
Abstract
Background
Fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) is commonly performed for cancer staging, as it can detect metastatic disease in multiple organ systems. However, there has been some controversy in the scientific literature when comparing FDG PET/CT and technetium-99 m-bone scintigraphy (bone scan) for the detection of skeletal metastases.
Purpose
To compare the accuracy of FDG PET/CT with bone scan for the detection of skeletal metastases.
Material and Methods
The study group comprised 202 adult cancer patients who underwent both FDG PET/CT and bone scan within 31 days for staging. Bone scans and FDG PET/CT were evaluated by two musculoskeletal radiologists for the presence and location of skeletal metastatic disease. Confirmation of the final diagnosis was based on the CT or magnetic resonance imaging (MRI) appearance, follow-up imaging, or histology.
Results
The sensitivity, specificity, and accuracy for detecting skeletal metastatic disease of FDG PET/CT were 97%, 98%, and 98%, respectively, and of bone scan were 83%, 98%, and 93%, respectively. The lesions that bone scan most commonly missed were located in the pelvis, spine, and sacrum. FDG PET/CT missed mostly lesions that were outside of the field of view, but in all of these cases the patient had additional sites of skeletal metastatic disease. Bone scan falsely identified six metastatic lesions and FDG PET/CT falsely identified three metastatic lesions.
Conclusion
FDG PET/CT is an accurate technique for detection of skeletal metastases, and is superior to bone scan, especially in the spine and pelvis.
Keywords
Introduction
Skeletal metastatic disease is common, with a prevalence of approximately 280,000 adults in the United States, and with approximately 68% of cases occurring in patients with primary breast, prostate, or lung cancer (1,2). Most skeletal metastases are not painful at the time of detection, but some of these may progress to pathologic fracture and/or nerve and spinal cord compression; therefore, early detection of metastases is important to decrease morbidity (3–5). Detection of metastatic disease is also important for staging, outcome prediction, and treatment planning.
Positron emission tomography/computed tomography (FDG PET/CT) is commonly performed for cancer staging, as it can detect metastatic disease in multiple organ systems (6–8). It is also sensitive for the detection of skeletal metastases (8), however, the detection of skeletal metastases may be lower when compared to other anatomical sites (9). Therefore, Technetium-99 m-methylenediphosphonic acid skeletal scintigraphy (bone scan) is the mainstay of evaluation for skeletal metastases (3,10). There has been some controversy when comparing FDG PET/CT and bone scan for detection of skeletal metastatic disease. Some studies suggest that FDG PET/CT may be more sensitive than bone scan for the detection of osteolytic metastases but less sensitive for the detection of osteoblastic metastases (11–13), while other studies suggest that FDG PET/CT is comparable (8,14) or superior (15) to bone scan in the detection of skeletal metastatic disease.
The purpose of this study was to compare the diagnostic accuracy of FDG PET/CT and bone scan in the detection of skeletal metastatic disease in a large patient population with different types of tumors. We hypothesize that FDG PET/CT would be more accurate in the evaluation of skeletal metastatic disease than bone scan.
Material and Methods
Patients
This study was approved by our institutional review board (IRB) and complied with HIPAA guidelines. We reviewed our database for patients who had undergone FDG PET/CT and bone scan for tumor staging within 31 days between February 2006 and September 2012. If the patient had more than one eligible set of studies, then the studies at initial presentation were selected. Subjects were all the consecutive patients who fulfilled the inclusion criteria. The average follow-up time was 725 days (range, 0–2925 days).
18 F-FDG PET/CT scan
The FDG PET/CT studies were performed on an integrated PET/CT scanner (Siemens Biograph 16 or 64, Siemens, Erlangen, Germany or GE Healthcare, Milwaukee, WI, USA), with a 16- or 64-slice CT and a full-ring HI-REZ LSO PET. Non-diabetic patients fasted for 6 h before the exam, and diabetic patients fasted for 4 h before the exam. Blood glucose levels were measured upon arrival, and patients were only injected with 18 F-fludeoxyglucose (FDG) if the blood glucose was less than or equal to 250 mg/dL (14 mmol/L). Two hours prior to the scans, 600 mL of 0.1% barium sulfate suspension (VoLumen; Bracco Diagnostics, Princeton, NJ, USA) were administered orally.
