
Abstract
Background
The rich neovascularization of renal angiomyolipoma (AML) has a tendency for spontaneous rupture with subsequent hemorrhage. Nephrectomy or nephron-sparing surgery has rarely been used as a primary treatment in urgent situations.
Purpose
To evaluate the safety and long-term outcomes for patients treated by urgent transcatheter arterial embolization (TAE) for spontaneous ruptured renal AML with severe hemorrhage.
Material and Methods
A retrospective evaluation was performed of 25 renal AML cases with spontaneous hemorrhage confirmed by imaging. Polyvinyl alcohol (PVA) particles and coils of multiple sizes were used to embolize the spontaneous renal AML ruptures.
Results
The technical success rate of TAE was 96% (24/25). One week post-TAE, 1 patient with recurrent hemorrhage underwent emergency nephrectomy. Minor complications affected 16 patients with post-embolization syndrome; 15 patients resolved using conservative measures and one patient received nephrectomy post TAE 1 week later. All patients were followed up for 24–72 months (median, 50.2 months). Surgical treatment was avoided for 92% (23/25) of patients, and the re-embolization rate was 0% at 2 years post TAE. In the 23 patients without surgical treatment, the mean maximum diameter of renal AML was reduced from 12.4 ± 5.5 cm to 6.3 ± 2.5 cm and no hemorrhage occurred during follow-up.
Conclusion
Urgent TAE is a technically feasible and minimally invasive procedure for controlling severe hemorrhage and preservation of renal function following spontaneous ruptured renal AML.
Introduction
Renal angiomyolipoma (AML) is a benign hamartomatous tumor containing elements of fat, smooth muscle, and abnormal blood vessels in varying proportions (1). Due to differing sizes of blood vessels in renal AML, some small vessels with insufficient elastic layers and muscle walls may form microaneurysms or macroaneurysms, which are prone to rupture and result in hemorrhage (2). Retroperitoneal bleeding or bleeding into the urinary collection system is the main complication of renal AML, which can be severe and life-threatening (3). Treatment options for renal AML include surgical nephrectomy or nephron-sparing surgery and transcatheter arterial embolization (TAE). Although some renal AML cases that meet selected criteria may require complete nephrectomy, the majority of these cases can be managed by a range of nephron sparing approaches, including observation, TAE, or nephron-sparing surgery (1). Nephrectomy causes loss of renal parenchyma and should only be used when clinically justified (4). In addition, the nephron-sparing surgical procedure is difficult to perform by delayed elective surgery due to severe tissue adhesion after bleeding (5). Selective TAE for renal AML and increasingly skilled operators have led to its widespread use in treating tumor bleeding (4,6), and it also has a prophylactic role in preventing future bleeding (7). The present study retrospectively evaluated the long-term efficacy and renal preservation capabilities of urgent TAE for the treatment of severe spontaneous hemorrhage due to ruptured renal AML.
Material and Methods
This study included 25 patients who were diagnosed with renal AML and spontaneous hemorrhage and underwent urgent TAE in our hospital from January 2008 to December 2012. Although informed consent was obtained from all patients pre-TAE, institutional review board approval was also sought for the review, and consent was granted for this retrospective study. The subjects included 17 female and eight male patients aged 26–77 years (mean, 48 years). Two patients (8%) were diagnosed with a tuberous sclerosis complex (TSC).
Unenhanced abdominal computed tomography (CT) images revealed that the kidneys had lost their normal morphological structure and the density of the internal renal AML structures was heterogeneous, including multiple low-density (fatty tissue) areas. Intratumoral hemorrhage of the renal AML presented as a sheet or map-like high-density area. Retroperitoneal hemorrhage was visualized as an inhomogeneous fluid density in the perirenal space and around large blood vessels. A contrast-enhanced CT scan showed augmented images of some parts of the tumor; the high-density areas visible on the unenhanced CT image did not show significant enhancement on the enhanced images. The diagnosis of renal AML rupture was based on CT scan findings (8), symptoms such as abdominal or back pain, and laboratory findings, such as decreased hemoglobin levels.
