
Abstract
Background
Incidental renal cysts are a very common finding in routine lumbar spine magnetic resonance imaging (MRI). However, there is no report of the renal cyst detection rate on routine lumbar spine MRI.
Purpose
To determine the renal cyst detection rate in routine lumbar spine MRI based on findings of abdominal computed tomography (CT), and to investigate if the largest renal cyst seen by abdominal CT could be also detected by routine lumbar spine MRI.
Material and Methods
A retrospective study was conducted of 70 patients who underwent both routine lumbar spine MRI and abdominal CT between December 2011 and January 2014. The detection rate of all renal cysts>5 mm as well as the largest renal cyst seen by abdominal CT were assessed in routine lumbar spine MRI.
Results
On routine lumbar spine MRI, the detection rate of renal cysts was 46.5% (73/157) for>5-mm renal cysts and 68.0% (34/50) for>10-mm renal cysts, correlating with abdominal CT. The detection rate of the largest renal cyst seen by abdominal CT was 60.0% (27/45). Non-detection of the largest renal cyst could be caused by upper positioning (n = 7), lateral positioning (n = 6), or relatively small cyst size (n = 5).
Conclusion
Approximately half of renal cysts>5 mm and two-thirds of renal cysts>10 mm were detected on routine lumbar spine MRI. However, radiologists should be aware that kidney lesions may not be included in the scan coverage of routine lumbar spine MRI.
Introduction
Routine lumbar spine magnetic resonance image (MRI) in the axial plane usually scans parts of abdominal organs in addition to vertebral bodies and the spinal canal. These scans can result in incidental findings of the abdominal organs such as abnormalities of vessels, kidneys, adrenal glands, uterus, ovaries, prostate gland, bladder, bowel, liver, spleen, and lymph nodes (1–4). Cystic lesions of the kidney are the most common incidental finding and the incidence of renal cysts increases with age. The incidence of detecting renal cystic lesions during routine lumbar spine MRI for evaluation of lower back pain can be as high as 35.5%. However, one study reported that only 4% of incidental renal cystic lesions were described in radiologic reading reports, perhaps because of the limited interest of the interpreting radiologists (3).
Although the detection of incidental renal lesions has important clinical implications, to our knowledge, no reports have compared the detection rate of kidney lesions on routine lumbar spine MRI and abdominal CT. The purposes of our study were to: (i) determine the renal cyst detection rate on routine lumbar spine MRI for patients with complaints of low back pain with reference to the findings of abdominal CT; and (ii) investigate whether the largest renal cysts seen on abdominal CT were also detected on routine lumbar spine MRI.
Material and Methods
Case selection
Our study population included 70 patients (male:female ratio, 31:39; age range, 29–87 years; average age, 62.9 years) with complaints of low back pain and clinically suspected intervertebral disc disease who underwent both routine lumbar spine MRI and abdominal CT between December 2011 and January 2014. The interval between lumbar spine MRI and abdominal CT was 0–22 months with an average of 5.9 months. Patients with vertebral compression fracture of the thoracolumbar junction were excluded. This retrospective study was approved by the Institutional Ethics Review Board. Informed patient consent was not required.
Parameters of MRI and CT
Lumbar spine MRI was performed on a 1.5 T MRI system (Signa Horizon; GE Healthcare Systems, Milwaukee, WI, USA) according to the standard protocol for spinal MRI. Each study included sagittal T1-weighted (T1W) images, sagittal T2-weighted (T2W) images, fat suppressed sagittal T2W images, and axial T2W images with fast spin-echo sequence as the routine protocol. Axial T1W images were not included in our hospital’s routine protocol. We used only axial T2W images in the study. Axial T2W fast spin-echo sequences from the T12–L1 level to the L5–S1 level were conducted with following parameters: TR/TE, 3300/110; matrix size, 320 × 224; field of view (FOV), 18 × 18 cm; slice thickness, 4.5 mm; intersection gap, 0.3 mm; echo train length, 32; read-out bandwidth, 162 Hz/Px; NEX, 2; and flip angle, 90°. An 8-channel C-T-L Spine Array GE coil was used. Axial images had a FOV appropriate for covering the area of interest and included levels of at least the lowest three lumbar discs, corresponding to the American College of Radiology guidelines (5).
