
Abstract
Background
Tumor volumetry with magnetic resonance imaging (MRI) is very common; however, the accuracy of such measures remains unclear, especially after treatment.
Purpose
To determine the accuracy of preoperative volume measurements of uterine cervical carcinomas resected with and without neoadjuvant chemotherapy (NAC) on T2-weighted (T2W) and diffusion-weighted (DWI) MRI.
Material and Methods
Twenty-nine consecutive patients with surgically confirmed uterine cervical carcinoma were included in this study. MRI scans were performed before preoperative treatment in 17 patients and after two courses of NAC in 12 patients. In all patients, T2W images and DWI were obtained to measure the tumor diameters. The maximum diameter of the surgical specimens was macroscopically measured. The correlation coefficients between the measured tumor size using T2W imaging and DWI and the size measured on the surgical specimens were calculated for all specimens.
Results
The correlation coefficient of the three-dimensional (3D) tumor volume measurement using T2W imaging and DWI was 0.97 in the primary surgery group and was 0.96 in the NAC group. The 3D tumor volume measurement using MRI and the measurement of the actual surgical specimen was 0.55 for T2WI and 0.48 for DWI in the primary surgery group and 0.88 for T2WI and 0.95 for DWI in the NAC group.
Conclusion
T2WI and DWI can provide accurate 3D tumor volume measurements of uterine cervical carcinomas in patients with and without preoperative chemotherapy, suggesting that tumor volumetry using 3 T MRI after uterus-preserving treatment is feasible.
Introduction
Tumor size is one of the most important prognostic factors for uterine cervical carcinoma and is used by the revised staging criteria established by The Federation of Gynecology and Obstetrics (FIGO) (1) and the revised criteria of the new response evaluation criteria in solid tumors (RECIST) (2). The maximum tumor diameter (the two-dimensional [2D] tumor measurement) is used by both systems. It is unclear whether the 2D or the three-dimensional (3D) measurement is better correlated with the true tumor volume. T2-weighted (T2W) images obtained using magnetic resonance imaging (MRI) are generally used for evaluating uterine cervical cancer (3–5). The utility of diffusion-weighted images (DWI) in oncological imaging has also been established (6,7). However, the direct correlation between the tumor volume measured via imaging and the volume measured of the actual surgical specimen has not been completely elucidated (8).
Some clinical trials have demonstrated that treatment with neoadjuvant chemotherapy (NAC) for advanced uterine carcinoma is feasible and effective (9,10). However, the correlation between tumor volume measured using preoperative T2W images or DWI and the surgical specimen in patients treated with NAC has not yet been reported.
Therefore, the aims of this study included the following: (i) determine the more accurate measurement method (measurement of maximum diameter or 3D tumor volume using T2W imaging); (ii) investigate the feasibility of preoperative DWI obtained using 3 T MRI for tumor volumetry; and (iii) investigate whether tumor volume in patients who undergo NAC can be accurately measured using preoperative 3 T MRI.
Material and Methods
This was a retrospective, single-center analysis. The study was approved by the institutional review board (No. H25-64). Because this study was performed retrospectively, informed consent from each patient was not required.
Patient selection
From January 2009 to December 2011, 183 patients with newly suspected invasive uterine cervical carcinoma underwent preoperative MRI. The exclusion criteria are listed in Fig. 1. Sagittal and axial T2W images (parallel and perpendicular to the uterine cervix) were obtained for all patients; however, we obtained DWI with a resolution that was high enough to calculate tumor diameter in only 17 participants in the primary surgery group and 12 participants in the NAC group. Therefore, 29 participants were included in this study (Fig. 1). The clinical staging was IB1 in 16 participants and IB2 in one participant in the primary surgery group. In the NAC group, the clinical staging was IB1 in one participant; IB2 in two participants; IIA1 in one participant; and IIB in eight participants. The histopathological diagnosis was: squamous cell carcinoma (n = 13); adenocarcinoma (n = 3); adenosquamous carcinoma (n = 1); and neuroendocrine carcinoma (n = 0) in the primary surgery group and eight, three, zero, and one in the surgery with NAC group, respectively.