The endovascular treatment plan was based on proposals by urologists and interventional radiologists in our hospital. Three interventional radiologists performed all of the procedures, one of whom participated in all of the procedures. TAE was performed through the common femoral artery using 5-French angiographic catheters. Abdominal aortography was performed to locate the renal arteries, ascertain the number and morphology of the renal arteries, and evaluate extrarenal arterial tumor feeders. Next, selective renal angiography was performed to determine the number and size of the arteries that supplied blood to the tumor. After careful review of the arteries feeding the tumor, super-selective catheterization into the tumor vessels was performed using a 2.7 F coaxial catheter (Terumo, Tokyo, Japan) to spare as much of the renal parenchyma as possible. A bottle of polyvinyl alcohol particles (350–560 µm; Cook, Bloomington, IN, USA) was mixed with 10 mL contrast media (diluted 1:1) and 1 million units of penicillin G and/or 80 mg gentamicin. Under fluoroscopic guidance, the mixture was carefully injected through the catheter into the tumor arteries.
For patients with aneurysms, PVA was used to embolize bleeding arteries and the feeding vessels of the aneurysms, and then coils (3–10 mm × 5–12 cm) or microcoils (2–3 mm × 2–3 cm; Cook Inc.), according to the diameter of target vessel, were used to embolize the feeder artery trunk. Patients with large tumors rich in angiogenic components