Abdominal CT was performed using a 64-channel CT system (GE LightSpeed VCT, GE Healthcare). Each study included a portal venous phase with 2.5 mm section thickness after intravenous contrast injection. Reasons for undergoing abdominal CT included abdominal pain (n = 36), routine cancer follow-up (n = 10), dyspepsia (n = 9), constipation (n = 3), hematuria (n = 3), trauma (n = 3), sonographic hepatobiliary abnormality (n = 2), incidental renal cyst detected on routine lumbar spine MRI (n = 2), routine renal cyst follow-up (n = 1), and inguinal hernia (n = 1). No patients underwent abdominal CT for evaluation of lower back pain.
Image analysis
Abdominal CT examinations were interpreted by a fellowship-trained abdominal radiologist with 20 years of experience. MRI exams were interpreted by a fellowship-trained musculoskeletal radiologist with 8 years of experience. The abdominal radiologist evaluated axial CT images of the portal venous phase to determine the number of renal cysts larger than 5 mm and larger than 10 mm. Subsequently, the size and location of the largest renal cyst on each abdominal CT image was evaluated. Cysts smaller than 5 mm were excluded from counts because of ambiguity. The musculoskeletal radiologist evaluated the number of renal cysts seen on abdominal CT that were also detected by routine lumbar spine MRI. Detection rate of all renal cysts seen by abdominal CT and mean size of the cysts were assessed in routine lumbar spine MRI. Detection rate of the largest renal cyst seen by abdominal CT was also evaluated in routine lumbar spine MRI.
Statistical analysis
A chi-square test was used to analyze the relationship between the size of the renal cyst and detection rate of the renal cyst on routine lumbar spine MRI.
Results
Of the 70 patients included in this study, none had renal cell carcinoma (n = 0/70, 0%). One or more renal cysts larger than 5 mm were detected in 45 patients (n = 45/70, 64.3%) on abdominal CT and the total number of renal cysts was 157 (average 3.5/patient). All renal cysts were included in Bosniak classification 1 (n = 39, 86.7%) or 2 (n = 6, 13.3%) based on abdominal CT. On routine lumbar spine MRI, 73 renal cysts were detected from among the 157 cysts seen by abdominal CT. The detection rate of routine lumbar spine MRI for all renal cysts larger than 5 mm was 46.5% (n = 73/157) based on abdominal CT. For 16 of 45 patients, no renal cysts were detected by routine lumbar spine MRI (false negative rate=35.6%).
Detection rate for renal cysts (>5 mm vs.>10 mm) by L-spine MRI with correlation with abdominal CT.

CT, computed tomography; L-spine MRI, lumbar spine magnetic resonance imaging.
We selected the largest renal cyst larger than 5 mm from each abdominal CT scan of 45 patients who had one or more renal cysts. Of these 45 largest renal cysts seen by abdominal CT, 27 were also detected by routine lumbar spine MRI, resulting in a detection rate of 60.0% (n = 27/45) and a false negative rate of 40.0%. Limiting the size of the largest renal cyst to larger than 10 mm resulted in a detection rate of 80.0% (n = 20/25) and a false negative rate of 20.0%.
Levels of the largest renal cysts detected by routine lumbar spine MRI were T12–L1 (10 cysts, 37.0%), L1–2 (11 cysts, 40.7%), and L2–3 (6 cysts, 22.2%). Causes of non-detection of the largest renal cyst by routine lumbar spine MRI were upper positioning (7 cysts, 38.9%), lateral positioning (6 cysts, 33.3%), and relatively small cyst size (5 cysts, 27.8%).
Detection rate for the largest renal cysts by L-spine MRI and correlation with abdominal CT.

CT, computed tomography; L-spine MRI, lumbar spine magnetic resonance imaging.
Discussion
High-quality radiology interpretation requires that radiologists can detect incidental findings by various imaging modalities. The ability of radiologists to detect renal cysts incidentally on images such as lumbar spine MRI is clinically important. In particular, detecting low-grade incidental renal cell carcinoma can contribute to better patient survival and decreased tumor recurrence (6). Usually, radiologists and clinicians decide about malignant risk, required follow-up and treatment plans using Bosniak classification of CT findings (7). In our study, two patients with septated renal cysts larger than 5 cm on spine MRI underwent subsequent abdominal CT for Bosniak classification and were diagnosed with Bosniak class 2 based on the CT findings (Fig. 1).
