
Abstract
Background
Thyroid metastases (TM) are uncommon. Dependent on study design, the reported frequency of TM is in the range of 0.1–6% in different analyses. While clinical and histopathological features of TM were well described in the literature, radiological publications consist predominantly of isolated case reports or small series.
Purpose
To estimate the prevalence, clinical signs, and radiological appearances of TM.
Material and Methods
From 1997 to 2013, a total of 8849 patients with various disorders of the thyroid gland were treated in our institution. In 33 patients TM were diagnosed. Ultrasound (US) images were available in all patients, computed tomography (CT) of the neck in 16 patients, and magnetic resonance imaging (MRI) in nine patients.
Results
Clinically, most patients (85%) presented with a painless neck mass. Primary tumors were renal cell carcinoma (79%), colorectal cancer (12%), lung cancer (3%), rhabdomyosarcoma (3%), and breast carcinoma (3%). On US, most lesions were irregular in shape with inhomogenous texture. On CT, all TM were hypodense. On T1-weighted images, most TM were inhomogenously iso-to-hyperintense in comparison to the normal thyroid tissue, and slightly hyperintense on T2-weighted images with an inhomogenous contrast enhancement.
Conclusion
The prevalence of TM was 0.4%. Most of the TM originated from renal cell carcinoma. The identified radiological features of TM should be taken into consideration in the differential diagnosis of thyroid lesions.
Keywords
Introduction
Although the thyroid gland has a rich vasculature, thyroid metastases (TM) are uncommon (1–5). Dependent on study design, the reported frequency of TM was in the range of 0.1–6% in different analyses (1–6).
While clinical and histopathological features of TM have been well described in the literature, radiological publications consist predominantly of isolatmall series (1–6). Furthermore, the reported imaging features of TM comprised predominantly sonographic findings (7–10), and controversial data have been described (7–10).
Therefore, the purpose of this study was to estimate the prevalence and clinical signs of TM and to describe their radiological appearance.
Material and Methods
Patients
In 1997–2013, 8849 patients with various disorders of the thyroid gland were treated in the department of surgery of the Martin Luther University of Halle-Wittenberg. For this time period, 33 patients with TM were identified retrospectively in the databases of the department of surgery (search for key words in the reports). There were 18 women and 15 men with a median age of 69 years (age range, 8–82 years; mean age 65.2 ± 12.9 years).
Images
Ultrasound (US) images were available in all 33 patients. US was performed using an 8 MHz linear array transducer connected to a Toshiba TA 312 scanner (TOSHIBA Medical Systems GmbH, Neuss, Germany).
Computed tomography (CT) of the neck was available in 16 patients. Several CT scanner were used. In most cases (n = 11) CT was performed on a Somatom Sensation 64 (Siemens, Erlangen, Germany) of the neck or neck and thorax. In all cases 1.5 mL of iodinated intravenous contrast medium (Solutrast, Bracco Altana GmbH, Konstanz, Germany) per body mass was given at a rate of 1.5–3.5 mL/s by a power injector, with a scan delay of 60 s after onset of injection. Typical imaging parameters were 120 kVp, 150–300 mAs, and 0.6 slice thickness with a pitch of 0.8.
In nine patients, magnetic resonance imaging (MRI) of the neck was performed additionally using a head and neck coil on a 1.5 T scanner (Magnetom Vision, Siemens). The protocol included an axial T2-weighted (T2W) fast spin echo sequence and an axial T1-weighted (T1W) spin echo (SE) sequence. In all patients axial T1W SE and/or T1W SE fat-suppressed sequences were performed after intravenous administration of a paramagnetic contrast medium with a dose of 0.1 mg/kg. The slice thickness was in the range of 3–5 mm.
All available images were interpreted by one radiologist (AS, with 11 years of experience).
Lesion size was determined by measuring the maximum diameter.
Case histories were reviewed retrospectively to determine the clinical signs at the time of presentation.
Histological findings
In all patients the diagnosis of TM was confirmed histopathologically. Histological specimens were evaluated by one pathologist (HJH, with 40 years of experience). All available histological materials (sections stained by hematoxylin/eosin or by immunohistochemistry) were analyzed.
