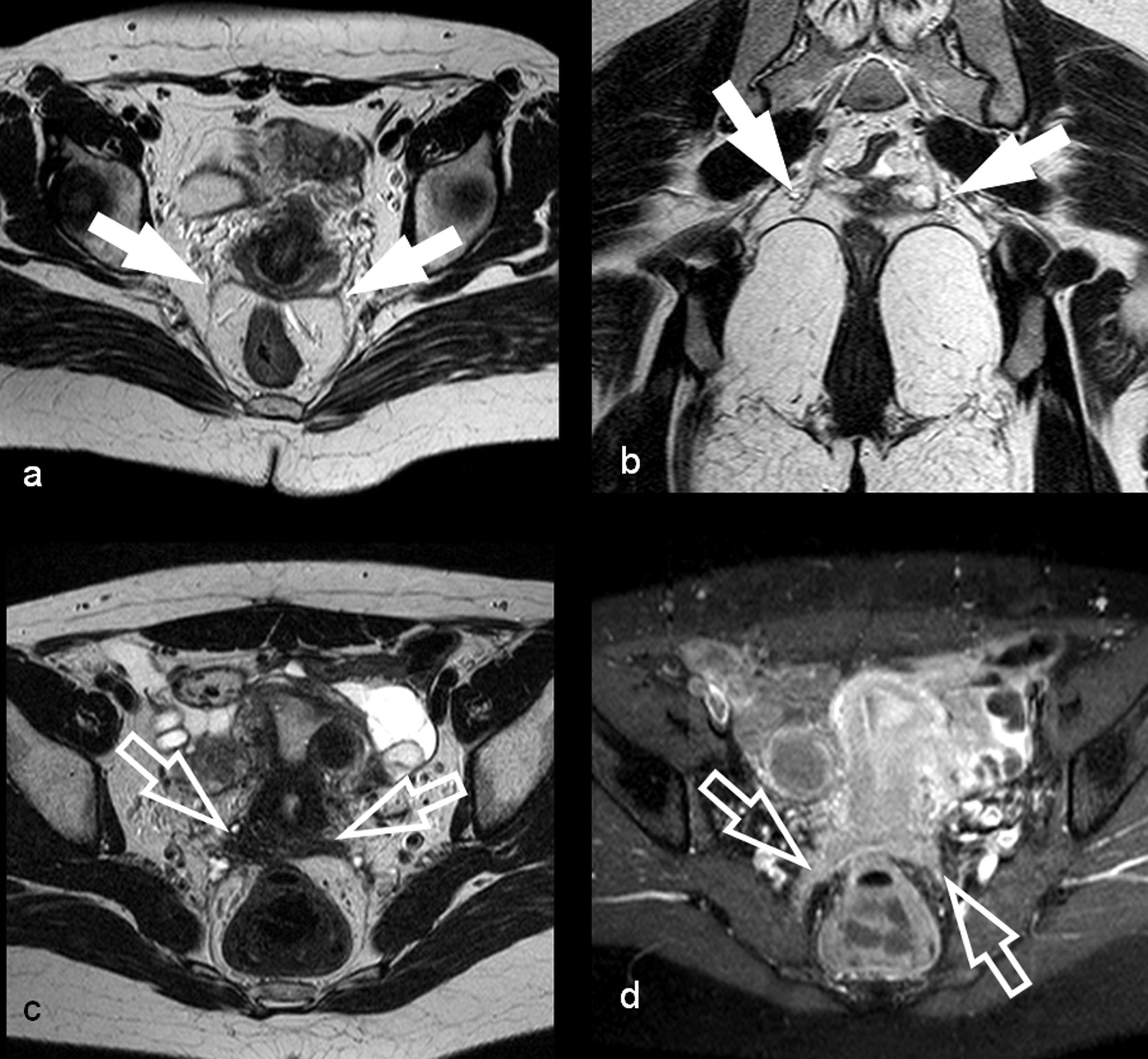
Rectovaginal septum
In this case, nodules of endometriosis are located between the posterior wall of the vaginal mucosa and the anterior rectal wall under the peritoneal fold of the Douglas pouch. In normal conditions the MRI depicts the rectovaginal septum as a hyper-intense signal area in T1W and T2W images whereas, in MRI, nodules of endometriosis affecting the rectovaginal septum usually appear as hypo-intense nodules on both T1W and T2W MRI images. Grasso et al. (26) showed very good results in the detection of nodules of endometriosis located in the rectovaginal septum with a sensitivity of 76% and a specificity of 100%.
