
Abstract
Background
Anti-1-amino-3-[18F]fluorocyclobutane-1-carboxylic acid (anti-3-18F-FACBC) positron emission tomography/computed tomography (PET/CT), 11 C-choline PET/CT, 111In–capromab pendetide, and T2-weighted magnetic resonance imaging (MRI) have been used for detecting prostate carcinoma relapse.
Purpose
To systematically review and perform a meta-analysis of published data regarding the performance of 18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma.
Material and Methods
A comprehensive review of the literature regarding the role of 18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma was performed. Pooled sensitivity, specificity, and the area under the receiver-operating characteristic of 18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma were calculated based on the included studies.
Results
Six studies comprising 251 patients, suspicious of prostate carcinoma recurrence, were included in this meta-analysis. 18F-FACBC PET/CT had an 87% pooled sensitivity, 66% pooled specificity, 0.93 the area under the receiver-operating characteristic curve on a per patient-based analysis in detecting prostate carcinoma recurrence.
Conclusion
18F-FACBC PET/CT was a non-invasive, metabolic imaging technique in the diagnosis of prostate carcinoma relapse.
Keywords
Introduction
About 30% of patients develop local or distant recurrences within 10 years from initial radical prostatectomy or radiation therapy (1). Symptomatic disease relapse is virtually in the form of a biochemical relapse. Up to now, the diagnosis of biochemical relapse has been based on the PSA level only. However, a precise and definite cutoff point for PSA relapse does not exist (2). Nowadays, 11 C-choline PET/CT has been used in identifying the site of recurrence (3,4). The most obvious disadvantage of 11 C-choline PET/CT is its low sensitivity. Nanni et al. reported that the detection rate of 11 C-choline PET/CT was suboptimal due to the slow proliferation of prostate carcinoma cells (2). In recent years the synthetic L-leucine analog [anti-1-amino-3-[18F]fluorocyclobutane-1-carboxylic acid (anti-3-18F-FACBC)] has been proposed as a possible alternative radiopharmaceutical for detecting prostate carcinoma relapse (5–10). However, these studies have relative small sample size and limited power for any individual study. The purpose of this study was to systematically review and perform a meta-analysis of published data on the performance of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma.
Material and Methods
Search strategy
A comprehensive literature search of the Pubmed, Embase, and Scopus databases was conducted to find relevant published articles on the performance of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma. We used a search algorithm that was based on a combination of the terms: (i) “PET”; (ii) “carboxylic acid”; and (iii) “prostate”. No beginning date limitation was set. The final date of search was 31 October 2014. The language of all included literature was English. All references of the retrieved articles were scrutinized for additional papers to maximize the search result.
Study selection
The included papers were studies investigating the performance of anti-1-amino-3-[18F]fluorocyclobutane-1-carboxylic acid (anti-3-18F-FACBC) PET/CT in the application of prostate carcinoma recurrence. The inclusion criteria included: (i) the paper should be written in English; (ii) the tracer and equipment in these study should be anti-3-18F-FACBC) PET/CT; (iii) the paper should describe clearly the “gold standard”, the gold standard being histology and/or follow-up methods; (iv) adequate sample size necessary to calculate sensitivity. The exclusion criteria were: (i) insufficient data to reassess sensitivity or specificity from individual studies; (ii) editorials, letters, review articles, comments, author reply, erratum, conference proceedings; (iii) case reports or very small case series; (iv) articles that had used other devices, such as coincidence imaging scanner, only PET; (v) same patient data (including duplicate publication).
Data extraction
For every included study, data were collected including patient demographics, basic information (authors, publication date, country), technical information (scanner, tracer injection dosage, image interpretation), the number of true positive, true negative, false positive, false negative finding for anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma.
Quality assessment
Three independent reviewers (JY, LL, JG) evaluated the methodology of the included papers using the quality assessment tool for diagnostic accuracy studies (QUADAS) (11). Based on the quality assessment of Van den Bruel et al. studies were given an A, B, C, or D rating (12).
