
Abstract
Background
Because peroneal tendons course from the lateral side of the proximal fibula through the posterior side of the distal fibula, correct diagnosis of the tendon pathology on an orthogonal sagittal plane can be difficult.
Purpose
To evaluate the diagnostic usefulness of oblique sagittal imaging (peroneal view) for evaluation of peroneal tendon pathology.
Material and Methods
This retrospective study included 69 patients at our institution who underwent routine ankle magnetic resonance imaging (MRI) using the peroneal view. Twenty-three patients underwent arthroscopy. Anatomic identification of the peroneal tendons on orthogonal sagittal MRI sequences and peroneal views were evaluated. Two radiologists evaluated the peroneal tendons based on an entire length view, an entire width view, and margin sharpness using a 4-point scale. Diagnostic accuracy using orthogonal sagittal and peroneal views was evaluated by calculating sensitivity, specificity, and accuracy. Arthroscopic or clinical findings were used as the reference standard.
Results
Total anatomical scores on the peroneal view were higher than those of the orthogonal sagittal views (P < 0.001). Both readers were able to identify anatomy of the tendon using the full length, full width and sharp margin, and determined that the peroneal view was better when compared with the orthogonal sagittal views (P < 0.001). Although the sensitivity and accuracy of the peroneal view in the diagnosis of peroneal tendon injury were slightly higher than orthogonal view, the values were not statistically significant.
Conclusion
Peroneal views provide better anatomic evaluation of the peroneal tendons itself, although cannot show significant superiority in the diagnostic performances.
Introduction
Peroneal tendon disorders including tenosynovitis and partial tearing are caused by trauma, overuse, and chronic inflammation (1). Magnetic resonance imaging (MRI) has been regarded as a useful diagnostic tool for peroneal tendon pathology prior to surgical intervention (2). However, because peroneal tendons course from the lateral side of the proximal fibula through the posterior side of the distal fibula (retromalleolar portion), correct diagnosis of the tendon pathology on an orthogonal sagittal plane can be difficult (2–4). Although the orthogonal sagittal view can sometimes reveal increased signal intensity along the longitudinal axis of the tendon, this signal intensity is difficult to characterize in some cases and can be confused by artifactual signals that result from the inability to image along the true course of the tendon or from partial volume artifacts (5). Several studies have shown that an additional oblique view can be a helpful imaging plane to diagnose ligament pathology, especially when evaluating the anterior cruciate ligament (6–9). Our study worked to determine the diagnostic efficacy of an additional oblique sagittal view that was parallel to the real course of peroneal tendons at the distal fibular level (retromalleolar portion). The purpose of this study was to evaluate the diagnostic usefulness of oblique sagittal imaging (peroneal view) which connects lateral border of posterior portion of calcaneus and peroneal tubercle for evaluation of peroneal tendon pathology, especially in the retromalleolar portion.
Material and Methods
Case selection
The study was approved by the institutional ethics review board (IRB) of our hospital, and the requirement for informed consent was waived due to the retrospective study design. We retrospectively evaluated 69 consecutive patients who had visited our hospital for ankle pain and that had undergone ankle MRI with an additional peroneal view between September 2011 and July 2013. The MRI examination of the patients was conducted to evaluate ankle pain and impaired mobility. All patients had pain and tenderness on the posterolateral portion of the ankle for at least 1 month. The sample included 48 (70%) men and 21 (30%) women (mean age, 38.8 ± 17.8 years; age range, 6–82 years). Two children aged less than 10 years were included in the study. Nine patients were diagnosed with peroneal tendinosis, eight patients were diagnosed with a synovitis, and one individual had a split tendon. The exclusion criteria were fracture (two cases) and postsurgical state (two cases). One surgeon, who had completed fellowship training in ankle repair and had 10 years of surgical experience, performed all surgical procedures, and clinically diagnosed each patient. The surgeon explored the tendons if the tendon had split or a tear existed, measured the size of the tendon, and ascertained fluid collection in the tendon sheath. If the tendon was swollen to 50% greater than the normal proximal portion of the tendon or the other peroneal tendon or discoloration with loss of normal striation was seen, the surgical diagnosis was tendinosis. Twenty-three patients (33%) underwent surgical interventions and 46 patients (67%) were diagnosed both clinically and radiologically. The mean interval between MRI and arthroscopy was 8.4 days (range, 1–30 days). No ancillary treatment, such as non-steroidal anti-inflammatory drugs (NSAIDs) or physical therapy, was provided during this interval. Once the radiologists had conducted blind reading of the MR images, the surgeon and radiologists correlated the surgical, clinical, and imaging findings. The final diagnosis was based on clinical manifestation, physical examination, and MR findings (other MR sequences containing axial views) by a consensus between two radiologists and a clinician. Positive symptoms and physical examinations of peroneal tendon injuries revealed retromalleolar pain, swelling, and tenderness along the course of the peroneal tendon (5,7).
MRI parameters
Parameters for MRI sequences.
FS, fat saturation; FSE, fast spin-echo; PD, proton density.