18 F-FDG was produced using an on-site 230 MeV isochronous cyclotron. The dose injected was based on patient’s body mass index (BMI). Patients with BMI less than 30 were given 15 mCi (555 MBq), patients with BMI in the range of 30.1–44 were given 20 mCi (740 MBq), and patients with BMI greater than 44.1 were given 25 mCi (925 MBq). After injection, the patient relaxed in a semi-reclined chair for at least 45 min. Attenuation correction CT obtained in mid-expiration phase without intravenous contrast (slice thickness 5 mm; table feed per rotation, 18 mm; time per table rotation, 0.5 s; tube voltage, 120 kVp; tube current, 11 mAs; field of view, 20 cm) and PET images were acquired with the patient’s arms over his/her head. Three-dimensional (3D) mode PET images were obtained from the skull base to the mid-thigh, with six to eight bed positions lasting 3–7 min each, with the duration depending on the patient BMI. Images were reconstructed to a slice thickness of 2.4 mm.
In addition, a diagnostic CT of the chest, abdomen, and pelvis with intravenous contrast was performed (slice thickness, 2.5 mm for chest and 5 mm for abdomen/pelvis; table feed, 15 mm/s; pitch, 1.5; tube voltage, 120 kVp; tube current, 200 mAs; sagittal and coronal reconstruction thickness, 2 mm with 2 mm intervals). The injected contrast was iopamidol (Isovue-370; Bracco Diagnostics), 300 mg/mL of iodine, injected at 2 mL/s, scanned with a 60-s post-injected delay in mid-expiration phase. For lymphoma or head and neck cancer patients, a dedicated neck CT was also performed.
Skeletal scintigraphy (bone scan)
Bone scans were performed using a double headed gamma camera (ECam, Siemens Medial Solutions, Hoffman Estates, IL, USA). 99 m-Technetium-methylene diphosphonic acid (MDP) dose injected was based on BMI. If the patient’s BMI was less than 31, 20 mCi (740 MBq) was injected. If the patient’s BMI was in the range of 31–45, 25 mCi (925 MBq) was injected. If the patient’s BMI was greater than 45, then 30 mCi (1110 MBq) was injected. Images were obtained a minimum of 2.5 h after injection of the 99 m-Technetium-MDP with a scan speed of 10 cm/min in both anterior and posterior projections. At the request of the attending nuclear physician or radiologist, additional static planar images of specific body parts were obtained.
Image analysis
Studies were reviewed in consensus by two fellowship trained musculoskeletal radiologists, who were blinded to the final diagnosis. The studies were reviewed on a Picture Archiving and Communication System (PACS) workstation (Agfa, Morstel, Belgium). Images were assessed for abnormal radiotracer uptake on FDG PET/CT and bone scans and the sites of abnormal uptake were recorded. We evaluated the unfused, corrected, axial PET images (cross correlation with CT was performed using PACS tools) and the planar, equilibrium (at least 4 h after injection) bone scan images.
Verification of detected lesions was performed using CT appearance, magnetic resonance imaging (MRI) appearance, follow-up imaging, or histology. The CT used for the FDG PET/CT evaluation was a non-contrast, low-dose CT. The CT used for verification was a separate, contrast-enhanced, diagnostic CT scan.
Statistical analysis
Sensitivity and specificity with their 95% confidence intervals and accuracy were calculated using MedCalc (version 12.7.8, MedCalc, Ostend, Belgium).
Results
Patients
Primary malignancy of patients.

