
Abstract
Background
Cancer-related obstruction of large abdominal and pelvic veins might become symptomatic with clinical signs of lower limb venous congestion. Technical and clinical outcome after interventional treatment is not well studied yet.
Purpose
To retrospectively assess the technical and clinical outcome of endovascular management of symptomatic cancer-related iliocaval venous obstructive disease.
Material and Methods
From 1998 to 2013, 19 patients (15 men, 4 women; mean age, 63.6 years) referred for interventional treatment of cancer-related iliocaval obstructive disease were identified. Patients’ symptoms included unilateral (n = 16; 84%) or bilateral (n = 3; 16%) painful swelling of the lower limbs. Patients’ demographics as well as interventional and clinical outcome data were collected.
Results
All 19 patients underwent, under local anesthesia, stenting of the iliac vein (n = 16; 84%) or inferior vena cava (n = 3; 16%). Immediate technical success (n = 19) was 100%; immediate clinical success (n = 18) was 94.7%. During follow-up, seven patients (36.8%) presented with recurrent symptoms of painful limb swelling. Estimated survival after 3 and 6 months was 68.4% (95% confidence interval [CI], 47.8–82.3%) and 19.8% (95% CI, 11.9–29.2%), respectively.
Conclusion
Endovascular stenting of cancer-related iliocaval venous obstructive disease is safe and results in immediate relief of symptoms. However, recurrent venous obstruction is common. At 3 months follow-up, the majority of patients with iliac vein stenting were still alive.
Introduction
Symptomatic obstruction related to malignant involvement of large veins may occur both in the central thoracic veins (1) and in the pelvic and abdominal region (2–4). Malignant iliac vein and inferior vena cava obstruction may result in debilitating symptoms of painful leg swelling, sometimes associated with penile, scrotal, and preputial edema or anterior abdominal wall collaterals (5,6). However, published data on the diagnosis and interventional treatment of symptomatic iliocaval cancer-related obstruction are scarce and mainly consist of case reports and small case series (3,4,7–11), or deal with a mixed patient population presenting with malignant or benign venous obstructive disease (2,6). In addition, these few brief reports focus on the interventional technique to manage these venous compressions and its immediate clinical outcome, but data on overall survival and analysis of recurrent venous obstruction are frequently lacking. In this retrospective analysis, data were collected on patients presenting with cancer-related iliocaval venous obstruction treated with percutaneous, interventional radiological techniques. Finally, overall survival, recurrent venous obstruction and factors potentially influencing outcome were analyzed.
Material and Methods
Study design
This is a retrospective study including patients referred to the department of interventional radiology of a tertiary care university hospital from January 2000 to January 2013. Approval for the study was obtained from the institutional ethics committee (S 56056) and informed consent was obtained from all patients prior to the interventional procedure.
Technique of venous stenting
All endovascular procedures were performed under local anesthesia. Depending on the involved vein, the right or left common femoral vein or ipsilateral popliteal vein was punctured and an 8 or 10 French (F) sheath was introduced. The venous access was always achieved under ultrasound guidance. After intravenous administration of 5000 international units (IU) of unfractioned heparin, non-ionic iodized contrast medium iopromide (Ultravist-240, Bayer-Schering Health Care, Diegem, Belgium) was injected through the sheath in order to identify the venous obstruction. In the event of renal insufficiency or allergy to iodized contrast medium, carbon dioxide injected through a hand injection system (CO2-set, Optimed, Ettlingen, Germany) was used. Recanalization of the obstruction was typically performed with the use of a 0.035 inch hydrophilic guide wire (Glidewire, Terumo Europe, Leuven, Belgium) and a 4 or 5 F diagnostic catheter. If concomitant iliofemoral deep venous thrombosis was detected, catheter-directed thrombolysis using Urokinase (Actosolv, Eumedica, Brussels, Belgium) was performed. The infusion schema included an upload dose of 960,000 international units (IU) over 4 h followed by a continuous infusion of 120,000 IU per hour. Daily venographic controls are performed until less than 5% of residual thrombus is seen on venography. All malignant obstructive lesions were primarily stented with the use of self-expanding stents (Easy Wallstent, Boston Scientific, Natick, MA, USA; Zilver stent, Cook Medical, Bjaeverskov, Denmark; Memotherm, BARD-Angiomed, Karlsruhe, Germany). The diameter of the self-expanding stents was oversized with 1–2 mm to the vein diameter below and above the underlying stenosis. Postdilatation of the stents was performed with conventional angioplasty balloon catheters with the same diameter as the vein below and above the underlying stenosis to avoid overdilatation and venous rupture. In the event of significant stent recoil after repeated postdilation, an additional balloon-expandable stent (Scuba, Invatec-Medtronic, Roncadelle, Italy) was inserted within the self-expanding stent. After completion venography of the stented segment, the vascular sheath was removed and manual compression of the puncture site performed. Therapeutic low molecular weight heparin (LMWH) was administered subcutaneously for the first 24 h after stenting. Afterwards, therapeutic LMWH was prescribed for 1 month. Continued therapeutic LMWH administration was based on the patient’s comorbidities, the general status and the risk for paraneoplastic venous thrombosis.