Statistical analysis
Sensitivity, specificity, and accuracy of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma were obtained from individual studies on a per-patient-based analysis. Pooled sensitivity, specificity of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma were based on the pooled number of true positive, false positive, false negative, and true negative. Pooled data are presented with 95% confidence intervals. An I-square statistical analysis was also performed to test for heterogeneity between studies (13). The statistical analysis of this meta-analysis referred to previous meta-analysis (14–17). Statistical analyses were performed using Meta-DiSc statistical software version 1.4 (Unit of Clinical Biostatistics, Ramon y Cajal Hospital, Madrid, Spain) (18).
Results
Literature search
The comprehensive computer literature search from the Pubmed, Embase, and Scopus databases showed 104 papers on initial analysis. After review, a total of six studies, comprising a total sample size of 251 patients, met all inclusion and exclusion criteria. All these patients were included into the present meta-analysis (Fig. 1).
Flow chart of the search for eligible studies on the diagnostic performance of 18 F-FACBC PET/CT in the diagnosis of prostate carcinoma: a meta-analysis.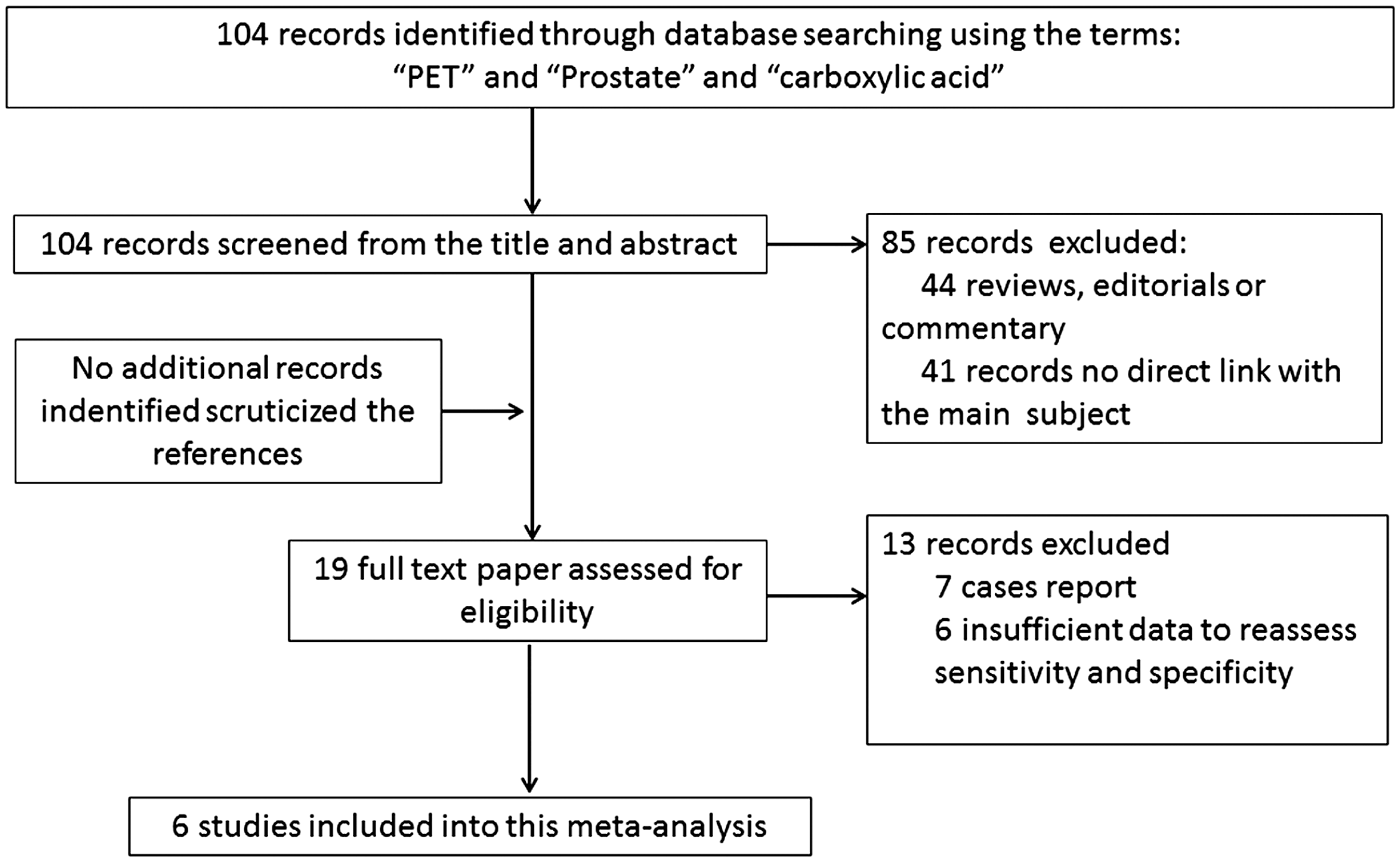
