
Abstract
Background
Lumbar spine radiography is often performed instead of CT for radiation dose concerns.
Purpose
To compare image quality and diagnostic information from low dose lumbar spine CT at an effective dose of about 1 mSv with lumbar spine radiography.
Material and Methods
Fifty-one patients were examined by both methods. Five reviewers scored all examinations on eight image quality criteria using a five-graded scale and also assessed three common pathologic changes.
Results
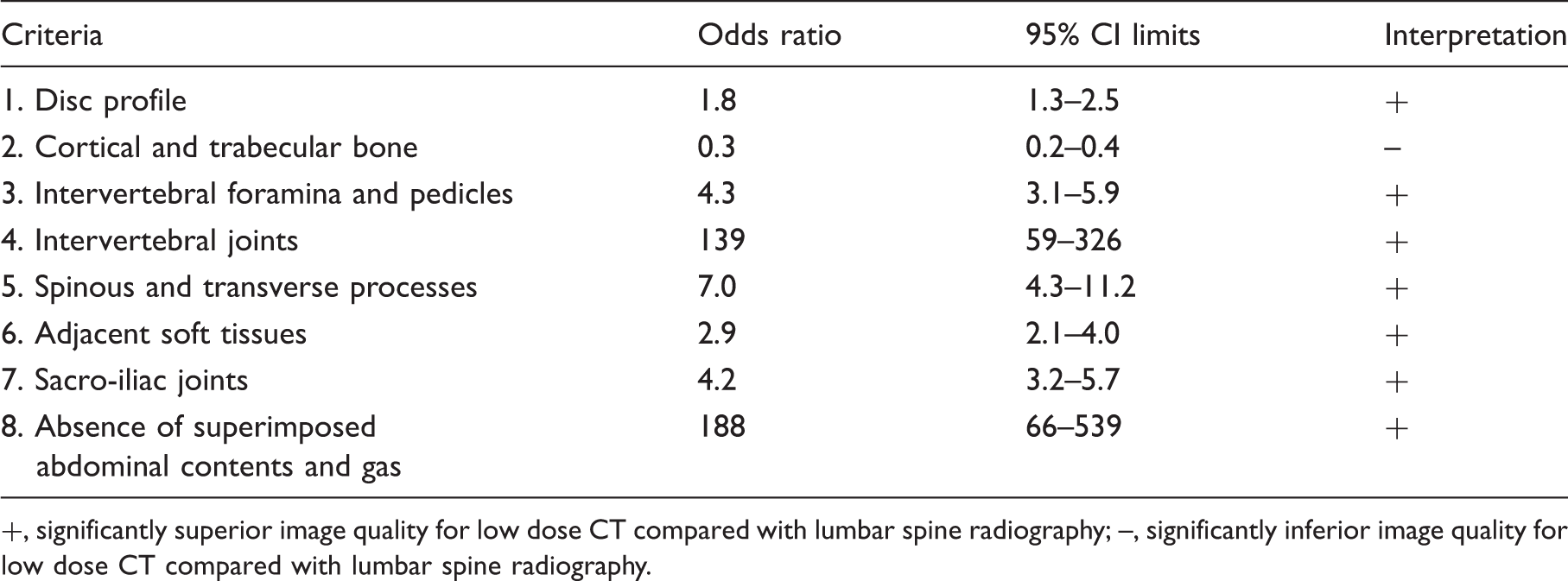
Low dose CT scored better than radiography on the following: sharp reproduction of disc profile and vertebral end-plates (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.3–2.5), intervertebral foramina and pedicles (OR, 4.3; 95% CI, 3.1–5.9), intervertebral joints (OR, 139; 95% CI, 59–326), spinous and transverse processes (OR, 7.0; 95% CI, 4.3–11.2), sacro-iliac joints (OR, 4.2; 95% CI, 3.2–5.7), reproduction of the adjacent soft tissues (OR, 2.9; 95% CI, 2.1–4.0), and absence of any obscuring superimposed gastrointestinal gas and contents (OR, 188; 95% CI, 66–539). Radiography scored better on sharp reproduction of cortical and trabecular bone (OR, 0.3; 95% CI, 0.2–0.4). The reviewers visualized disk degeneration, spondylosis/diffuse idiopathic skeletal hyperostosis (DISH) and intervertebral joint osteoarthritis more clearly and were more certain with low dose CT. Mean time to review low dose CT was 204 s (95% CI, 194–214 s.), radiography 152 s (95% CI, 146–158 s.). The effective dose for low dose CT was 1.0–1.1 mSv, for radiography 0.7 mSv.
Conclusion
Low dose lumbar spine CT at about 1 mSv has superior image quality to lumbar spine radiography with more anatomical and diagnostic information.
Introduction
Despite abundant evidence of the limited value of lumbar spine radiography (1,2), it is still the most common radiologic investigation of the lumbar spine. Many physicians rely on it as a simple, cheap, and widely available preliminary diagnostic modality with relatively low radiation, with effective dose about 1 mSv (3,4).