and without aneurysms underwent embolization using PVA. Coils were used to embolize the main feeder arteries when complete embolization could not be achieved by using PVA only. Contrast medium was injected through the catheter to detect the progress of the embolization at different intervals. Complete embolization was defined as complete obliteration of tumor vessels and a lack of opacification of the tumor on post-TAE images (4).
After groin hemostasis was achieved, patients were transferred to the interventional ward and their vital signs, urine color, and urine output were observed. Patients with post-embolization syndrome (low-grade fever, abdominal or back pain, and vomiting 3–7 days after TAE) were given supportive treatment until the symptoms disappeared. Routine blood, urine, serum creatinine, and urea nitrogen tests were conducted within 5–7 days after TAE.
Follow-up and statistical analysis
Demographic features, symptoms, clinical course, complications, and relapse were all recorded. Enhanced CT, serum creatinine, and urea nitrogen were evaluated 1 week, 6, 12, and 24 months post TAE to assess the changes in renal function, maximum diameter of renal AML, and aneurysms. Mean and standard deviation (SD) of tumor size were calculated based on pre-TAE and follow-up images. Data are shown as mean ± SD. Statistical analysis was performed using SPSS 13.0 (SPSS Inc., Chicago, IL, USA). One-way analysis of variance (ANOVA) was used to compare the maximum diameter of renal AML, serum creatinine, and urea nitrogen during follow-up. Significance was established at P < 0.05.