Patient selection.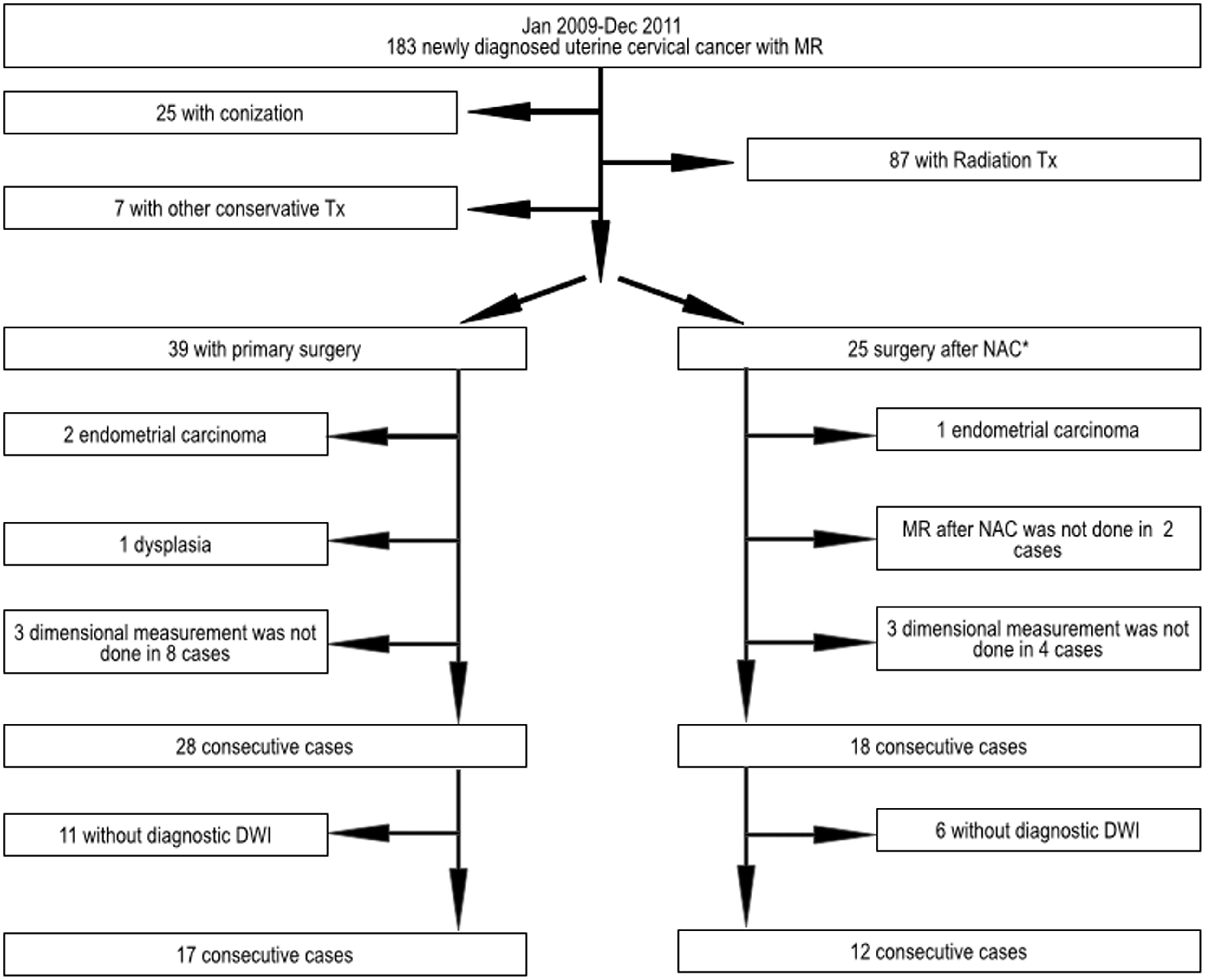
MRI protocol and surgical specimen measurements
MRI was performed using a 3 T-superconducting unit (Gyroscan, Philips Healthcare, Best, The Netherlands) with a phased-array body coil. Butyl scopolamine (Buscopan, Boehringer Ingelheim, Ingelheim am Rhein, Germany) was intramuscularly administered prior to imaging to decrease bowel peristalsis. Sagittal T2W imaging (parallel and perpendicular to the uterine cervical axis) with a 28-cm field of view were obtained for all participants using a fast spin-echo sequence (repetition time [TR]/echo time [TE], 1400–1800/99–100 ms; echo train length, 19; slice thickness, 3 mm with a 0.3-mm intersection gap; SENSE factor 1.5; excitations, 2; matrix, 512 × 512) (Fig. 2a and b). DWI were also obtained for all participants, and images perpendicular to the uterine cervical axis were obtained using echo-planar imaging (TR/TE, 5000/55 ms; echo train length, 19; slice thickness, 3 mm with a 0.3-mm intersection gap; excitations, 2; b value, 1000 s/mm2; matrix, 256 × 256).