Rectum-sigmoid bowel and intestine
The rectosigmoid is the segment of bowel that is most commonly involved by endometriosis and adhesions, bowel strictures, or intestinal obstruction may result from the inflammatory response to cyclic hemorrhage. The implants are usually serosal but can sometimes involve the subserosal layers and cause thickening and fibrosis of the muscularis propria. Usually, an intact overlying mucosa is present, since the implanted tissue only rarely invades through to the mucosa (9). The identification of deep infiltrating endometriosis of the rectum-sigmoid bowel can be complex and it is usually visible as a plaque of hypo-intense signal in the T1W and T2W images (Fig. 6); it is sometimes possible to observe the presence of punctate hyperintense foci of hemorrhage. The MRI shows very good value in detecting nodules involving the intestine and the rectum-sigmoid bowel with a sensitivity value up to 88% (21) and specificity up to 100% (26).
MRI study of a 24-year-old patient. (a) Sagittal T1W, (b) sagittal T2W, (c) coronal T2W, and (d) axial T2W demonstrate the presence of a nodule of endometriosis between sigmoid bowel and posterior wall of the uterus (black arrow).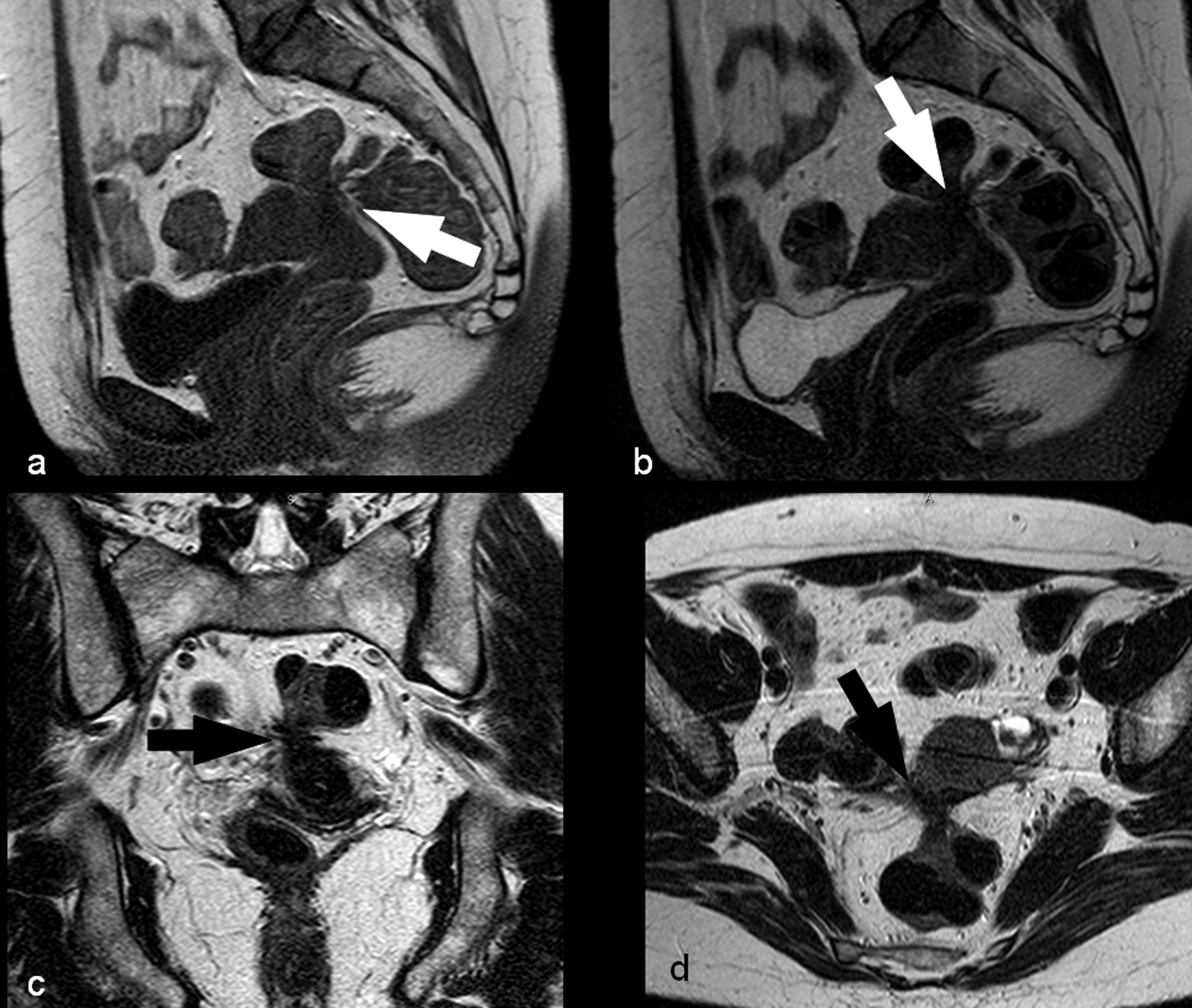
When nodules of endometriosis are localized in the retroperitoneal section frequent concomitant findings are the adherences that identify fibrotic tissue originating from the nodules of endometriosis and involves the closest organs (Fig. 3). Sometimes the adherences determine traction of the affected organs (38). This is an important finding because it can be considered an indirect sign of endometriosis. It is quite frequent, in the cases of nodules of endometriosis affecting the rectum or sigmoid bowel, to observe an angulation of the organ. The same phenomenon is visible frequently in the case of nodules of endometriosis affecting the rectovaginal pouch and retro-cervical area: the fibrous tissue involves the uterus that is angulated in retroverse position.
Other locations