A 70-year-old woman with an incidentally found large renal cyst. (a) Lumbar spine MRI reveals incidental renal cysts. Left renal cyst is 53 mm and shows an inner septum on axial T2W image (arrow). (b) Abdominal CT for evaluation of renal cysts shows a larger left renal cyst with Bosniak classification 2 and a smaller right renal cyst with Bosniak classification 1.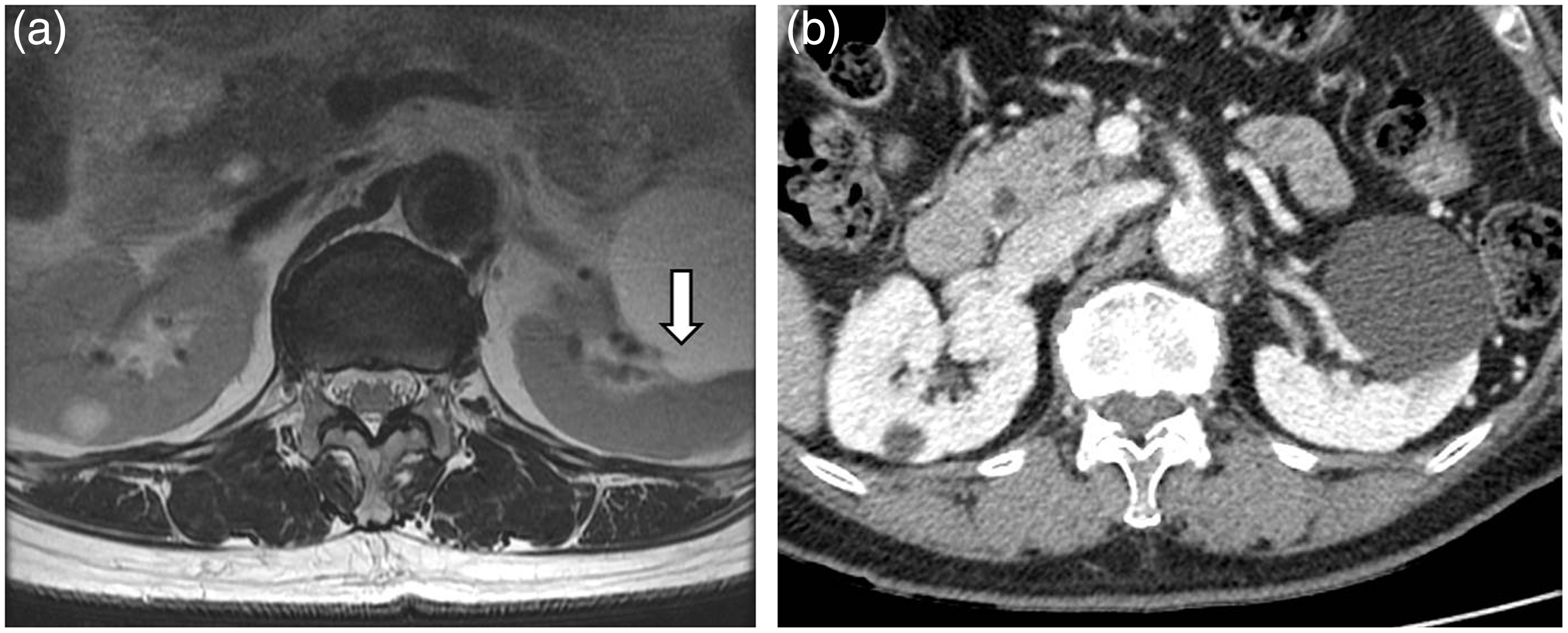
Because the axial FOV of routine lumbar spine MRI usually covers the renal region, part or all of an incidental renal lesion can be easily distinguished on axial images. However, referring physicians who ordered spine MRI and some radiologists fail to detect incidental renal lesions when analyzing spine MRI images. A possible reason for this oversight could be lack of confidence in the spine MRI detection rate for renal lesions, which is related to routine lumbar spine MRI generating axial images only at disc levels. Another potential reason for the failure to detect incidental renal lesions on routine lumbar spine MRI is that most intervertebral disc problems occur at lower lumbar levels while the position of the kidney is usually at the level of the T12 to L3 vertebral bodies (8). Therefore, being knowledgeable about the reliability of routine lumbar spine MRI for detection of renal cysts is important for radiologists who interpret routine lumbar spine MRI.