Results
Patient demographics and clinical characteristics.
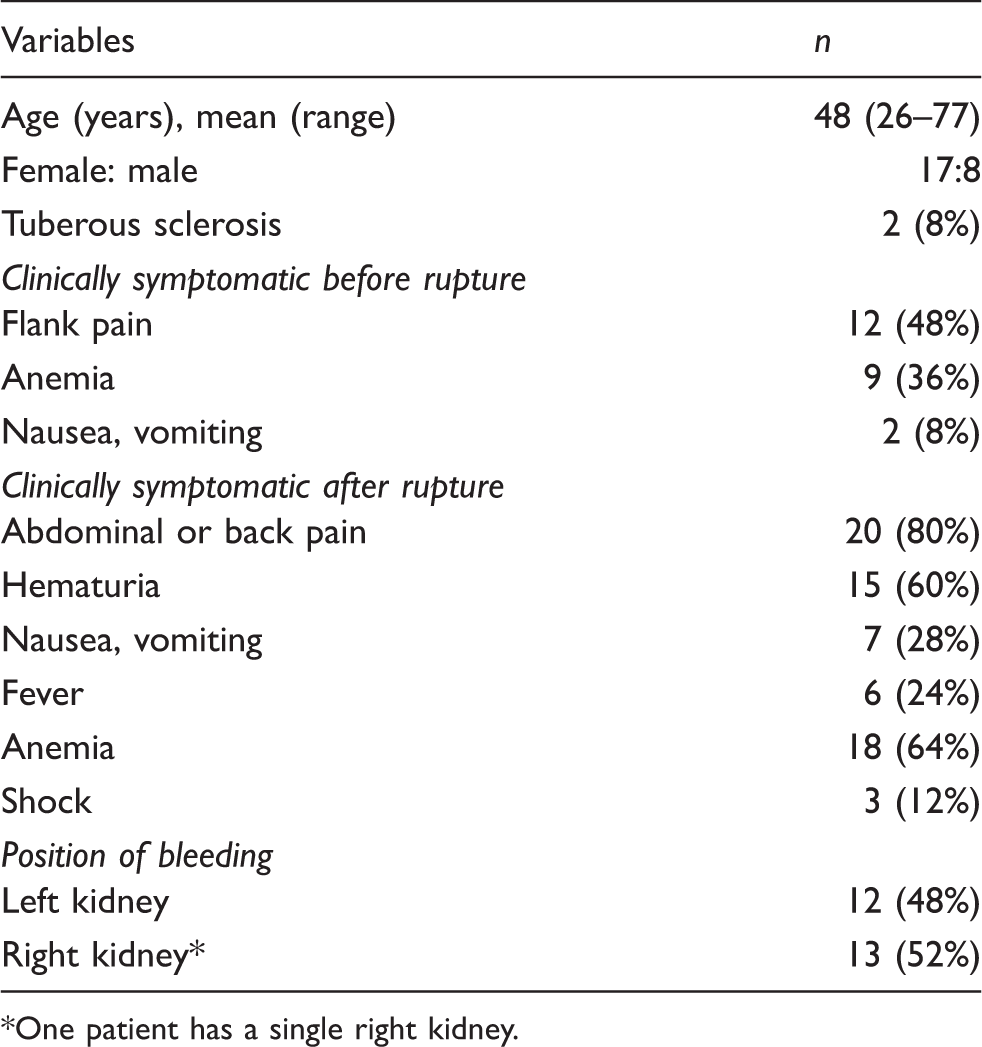
One patient has a single right kidney.
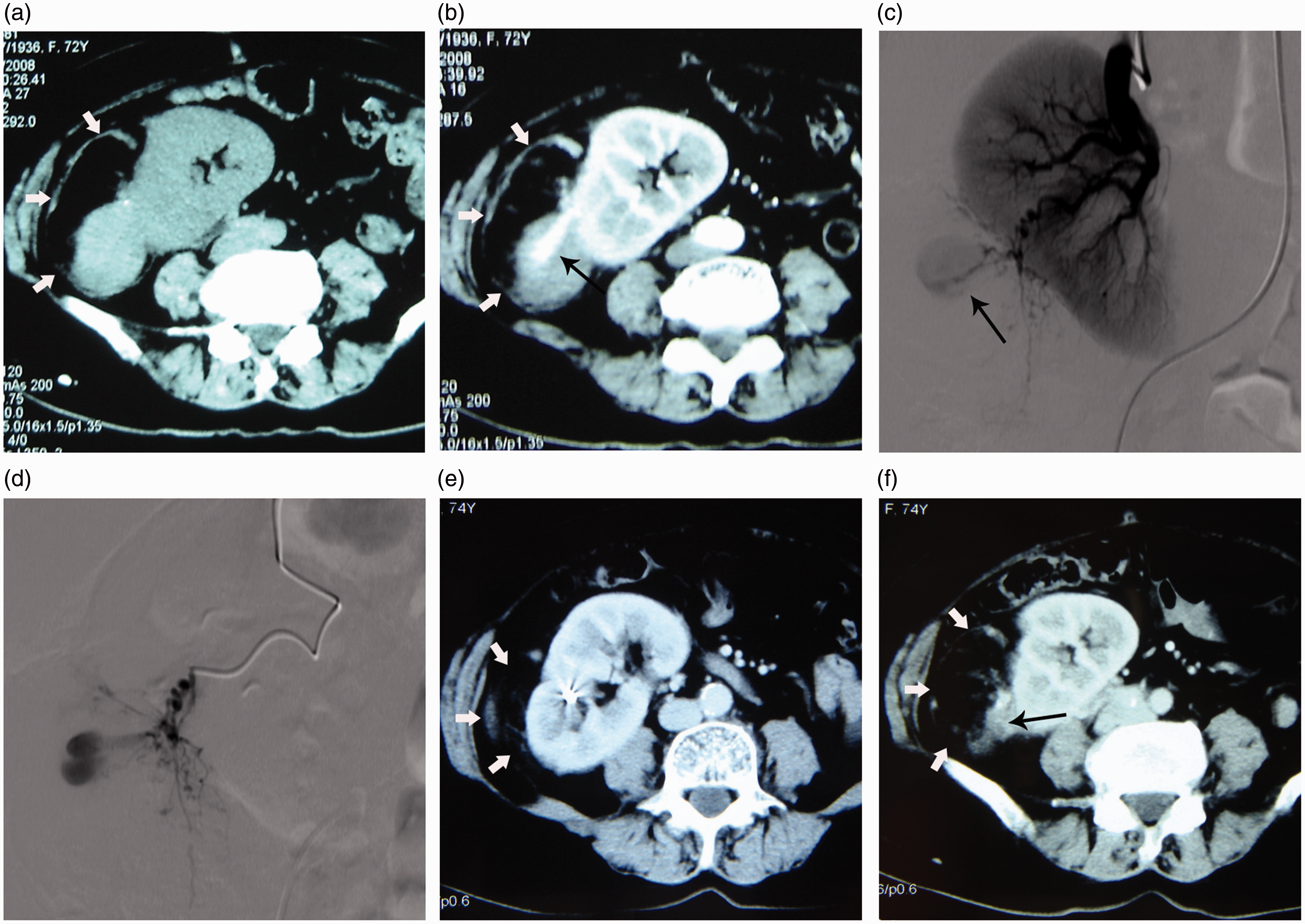
A 72-year-old woman with a single kidney had a right AML, accompanied by acute flank pain and hematuria. (a) CT revealed the renal AML as a mixed, low-density area, including adipose tissue, smooth muscle, and vascular tissue in the right renal lower regions. (b) Enhanced CT demonstrated a capsule-like aneurysm with a largest diameter of 3.2 cm (long arrow). (c) Renoarteriography showed multiple tumor vessels and an aneurysm (long arrow). (d) Superselective catheterization with a 2.7 F coaxial catheter revealed the AML feeder and aneurysm. Complete embolization with two coils and PVA was achieved (not shown). (e, f) Follow-up CT showed tumor shrinkage from 12.1 × 6.5 cm to 7.6 × 5.1 cm (white arrows) with no remaining aneurysm (long arrow) after 24 months.
Patients’ outcomes and prognosis.
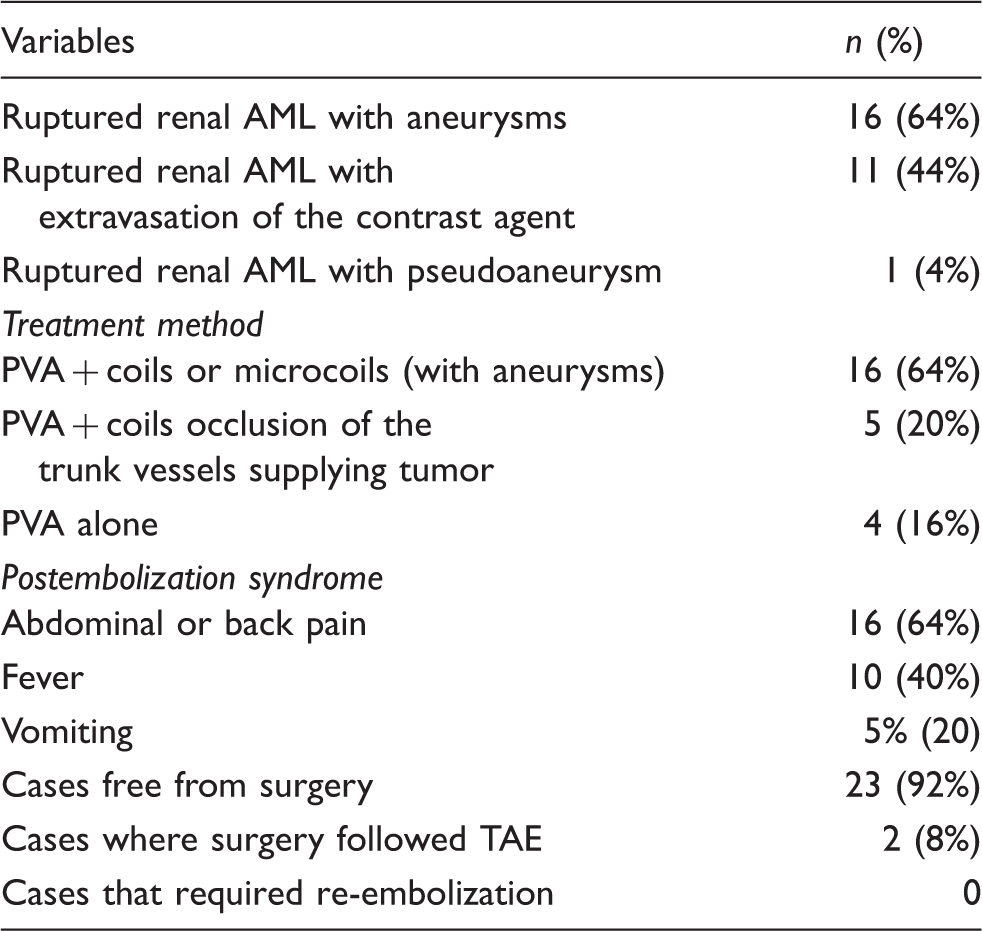
To spare as much renal parenchyma as possible, 2.7 F coaxial catheters were used for super-selective catheterization into the vessels of all tumors. Twenty coils and 10 microcoils were used in these 25 cases. TAE was performed once in all patients. Sixteen patients with aneurysms underwent embolization using PVA and coils or microcoils (Fig. 1), and four patients without aneurysms underwent