Statistical analysis
For statistical analysis the SPSS statistical software package was used (SPSS 17.0, SPSS Inc., Chicago, IL, USA). Collected data were evaluated by means of descriptive statistics (absolute and relative frequencies).
Results
Frequency, primary tumors, localization, and clinical signs of TM
Metastases to the thyroid were identified in 0.4% of all surgical interventions on the thyroid gland.
Clinical characteristics of the cases with identified thyroid metastases (TM).
RCC, renal cell carcinoma.
In most patients metastases originated from renal cell carcinomas (n = 26, 79%). Other primary tumors were colorectal cancer (4 patients, 12%), lung cancer (1 patient, 3%), rhabdomyosarcoma (1 patient, 3%), and breast carcinoma (1 patient, 3%).
The number of TM was in the range of 1–3 per patient. Overall, 39 metastatic lesions were identified. They were localized in the right lobe in 17 patients (52%), in the left lobe in 12 (36%), and in four patients (12%) TM were bilateral. The mean size of the metastases as measured in US was 36.9 ± 16.9 mm (median size, 32.5 mm; range, 10–80 mm) in anterior–posterior and 30.9 ± 13.9 mm (median size, 30.0 mm; range, 10–65 mm) in left–right direction.
In most patients (n = 28, 85%), the TM were diagnosed after the diagnosis of the primary tumor (Table 1). The latency was in the range of 2–18 years (mean age, 9.5 ± 4.5 years; median age, 9 years). For the remaining five cases, TM were detected before the primary tumors in four patients (12%), and in one patient (3%) metastatic invasion of the thyroid was identified simultaneously with the primary malignancy.