Follow-up
All patients were followed up clinically by the referring oncologist and general practitioner until March 2013 or the patient’s death. Assessment of the clinical outcome and survival was performed based on the electronic medical records and telephone calls to the general practitioner. Radiological follow-up was available if the underlying malignant disease was re-evaluated by imaging.
Statistical analysis
Kaplan-Meier estimates were used to construct survival curves. All analyses were performed using SAS software, version 9.2 of the SAS System for Windows (SAS Institute Inc., Cary, NC, USA).
Results
Study population
Patient demographics.

Radiological examinations prior to interventional treatment included duplex-ultrasound (n = 9), computed tomography (CT) (n = 18), and magnetic resonance imaging (MRI) (n = 1) showing a mass lesion compressing or invading the inferior vena cava (n = 3) or iliac vein (n = 16). In two patients, catheter-directed thrombolysis of the acute iliofemoral deep venous thrombosis, localized over the whole iliac axis, was performed prior to the stent procedure. Total dose of Urokinase infused was 900,000 IU and 1,200,000 IU, respectively. Finally, insertion of self-expanding stents was performed to treat the underlying venous obstruction.
Technical outcome
All procedures were performed under local anesthesia. In 18 out of 19 patients, the common femoral vein was punctured and in the remaining patient, the ipsilateral popliteal vein was punctured because of extensive tumor invasion of the external iliac vein and the proximal part of the common femoral vein. In three patients, a contralateral approach was performed, in 12 patients the ipsilateral common femoral vein was punctured and in the three patients with inferior vena cava obstruction, the right common femoral vein was selected.
Venography was performed in two patients (11%) with the use of carbon dioxide (CO2) because of renal impairment; in the remaining 17 patients (89%), iodized contrast medium was used. Venography revealed a complete occlusion of the involved vein in two patients (11%) (Fig. 1); in 17 patients a severe stenosis > 90% was observed (Fig. 2). Guide