A 61-year-old woman with stage IIb uterine cervical cancer in the primary surgery group. (a) Axial T2W image indicating the cutline of the sagittal plane. (b) Sagittal T2W image indicating the cutline of the axial plane. (c) Axial T2W image and (d) DWI demonstrating the measurement of the largest transverse (“RL” in (c, d) and longitudinal diameters of the tumor (“SI” in (e)). Sagittal T2W image demonstrating the measurement point of the vertical diameter. The transverse (“RL”) and vertical (“AP”) diameters of the surgical specimen are measured on the specimen cut at the anterior median line after fixation (f). The longitudinal diameter (“SI”) of the surgical specimen is measured on the fragment cut in a radial fashion (g).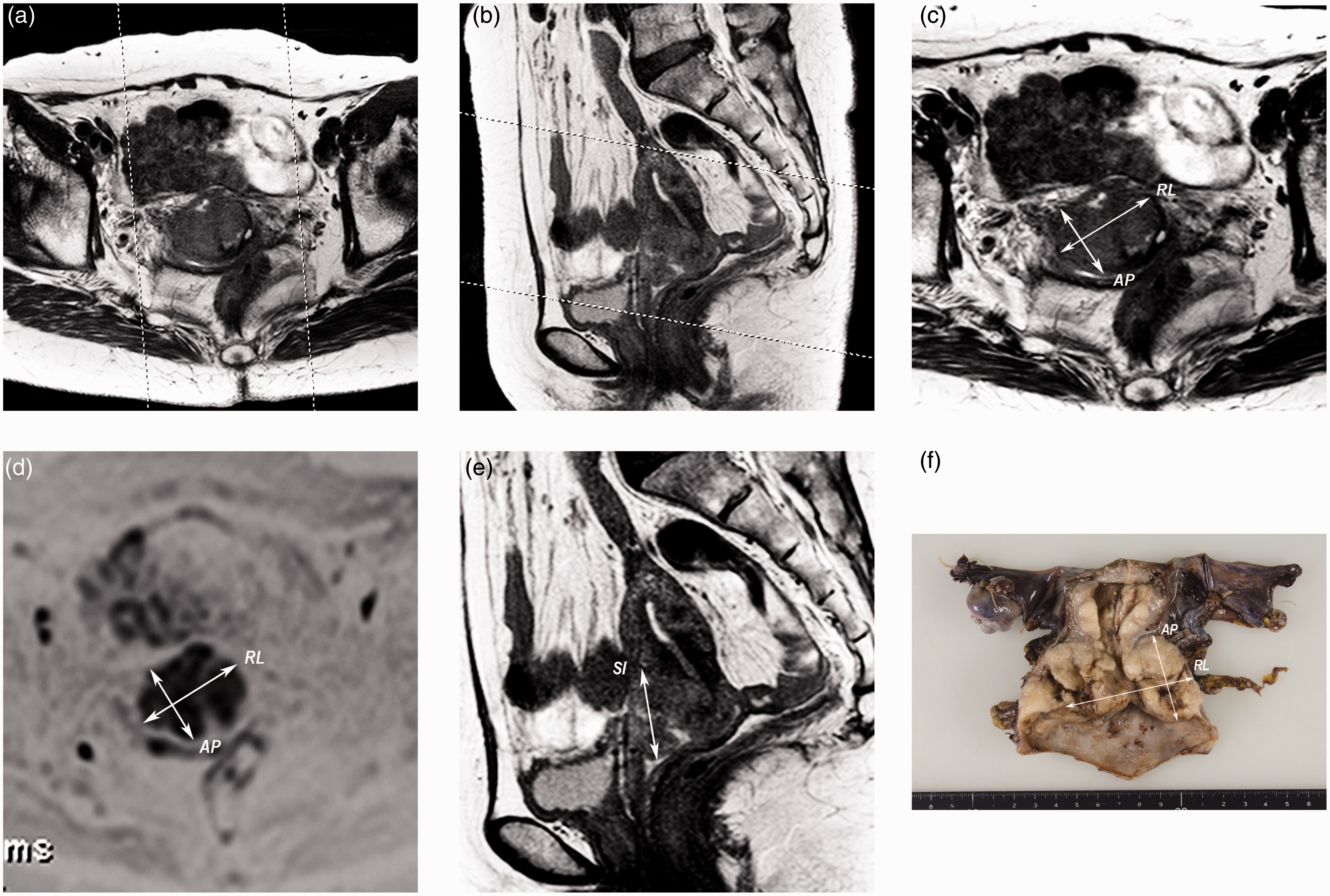
A board-certified radiologist retrospectively measured the largest diameter in 3D without clinical information regarding the staging. The longitudinal and transverse diameters on the axial T2W imaging and DWI (perpendicular to the cervix) (Fig. 2c and d) and the vertical diameter were directly measured on the sagittal T2W imaging (Fig. 2e) on an image viewer (R1000, GE Healthcare IT, Barrington, IL, USA). The vertical diameter was obtained using the sum of the number of axial planes passing through the tumor on the DWI.