Computed tomography (CT) has improved musculoskeletal imaging. CT is more sensitive than radiography for evaluation of multiple myeloma (5), is superior to radiography in cervical spine injury (6), and reduces the risk of missing a fracture of the thoracolumbar spine (2). Spiral CT with three-dimensional (3D) reconstructions gives better and more accurate demonstration of different types of fractures and allows for more precise preoperative surgical planning. On the other hand, the dramatic increase in the number of CT examinations globally has increased the collective radiation dose. Awareness has been raised of both the hazards of medical ionizing radiation and the need to reduce it as much as possible (7). The effective dose of lumbar spine CT has been reported as about 8.7 mSv in Sweden (3), but can be as high as 19 mSv (8). To minimize radiation exposure clinicians may try to avoid or minimize the use of unnecessary “standard” CT by using conventional radiography. However, it is possible to perform CT at much lower dose than with standard CT, at the expense of increased noise and reduced image quality; it can even be done using the same relatively low radiation dose as lumbar spine radiography (7,9,10). CT at this low dose level may have a higher diagnostic value than radiography and may give more information on anatomy as well as on pathologic changes.
The current study was performed to evaluate and compare image quality and anatomic and diagnostic information from low dose CT lumbar spine at about 1 mSv with lumbar spine radiography.
Material and Methods
Patients
The study was approved by the regional ethics committee. Inclusion criteria were adults referred for lumbar spine radiography. Exclusion criteria were age below 18 years, pregnancy, coma, dementia or inability to understand oral or written instructions. A power analysis showed that with better image quality than the reference method in 70% of the cases, 51 cases would be needed for 80% power. In a convenience sample, 51 patients (16 men, 35 women) gave informed consent and accepted to participate (53 were invited, two declined to participate). Most patients were referred from primary healthcare (n = 48), two were referred from the orthopedic department and one from the neurological department. The major primary indication was low back pain without known serious underlying conditions (48 cases with back pain; 10 with neurological symptoms, 38 without, one with paraesthesia in the thigh, one for control of osteosynthesis material, one control for vertebral compression fracture).
Mean age was 58 years (SD, 13.9; age range, 21–81 years). Mean weight was 79.6 kg (SD, 15.6; range, 55–125 kg) and mean height was 169 cm (SD, 9.3; range, 152–194 cm). Mean BMI was 27.7 (SD, 4.0; range, 20–38). There were no underweight study patients. The patients were classified as being of normal weight (BMI 18.5–24.9), overweight (BMI 25.0–29.9), or obese (BMI > 30.0) (11).
Imaging
Lumbar spine radiography and low dose CT were performed the same day. Radiography was performed on a digital X-ray system (DRX-Evolution, Carestream Health, Rochester, NY, USA) with a flat panel detector (PaxScan CsI, pixel spacing 0.139 × 0.139 mm, image depth 12 bits). Standard clinical settings for lumbar spine were used; 75 kV for the anterior-posterior (AP) projection, 85 kV for the lateral and lumbosacral joint projections using automatic exposure control. The average number of exposures was 3.5 (range, 2–5) due to clinical status, imaging requirements, and possible re-takes.
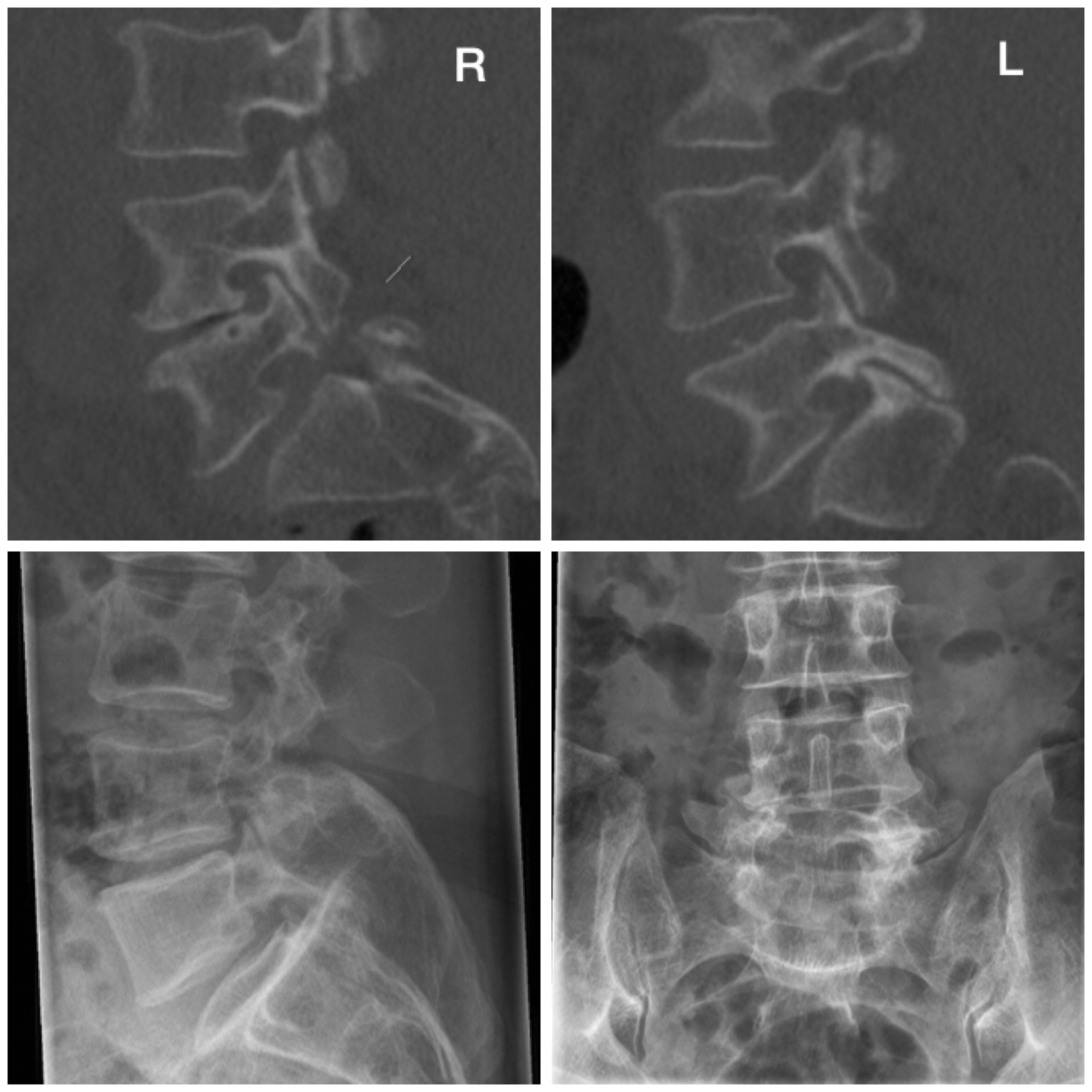
Low dose CT was performed using a Somatom Definition AS scanner (Siemens, Erlangen, Germany; 40 channels), using settings from a phantom study (10), giving about 1 mSv effective dose; tube potential 120 kV, reference mAs 30, collimation 40 × 0.6 mm, rotation time 0.5 s, pitch 1.4, field of view 200 × 200 mm, convolution filter B41f (medium plus), with automatic dose modulation. Axial, coronal, and sagittal multiplanar reformations (MPR) with 2 mm thickness and 2 mm increment were sent to the picture archiving and communication system (PACS) (Fig. 1).