Comparison between FDG PET/CT and bone scan
Out of the 202 patients, 71 (35%) had proven metastatic disease, with one metastatic lesion in 17 cases, two metastatic lesions in 12 cases, three metastatic lesions in three cases, four metastatic lesions in three cases, and five or more metastatic lesions in 36 cases. The outcome references were histology (38/202, 19%), MRI (22/202, 11%), CT (3/202, 1%), follow-up FDG PET/CT (57/202, 28%), comparison with prior FDG PET/CT (3/202, 1%), follow-up CT (66/202, 33%), or follow-up bone scan (13/202, 6%). The mean time between the FDG PET/CT/bone scan and outcome reference was 279 days (range, 0–2925 days). In 131 (65%) patients, no metastatic disease could be detected. FDG PET/CT detected metastatic disease in 69 of the 71 (97%) patients with skeletal metastatic disease, and bone scan detected metastatic disease in 59 of the 71 (83%) patients with skeletal metastatic disease. FDG PET/CT and bone scan both correctly identified 128 of the 131 (98%) patients without skeletal metastatic disease. The sensitivity, specificity, and accuracy of FDG PET/CT were 97% (95% confidence interval [CI], 90–100%), 98% (95% CI, 93–100%), and 98%, respectively, and of bone scan were 83% (95% CI, 72–91%), 98% (95% CI, 93–100%), and 93%, respectively.
In 172 out of the 202 patients (85%) FDG PET/CT and bone scan results were concordant.
Bone scan: false negative results
In 21 out of 202 cases (10%), FDG PET/CT showed more lesions than the bone scan, with some cases having more than one site of missed disease on bone. The sites of disease missed by bone scan were the pelvis (n = 12), spine (n = 12), sacrum (n = 9), ribs (n = 8), femur (n = 6), humerus (n = 3), sternum (n = 3), and scapula (n = 2). Among the 12 cases with lesions in the pelvis, 10 involved