
Abstract
Background
Iodinated contrast agents (ICAs) are crucial to the use of many imaging studies. Reported allergies to ICAs in the medical record can interfere with optimal diagnostic imaging workups.
Purpose
To investigate the accuracy with which the label “allergic to ICAs” is applied.
Material and Methods
The medical records of 500 patients labeled “allergic to ICAs” at a single tertiary care hospital were reviewed. Patients were separated into three groups based on documentation in their medical records, as follows: Group 1, documented hypersensitivity reaction to ICAs; Group 2, documented ICA exposure with non-hypersensitivity adverse event (Group 2a) or without documented reaction (Group 2b); and Group 3, no documented prior exposure to an ICA. We then further reviewed the EMR to determine whether or not patients had subsequent administration of an ICA, whether or not they were given specific premedication, and whether or not they had a subsequent ICA-related event.
Results
A total of 16.6% of patients (n = 83) listed as “allergic to ICAs” had a documented hypersensitivity reaction following ICA administration (Group 1) while 58.6% (n = 293) of patients (Group 2) had a documented exposure to ICAs with either: (i) a non-hypersensitivity adverse event (23.5%, n = 69) or (ii) no record of a reaction to ICAs (76.5%, n = 224). The remaining 24.8% (n = 124), Group 3, had no record of exposure to an ICA, yet still carried the label.
Conclusion
The majority of patients carrying the label “allergic to ICAs” had no record of a prior hypersensitivity reaction to ICAs.
Introduction
Iodinated contrast agents (ICAs) are among the most widely used and safest of all pharmaceuticals. They play a major role in the growing utilization of many types of imaging. They are crucial to the use of computed tomography (CT), cardiac interventions, and other studies that are central to improving healthcare. By increasing the visibility of the organ or tissue being studied, they can enhance the detection and determine the extent of disease or injury (1). Additionally, ICAs are widely relied upon to improve conspicuity of many pathological conditions, increasing both the sensitivity and the accuracy of detection (2).
There is extensive literature on adverse reactions to ICAs. Classifications and incidence vary, based on the definitions as well as on the methodology of the specific study (3,4). Although the use of low-osmolality, non-ionic ICAs has reduced the incidence of many of these reactions (4–6), adverse reactions still occur in 0.15–3.13% of cases overall (6–11) and severe, potentially life-threatening reactions requiring acute intervention and hospitalization occur in 0.005–0.04% (6,7,9,11).
Some reactions to ICAs represent non-hypersensitivity adverse events. Examples include a feeling of warmth, nausea, vomiting, taste perversion, pain at the injection site, and subcutaneous extravasation. Such responses, whether or not classified as adverse events, largely correlate with the ionicity, osmolality, and perhaps specific formulation of the ICAs (4,12). The rate and volume of ICA administration may also play a role (4,13). Similar reactions often occur, although less frequently, in patients receiving non-ICA enhanced imaging studies, suggesting that ICA exposure alone may not be entirely to blame (14). Other adverse events, such as nephrotoxicity, are related to direct or indirect organ effects (4,12,15). On the other hand, hypersensitivity reactions to ICAs do not appear to be dose-related and, in general, are not clearly influenced by the specific ICA formulation (3,4,16,17). Many of these reactions seem to result from immunologic phenomena and, therefore, may result in positive skin tests (18). Examples of hypersensitivity reactions include urticaria, bronchospasm, hypotension with tachycardia, cardiovascular arrest, and delayed skin reactions (4,7,9,16,19,20).
Regardless of severity or etiology, non-hypersensitivity adverse events do not appear to predispose patients to subsequent and more severe hypersensitivity reactions. Conversely, a prior hypersensitivity reaction to an ICA does increase the risk of a recurrent reaction, although the likelihood and the level of severity remain unclear (17,21). The label “allergic to ICAs”, therefore, is not accurate in a classical sense and should ideally only be applied to those patients who experience hypersensitivity reactions to ICAs. Assignment of this label to patients without evidence of a prior hypersensitivity reaction could unnecessarily delay or even prevent those patients from receiving future important ICA-enhanced studies. To investigate the apparent accuracy of the label “allergic to ICAs” from the perspective of an ordering physician and the radiology department, we performed a retrospective electronic medical record review of 500 patients carrying this label.
Material and Methods
This study was approved by the Institutional Review Board. A waiver was given for informed consent, as this was a retrospective review. Using the electronic medical record (EMR) at a single academic tertiary care hospital, we identified and reviewed in detail the EMRs of the first 500 patients listed as “allergic to ICAs”, in 1999–2009, to investigate why the label was applied. Patient records were screened to determine at what point the label was entered into the EMR, which specific event(s) it was based on, what ICA-enhanced studies preceded that label, what ICA-enhanced studies were performed after the label was applied, and whether or not premedication was used either before or subsequent to the application of this label. Based on clinical documentation within the patient record, reactions to ICAs were divided into three broad groups: Group 1, documented hypersensitivity reaction to an ICA (including urticaria, bronchospasm, and shock); Group 2, documented exposure to ICAs with either a non-hypersensitivity reaction to an ICA (i.e. physiologic reactions such as localized swelling, warmth, flushing, nausea, vomiting, taste perversion, injection site pain, ICA extravasation) (Group 2a), or no documented reaction (Group 2b); and Group 3, no history of ICA exposure.