Low dose CT of a 27-year-old woman of normal weight with good image quality, which demonstrates the sharp reproduction of different anatomical structures of the lumbar spine.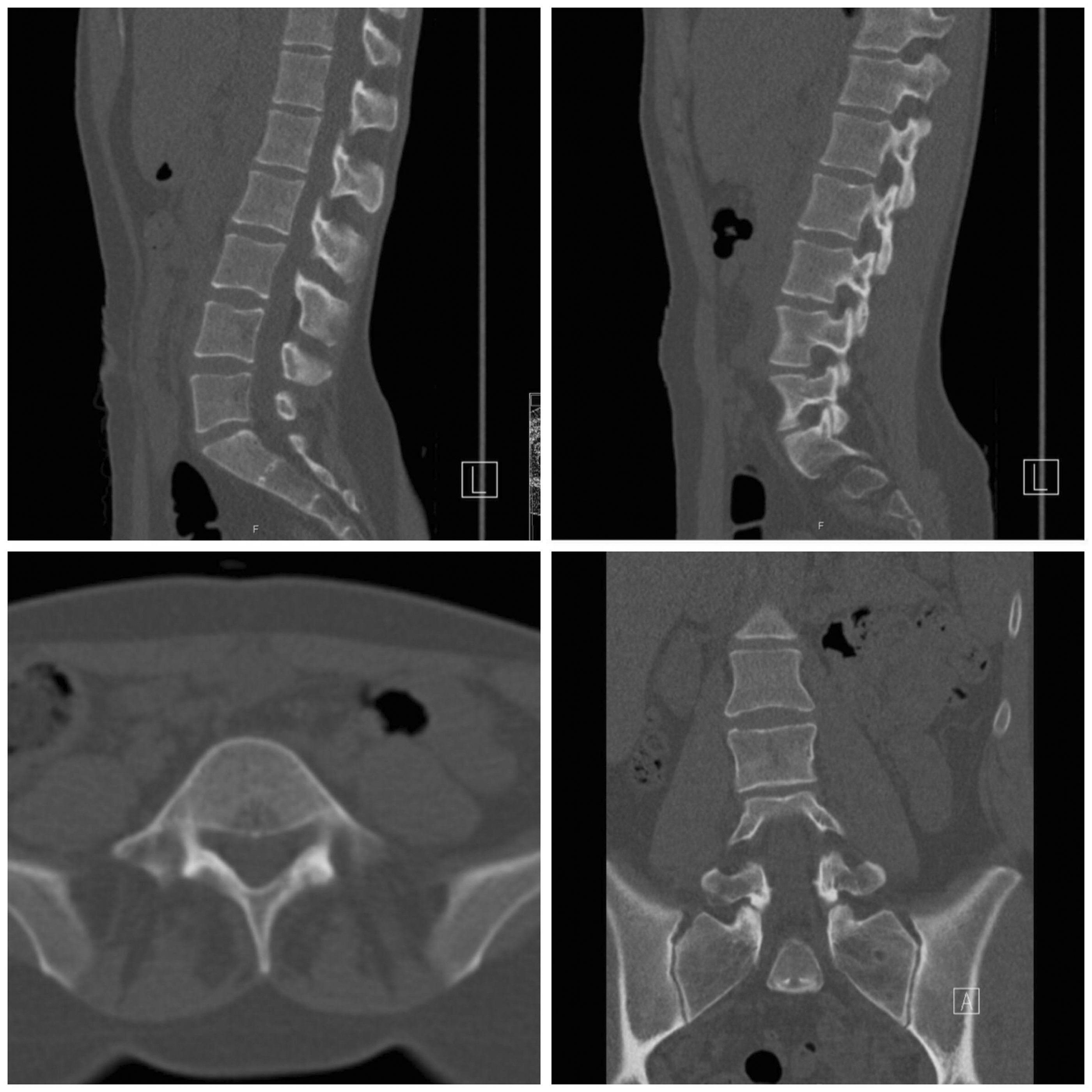
Image evaluation
The 102 examinations (51 from each modality) were presented in random order. Five reviewers with 8, 10, 12, 25, and 32 years of experience in diagnostic radiology independently scored all studies blinded to patient data using the PACS with free use of the PACS tools:
A) Scoring of image quality according to a modification of the European guidelines on image quality for CT (EUR 16262) (12) and diagnostic radiographic images (EUR 16260) (13). Each reviewer scored the following criteria from 0 to 4:
Sharp reproduction of the disc profile and the upper and lower-plate surfaces of vertebrae. Sharp reproduction of the cortical (cortex) and the trabecular bone. Sharp reproduction of the intervertebral foramina and pedicles. Sharp reproduction of the intervertebral joints. Sharp reproduction of the spinous and transverse processes. Reproduction of the adjacent soft tissues. Sharp reproduction of the sacro-iliac joints (the included part of the joints in the examination). Absence of any obscuring superimposed abdominal contents or gastrointestinal gas.