Quality assessment
Studies that scored in the range of 9–13 with a median score of 11. Two (33.3%) received A rating, two (33.3%) received B rating, two (33.3%) got a C rating, and no studies got a D rating. The gold standard of all these studies of this meta-analysis were histology and/or follow-up.
Diagnostic performance
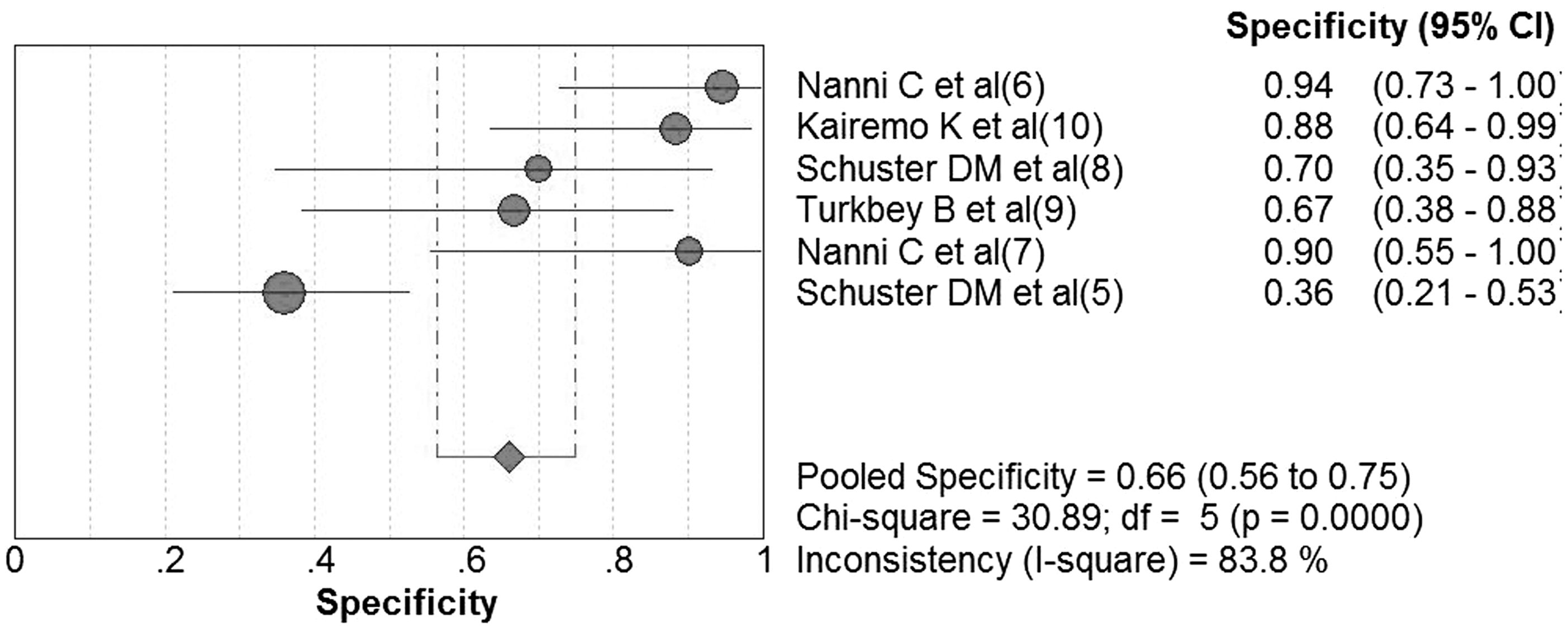
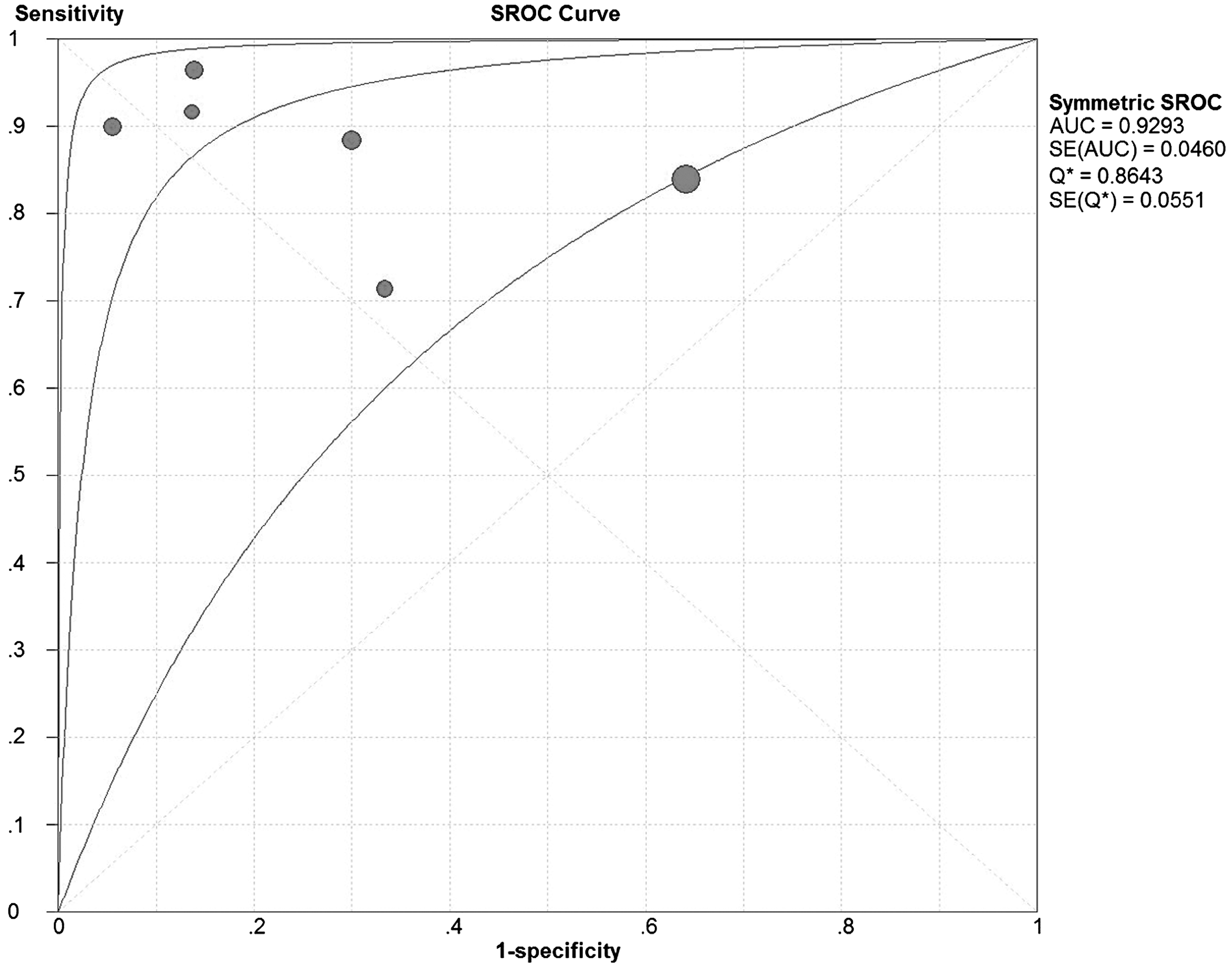
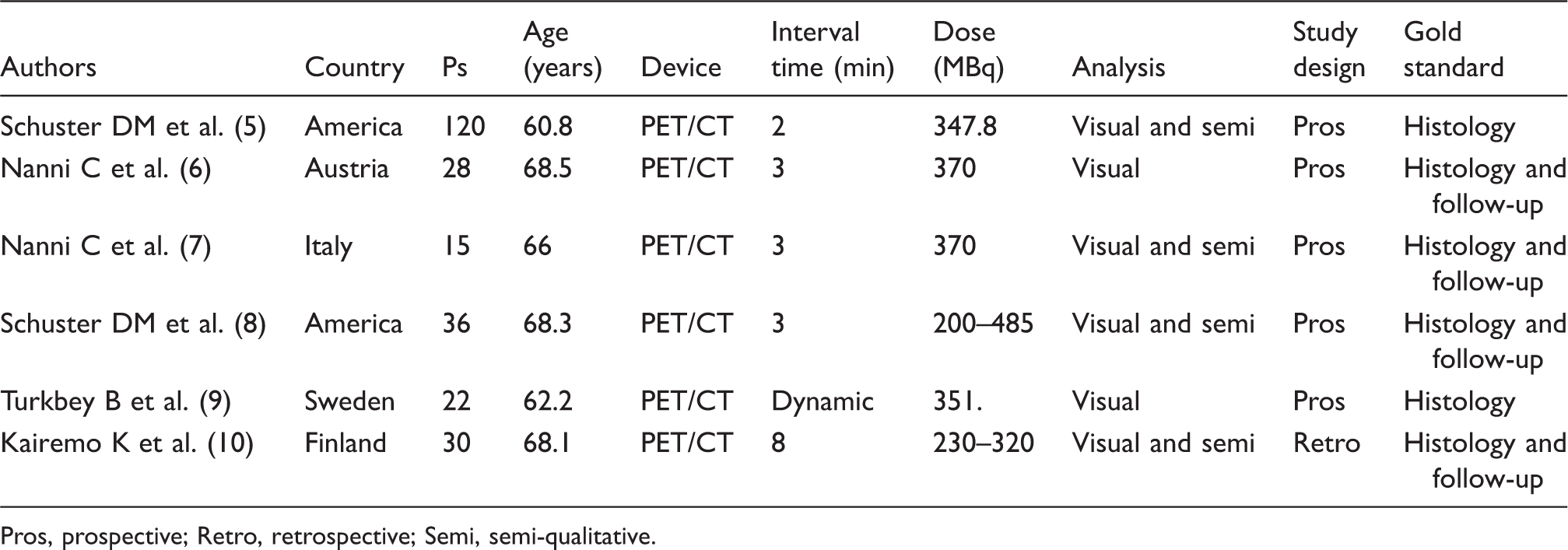
The performance of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma included studies presented in Figs. 2–4 and Table 1. The sensitivity of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma calculated on a per-patient-based analysis was 87% (95% confidence interval [CI] 80–92%). There was no statistically heterogeneity in the estimates of sensitivity on a per-patient-based analysis of included studies (I-square 27.9%) (Fig. 2). The pooled specificity of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma calculated on a per-patient-based analysis was 66% (95% CI 56–75%). The included studies were statistically heterogeneity in estimating specificity (I-square 83.8%) (Fig. 3). The area under the receiver-operating characteristic curve was 0.93 on a per-patient-based analysis (Fig. 4).