In our study, 73 of 157 renal cysts larger than 5 mm were detected on routine lumbar spine MRI resulting in a detection rate of 46.5%. When analysis was limited to renal cysts larger than 10 mm, i.e. potentially more impactful renal cystic lesion, the detection rate increased to 68.0% (34 of 50), which was statistically significant (P < 0.05), suggesting that larger renal cysts have a greater chance of detection on routine lumbar spine MRI. Of course, smaller renal cysts may not be found with high probability on routine lumbar spine MRI. We considered other cyst size cutoff values such as 2 cm or 3 cm, but the number of matching cysts was too small for sufficient evaluation. Only 12 cysts were larger than 2 cm and seven were larger than 3 cm.
In this study, we determined the detectability on routine lumbar spine MRI of the largest renal cysts primarily seen by abdominal CT. The main purpose of the study was to predict the possibility of incidental detection of clinically important lesions such as renal cell carcinomas, even though no cases of renal cell carcinoma were observed in this study because of the small number of patients. We selected the largest renal cysts as study targets for ease and accuracy of assessment and because renal cyst size is clinically important. For example, the well-known Bosniak classification uses a 3 cm criterion when distinguishing hyperdense cysts of class 2 from 2 F. Moreover, a recent study reported that malignancy is significantly associated with renal cyst size (9). In future studies of larger patient populations, we plan to continue to evaluate incidence of incidental renal cell carcinoma on routine lumbar spine MRI.
Only 27 cysts were detected on routine lumbar spine MRI from 45 largest cysts in 45 patients that were visualized by abdominal CT, resulting in a detection rate of 60.0% and a false negative rate of 40.0% (18 of 45). When analysis was limited to cysts larger than 10 mm, 25 patients had one or more renal cysts larger than 10 mm and the MRI detection rate for the largest renal cyst was 80.0% (20 of 25) with a false negative rate of 20.0% (5 