embolization using PVA. After embolization, angiography of the above-mentioned 20 cases showed occlusion of all aneurysms and tumor vessels. In the other five patients without aneurysms, angiography showed occlusion of most vessels in the renal AML, but not the trunk vessels supplying renal AML after embolization with PVA. A final angiogram demonstrated that the target arteries were successfully embolized with coils and that there were no remaining tumor vessels.
In this study, all patients survived after receiving TAE. The technical success rate of TAE was 96% (24/25) with 24 angiomyolipomas with spontaneous hemorrhage successfully embolized in 25 patients. In the failed case, 7 days post TAE, the patient suddenly presented with tachycardia, decreased blood pressure, abdominal distension, and increased tension. When hemodynamic status was stabilized via blood transfusion, the patient underwent emergency nephrectomy. After the operation, the patient recovered well and was discharged after 1 week.
Minor complications affected 16 patients with post-embolization syndrome, which presented as flank pain (n = 16), fever (n = 10), or vomiting (n = 5); 15 patients underwent conservative measures, and one patient received nephrectomy to prevent uncontrollable post-embolization syndrome when hemodynamic status was stabilized with TAE 1 week later.
In the 23 patients free of surgery post TAE, sequential changes of serum creatinine, urea nitrogen, and tumor size during follow-up were compared.