Nodules of endometriosis can sometimes develop in Cesarean section scars involving the Pfannenstiel incision. MRI is characterized by hemorrhagic signal intensity on T1W and T2W images, in the myometrium along the surgical scar. Endometriosis can also demonstrate isolated involvement of the vagina, intestinal loops, or other extraperitoneal sites, such as the ischioanal (ischiorectal) fossa and and sciatic nerve (9). The abdominal wall is another site of extra-pelvic endometriosis usually developing in a surgical abdominal scar with an incidence of 0.1% and the differential diagnosis includes lipomas, sebaceous cysts, hernias, and malignant tumors (39); abdominal wall endometriosis usually appears as homogeneously hypointense or isointense nodules, or less frequently as focal areas of high and low signal intensity, suggesting old hemorrhage or fibrosis on T2W images and T1W fat-suppressed images. Rare extraperitoneal sites of endometriosis include the lungs and the central nervous system (40).
MRI findings in malignant degeneration
Malignant transformation of endometriosis is uncommon and the typical MRI finding is the presence of an enhancing mural nodule on T1W gadolinium-enhanced sequence (41). Authors found that endometrioma with malignant transformation may show a loss of shading on T2W images because of the dilution of hemorrhagic fluid by tumor secretion (Table 2) (41). It is important to pay attention to the MR images after contrast material because this can be an important sign of malignant degeneration. Sometimes asymmetric signal intensity on contrast-enhanced fat-saturated images can be found and in this case parametrial involvement should be suspected; this finding should not be misinterpreted as a focus of endometriosis (14). However, preoperative extension of endometriosis has been demonstrated even without use of contrast material (14). Sometimes, ovarian cancer can have internal hemorrhage. Features suggestive of malignancy are the visualization of septations, solid components and a size larger than expected for an endometrioma. Moreover, lesions larger 15 cm and with wall nodules should be sampled to rule out malignancy.