the posterior ilium near the sacroiliac joint and eight involved the acetabulum (Fig. 1). In six cases, bone scan also missed lesions in the femurs. In one case the bone scan demonstrated no uptake, but the CT showed innumerable sclerotic lesions, with increased 18 F-FDG uptake, which were confirmed to represent metastatic disease by biopsy.
A 42-year-old man with metastatic melanoma and biopsy proven sites of skeletal metastatic disease, including the spine, sacrum, pelvis, and both femurs. Anterior and posterior views from whole body bone scan (a) demonstrate no abnormal 99 m-Tc-MDP uptake to suggest metastatic disease. Axial non-contrast CT (b) from FDG PET/CT obtained the same day demonstrates a sclerotic right acetabular lesion (arrow) which demonstrates increased 18 F-FDG uptake on axial fused FDG PET/CT (c) consistent with a metastasis. Contrast-enhanced CT scan 1 month later shows enlargement of the right acetabular marrow abnormality, confirming that it is a metastasis.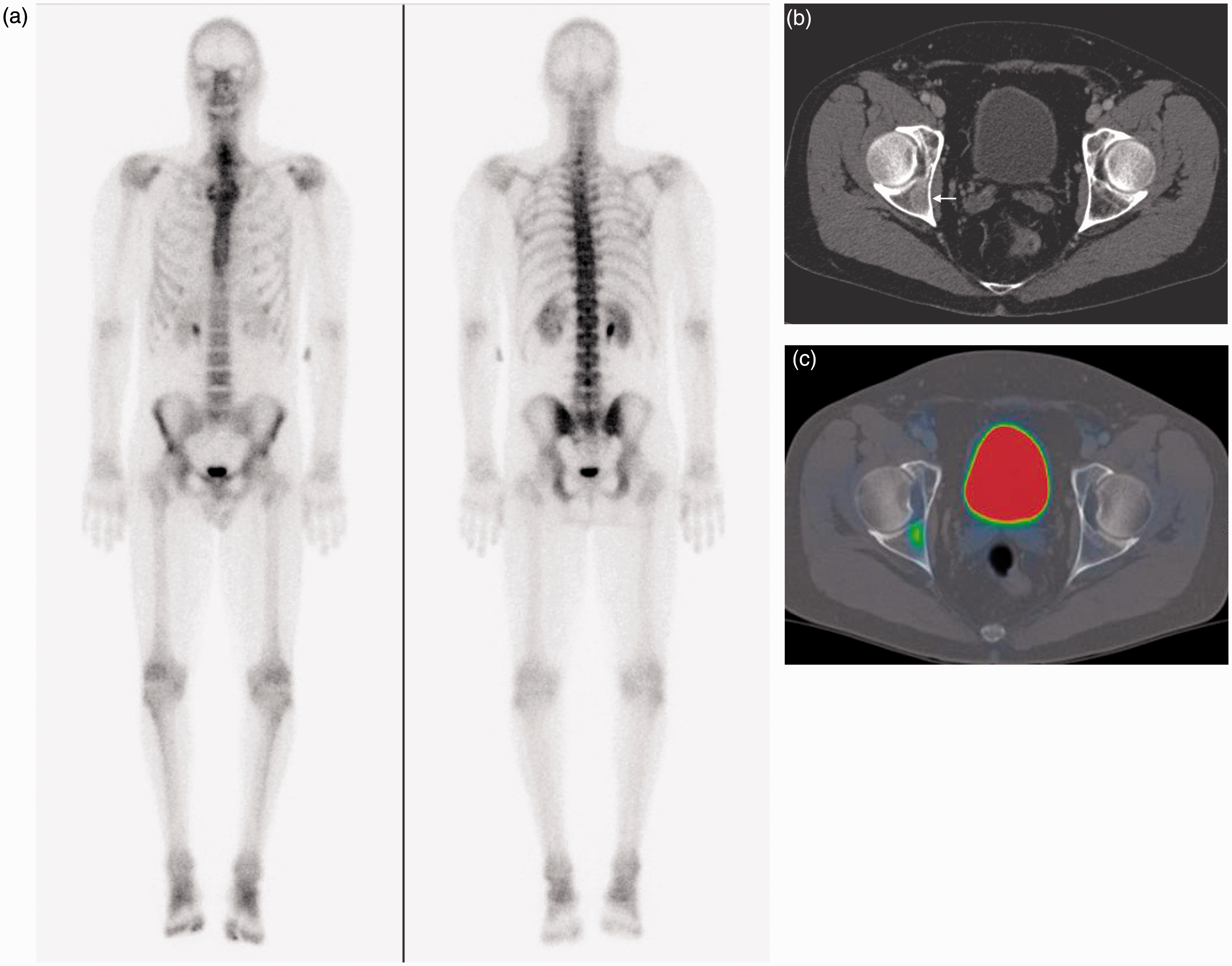
The cases missed with lesions missed by bone scan had the following tumor types: breast (n = 5), lung (n = 4), esophageal (n = 2), prostate (n = 2), and other (n = 8).
Bone scan: false positive results
In six out of 202 cases (3%), bone scan falsely identified metastatic lesions. The benign conditions mistaken for metastases included normal marrow (n = 2, thoracic spine and calcaneus), fracture (n = 2, acetabulum and clavicle) (Fig. 2), enchondroma (n = 1, humerus), and Baastrup’s disease (n = 1). Three of these cases (normal marrow in the thoracic spine, normal marrow in the calcaneus, and Baastrup’s disease) had other sites of metastatic disease, but these particular sites, which were initially considered suspicious, were later shown to not be metastases.