Furthermore, at the time of the diagnosis, TM were the only manifestation of metastatic disease in 25 cases (76%). Systemic metastases outside the thyroid were diagnosed in eight patients (24%). Of the eight patients, other metastases were identified simultaneously with TM in seven cases. In these patients, primary thyroid cancer was suspected. In one case, TM infiltrating the trachea occurred in patient with multiple systemic metastases.
Radiological features of TM
Ultrasound: Ultrasound images were available for 33 patients (39 TM). On ultrasound, 30 lesions (77%) were irregular in shape and nine lesions (23%) were oval. The identified metastases were homogenously markedly hypoechoic in relation to strap muscle in two cases (5%) and hypoechoic in 37 cases (95%) (Fig. 1). Most TM (n = 25, 64%) showed indistinct margins, 13 lobulated (33%), and one lesion (3%) had circumscribed margins. Thirty lesions (77%) were irregular in shape, and nine (23%) were oval.
Thyroid metastasis from renal cell carcinoma. (a) CT without contrast medium showing a large hypodense lesion (arrow) in the right thyroid lobe. (b) On MRI, the lesion (arrow) is hypointense on the T1W image. (c) On the T2W image, the lesion (arrow) is slightly hyperintense. (d) After intravenous administration of contrast medium, the lesion (arrow) shows a slight inhomogeneous enhancement and areas of necrosis. The images show invasion of the cricoidal ring with a component protruding in the subglottic region. (e) Histological examination reveals metastasis of renal cell carcinoma (hematoxylin & eosin stain, ×25).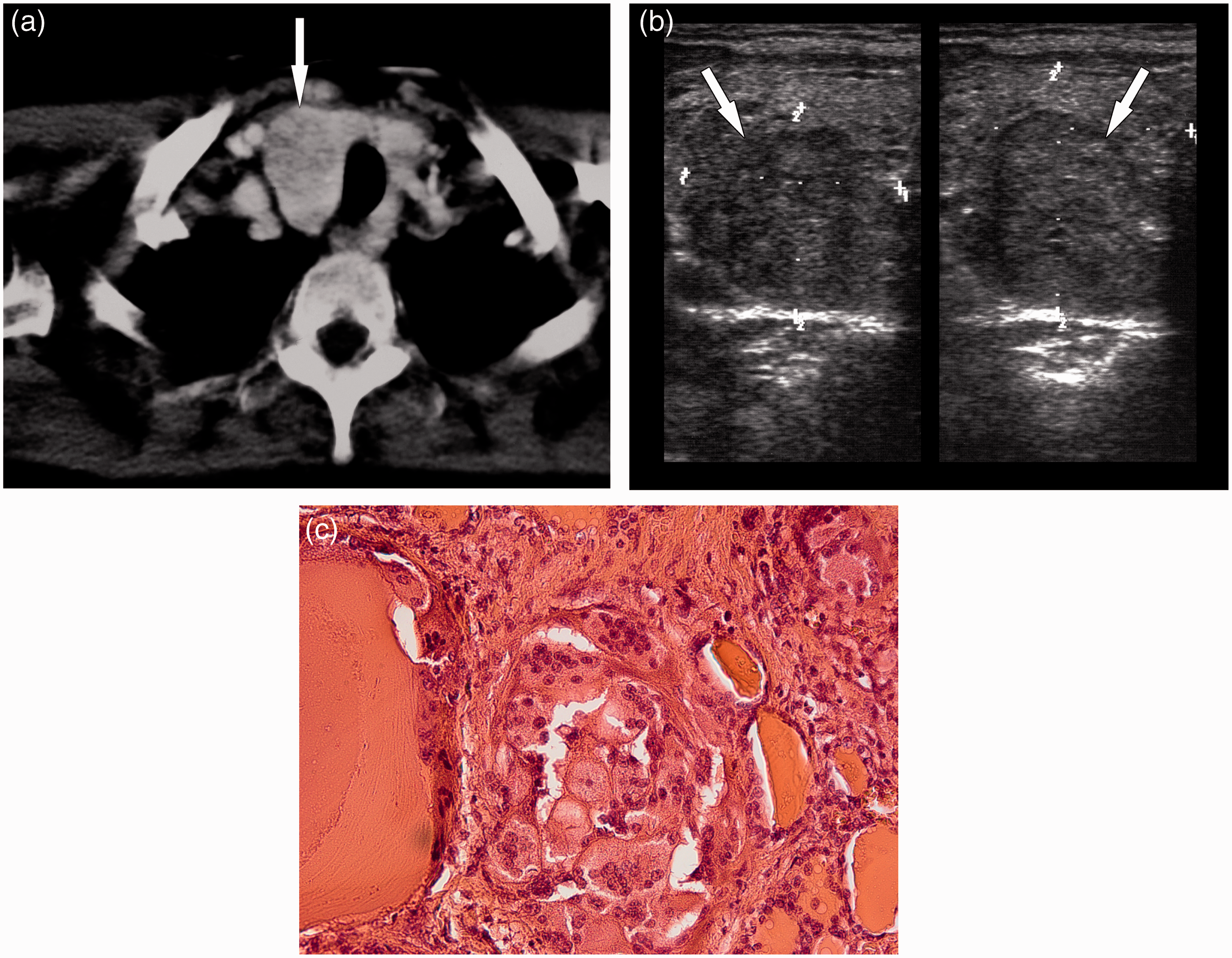
CT: CT was available for 16 patients (21 lesions). All TM were hypodense in comparison to the thyroid and showed an inhomogeneous enhancement (Figs 1 and 2).