Plot of individual studies and pooled sensitivity of 18 F-FACBC PET/CT in the diagnosis of prostate carcinoma, including 95% confidence intervals. The size of circles indicates the weight of each study. The included studies were statistically heterogeneous in their estimates of sensitivity. Plot of individual studies and pooled specificity of 18 F-FACBC PET/CT in the diagnosis of prostate carcinoma, including 95% confidence intervals. The size of circles indicates the weight of each study. The included studies were statistically heterogeneous in their estimates of specificity. Summary receiver-operating characteristic curves of diagnostic accuracy of 18 F-FACBC PET/CT in the diagnosis of prostate carcinoma, including 95% confidence intervals. The area under the receiver-operating characteristic curve was 0.93, demonstrating that 18 F- FACBC PET/CT was an accurate method in the diagnosis of prostate carcinoma recurrence. Basic study, patient characteristics, and technical aspect of 18 F-FACBC PET/CT in these studies. Pros, prospective; Retro, retrospective; Semi, semi-qualitative. The diagnostic value of other methods in the diagnosis of prostate carcinoma recurrence. ND, non-description; NPV, negative predictive value; PPV, positive predictive value.

Discussion
Prostate carcinoma, accounting for about 33% of incidental cases of cancer in the male population of the United States, is the most common malignancy in the male population in Western Europe and North America (19). The most frequently applied first-line curative treatment method is radical prostatectomy. However, about 30% of patients develop local or distant recurrences within 10 years from initial radical prostatectomy or radiation therapy (1). Therefore, the accurate differentiation of local recurrence from distant metastasis is very important, which may influence further treatment protocol. Different imaging methods, such as computed tomography (CT), magnetic resonance imaging (MRI), bone scintigraphy, and ultrasonography, have been used in the restaging of prostate carcinoma. The diagnostic efficiency of these methods varies remarkably (20). Nowadays, 11 C- or 18F-choline PET/CT has been used in identifying site of recurrence (3,4). The diagnostic performance of 11 C- or 18F-choline PET/CT in recurrent prostate carcinoma are influenced by many factors, including PSA level, age, the various clinical stage, past biochemical failure, PSA kinetics, and androgen deprivation therapy (21). Totally, the most obvious disadvantage of 11 C-choline PET/CT is its low sensitivity. Nanni et al. reported that the detection rate of 11 C-choline PET/CT was suboptimal due to the slow proliferation of prostate carcinoma cells (2). Some metastatic lesions >10 mm may be negative by choline PET/CT scan.
In recent years, a synthetic L-leucine analog (anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid [FACBC]) has been used in the diagnosis of prostate carcinoma relapse (5–9). Based on this present meta-analysis, the sensitivity and specificity of anti-3-18F-FACBC PET/CT in the diagnosis of recurrent prostate carcinoma calculated on a per patient-based analysis was 87% (95% CI 80–92%) and 66% (95% CI 56–75%), respectively. The area under the receiver-operating characteristic curve was 0.93 on a per-patient-based analysis. It demonstrated that 18F-FACBC PET/CT is a valuable, non-invasive, metabolic imaging technique in the diagnosis of prostate carcinoma relapse.