False positive bone scan and FDG PET/CT. A 71-year-old man with history of tonsillar carcinoma. Anterior view from whole body bone scan (a) demonstrates increased 99 m-Tc-MDP uptake of the right clavicle (arrow), suggestive of metastatic disease. Axial FDG PET/CT (b) demonstrates increased 18 F-FDG uptake, suspicious for metastatic disease. CT-guided percutaneous biopsy of the right clavicle was performed (c) and histology revealed pseudotumor (fibrin, hemorrhage) from benign fracture. The patient’s cancer was treated 16 years prior to these studies, and he did not have any other sites suspicious for metastatic disease. This case is an example of a false positive bone scan.
FDG PET/CT false negative results
In six out of 202 (3%) cases with confirmed metastatic disease, bone scan identified more metastatic lesions than FDG PET/CT. The sites of disease missed by FDG PET/CT were the skull (n = 3), spine (n = 1), sternum (n = 1), and toe (n = 1). In four out of the six cases (67%), the site of metastatic disease was outside of the field of view of the FDG PET/CT (skull, toe). In all of these cases, the patient had additional sites of skeletal metastatic disease.
In two cases, metastatic lesions did not demonstrate increased 18 F-FDG uptake but did demonstrate increased 99 m-Tc-MDP uptake. One of these cases was an L4 metastasis (Fig. 3). The other case was a breast cancer patient with a recurrent sternum metastasis in a site of prior resection.
False negative FDG PET/CT. A 74-year-old man with metastatic bladder carcinoma. Anterior and posterior views from whole body bone scan (a) demonstrate increased 99 m-Tc-MDP uptake in the L4 vertebral body (arrows), suspicious for metastatic disease. Axial FDG PET/CT (b) obtained the same day shows increased 18 F-FDG uptake of paravertebral lymphadenopathy but no abnormal skeletal 18 F-FDG uptake and no suspicious lytic or blastic lesion on CT. Follow-up CT performed 10 months later (c) confirmed L4 metastatic disease (arrows).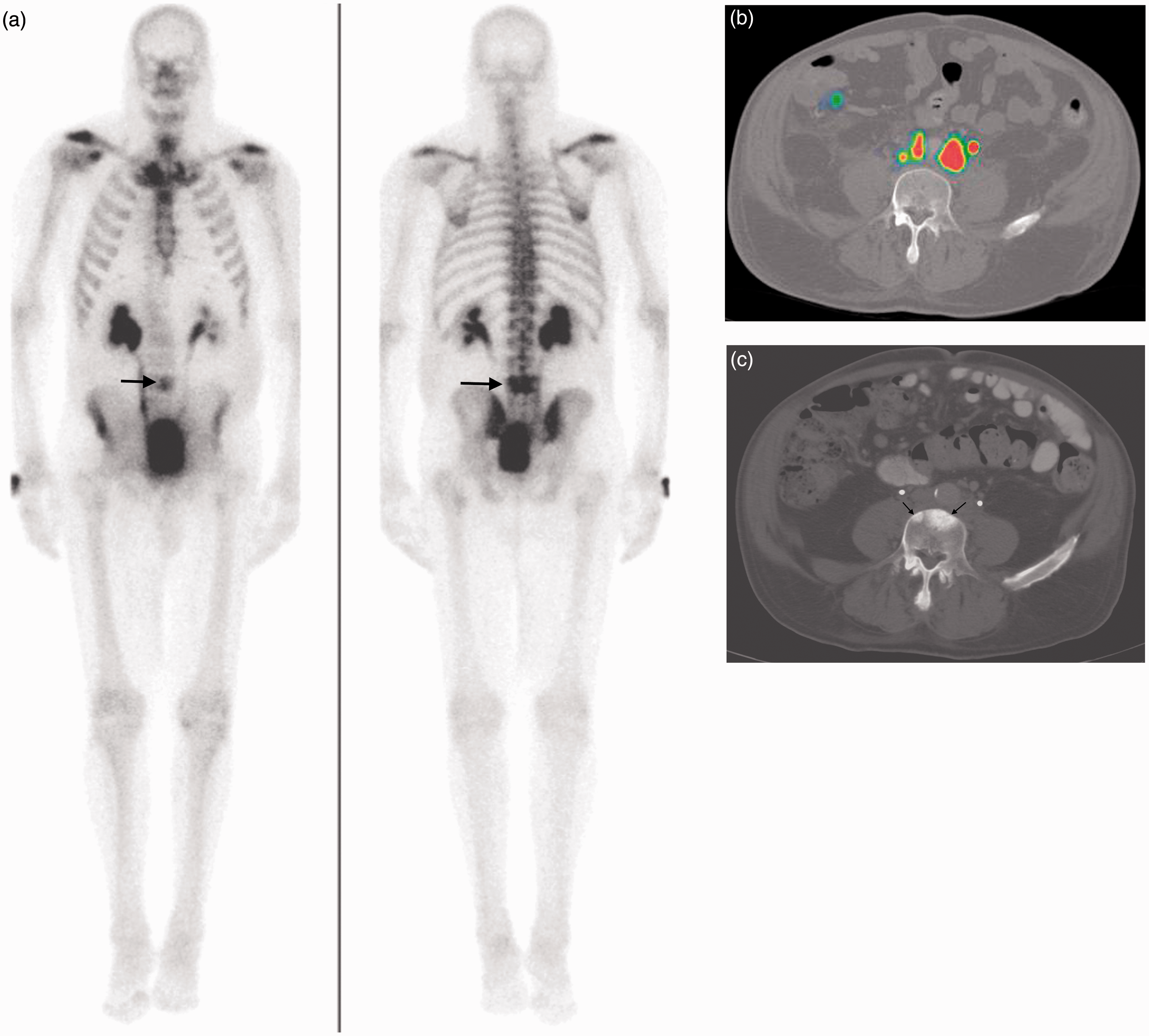
The cases missed with lesions missed by FDG PET/CT had the following tumor types: breast (n = 3) and other (n = 3).
FDG PET/CT false positive results