The scoring levels for each criterion were: 0, confident that the criterion is not fulfilled; 1, somewhat confident that the criterion is not fulfilled; 2, indecisive whether the criterion is fulfilled or not; 3, somewhat confident that the criterion is fulfilled; and 4, confident that the criterion is fulfilled. One reviewer scored all examinations again 6 months later to assess intra-observer agreement.
B) Assessment of pathology. Three common radiologic findings (disk degeneration, intervertebral joint osteoarthritis, and spondylosis/diffuse idiopathic skeletal hyperostosis (DISH)) were evaluated. For each detected type of pathology the vertebral level(s) was noted. Reviewers also scored how clearly the lesions were seen and how certain the diagnosis was on a three-graded scale.
C) Time needed to review each case.
Radiation dose
For radiography the dose-area product (DAP) was measured for each projection with a DAP meter integrated in the equipment. The PCXMC computer program v2.0 (Finnish Radiation and Nuclear Safety Authority, Helsinki, Finland) was used to calculate the effective dose for each BMI category with the average DAP of each projection. The field size at the detector was 18*42 cm for the AP and lateral projections and 18*30 cm for the lumbosacral projection. For CT, the effective tube loading was recorded for each examination and the average value used to calculate the effective dose for each BMI category with the software CT-Expo v 2.3 (SASCRAD, Buchholz, Germany). The scan area covers Th12 to S2 in a virtual phantom.
Statistical analysis
The data for each image quality criterion were analyzed with the generalized estimating equation (GEE) model (14) due to repeated measurements as each patient was assessed by five observers for each method. The measure of associations was odds ratios (OR) with 95% confidence intervals (CI). An OR of 1 is interpreted as no difference between methods and an OR higher than 1 is interpreted as low dose CT a better method compared with radiography. All statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA). The same analysis was performed after stratifying data into BMI subgroups. Inter-observer agreement for all five reviewers according to free-marginal multirater kappa (multirater κfree) was estimated (15). The scoring scale was converted from a 5-grade scale to 3 grades (0–1 as 1, criterion is not fulfilled; 2 as 2, indecisive; and 3–4 as 3, criterion is fulfilled). Data from the first and second observation of one reviewer were used to evaluate the intra-observer agreement. Calculations were performed with an online kappa calculator (16). Values of free marginal kappa can range from −1.0 to 1.0, with −1.0 indicating perfect disagreement worse than chance, 0.0 indicating agreement equal to chance, and 1.0 indicating perfect agreement. A rule of thumb is that a kappa of 0.70 or above indicates adequate agreement (16).
Results
Image quality was rated significantly higher for CT compared with lumbar spine radiography (Fig. 2) for all criteria except “Sharp reproduction of the cortical and the trabecular bone” which was rated significantly better for radiography (Table 1).
Scores for all reviewers (R1–5) on all criteria for (a) low dose CT and (b) lumbar spine radiography. Full score for each criterion is 1020 (4 max score × 5 reviewers × 51 cases). CT was scored higher on all criteria except on “Sharp reproduction of cortical and trabecular bone”. Image quality scoring for low dose lumbar spine CT compared with lumbar spine radiography. Odds ratios with 95% CI limits according to the generalized estimating equation (GEE) model for repeated measurements. +, significantly superior image quality for low dose CT compared with lumbar spine radiography; –, significantly inferior image quality for low dose CT compared with lumbar spine radiography.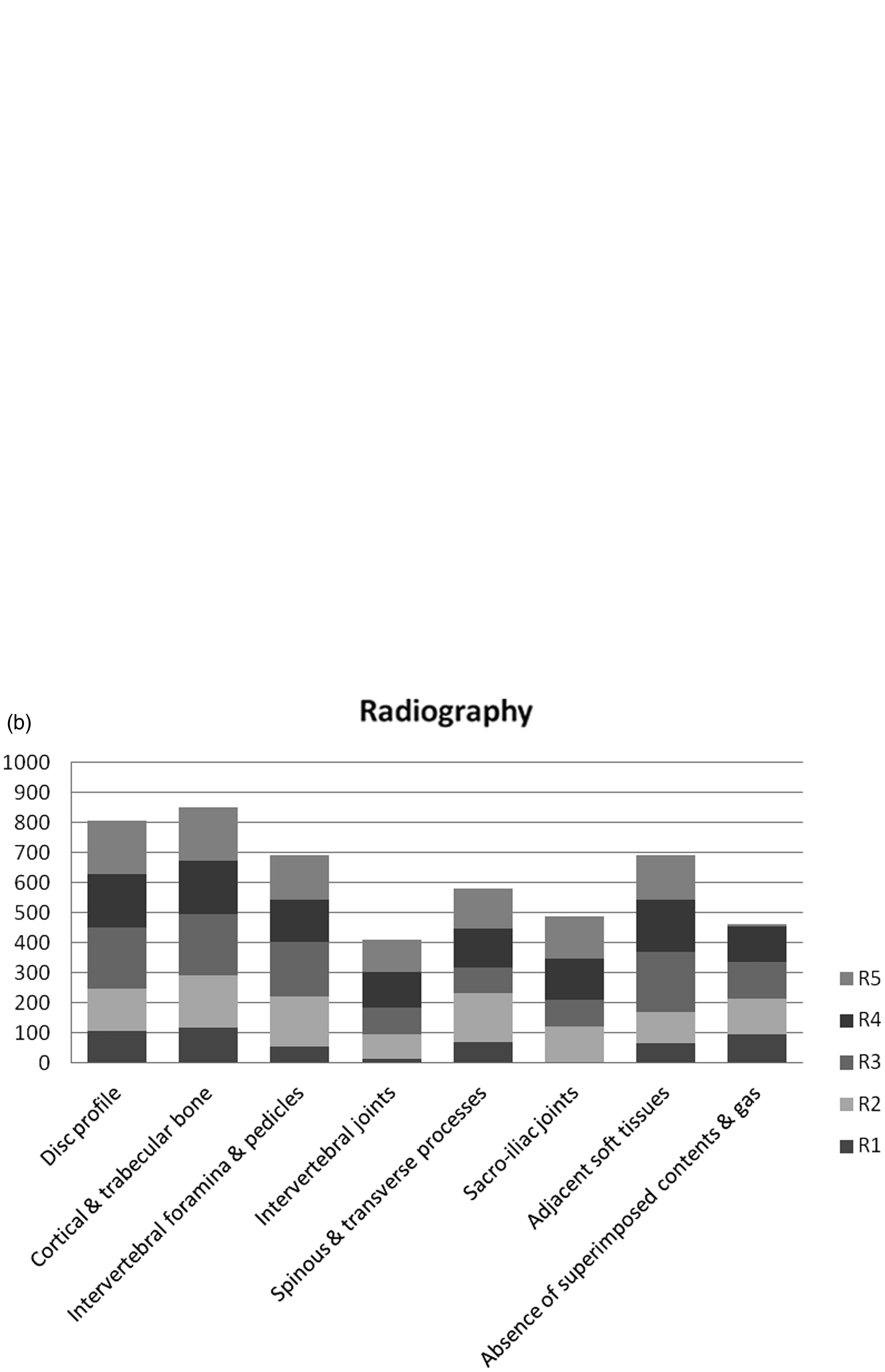
When the GEE analysis was performed after stratifying data into BMI subgroups, the result for each subgroup was similar to the results for all data (Table 1), i.e. all criteria were scored significantly better for low dose CT except the criterion “Cortical and trabecular bone”. Only the criterion “Disk profile” showed no significant difference between low dose CT and radiography for the obese subgroup.
Inter- and intra-observer agreement in the scoring of eight image quality criteria for low dose CT and radiography according to free-marginal Kappa.
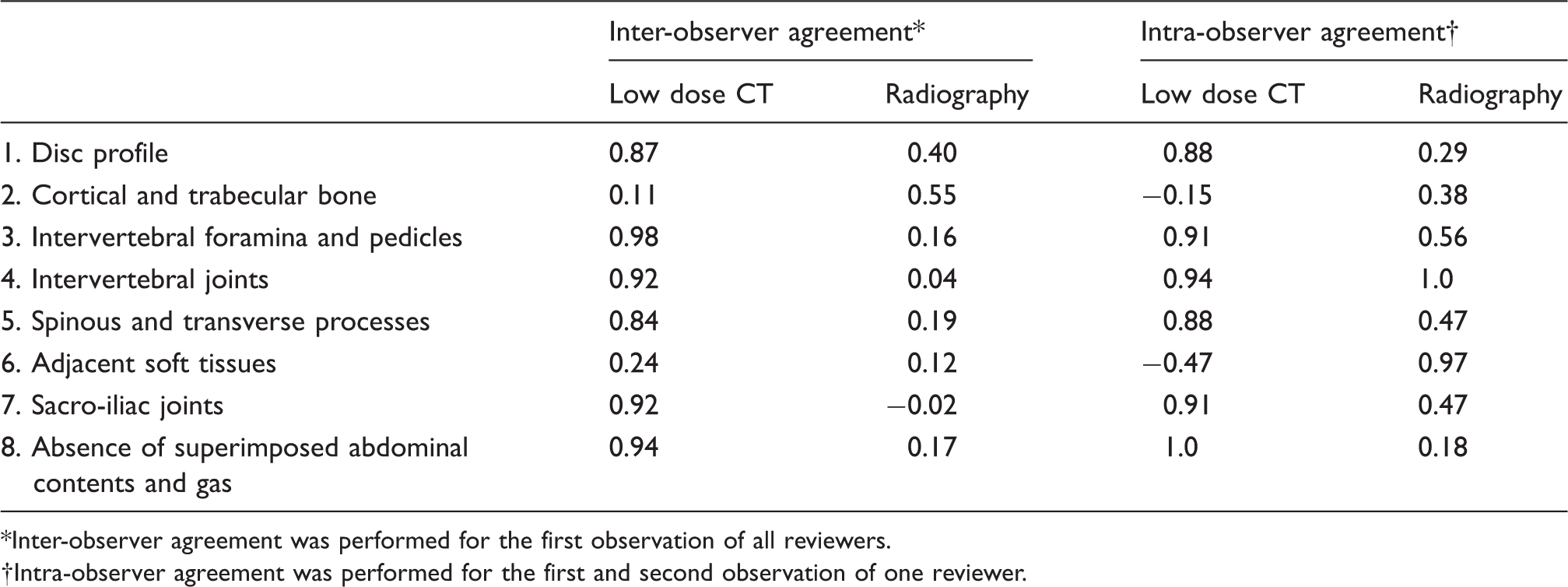
Inter-observer agreement was performed for the first observation of all reviewers.