The maximum diameters of the surgical specimens were recorded by reference to the official pathological report of our institute (Fig. 2f and g). However, the pathologists recorded the maximum diameter in 3D for only 12 cases (because the tumor invasion depth was too small to be measured in most subjects). The product of the three dimensions of each tumor was used as the 3D tumor volume for both MRI and specimen measurements.
Statistical analysis
Maximum tumor diameter versus 3D tumor volume
Twenty-eight consecutive participants undergoing primary surgery and 18 participants undergoing NAC followed by surgery with and without diagnostic DWI were analyzed. Tumor measurement comparisons were possible only with T2W imaging. We obtained correlation coefficients (Pearson r) between the maximum tumor diameter and the 3D tumor volume measured with T2W imaging and the volume measured on the surgical specimens for all participants in each group. The exact two-tailed (binominal distribution) P values were calculated (Prism 5, GraphPad Software Inc., La Jolla, CA, USA).
Relationship between the tumor sizes measured with T2WI and DWI
The correlation coefficient between the maximum tumor diameter measured with T2W imaging and DWI in 17 participants in the primary surgery group and 12 participants in the NAC group was obtained. The correlation coefficient between the tumor volumes measured with T2W imaging and DWI for all subjects was obtained for each group. The exact two-tailed (binominal distribution) P values were determined for each of the correlation coefficients.
3D tumor volumetry: primary surgery group versus NAC group
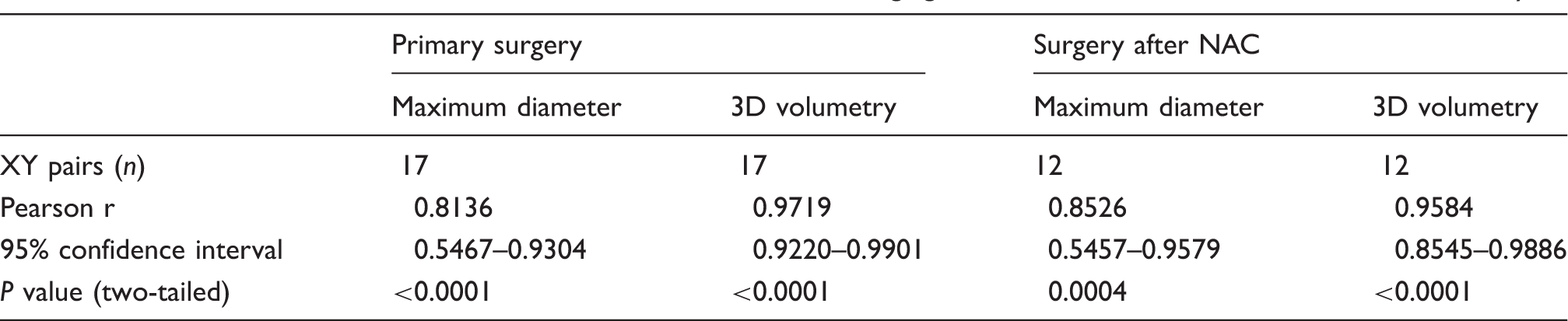
We obtained the correlation coefficient between MRI-measured tumor size (maximum diameter and 3D tumor volume) and surgical specimen-measured tumor size in 17 participants in the primary surgery group and 12 participants in the NAC group. The exact two-tailed (binominal distribution) P values were obtained for each group.