In three out of 202 cases (2%), there were areas of increased 18 F-FDG uptake on FDG PET/CT, without evidence of malignancy or metastatic disease on follow-up imaging (n = 2) or biopsy (n = 1). In one case, the FDG PET/CT falsely suggested metastatic lesions in three thoracic vertebrae, which showed no 99 m-Tc-MDP uptake on the concurrent bone scan and did not have abnormal 18 F-FDG uptake or abnormal findings on CT on a follow-up FDG PET/CT 5 years later. In a different case, FDG PET/CT identified an area of increased uptake in the acetabulum. The patient also demonstrated false positive radiotracer uptake of the thoracic spine on bone scan. All areas did not show metastatic disease on MRI or CT and remained normal on follow-up CT 1 year later, and these areas were presumed to represent normal marrow. In the third case, both FDG PET/CT and bone scan identified a region of increased uptake in the clavicle suspicious for metastasis. Histology from percutaneous biopsy showed fracture callus (Fig. 2).
Discussion
Our study showed that FDG PET/CT is an accurate technique for the detection of skeletal metastatic disease in a variety of malignancies with higher sensitivity and specificity when compared to bone scan.
Accurate assessment of skeletal metastases is important for staging, outcome, and treatment planning. Bone scan is the mainstay of assessment of skeletal metastatic disease; however, several studies have suggested that FDG PET/CT might be as accurate as bone scan in identifying skeletal metastatic disease. The advantage of FDG PET/CT is the ability to perform cancer staging of different organ systems in the same examination. Moon et al. (9) showed a sensitivity and specificity of 93% and 79% of FDG PET/CT for the detection of skeletal metastatic disease in a study of 57 breast cancer patients. In a meta-analysis of six studies comparing FDG PET/CT and bone scan for breast cancer patients, the calculated pooled patient-based sensitivity and specificity for FDG-PET were 81% and 93% and for bone scan were 78% and 79%, respectively (16). In a study by Moog et al. (14) of 56 lymphoma patients, FDG PET/CT detected all confirmed lesions identified on bone scan, but it also detected three additional lesions not identified on bone scan. In addition, bone scan had more sites of nonmalignant uptake, similar to the results of our study. Another meta-analysis of seven studies comparing FDG PET/CT and bone scan in lung cancer patients showed a pooled patient-based sensitivity and specificity for FDG-PET of 93% and 95%; and for bone scan of 87% and 82%, respectively (17). Our calculated sensitivities and specificities in a variety of tumors are similar to these results.