Thyroid metastasis from breast cancer. (a) Contrast-enhanced CT shows a large inhomogenous hypodense lesion with enhancement and indistinct margins (arrow) in the right lobe. (b) On ultrasound, the lesion (arrows) is hypoechoic with microlobulated margins. (c) Histological examination shows metastasis of the known breast cancer (hematoxylin & eosin stain, ×25).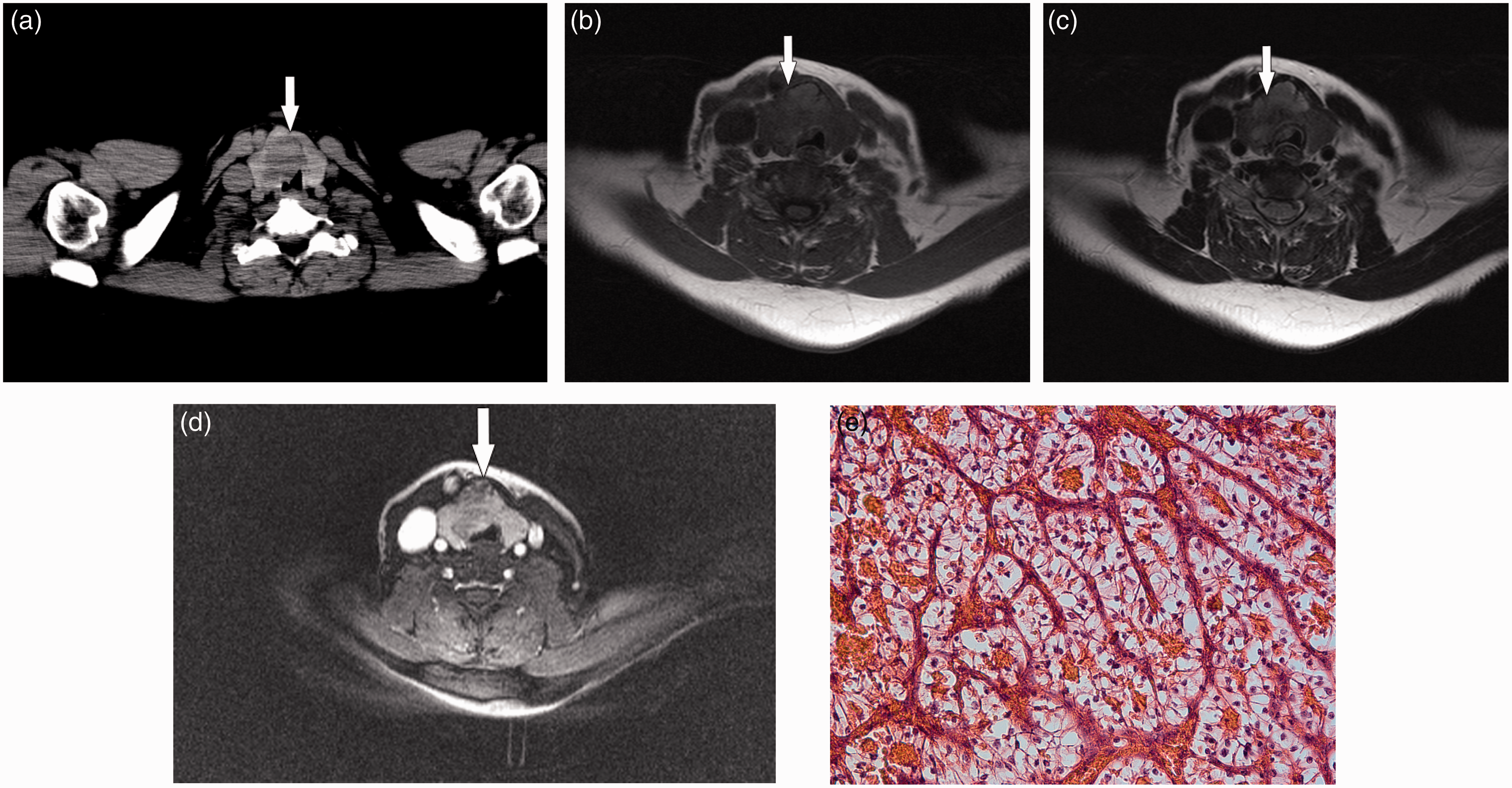
MRI: MR images were available for nine patients (11 lesions). On T1W images, most TM (n = 8, 73%) were inhomogenously iso-to-hyperintense in comparison to the normal thyroid tissue, and three lesions (27%) were hypo-to-isointense. On T2W images, nine metastases (82%) were slightly hyperintense and two TM (18%) were markedly hyperintense. After intravenous administration of contrast medium all metastases demonstrated an inhomogeneous light contrast enhancement. Central necrosis was seen in eight TM (73%) (Fig. 2).