Intra-observer agreement was performed for the first and second observation of one reviewer.
Pathological findings in 255 observations (51 cases × 5 reviewers), including scoring for visibility and certainty.
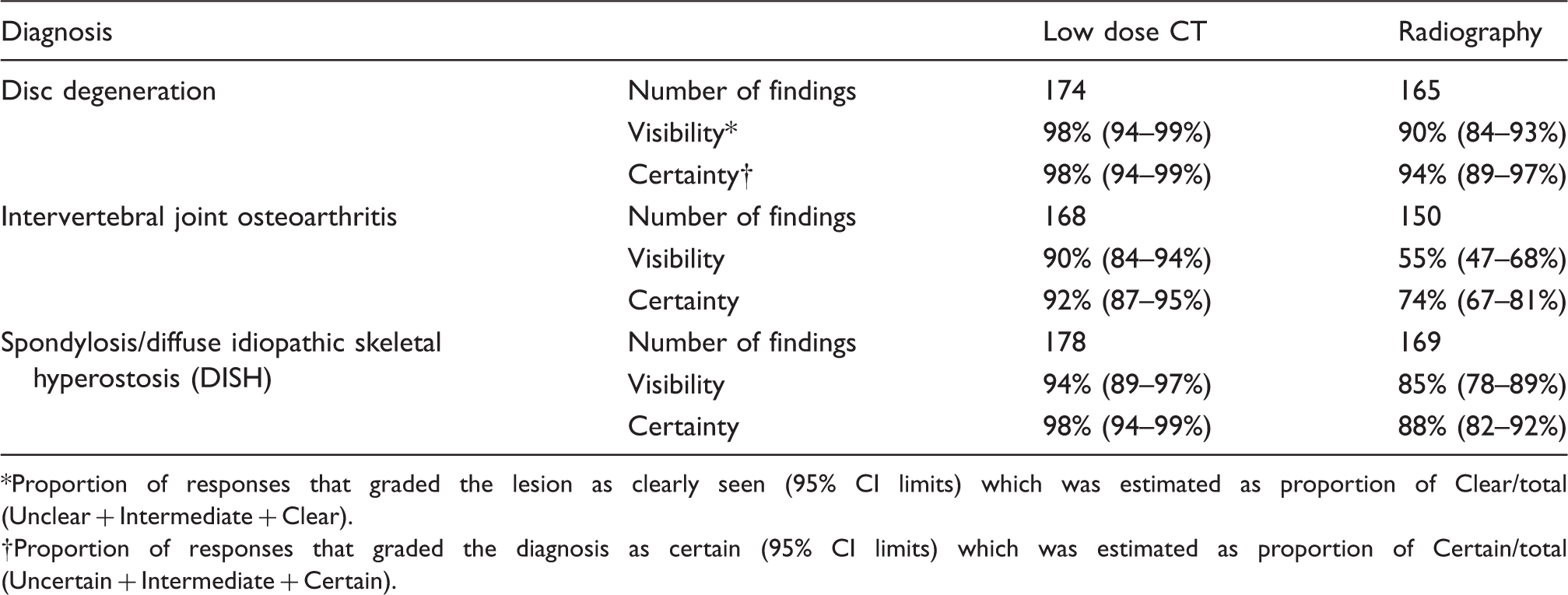
Proportion of responses that graded the lesion as clearly seen (95% CI limits) which was estimated as proportion of Clear/total (Unclear + Intermediate + Clear).
Proportion of responses that graded the diagnosis as certain (95% CI limits) which was estimated as proportion of Certain/total (Uncertain + Intermediate + Certain).
A 64-year-old man with unilateral spondylolysis at the L5-S1 level, well demonstrated at low dose CT (line). This finding was difficult to detect and to determine if it was uni- or bilateral on lumbar spine radiography.