Results
Maximum tumor diameter versus 3D tumor volume
Correlation coefficient between T2W imaging and surgical specimen: Maximum diameter versus 3D volumetry.

Relationship between tumor sizes measured with T2W imaging and DWI
Correlation coefficient of the tumor volume between T2W imaging and DWI: Maximum diameter and 3D volumetry.
3D tumor volumetry: primary surgery group versus NAC group
Correlation coefficients of the tumor volume measured on MR and surgical specimen: Cases with primary surgery versus surgery after NAC.

Discussion
Uterine cervical carcinoma is still one of the leading causes of cancer-related death among women (11). The staging classification is important because the stage and prognosis are well correlated. In the FIGO classification system, stage IB and IIA diseases are divided into subcategories according to tumor size (>4 cm or ≤4 cm) (1), and tumor size is also correlated with prognosis (2,12,13). The general rules for clinical and pathological management of uterine cervical cancer suggest that the tumor volumetry should be performed on the cut specimen (Fig. 2f and g) (14). In contrast, most radiologists measure the tumor volume according to the largest length in the sagittal or axial plane. Therefore, the largest diameter measured using MRI and using surgical specimens may differ from each other. Therefore, the maximum diameter measured using MRI and the surgical specimens are not well correlated. Therefore, we used the 3D volume rather than the maximum diameter for further examinations.
Tumor volumetry using MRI plays an important role in diagnosing uterine cervical cancer. Tumor volume measured using T2W imaging is well correlated with the measurements from the surgical specimens (3,4,15). After contrast materials became widely used, the utility of dynamic contrast studies visualizing uterine cervical carcinoma was reported (16,17); however, contrast-enhanced MRI was not routinely used due to lower cost effectiveness (18). In contrast, DWI is widely used to evaluate uterine cervical carcinoma (6,7,19) because it does not require contrast material and requires only a few more seconds of examination time (19,20). However, the accuracy of tumor volumetry using DWI and the relationship between volumetry using T2W imaging and DWI has not been fully defined. Our results revealed that tumor volumes measured using T2W imaging were well correlated with measurements using DWI demonstrating the feasibility of DWI for tumor volumetry.
In our study, the tumor volumes measured using MRI were more highly correlated with the measurements of the surgical specimens in the NAC group. We speculate that inflammation caused by biopsy or bleeding prior to the MR in the primary surgery group led to inaccurate MRI measurements. In addition, tumors treated by NAC may have more defined margins because scattered tumors at the periphery of the masses may disappear as a result of the chemotherapy. Although it was not clear why tumor volumetry was more accurate in the NAC group, our study revealed that both T2W imaging and DWI could measure tumor volumes accurately, even following chemotherapy. Tumor volume after radiation is not accurate using T2W imaging (21), but residual disease can predict recurrence (22). However, there have been no reports concerning MRI tumor volumetry after NAC for invasive cervical carcinoma. Recently, the advantages of NAC before radical hysterectomy in patients with bulky tumors was reported (10). Therefore, we believe that there is clinical value in determining the accuracy of MRI volumetry after NAC.
There were some limitations in this study. First, the number of patients was relatively small because most patients with invasive cervical carcinoma were treated with CCRT. A study with a greater number of cases is required before drawing a reliable conclusion on the utility of MRI for tumor volumetry after preoperative NAC. Second, we could not include participants with tumors that were not large enough to measure in 3D by the pathologists’ gross inspection, which may have introduced bias. Third, DWI with a quality that was high enough to measure the tumor volume was not always obtained because of the artifacts primarily generated from intestinal gas; this susceptibility may have been exaggerated by the use of 3 T MRI. Efforts should be undertaken to decrease the volume of gas within the rectum and colon, including the use of glycerin enemas, before MRI.
In conclusion, the tumor volume measurements using T2W imaging and DWI were well correlated with each other and with tumor volume measured using surgical specimens with an acceptable margin of error. Our study also suggested that tumor volumetry using 3 T MRI can be accurate, even in patients that undergo NAC.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not- commercial.