Treatment and outcome
All patients underwent fine-needle biopsy of the thyroid lesions. Intrathyroidal metastases were diagnosed in 26 cases (79%). In seven patients (21%), anaplastic thyroid cancer was suspected. There were patients, in whom systemic metastases outside the thyroid were diagnosed simultaneously with TM. In all cases the identified TM were resected surgically. In 20 patients (61%) total thyroidectomy, in six cases (18%) subtotal thyroidectomy, and in seven patients (21%) hemithyroidectomy was performed. The postoperative course was uneventful in all patients within 1 year. The late follow-up was unknown.
Discussion
Metastases to the thyroid have been reported previously as a rare condition (1–5). Their frequency was in the range of 1.2–6% of all malignancies of the thyroid (2,3,11). Furthermore, it was in the range of 0.07–1.7% from all surgical interventions of the thyroid (1,11–13). The frequency of TM in the present study was in the range reported previously.
According to the literature, most frequently kidney tumors, especially renal cell carcinomas, metastasize to the thyroid (4,5,10,12,14). In a literature review TM from renal carcinomas were diagnosed in 48% of the cases (4). In a retrospective series the Mayo clinic identified 43 cases with TM, 33% of the metastases originated from kidney tumors, 16% from lung cancer, and 16% from breast carcinoma (5). TM from other malignancies occurred with less frequency, in the range of 2–9% (5). However, in a series by Saito et al., including 29 patients from Japan, 34% of the TM derived from breast cancer followed by lung cancer (21%), whereas TM from kidney tumors were identified in 9% only (7). Furthermore, in a Chinese population TM derived in 53% from lung cancer (6). In an Italian study of 36 cases, the contribution of different primary tumors to thyroid metastases was in the range of 1–5% (11). This discrepancy in the literature data may reflect variation in selection of patients as well as geographical differences in tumor frequency. In our series, most of the TM (79%) originated from renal cell carcinomas. Other primary malignancies were rare.
According to some reports, TM occurred most frequently in female patients, the female:male ratio in the range of 1.4:1 to 2.7:1 (4,15,16). Other authors, however, found no gender predominance in TM (5,6,11,13).
Interestingly, according to the literature, TM occur often with a significant latency after the diagnosis of primary tumors (4,17). For example, Chung et al. reported that TM occurred metachronously in 70% of the cases with a mean delay of 5.8 years after the diagnosis of the primary tumors (4). In addition, previous reports have shown that the mean time interval between to detection of TM was longer in renal cell carcinomas (9.4 years), followed by metastases from breast cancer (6.9 years), and esophageal cancer (2.3 years) (17). Our study confirmed these findings.
According to the literature, most patients had additional non-thyroidal metastases (1–6). For instance, in the study of Hegerova et al., the rate of other metastases was 79% (17). However, in a large review of Chung et al., 40.3% of the patients had isolated TM (4). In agreement with this review, 76% of TM of our series were solitary metastases.
As reported previously, TM had no specific clinical signs and they mimic those of benign thyroid masses or thyroid cancer (1–6,14,17). For example, in the present study, 85% of TM presented with a painless neck mass. However, 15% of TM were clinically silent and were detected during staging examination. This fact suggests that the thyroid should be evaluated carefully on staging or follow-up CT in patients with non-thyroid malignancies.
Radiological features of TM have been described previously in a few reports (7–10). Most frequently, ultrasound findings were reported (7–10). Except for isolated case reports, the number of the reported metastases was in the range of 7–27 (7–10). Two sonographic patterns of TM have been described previously (7–10). First, diffuse hypoechoic enlargement of the thyroid, and second, isolated masses within the thyroid (7). According to the literature, most TM manifested as hypoechoic ill-defined lesions (7,8). In the series by Takashima et al., however, the identified metastases showed well defined margins and were markedly hypoechoic (9). Ahuja et al. found similar results (8). According to Chung et al., however, TM had heterogenous echogenic texture (10). In our study, TM manifested as inhomogeneous hypoechoic or markedly hypoechoic thyroid masses with indistinct margins. The difference between sonographic characteristics of TM in several reports may be related to the fact that the described metastases originated from different primary tumors. In fact, in the study of Saito et al. reporting ultrasound findings of 27 TM, most metastases derived from breast carcinoma (37%), several gastrointestinal tumors (33%), and from lung cancer (15%) (7). Chung et al. analyzed sonographic findings of nine TM, with six of these cases being metastases from breast cancer (10). In the present study, radiological features of TM represent mostly metastases from renal cell carcinoma.