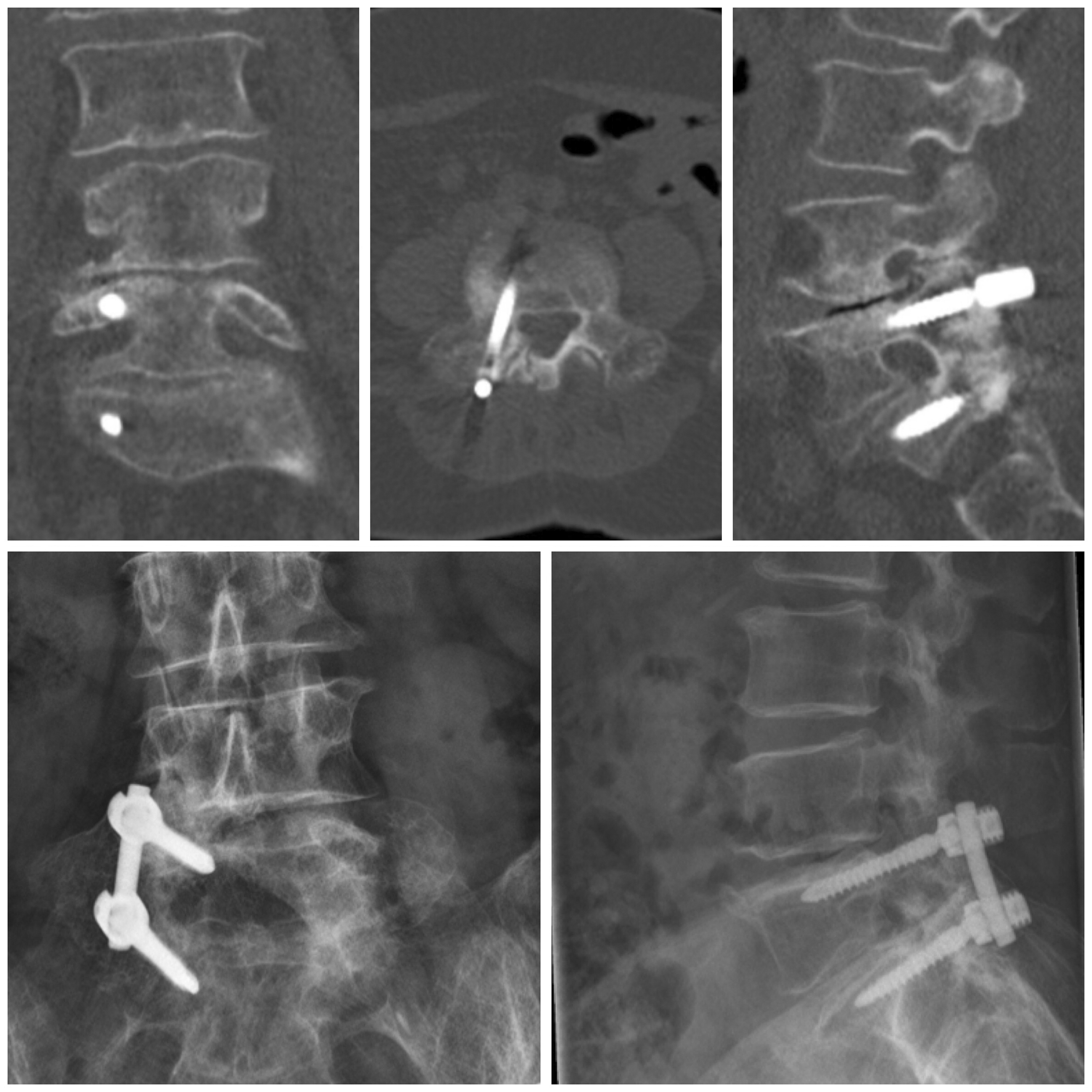
A 71-year-old woman with unilateral pedicle screws on the right side at the L5-S1 level. Metal artifacts at low dose CT were acceptable with clear visualization of the screw placement in the L5 and S1 vertebrae. This was more difficult to determine on lumbar spine radiography.
Dosimetry for low dose CT and radiography according to BMI.
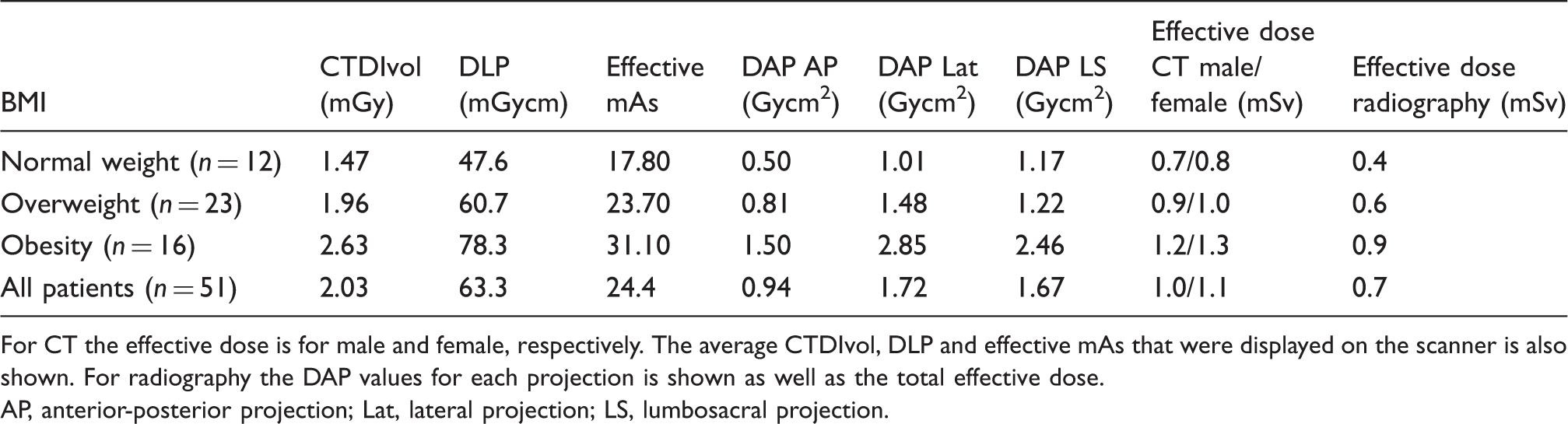
For CT the effective dose is for male and female, respectively. The average CTDIvol, DLP and effective mAs that were displayed on the scanner is also shown. For radiography the DAP values for each projection is shown as well as the total effective dose.
AP, anterior-posterior projection; Lat, lateral projection; LS, lumbosacral projection.