Only low-osmolality, non-ionic ICAs were used at the institution over the period of this study, and the type of ICA used was not changed. Initial review of the EMR was performed by one author (WV) and was subsequently reviewed and confirmed by two others (JM, MAB). Analysis was performed and reviewed by all authors.
Results
A total of 16.6% of patients (n = 83) fell into Group 1, with a clear, documented hypersensitivity reaction to an ICA (Fig. 1). Of these, 74.7% (n = 62) had urticaria documented as occurring after injection of an ICA. Group 2 contained 58.6% of patients (n = 293), with documentation of ICA exposure and no indication (in the EMR, in patient notes and radiology reports) of a hypersensitivity reaction. Within this group, 23.5% (n = 69) of patients had documented non-hypersensitivity adverse reactions to ICAs (Group 2a). About one-quarter of these patients (27.5%, n = 19) were noted to have “swelling”, with no evidence of bronchospasm, laryngospasm, or other specific manifestation. Thirty-eight patients (55.1%) in Group 2a were specifically labeled in the EMR as “allergic to ICAs” due to concerns about renal insufficiency. A further 17.4% (n = 12) had a documented non-hypersensitivity reaction to an ICA (e.g. warmth, flushing, nausea, taste perversion). Group 2b consisted of the remaining 76.5% (n = 224) of patients in Group 2. In these patients, extensive review of the EMR, including all radiology and cardiology reports, revealed clear documentation of administration of an ICA, but no record of any ICA-related adverse event or concern. About one-third of these Group 2b patients (32.6%, n = 73) were found to have had one or more subsequent, ICA-enhanced exams without premedication and without documented reaction. The final 24.8% of patients (n = 124) fell into Group 3. Extensive review of these patients’ EMRs showed no documentation from our institution or another institution indicating any ICA administration or reaction. There was no documentation of why this label had been applied to these patients.
Breakdown of patients by type of ICA reaction documented in the electronic medical record. Right: breakdown of the non-hypersensitivity reaction group.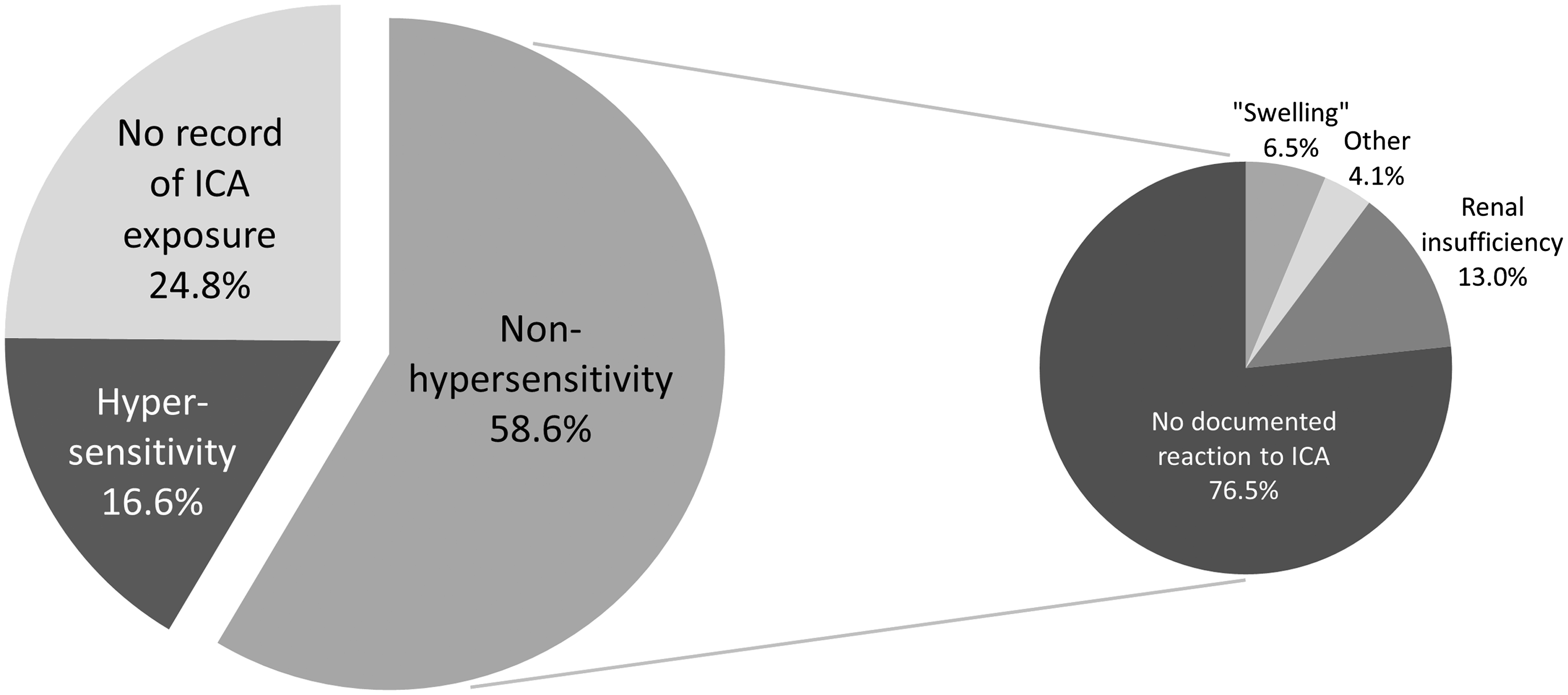
Discussion
We determined that patients labeled “allergic to ICAs” could be divided into three major groups based on EMR documentation: (i) prior hypersensitivity reaction to ICAs (i.e. the label appears to be accurate), (ii) prior exposure to ICAs without evidence of a hypersensitivity reaction; and (iii) no documented exposure to ICAs. The majority of patients labeled “allergic to ICAs” had no documented prior hypersensitivity reaction to ICAs.