Suggested flow-chart
In a diagnostic flow-chart (Figs. 7 and 8) the first images to analyze should be the T1W in order to identify the presence of endometrioma that is visible as one or more areas of hyper-signal. When the endometrioma is identified it is necessary to check the T1W fat suppressed images in order to perform a differential diagnosis with lipid mass neoplasm (namely teratoma, dermoid cyst). In the case of endometrioma, the signal of the lesion will remain hyper-intense in the T1W fat-suppressed images (because there is no drop of signal in the lesions containing blood. In the case of dermoid\teratoma, the signal of the lesion in the T1W fat-suppressed images will be very low because of the drop of the signal (42,43).
MRI diagnostic flow chart for the identification of endometriomas. MRI diagnostic flow chart for the identification of nodules of endometriosis.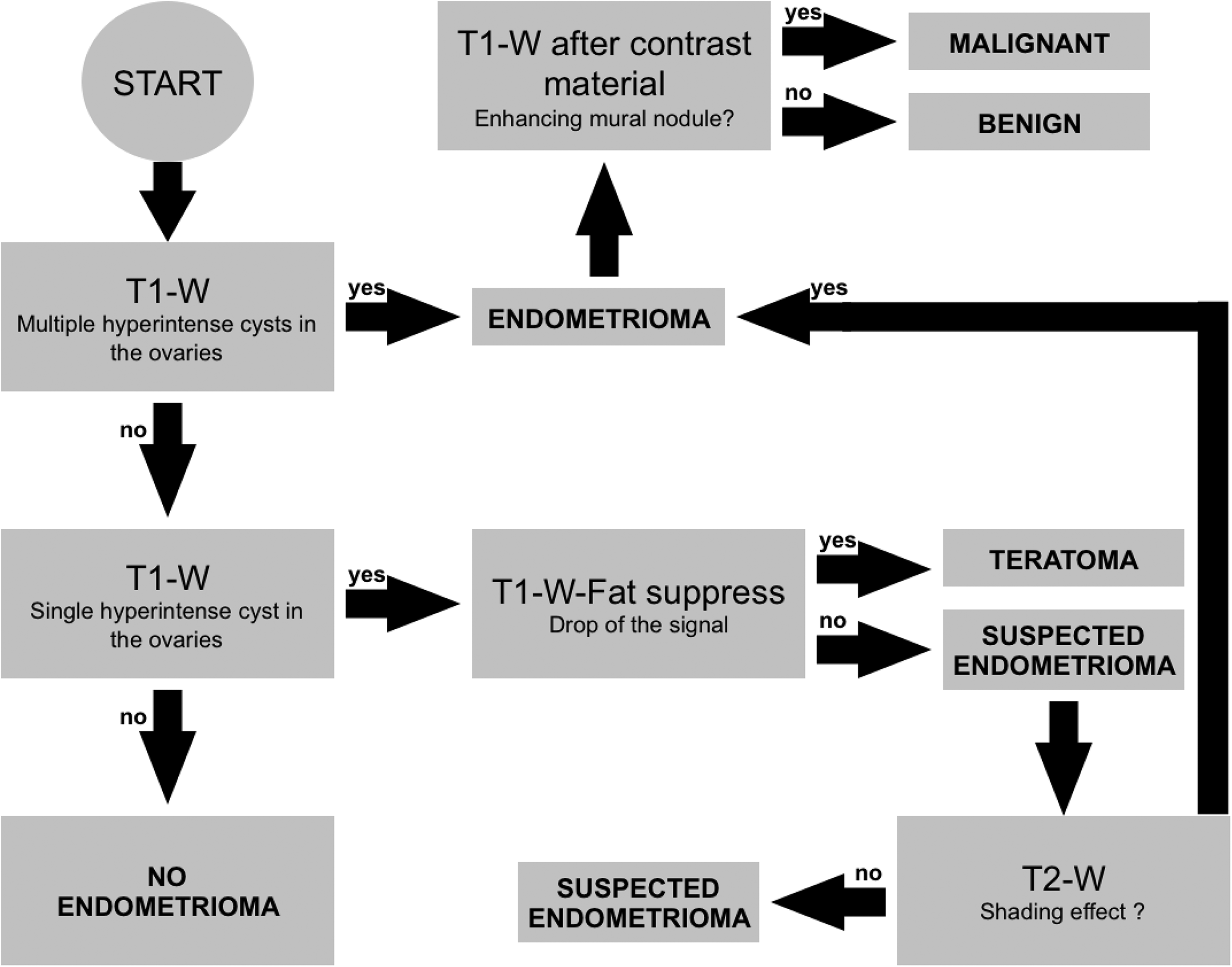

It has been described in the previous sections that it can sometimes be difficult to distinguish the endometrioma from other lesions (hemorrhage within a follicular cyst, a corpus luteum cyst, or even a neoplastic cyst): in this case it is important to look for the presence of multiple lesions hyperintense in T1W/T1W fat-suppressed images. To obtain a further confirmation of the presence of endometrioma a T2W image should be analyzed in order to look for the shading effect. However, in the T1W/T1W fat-suppressed images small nodules with hyper-signal should also be looked for because, although it is quite uncommon, the nodules of endometriosis can have a hemorrhagic signal. In summary the analysis of T1W/T1W fat-suppressed images is mainly used for the detection and characterization of endometrioma.