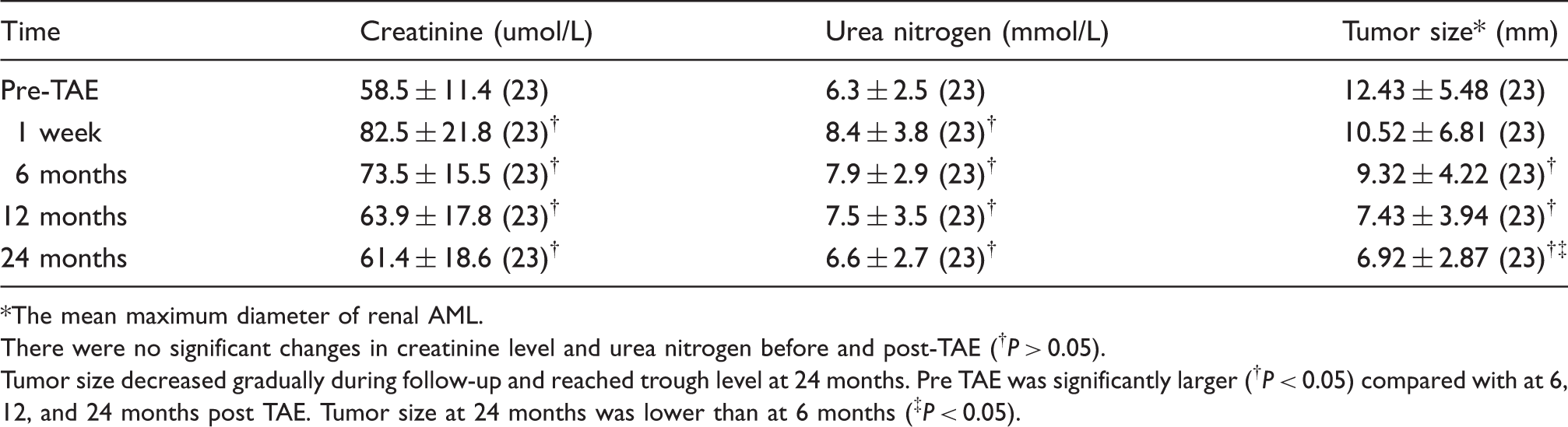
The mean maximum diameter of renal AML.
There were no significant changes in creatinine level and urea nitrogen before and post-TAE (†P > 0.05).
Tumor size decreased gradually during follow-up and reached trough level at 24 months. Pre TAE was significantly larger (†P < 0.05) compared with at 6, 12, and 24 months post TAE. Tumor size at 24 months was lower than at 6 months (‡P < 0.05).
Discussion
As a renal AML enlarges, it usually becomes more vascular and subsequently develops tortuous vessels and aneurysms, which in turn confer a higher probability of rupture (8,9). The most serious complication of renal AML is spontaneous rupture of the tumor with life-threatening hemorrhage (3,5). This tendency for bleeding originates from the irregular, tortuous, aneurysmal blood vessels that constitute the angiogenic component of the tumor (10). Additionally, the risk of bleeding grows together with the size of the renal AML (11). Nelson et al. (1) and Dickinson et al. (12) observed that an asymptomatic renal AML >8 cm had a high risk of bleeding; therefore, they suggested that such a tumor should be treated. In this study, the diameters of all the bleeding renal AML were >8 cm, and all of the patients had different degrees of clinical symptoms before tumor rupture according to their medical history.
However, some researchers have found that the presence of aneurysms larger than 5 mm had greater probability for predicting bleeding than renal AML size (8,13). The abnormal vessels in the renal AML are usually bent into a spiral-shaped kink or sinusoidal vascular network, and the wall of these abnormal vessels becomes glass-like, thereby allowing an aneurysm to easily form (2). In our cases, aneurysm formation was detected in 16 patients (64%), and the diameters of the aneurysms were all larger than 5 mm, as shown during angiography. These findings support our hypothesis that there is a significant relationship between tumor size, aneurysm formation, and spontaneous rupture.
The detection rate of aneurysm formation and extravasation of the contrast agent by angiography was higher than by enhanced CT scan in our patients. However, advances in CT diagnostic technology may improve the detection of aneurysm in renal AML. As aneurysms may be a predictor of spontaneous rupture, their detection by CT would help determine the most appropriate management strategy for renal AML. As renal AML is a benign tumor, radical nephrectomy and nephron-sparing surgery are the traditional treatments. Currently, TAE has become increasingly popular for the management of renal AML, as it spares the normal renal parenchyma, manages acute tumor bleeding, and is also to be used as a preoperative adjuvant treatment to reduce blood loss during surgery (1,5).