wire recanalization and stent placement was successful in all cases. In six patients, an Easy Wallstent with a nominal diameter of 14 or 16 mm was inserted; in nine patients, a Zilver stent with a nominal diameter of 12 or 14 mm was inserted; in the remaining patient with an inferior vena cava occlusion, a Memotherm with a nominal diameter of 20 mm was placed.
A 78-year-old woman presented with a painful and swollen left lower limb; (a) axial and (b) reconstructed coronal contrast-enhanced CT images revealed a hypodense mass lesion (arrows). The mass lesion was a necrotic lymph node of a urethral transitional cell carcinoma and invaded the left external iliac vein; (c) corresponding venography confirmed the malignant occlusion of the external iliac vein; (d) recanalization and stenting of the occluded segment resulted in restored iliac venous patency. A 55-year-old man with a history of metastatic prostate carcinoma presented with a painful left swollen lower limb; (a) CT scan demonstrated a hypodense mass lesion in close proximity to the left iliac vein; (b) corresponding left iliac venography showed a focal high-grade stenosis owing to malignant invasion of the malignant lymph nodes; (c) after stent placement, a restored patency of the left venous iliac axis was demonstrated.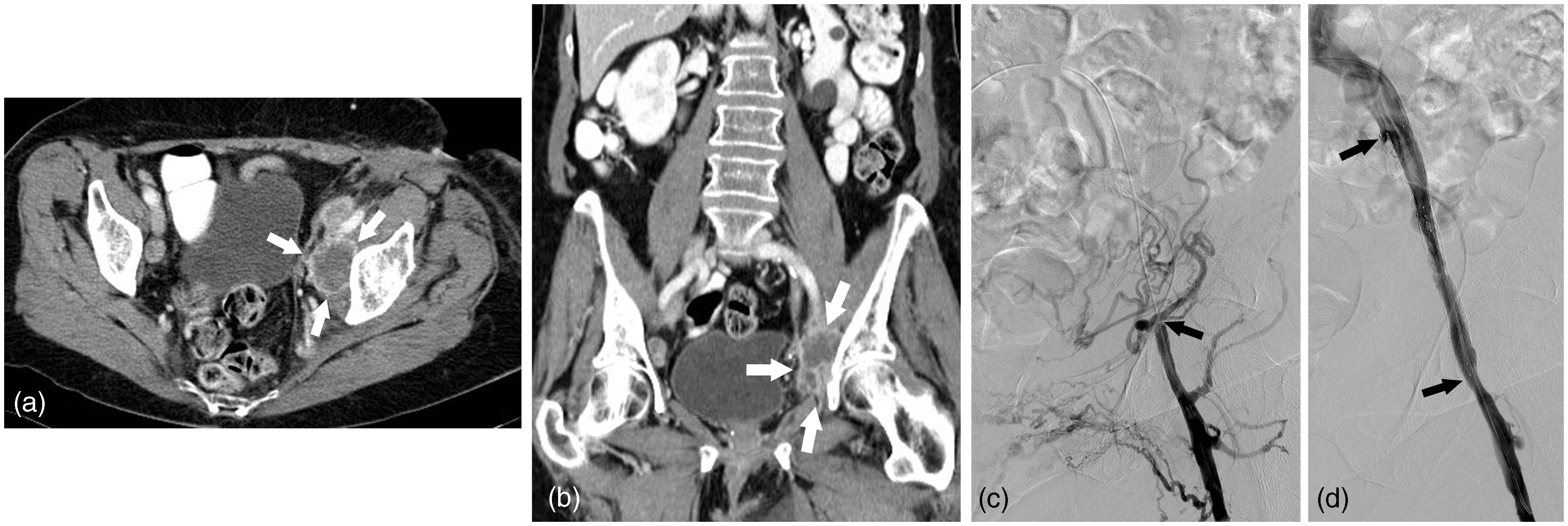

In one patient, a balloon-expandable Scuba stent, 4 cm in length and 10 mm in diameter was placed within the Zilver stent for complete re-expansion of the stented iliac vein segment. Completion venography showed re-expansion of all stented segments with a <30% residual stenosis. No peri- or immediate postprocedural complications were noted.
Clinical outcome
Initial clinical symptoms of painful leg swelling disappeared in 18 patients (95%) within the first 3 days after the stent procedure. One patient with an initial obstruction of the inferior vena cava did not respond clinically to the technically successful endovascular stent placement, with major residual bilateral lower limb swelling.
Late complications of stent re-occlusion.
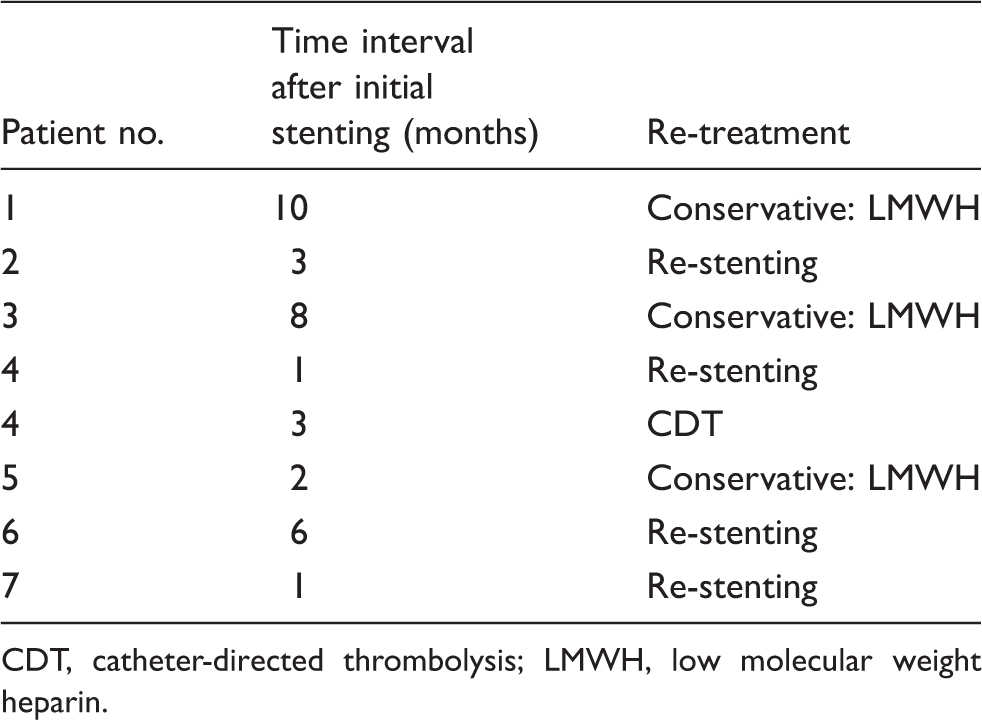
CDT, catheter-directed thrombolysis; LMWH, low molecular weight heparin.