18F-FACBC is an investigational synthetic non-metabolized amino acid analog PET tracer. The uptake of 18F-FACBC is related to the functional activity of two different amino-acid transporters, including alaninie serine cysteine transporter 2 and L-type amino acid transporter 1. The two transporters were upregulated in prostate carcinoma progression to metastatic disease (2). Shuster et al. reported that the intracellular levels of many amino acids increased compared with non-cancerous tissues (22). 18F-FACBC has been most actively investigated in patients with prostate, cerebral gliomas, breast, lung, and head and neck cancers (23). The advantages of 18F-FACBC include a favorable distribution of the 18F-FACBC in the body in evaluating prostate carcinoma, moderate heterogeneous marrow activity, mild muscle activity, moderate uptake in salivary, lymphoid, and pituitary tissue, mild to moderate activity in the bowel, less uptake in the kidney, very slow renal excretion, no activity in the urinary tract or in the bladder (2). Less distribution in the urinary system can reduce significantly the possibility of small sites of disease relapse missed due to the physiological presence of the tracer in the urinary tract (24). Lack of significant parenchymal uptake in the brain and relatively minimal renal excretion might be advantageous for cerebral and pelvic imaging. Intense liver and pancreatic uptake would limit disease detection in these organs. Another important advantage of anti-3-18F-FACBC is a longer half-life (109 min) and a shorter synthesis time, which makes anti-3-18F-FACBC PET imaging feasible without an onsite cyclotron (25).
Up to now, different imaging methods, such as CT, MRI, bone scintigraphy, and ultrasonography, have been used in the restaging of prostate carcinoma. Previous studies have compared the value of anti-3-18F-FACBC PET/CT (Table 2) in the diagnosis of prostate carcinoma recurrence with that of 11 C-choline PET/CT (6), 111In–capromab pendetide (8), T2-weighted (T2W) MRI (9). Nanni et al. compared the value of anti-3-18F-FACBC PET/CT with 11 C-choline PET/CT in the diagnosis of prostate carcinoma recurrence after radical prostatectomy. This study found that 11 C-choline PET/CT was positive in five patients and negative in 23 and anti-3-18F-FACBC PET/CT was positive in 10 patients and negative in 18 patients. This study also demonstrated that all positive lesions using 11 C-choline also were positive using anti-3-18F-FACBC PET/CT, but with the anti-3-18F-FACBC PET/CT, 11 additional tumors were identified including five additional patients (6). This study also reported that the target to background ratio of each lesion of anti-3-18F-FACBC was greater than 11 C-choline in 15 of 18 lesions, confirming a better image quality and contrast (6). These good results might be related with the favorable uptake mechanism of anti-3-18F-FACBC. 111In–capromab pendetide is a radiolabeled murine monoclonal antibody that binds to prostate-specific membrane antigen (26). The diagnostic performance of 111In–capromab pendetide varied widely, with a sensitivity of 17–92% and a specificity of 47–86%, which may be due to intra-observer variability, study population difference, and study design difference (8). Schuster et al. compared the diagnostic performance of anti-3-18F-FACBC with that of 111In-capromapendetide in the detection of recurrent prostate carcinoma. Fifty suspected recurrence of prostate carcinoma patients were included in the study and underwent anti-3-18F-FACBC PET/CT and 111In-capromab pendetide SPECT/CT. This study demonstrated that anti-3-18F-FACBC PET/CT had a sensitivity of 89%, specificity of 67%, and accuracy of 83%. 111In-capromab pendetide had a sensitivity of 69%, specificity of 58%, and accuracy of 67% for the disease detection in the prostate bed. In the detection of extraprostatic recurrence, anti-3-18F-FACBC had a sensitivity of 100%, specificity of 100%, and accuracy of 100%. 111In-capromab pendetide had a sensitivity of 10%, specificity of 100%, and accuracy of 47%. This study concluded that anti-3-18F-FACBC PET/CT was more sensitive than 111In-capromab pendetide SPECT/CT in the detection of recurrent prostate carcinoma and was highly accurate in the differentiation of prostatic from extraprostatic disease (8). Turkbey et al. evaluated the uptake of 18F-FACBC in patients with localized prostate cancer, benign prostatic hyperplasia, and normal prostate tissue and compared the value of 18F-FACBC PET/CT in the diagnosis of intraprostatic cancers with MRI. This study demonstrated that the sensitivity and specificity of 18F-FACBC PET/CT were 67% and 66%, respectively, 73% and 79% for T2W MRI, respectively. Mean prostate tumor SUVmax was significantly higher than that of the normal prostate; however, it was not a significant difference between prostate carcinoma and benign prostatic hyperplasia. This study concluded that combined 18F-FACBC PET/CT and T2W MRI enabled more accurate localization of prostate cancer lesions than 18F-FACBC PET/CT and T2W MRI alone (9).