According to the literature, the identified sonographic features of TM were suspicious for malignancy and indicated further investigation (18,19). As reported previously, malignant sonographic characteristics of thyroid lesions were defined as microcalcifications, an irregular or microlobulated margin, and marked hypoechogenicity (18,19). The knowledge of these criteria is especially important in cases with isolated metastatic invasion of the thyroid without other metastases.
CT features of TM were reported in isolated cases only (10,14). Our analysis showed that most identified metastases were hypodense in comparison to the thyroid and showed an inhomogenous enhancement.
MRI findings of TM have been reported in one series only (9). In this report, four TM were analyzed (9). Three of the identified lesions were isointense on T1W images and one lesion was hypointense (9). On T2W images, two TM were hyperintense and two other metastases were hypointense (9).
In our series, 11 lesions were analyzed on MRI. On T1W images, most TM were inhomogeneously iso-to-hyperintense in comparison to the normal thyroid tissue and on T2W images most lesions were slightly hyperintense. All metastases demonstrated an inhomogenous light contrast enhancement.
In 3% of our TM infiltration of the adjacent organs was identified. The fact that TM can also affect the trachea, larynx, or other organs should be known for radiologists.
According to the literature, diffusion-weighted imaging can be helpful to distinguish malignant and benign thyroid lesions (20,21). For instance, Shi et al. found that an ADC value of 1.70 × 10–3 mm2s–1 can be threshold differentiating malignant from benign nodules, with 92% sensitivity, 88% specificity, and 87% accuracy (20). In the study of Schueller-Weidekamm et al., an ADC value of 2.25 × 10–3 mm2s–1 was proven to be the cutoff value for differentiating between benign and malignant thyroid nodules, with an accuracy of 88%, a sensitivity of 85%, and a specificity of 100% (21). Our patients were not investigated by DWI.
According to the literature, the diagnosis of TM could be established by fine-needle biopsy (4,11,17). However, as mentioned previously, cytological examination in cases with TM can be a dilemma for the cytopathologist (4,11–13). Cytopathological findings in TM may masquerade as primary thyroid tumor, especially as anaplastic carcinoma (11–13). Furthermore, additional immunohistochemical staining, for example against thyroglobulin or calcitonin, has been reported to be often difficult to distinguish between TM and primary poorly differentiated thyroid carcinoma (11–13,17). In the present analysis, fine-needle biopsy provided the correct diagnosis in 79% of the cases. In 21%, however, the diagnosis of anaplastic thyroid cancer was made cytopathologically. Our data were in agreement with those of Chung et al., who reported the correct diagnosis of TM at fine-needle biopsy in 73.7% of all cases (4).
There is no general recommendation regarding treatment of TM. Isolated TM can be resected curatively (5,22). Some authors suggested a lobectomy in cases of solitary TM and a total thyroidectomy in patients with bilateral lesions (5,22–25).
Our study had several limitations. First, it is retrospective. Second, not every patient underwent all investigations (ultrasound, CT, and MRI).
In conclusion, in the present study, 0.4% of all interventions on the thyroid revealed TM. Most of the TM originated from renal cell carcinomas. Seventy-six percent of the TM were solitary metastases. Furthermore, in 85% of the cases, TM were metachronous metastases. On ultrasound, TM manifested as inhomogeneous hypo-to-isoechoic thyroid masses with indistinct margins. On CT, most identified metastases were hypodense in comparison to the thyroid. On MRI, on T1W images, most TM were inhomogeneously iso-to-hyperintense and on T2W images most lesions were slightly hyperintense in comparison to the normal thyroid tissue. These findings should be taken into consideration in the differential diagnosis of thyroid lesions.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.