Among the sites missed by bone scan in our study, a large number involved the posterior ilium near the sacroiliac joint, the sacrum, the acetabulum and the femurs. This combination of normal, increased background uptake on bone scan in the pelvis near the sacroiliac joints and multiple overlapping osseous structures in the sacrum, pelvis, and proximal femurs may lower the sensitivity for lesion detection. Multiple or large lesions in these weight-bearing bones could potentially lead to pathologic fractures, a source of morbidity for cancer patients (1,18,19), especially as many patients with proven skeletal metastatic disease are asymptomatic (20,21). Bone scan also showed abnormal uptake in several benign lesions, which were thought to represent metastatic disease. FDG uptake was variable in these lesions – such as enchondroma in the humerus and Baastrup’s disease of the spine – but the CT appearance was diagnostic for non-malignant etiology. Using single-photo emission computed tomography (SPECT) imaging may be helpful due to its multiplanar capability in the evaluation of skeletal metastatic disease. SPECT/CT has had increasing applications for both soft tissue and osseous disease. Currently, SPECT and SPECT/CT are not routinely performed for skeletal metastases. FDG PET/CT has the benefit of detecting metastases in other organ systems, but SPECT and SPECT/CT allow for the use of a greater variety of different radionuclides (22–31).
The false negative FDG PET/CT L4 metastases with bone scan uptake shown in Fig. 3 is interesting. Ozulker et al. (15) describes two cases of sclerotic metastases missed by FDG PET/CT, but does not mention whether these cases were detected by bone scan. Ulaner et al. (32) describes one case of Ewing’s sarcoma which was not detected by FDG PET/CT but was seen on bone scan. This case had a sclerotic primary tumor. This bladder carcinoma metastasis was also sclerotic 10 months later on CT. Of note, the patient was also receiving chemotherapy (Taxotere and cisplatin) during this period of time, and the increased density of the metastasis on CT could represent treatment response.
FDG PET/CT missed several sites of disease. The majority of these sites were outside of its field of view. However, all of these patients also had additional sites of metastatic disease that were detected in the field of view, and missing these lesions did not change the staging. Two true sites of metastatic disease were missed on FDG PET/CT, one lesion in the spine and one recurrent lesion in the sternum adjacent to a previously resected metastasis. Two of the three false positive lesions on FDG PET/CT also had abnormal bone scan uptake, and biopsy or follow-up imaging was needed to arrive at the correct diagnosis.
Using a single examination for primary tumor staging and evaluation for metastatic disease reduces radiation dose and costs. The average dose for a FDG PET/CT is 16 mSv and for bone scan is 6 mSv. Limiting radiation exposure to one study is desirable, especially in young and radiosensitive cancer patients who frequently have multiple consecutive follow-up radiologic examinations.
The number of missed lesions for both PET/CT and bone scan was relatively low. Although we stratified the missed lesions by tumor type, the numbers were too small to draw any specific conclusions.
Our study had several limitations. First is the retrospective nature of the study. Second, histologic confirmation was not available in all patients; however, follow-up imaging was performed in those patients to confirm the presence or absence of metastatic disease. Strength of our study is the large number of patients with different types of tumors.
In conclusion, our study suggests that FDG PET/CT is a sensitive, specific, and accurate technique for the detection of skeletal metastatic disease that can be applied to a wide range of tumors, without the need for routine bone scan.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.