In Group 1, most patients had documented urticaria without further anaphylactoid symptoms. This study did not identify any delayed-type cutaneous hypersensitivity reactions, perhaps because they are infrequent or perhaps because they are often not ascribed to ICA administration (4).
In Group 2, common documented non-hypersensitivity reactions to ICAs included warmth, localized pain or swelling, nausea, vomiting, anxiety, and taste perversion. Additionally, this group included patients thought to be at risk for, or who had previously developed, ICA-induced nephropathy. It is widely held that underlying renal insufficiency places patients at an increased risk of contrast-induced renal failure (3,4,15,22,23). However, labeling these patients as “allergic to ICAs” to encourage special attention when administering ICAs to them is not an optimal approach. If the renal failure resolves, the label is not likely to be removed. More importantly, there are now prophylactic measures that may prevent the development of ICA-induced nephrotoxicity (3,24). The use of ICAs in such patients should be optimized for the clinical situation, not altered by a misleading diagnosis. Finally, among patients with exposure to ICAs but no documented reaction, nearly one-third had multiple ICA-enhanced examinations that were performed without premedication and without adverse reaction after receiving the label. It was surprising that the label nonetheless remained in the EMR.
In Group 3, no documentation could be found as to why this label was entered into the EMR. These patients had no ICA-enhanced examinations at our institution and no documented reactions to ICAs. Of course, these patients may have had documented reactions to ICAs at outside institutions. It is possible that some of these patients had experienced remote reactions to older preparations of ionic, high osmolality ICAs and would tolerate newer formulations without problem. It is also possible that previous reactions to non-iodinated contrast media, such as gadolinium, may have been mistakenly reported by the patients or recorded as allergies to ICAs.
The label “allergic to ICAs” was entered into patients’ medical records by a variety of healthcare personnel, including nurses, nurse practitioners, pharmacists, and physicians. Failure of medical personnel to reevaluate and update the EMR is likely the reason for the persistence of this label in the medical records of patients who went on to receive ICA-enhanced studies without record of hypersensitivity reaction.
This study intentionally did not investigate the truthfulness of reported allergies to ICAs. As such, we did not review outside records, nor did we contact patients directly. Although both would have been of interest, our intent was to determine the apparent accuracy of the label “allergic to ICAs” from the perspective of an ordering physician or radiology department who also might not have access to outside records. We chose to focus solely on documentation of reactions to ICAs in the EMR rather than investigate the validity of those labels because documentation inevitably drives patient care, whether or not it is true. Also, due to inconsistent documentation of the physician thought process when ordering studies, we were unable to quantify the effect of the label on patient care. That is, it is not evident whether or not certain imaging studies were delayed or avoided entirely due to the label. It is very likely, however, that both occurred. On the other hand, the review of records clearly demonstrated that some patients did have ICA-enhanced studies despite this label, often without premedication. This finding is likely due to either inattention to the label, or to a conscious decision to ignore it. However, it is safe to assume that, in some instances, the label led to delay or avoidance of subsequent ICA-enhanced imaging studies.
There are shortcomings to this study, as noted. Additionally, it is only a sample, albeit a fairly large one, of patients from a single institution. It is possible, although unlikely, that the results might be different over a different time frame, with a larger group, or at other similar institutions. The label in the EMR may have been entered in error, or as a caution due to perceived risk factors, such as renal dysfunction. Nonetheless, the findings are an accurate reflection of the EMR. Patients might have been able to supply additional information that would have, in certain cases, validated the entry. Anecdotally, however, we have found that when such patients are questioned, they indicate that they have been told that they are allergic to ICAs, but are generally unable to provide details.
In conclusion, the apparent accuracy of the label “allergic to ICAs” in the EMR of a tertiary care hospital was only 16.6%. The label was more commonly reflective of unknown reactions or non-hypersensitivity adverse reactions than it was of true hypersensitivity reactions to ICAs. It is apparent that further education of the medical community is warranted to appropriately and accurately document adverse events that relate to ICAs.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.