After the analysis of the T1W and fat-suppressed images, T2W images should be studied. Usually T2W images should be acquired in the three spatial planes (axial, coronal, and sagittal) and each specific plane offers, based on our experience, specific information. The sagittal T2W images allow us to study the recto-vaginal septum, the utero-vescical area, the retrocervical area, and the Douglas pouch very well; in the analysis of sagittal T2W images it is possible to find the “hourglass-shaped” lesion (14) that indicates the posterior extension of a posterior forniceal lesion toward the anterior rectal muscularis.
The analysis of T2W axial images is extremely useful in the identification of nodules of endometriosis affecting the utero-sacral ligaments and the intestinal involvement (in particular the rectum, sigmoid bowel, and intestines). The axial images are very useful because these allow for the identification of the mesorectum that is the fold of peritoneum connecting the upper portion of the rectum with the sacrum. In the mesorectum is contained the rectum and the fat. Usually when a nodule of endometriosis affects the rectum there is an alteration of the mesoretum where it is possible to observe multiple hypointense areas with a morphologic aspect of a “web”. The presence of this “web” is suggestive of the presence of a nodule of endometriosis with fibrous adherence. The analysis of coronal T2W images is extremely useful for the detection of nodules of endometriosis located in the urinary tract (in particular the bladder and ureters).
The exam should be completed with the analysis of the T1W images after the administration of contrast material (in the case of endometrioma) to exclude malignant transformation where it is usually visible an enhancing mural nodule or the visualization of septations or solid components. It is also important to include a T1W fat-suppressed image in the context of a bright T1 lesion since enhancement may be difficult to detect.
MRI versus ultrasound: where are we going?
Transvaginal ultrasonography (US) is usually the first imaging technique used to diagnose endometriosis. US is considered the method of choice for differentiating endometriomas from other ovarian cysts (44) and, in recent years, authors have emphasized the use of transvaginal US in identifying deep endometriosis (45). However, the accuracy of transvaginal US in the detection of some deep endometriotic lesions may vary depending on the location of the lesions and the experience of the operator (9).
Recently some authors suggested that US and MRI may be viewed as complementary techniques (28); in particular, it has been demonstrated that MRI and TVUS have a complementary accuracy in the identification of recto-sigmoid endometriosis according to their localization. The authors performed a step-wise logistic regression analysis to identify a mathematical model and they found that the probability of the presence of nodules of endometriosis varied between a minimum of 14% for patients with both MRI and tg-TVUS negative to 95% for patients with both MRI and tg-TVUS positive.
Conclusion
The identification and staging of endometriosis represents a key-point for the identification of the correct therapeutical approach. Nowadays, the multi-planar capability, high sensitivity for detection of blood products, and ability to identify sites of disease hidden by dense adhesions have made pelvic MRI the non-invasive imaging technique of choice for more accurate detection and staging of endometriosis. Moreover, the introduction of stronger magnetic field as well as the refining of the mathematical sequence will further improve the spatial and contrast resolution of this technique.
Footnotes
Acknowledgements
The authors are deeply indebted to the technicians Paolo Contu, Diana Caravana and Franco Conti for their precious help. A special thanks to Barry Mark Wheaton for the linguistic revision of this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.