Estimated survival percentages (+95% CI).

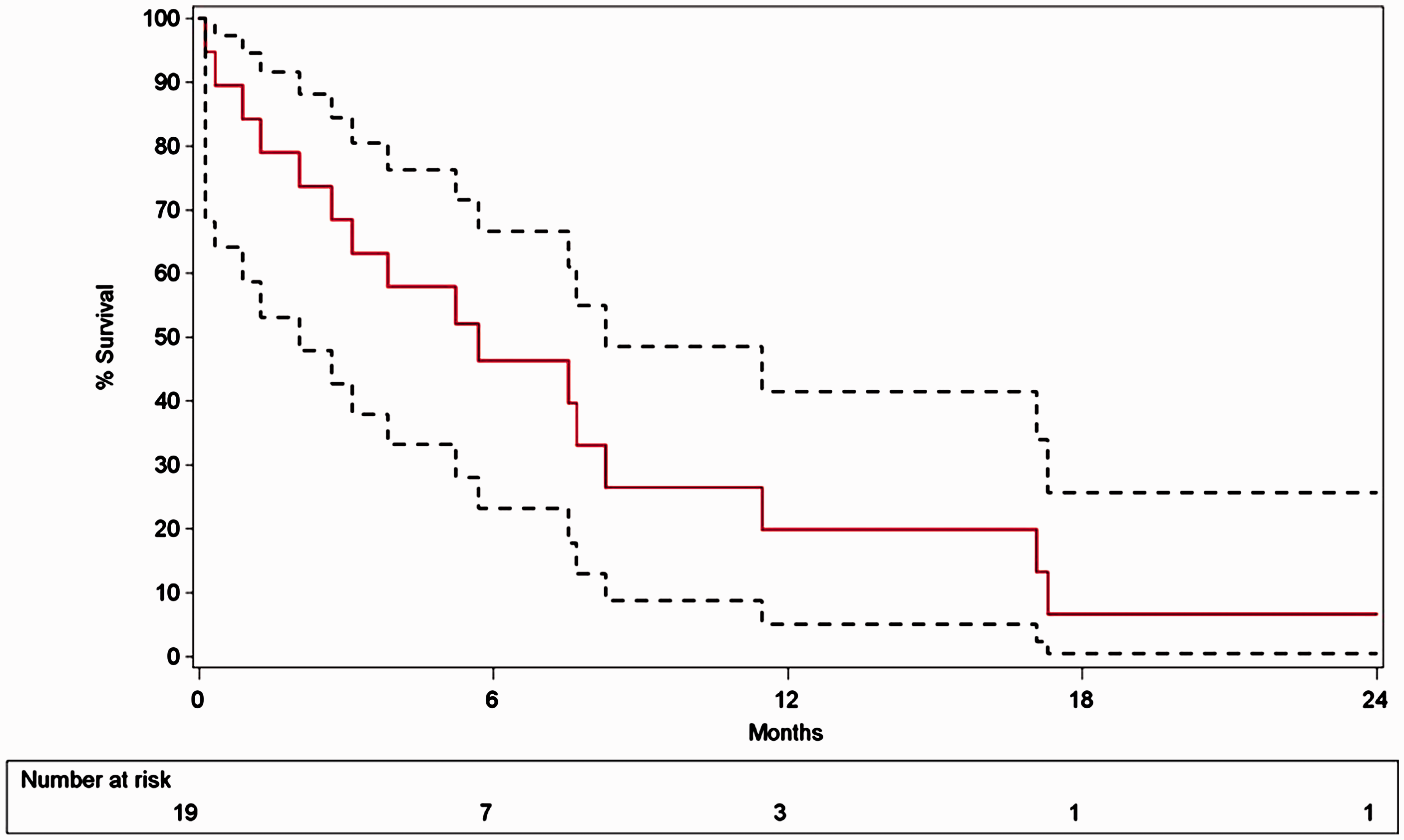
The Kaplan-Meier overall survival curve demonstrates an estimated survival percentage (95% CI) of 68.4% (47.8–82.3%) and 19.8% (11.9–29.2%) at 3 and 12 months follow-up, respectively.