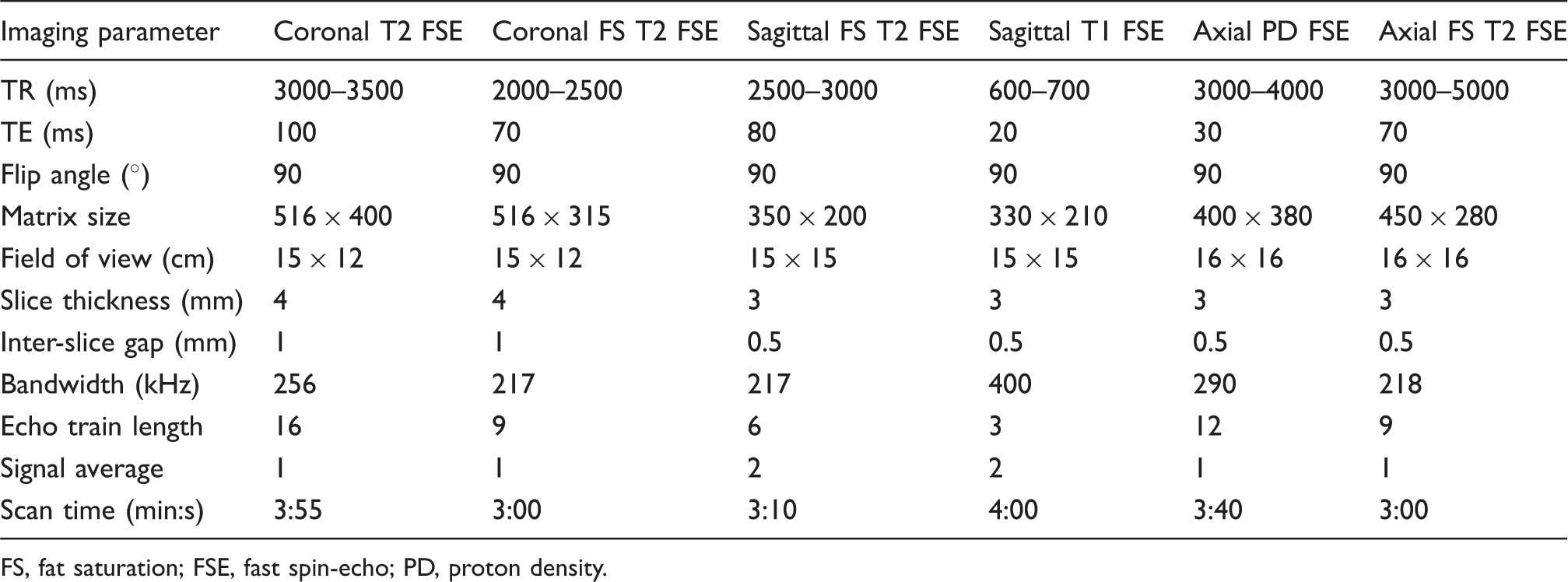
An axial T2W image demonstrating the technique to obtain an oblique sagittal view of the peroneal tendons (peroneal view). Peroneal views were obtained using 2 mm slice thickness in the plane parallel to the line between the lateral border of the posterior portion of the calcaneus and lateral margin of the peroneal tubercle based on axial T2W image at the mid-calcaneal level, indicated by prominent bony proturberance.
Image analysis
Orthogonal sagittal T1-weighted and fat-suppressed T2W MR images (orthogonal sagittal views) and peroneal views were interpreted separately by two fellowship-trained musculoskeletal radiologists with 12 and 8 years of experience, respectively, who were blinded to clinical information and radiologic reports. Anatomic identification of the peroneus brevis and peroneus longus tendon on orthogonal sagittal views and peroneal views was performed according to the reader’s discretion throughout the entire length (full length), the entire width (full width), and margin sharpness according to a 4-point scale (0, poor; 1, fair; 2, good; 3, excellent). The readers first evaluated only the orthogonal sagittal views and during sessions that were spaced 1 or 2 weeks apart, the image readers evaluated the peroneal view. For evaluation of the full length of tendon, a score of 3 indicates that the evaluation was able to assess more than 75% of the entire length of tendon from the myotendinous junction to the metatarsal insertion of the peroneus brevis tendon on a single slice image. A score of 2 indicates that 50–75% of the length was assessed, a score of 1 indicates that 25–50% of the length was assessed, and a score of 0 indicates less than 25% of the length was assessed. In the full-width evaluation section, a score of 3 indicates the ability to evaluate more than 75% of the width of both tendons from the upper to the lower margin of each tendon. A score of 2 indicates an evaluation range of 50–75%, a score of 1 25–50%, and a score of 0 less than 25%. In the sharp margin evaluation section, a score of 3 indicates excellent differentiation of the tendon from the adjacent soft tissue. A score of 2 indicates good differentiation, a score of 1 indicates fair differentiation, and a score of 0 indicates poor differentiation. Diagnostic assessment of the orthogonal sagittal views and peroneal view were also independently evaluated. The peroneus tendon (brevis or longus) was considered intact if continuous low signal intensity was observed along the entire tendon (10) (Fig. 2). The tendon was considered to have tendinosis if there was a focal or diffuse high signal intensity within the tendon (Fig. 3). Synovitis was considered when abnormal fluid collection was seen in the peroneal tendon sheath. Significant fluid collection was defined as the presence of circumferential fluid within the common peroneal tendon sheath with a maximal width greater than 3 mm (11). If the tendon showed clefts and defects that extended into the substance of the tendon itself, a tendon split was diagnosed (12).