Discussion
The current study has shown that low dose CT improves visualization of most anatomical structures as well as giving observers higher confidence in evaluating some common pathologic lesions compared with radiography. Pathology was more clearly seen with low dose CT and the reviewers were more certain of their findings. Even though these benign lesions are of no clinical concern, the easier detection with CT may reflect the benefit of using low dose CT to visualize small lesions in general, including metastases. Further research on evaluation of the diagnostic accuracy of low dose CT is warranted, especially for the detection of lesions that are highly dependent on visualization of cortical or trabecular bone such as fracture detection.
The GEE model (14) was used since it accounts for the fact that each image was assessed with repeated measurements by five observers for each method. Well-defined criteria, such as the EU criteria (12), are often used, and the score is typically set on a scale with a limited number of steps. In statistical terms, the score is defined on an ordinal scale, and this requires adapted statistical methods. This kind of model is a form of logistic regression for repeated measurement with ordinal scaled outcome and is also called proportional odds model for repeated measurement.
Several successful applications of low dose CT in musculoskeletal imaging have been reported. Low dose CT has been shown to be a suitable method to implement in the pre- and postoperative investigation of young patients with scoliosis, where a significant dose reduction compared with standard CT did not convey any negative impact on image quality (17). According to Abul-Kasim et al. (18), low dose CT of the spine is a reliable method to assess the accuracy of pedicle screw placement in patients with adolescent idiopathic scoliosis. Low dose cervical spine CT in patients with blunt trauma has acceptable image quality compared with standard dose CT (19). According to Horger et al. (20), low dose whole-body CT, compared with plain radiography, in the staging and monitoring of multiple myeloma patients, is a precise and quick diagnostic tool.
Low dose CT is also well established in clinical practice in other regions. For example, the overall diagnostic accuracy of low dose CT for urolithiasis was calculated as 99.32% according to a systematic review by Niemann et al. (21). Screening for lung cancer using low dose CT reduces mortality by 20% (22). Low dose, dual-source CT coronary angiography in step-and-shoot mode allows, in patients with a regular heart rate, accurate diagnosis of significant coronary stenoses (23). Low dose CT colonography has excellent sensitivity for detection of colorectal carcinomas and polyps larger than 6 mm (24).
Magnetic resonance imaging (MRI) is a good method in spine imaging without ionizing radiation. It has been shown to be superior to radiography and CT in the diagnosis of bone marrow edema, medullary infiltration, and disc herniation. But MRI alone may not be sufficient for a complete understanding of the morphological changes of the skeletal structure, where radiography or CT can add information. Furthermore, the assessment of fracture risk in osteolytic lesions and instability has been proven superior with CT (25). MRI is also more costly and more time-consuming, there are some contraindications, and there may be limited availability. All these factors may influence the choice of imaging.
The protocol for low dose CT at 1 mSv level used in the current study was derived from a phantom study (10). The dose level was set as the average effective dose of lumbar spine radiography in Sweden, 1.1 mSv, according to a report from 2010 (26). Wall et al. reported 0.6 mSv as a typical effective dose in the UK using only two projections (27), but there were large variations between hospitals. Hart et al. reported DAP values from lumbar spine examinations indicating effective doses in the range of approximately 0.2–5 mSv (4). The calculations of effective dose are in general hampered by uncertainties and are calculated through multiple steps and depend on a number of approximations (28). In the current study, the differences in dose for different sizes of patients have been taken into account by using average values for each BMI category. However, one should be aware that the organ doses used in the calculations are valid for mathematical phantoms equal to a standard patient and should not be used for individual patients and deviations in the different BMI categories likely lead to different dose distributions and organ doses. The concept effective dose was never meant to be used for individual patients. Any discussion of effective dose must recognize that it is a broad, generic estimate of risk, and that differences of a few mSv do not imply any true differences in biologic risk (28–30). Rather risk should be described using broad categories: negligible, <0.1 mSv; minimal, 0.1–1 mSv; very low, 1–10 mSv; and low, 10–100 mSv (30,31). Thus, the methods evaluated in the current study belong to the same risk category, i.e. minimal. CT at the low dose set in the current study, about 1 mSv, has a high possibility to become part of the clinical routine in imaging the lumbar spine. The CT protocol can be further developed by adapting the settings of other parameters than reference mAs, tube potential (kV) and convolution filter, or by applying other reconstruction techniques such as iterative reconstructions (7,32).
The strengths of the current study are that five reviewers took part in this study providing a wide range of experience in evaluating image quality, and that the study included tests of intra-observer and inter-observer agreement and an evaluation of whether BMI was a confounder.
A limitation of the study was that the major part of the sample was referred from primary healthcare with a history of low back pain without any known serious underlying condition. The expectation of pathological findings was thus low compared with more advanced cases such as cases with trauma, known malignancy, or skeletal metastasis. Another limitation was the difficulties in comparing image quality of two different modalities. However, the purpose of the current study was to test the capability of the new method to demonstrate different anatomical structures compared with the standard method, radiography, as a minimum requirement of the diagnostic method. The fact that all observers were consistent in their assessments indicates that this comparison was working.
In conclusion, low dose CT of the lumbar spine at 1 mSv has superior image quality to lumbar spine radiography. Low dose CT may give more anatomical and diagnostic information than lumbar spine radiography and thus can replace it in daily clinical practice.
Footnotes
Acknowledgments
The authors wish to thank the staff of the Radiology Department at Örebro University Hospital, with special thanks to M Gustavsson, G Söder, and S Lager. Many thanks to A Magnuson for statistical consultations.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.