of 25). This result was statistically significant (P < 0.05). We concluded that the larger the renal cyst, the higher the chance of detection on routine lumbar spine MRI. The mean sizes of the 45 largest renal cysts were 18.6 mm on CT and 17.1 mm on MRI. Limiting the size of the largest renal cyst to larger than 10 mm, mean sizes of the detected largest renal cysts were 23.4 mm on CT and 24.4 mm on MRI.
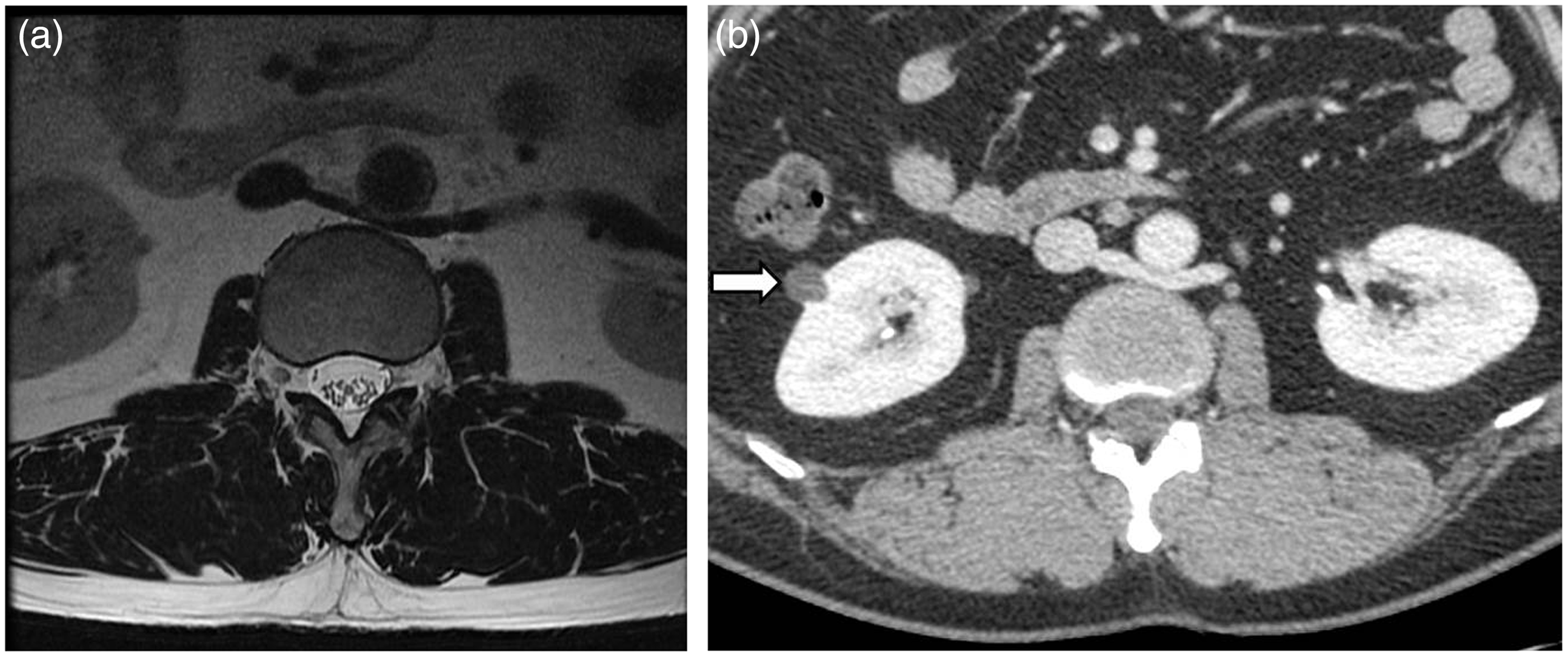
Our analysis of the undetected largest renal cysts on MRI from 18 patients indicated that these cysts were positioned in the upper part of the kidney rather than at T12–L1 disc level (n = 6), had lateral positioning out of the FOV (n = 7), or had a relatively small cyst diameter (<6 mm) (n = 5). This analysis was clinically important because it indicated that a clinically significant renal lesion may go undetected on routine lumbar spine MRI if located in the upper portion of the kidney (Fig. 2) or beyond the FOV in obese patients (Fig. 3). However, the detection rate may be greater when the renal lesions are located in the lower portion of the kidney, when the interval space between discs is relatively small because of osteoporosis or vertebral compression fracture, or in relatively thin patients.
An 82-year-old man with an upper polar renal cyst. (a) Axial T2W image of the highest T12–L1 level by lumbar spine MRI shows no kidney lesion. (b) Abdominal CT after a few weeks for evaluation of trauma shows a 36-mm cyst in the upper portion of the left kidney. A 47-year-old man with body mass index>23. Lateral kidney portions are not visible. (a) No visible renal cysts on axial T2W images of lumbar spine MRI with FOV of 18 cm. (b) Abdominal CT after 2 months for evaluation of constipation shows a 13-mm cyst with septation in the lateral portion of the right kidney, Bosniak classification 2 (arrow).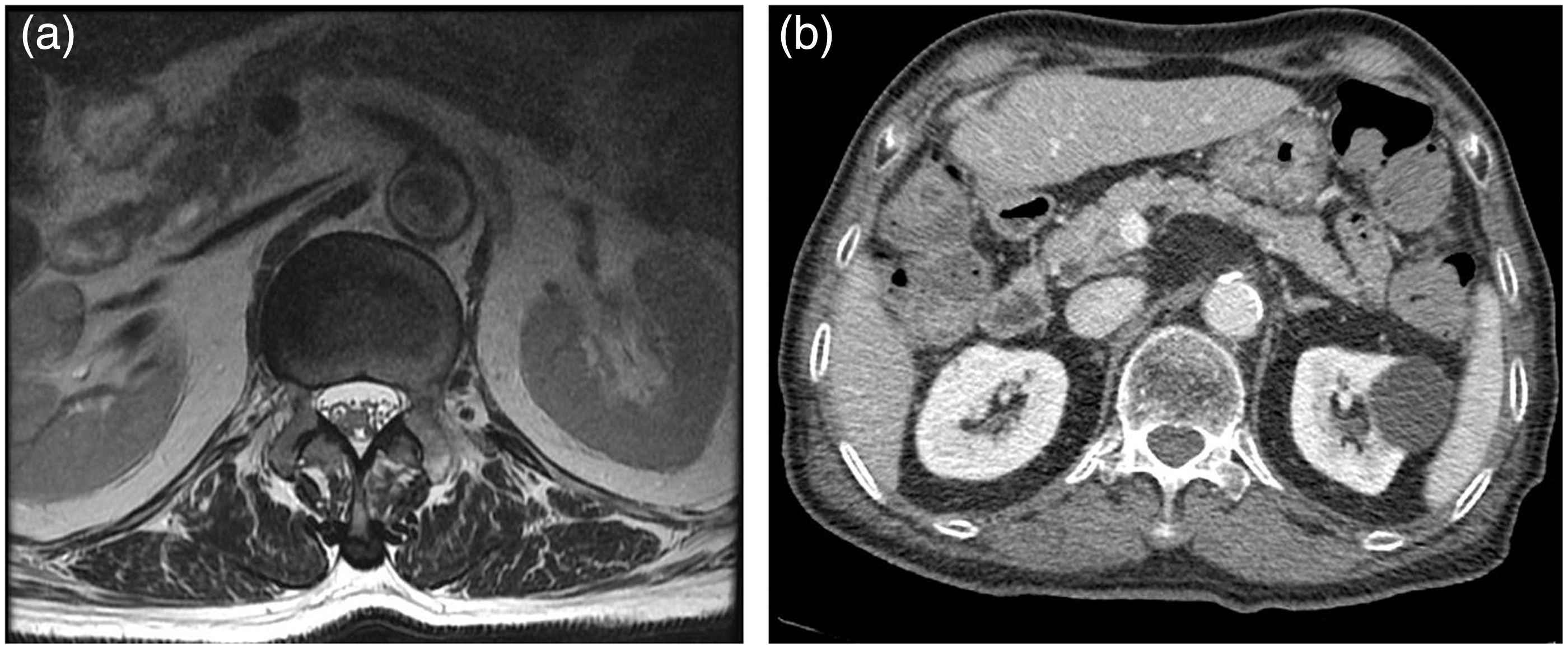
Once a renal cyst was detected on routine lumbar spine MRI, the contour of the thin septa or wall could be seen more clearly on T2W axial MRI images than on CT images (Fig. 1). T1W axial images or postcontrast images can be helpful for evaluating hyperdense renal cysts (10).