Although the uptake of 18F-FACBC increase in different malignant tumors, the uptake of 18F-FACBC is not specific to malignant tumors. The amino acid scan was reported to be less prone to inflammatory uptake, but amino acid uptake also occurs in benign inflammation (23). Some common sources of false positive results of 18F-FACBC PET/CT, especially if focal, intense, and accompanied by an anatomic abnormality on CT, MRI or ultrasound, should be kept in mind, including osteoid osteoma (7), pituitary adenoma, meningioma, adrenal gland adenoma, prostatic hyperplasia, acute and chronic inflammation (23), benign glands and stroma, treatment-related changes, benign gland and stroma with fibromuscular tissue and a single lymphoid aggregate (8), inflammatory and reactive changes to external beam radiation therapy (10), mild to moderate in benign hilar, axillary and inguinal lymph nodes caused by acute and chronic inflammation and infection, inflammatory skin lesions, inguinal nodes due to ringworm infection, and musculoskeletal inflammation, degenerative facet disease. The false negative causes included: radical prostatectomy, and non-radical prostatectomy treatment (8). The included studies were statistically heterogeneous in their estimates of sensitivity, specificity and the area under the receiver-operating characteristic curve on a per-patient-based analysis. Many influencing factors may result in heterogeneity of these included studies. This heterogeneity was likely due to diversity in the methodological aspects between different studies. For example, five studies were prospective investigations (5–9), whereas only one study was retrospective in nature (10). The interval between injection and scanning, and different scan protocols may also contribute to the heterogeneity. Turkbey et al. reported that a rapid uptake of 18F-FACBC in the abnormal prostate (including prostate with tumors, lesions, or both), peaked at a mean of 3.6 min after injection. The difference between 18F-FACBC accumulation in a normal prostate and that in a prostate with a tumor, BPH, or both is essentially constant between 15 and 25 min. However, there was no difference between abnormal and normal prostate uptake by 60 min. This study suggested the best imaging time window was 15–20 min after injection (9). Schuster et al. also reported that highest combined diagnostic performance for anti-3-[18F] FACBC was acquired at 28 min. The sensitivity, specificity, and accuracy of 18F-FACBC at 28 min were 81.3%, 50.0%, 70.8%, respectively (5). Schuster et al. also reported that early imaging at less than 30 min was most useful for disease detection because of efflux of tracer from the tumor (23).
Finally, based on high sensitivity and moderate specificity, 18F-FACBC PET/CT may be considered as a good method in the diagnostic workup of prostate carcinoma relapse. The included studies were statistically heterogeneous in their estimates of specificity. This heterogeneity was likely due to diversity in the methodological aspects between different studies. For example, most studies were prospective investigations, whereas one study was retrospective in nature. Although the literature about the use of 18F-FACBC PET/CT in prostate carcinoma relapse remains limited, further large sample size, prospective, multicenter studies will be necessary to evaluate the diagnostic performance of 18F-FACBC PET/CT in prostate carcinoma relapse.
In conclusion, 18F-FACBC PET/CT is a non-invasive, metabolic imaging technique in the diagnosis of prostate carcinoma relapse. The possible influencing diagnostic factors of 18F-FACBC PET/CT in the diagnosis of prostate carcinoma relapse should be kept in mind.
Footnotes
Conflict of interest
None declared.
Funding
Jigang Yang was partially supported by the Beijing Natural Science Foundation (no. 7152041), and by the Beijing Health Technical Personnel Training Plan (no. 2013-3-066).