Discussion
This study shows that percutaneous stent insertion for the palliative treatment of patients with symptomatic cancer-related venous iliocaval obstructive disease is safe and effective, with a very high rate of immediate, symptomatic relief. The use of stents instead of balloon angioplasty alone is strictly required to avoid immediate recoil of the vein wall by the compressing tumoral mass lesion. These results are in line with published data showing immediate symptom relief in 80–100% of cases (2–4,7,8). In this series, no peri- or immediate postprocedural complications, in particular stent fracture or stent migration, were noted. Nazarian et al. (2) reported two out of 56 cases of stent fracture and four cases of stent slippage in patients presenting with both malignant and benign iliofemoral venous obstructions. They all occurred in patients treated with Gianturco-Rösch-Z-stents. These authors (2) as well as others (3,6), did not report similar complications when using Wallstents or nitinol-based self-expanding stents, and these findings are confirmed by this study. One out of nine patients treated with a Cook Zilver nitinol stent for a malignant external left iliac vein stenosis required an additional balloon-expandable stent to completely open the self-expanding nitinol stent. The need for an additional stent with a high radial force was also found in 22% of patients treated for cancer-related superior vena cava syndrome (1).
In this series, the majority of patients presenting with malignant iliac vein occlusion suffered from widespread metastatic urogenital cancers (n = 10; 62.5%). In a minority of patients, lymph node metastasis from other cancers, including rectal carcinoma and breast carcinoma, was responsible for the malignant venous involvement. These findings, based on a larger patient population, confirm the preliminary data of Tacke et al. (8) and Wilhelm et al. (7).
Although immediate clinical success is very high, the rate of recurrent venous obstruction in this series is also relatively high: 37% clinical relapse over a relatively short median follow-up interval of 5.23 months. Furthermore, a systematic radiological control for evaluation of stent patency was not performed, which may suggest that the in-stent restenosis ratio may be even higher, given that most of the patients were in the terminal phase of their disease and some may have been too frail or refused to be readmitted for stent re-evaluation. This relatively high re-occlusion rate may be explained by the hypercoagulable state or by tumor progression in or around the stents in this oncological patient group. A relatively high re-occlusion rate in venous stents was also found by Nazarian et al. (2): a 50% overall primary patency rate at 1 year in a patient population with mixed benign and malignant iliac vein stenoses. Moreover, these authors also found statistically higher secondary patency rates in benign disease than in patients with malignant disease (P = 0.05). Treatment of in-stent restenosis can be performed by balloon angioplasty with or without re-stenting; catheter-directed thrombolysis in the event of complete stent thrombosis may be an alternative option if there are no contraindications for thrombolysis. In oncological patients, it is important to exclude the presence of brain or spinal metastases, even if these metastases are asymptomatic, before initiating the thrombolysis, as demonstrated in a series of catheter-directed thrombolysis of thoracic deep venous thrombosis (12). Mechanical thrombectomy may be a valuable alternative to pharmacological thrombolysis in this subgroup of patients.
In case of allergy to iodized contrast medium or in case of renal function impairment, CO2 can be safely used instead of dye without any risk for pulmonary or other side effects as demonstrated by Heye et al. (13) for the mapping of upper limb veins in patients with preterminal renal insufficiency.
The estimated overall survival rate at 3 months follow-up was 68% (95% confidence internal [CI], 47–82%); however, at 1 year follow-up these numbers decreased to nearly 20% (95% CI, 12–29%), stressing the fact that patients with symptomatic iliocaval malignant obstruction have a limited prognosis. When the obstruction is at the level of the inferior vena cava, the survival rate might be even less: in this series, all three patients stented for malignant inferior vena cava obstruction died within 3 months of the procedure. Brountzos et al. (3) found a median follow-up at 62 days after intrahepatic inferior vena cava stenting. It is not clear why the prognosis is worse than for patients with malignant iliac vein obstruction. However, the type of underlying malignancy (primary hepatic cancers versus urogenital cancers), the extent of the tumoral mass or the potential chemotherapeutic treatment options may be different for tumors invading the inferior vena cava versus tumors invading the iliac vein.
Finally, given the minimal invasiveness of the procedure associated with immediate symptom relief, the low morbidity of the procedure and the possibility of withdrawing a patient, we believe that iliocaval stenting is a meaningful and minimally invasive palliative intervention for patients with debilitating symptoms of venous obstruction, despite the relatively high symptomatic in-stent restenosis rate, especially in patients with a life expectancy of at least 3 months.
In conclusion, in this series it is demonstrated that palliative, endovascular treatment of symptomatic, cancer-related iliocaval obstructive disease is safe and effective, with immediate relief of symptoms in the large majority of patients. However, a relatively high rate of recurrent venous obstruction is to be expected related to in-stent occlusion, and overall survival is limited, in particular in patients with inferior vena cava involvement.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.