Tsai et al. (11) suggested that TAE should be the first choice for spontaneous ruptured renal AML with severe hemorrhage. In this study, the technical success rate of TAE was 96% (24/25). Our treatment goal of complete obliteration of the angiogenic component was met in 24 (96%) of 25 tumors. Surgical treatment was avoided in 92% of patients (23/25), and the re-embolization rate was 0% at 2 years post TAE. In those 23 patients, the mean maximum diameter of renal AML was reduced from 12.4 ± 5.5 cm to 6.9 ± 2.9 during follow-up. These results suggest that urgent TAE with 2.7 F coaxial catheter in all patients has a reliable midterm effect. It is significant that no recurrent hemorrhage or tumor growth occurred in the 23 patients at 2 years post TAE, which is a better result, compared to that reported by others groups (13,14).
As a preoperative adjuvant treatment to reduce blood loss during surgery, TAE can be used for the prophylaxis of high-risk tumors and for acute management of tumor bleeding (1,15). Moreover, patients who suffer from hemodynamic instability and medical co-morbidities are able to undergo further surgery after urgent TAE, such as nephrectomy or nephron-sparing surgery. In this study, the reason for the single failure was the difficulty in superselectively catheterizing many small, tortuous tumor vessels, even when using a microcatheter. Considering the fact that the tumor’s diameter was >12 cm and that was located near the hilum, and had many blood clots and necrotic tumor tissues, re-embolization was less clinically effective. The patient eventually underwent emergency nephrectomy.
Liakakos et al. (16) observed that adhesion forms 72 h after renal AML tissue injury and becomes more intensive at approximately 10 days to 2 weeks. In the present study, one patient with recurrent hemorrhage and one patient with uncontrollable post-embolization syndrome underwent nephrectomy. In the two nephrectomy operations, the surgical areas were clear without severe adhesion. The blood loss was less than during the nephrectomy operations without TAE, and renal pedicle control was not necessary as the feeding arteries had been obliterated by TAE. Hence, we are in concordance with Jou et al. (5), who performed nephron-sparing surgery 1 week after urgent TAE when a patient’s hemodynamic status is stabilized. However, the reason of Jou et al. (5) performed nephron-sparing surgery was they believed renal AML would shrink with liquefactive necrosis and tend to induce abscess formation post TAE. PVA mixed with antibiotics and contrast has been widely used in partial splenic embolization (PSE) to prevent splenic abscess after PSE (17). In order to prevent infection, we mixed antibiotics into PVA and contrast to embolize the spontaneous renal AML ruptures as the embolization strategy used in PSE. In the present study, there was no local infection case with this modality of embolization during the follow-up.
During follow-up, there was no recurrent hemorrhage or re-embolization in the 23 patients free of surgery post TAE. Although TAE had risk factors of renal function deterioration, such as loss of renal parenchyma due to non-target embolization and nephrotoxicity of contrast media, no statistical differences were noted between serum creatinine and urea nitrogen before and post-TAE during the 2-year follow-up. Baba et al. (18) concluded that arterial embolization of renal AML using absolute ethanol may not induce renal dysfunction in the embolized kidney and may actually increase renal blood flow in the non-embolized kidney immediately after embolization. Furthermore, Lee et al. (4) demonstrated that TAE alone for the treatment of renal AML was able to preserve renal function, despite the presence of mild pre-existing renal insufficiency. The authors concluded that nephrectomy should generally be minimized because the outcome of total nephrectomy may be worse than TAE alone (4). Hence, we suggest that urgent TAE should be the first choice for treating renal AML with spontaneous hemorrhage. Nephrectomy should be reserved for the conditions summarized by Nelson et al. (1): unavailability of TAE for bleeding control, the tumor is located near the hilum, and the renal AML is so large that it nearly replaces the entire kidney.
This study had several limitations. For instance, due to the small number of cases, more data are needed to confirm the safety and efficacy of this method of treating ruptured renal AML. The follow-up CT images of some patients were obtained from other hospitals with different equipment than that available in our hospital. Finally, inaccurate tumor measurements made it difficult to obtain better data for analysis and to determine statistical significance. A prospective randomized controlled study with a large number of subjects is needed to investigate whether urgent TAE is a superior treatment for patients with severe hemorrhage due to spontaneously ruptured renal AML.
In conclusion, urgent TAE is a safe, minimally invasive procedure for the treatment of severe hemorrhage due to spontaneously ruptured renal AML, causes minimal damage to renal function, and has an acceptable complication rate and overall good AML volume reduction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.