Levels of the 27 detectable largest renal cysts were T12–L1 (n = 10, 37.0%), L1–2 (n = 11, 40.7%), and L2–3 (n = 6, 22.2%). This result is important because routine MRI protocols may differ, depending on where the MRI is performed. In institutions where axial images of the T12–L1 level are not routinely obtained, unlike at in our hospital, we estimated that the detection rate of the largest renal cysts on routine lumbar spine MRI would decline from 60.0% (27/45) to 37.8% (17/45).
There were several limitations to this study. First, renal cysts smaller than 5 mm were excluded even though some of these minimally sized cysts may have a more definite wall contour on MRI than on CT. This limitation could be an important difference between research findings and clinical situations. Second, because of the time interval of up to 22 months between CT and MRI, we cannot exclude the possibility that some renal cysts changed size, shape, or number during this period. Finally, results may vary because other institutes may employ different routine MRI protocols or parameters. For example, additional coronal T2W images or a wider axial FOV may increase the renal cyst detection rate. And we need to know that a wider axial FOV than used in our analysis could be helpful for evaluation of non-specific symptoms as well as detection of renal lesions.
In conclusion, 73 of 157 (46.5%) renal cysts larger than 5 mm were detected on routine lumbar spine MRI. When limiting the size of analyzed cysts to larger than 10 mm, the detection rate was significantly higher, at 34 of 50 (68.0%). This finding suggests that larger renal cystic lesions can be detected more easily than smaller lesions on routine lumbar spine MRI. And these incidental kidney lesions seen by routine lumbar spine MRI could be clinically important because of their large size. However, radiologists should be aware that kidney lesions might not be included in the scan coverage of routine lumbar spine MRI.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MEST) (2012R1A2A1A01011328).