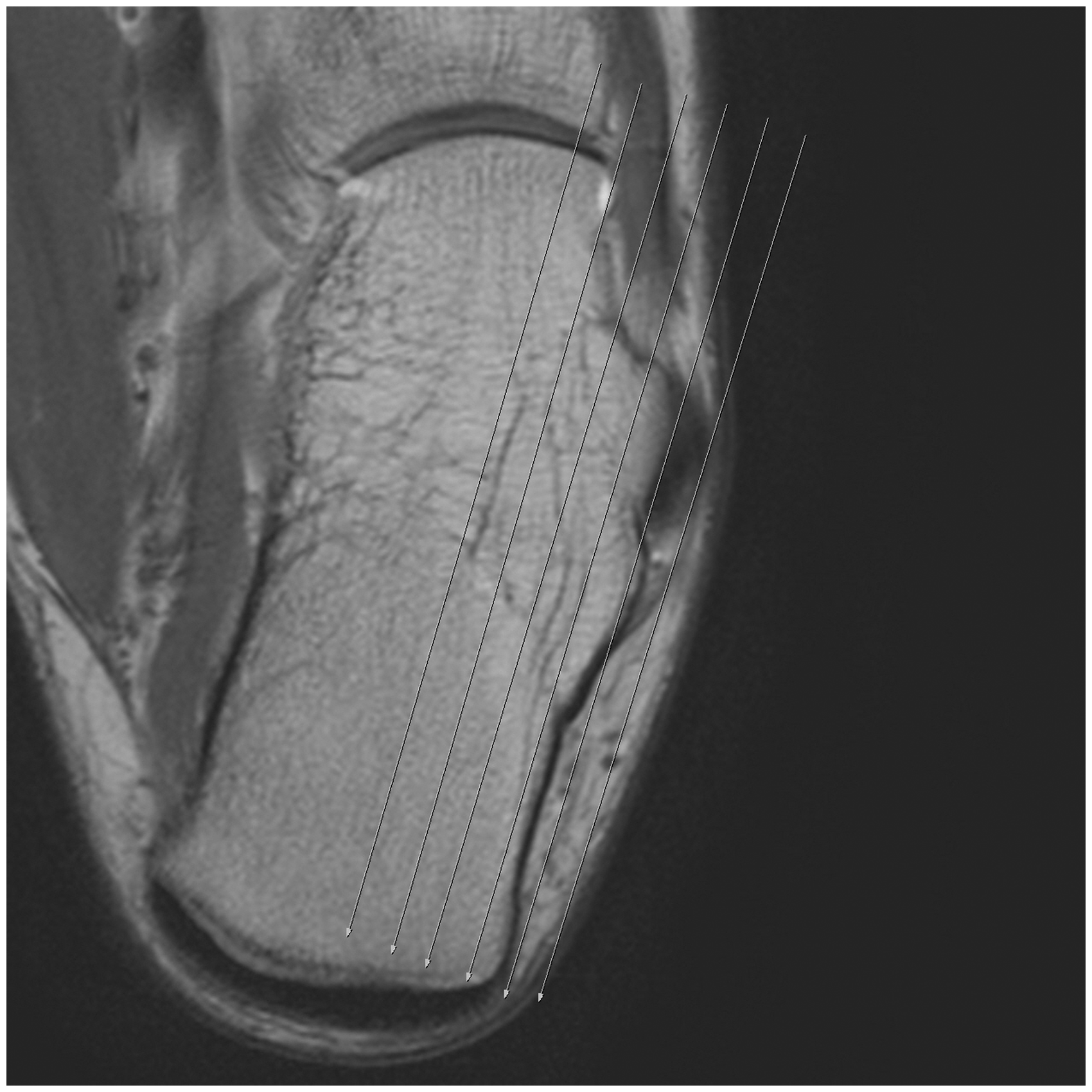
Normal peroneus longus. (a) Sagittal fat-saturated T2W MR image (TR/TE, 3000/80) shows poor delineation of the tendon in width. The entire course of the tendon does not appear on a slice (arrow). The total anatomic identification score was 6. (b) Peroneal view (TR/TE, 2000/60) that shows the sharp margin and almost the entire contour of the tendon (arrow). The total anatomic identification score was 9. A 25-year-old man with ankle pain for 6 months. (a) Sagittal fat-saturated T2W MR image (TR/TE, 2500/80) of the peroneus longus showing poor demarcation of the tendon (arrow). The diagnosis was an intact peroneus longus. (b) Peroneal view (TR/TE, 2000/60) revealed the entire course of the peroneus brevis and a prominent bright signal in the tendon at the distal portion (arrow). The diagnosis was tendinitis, which was confirmed upon surgery.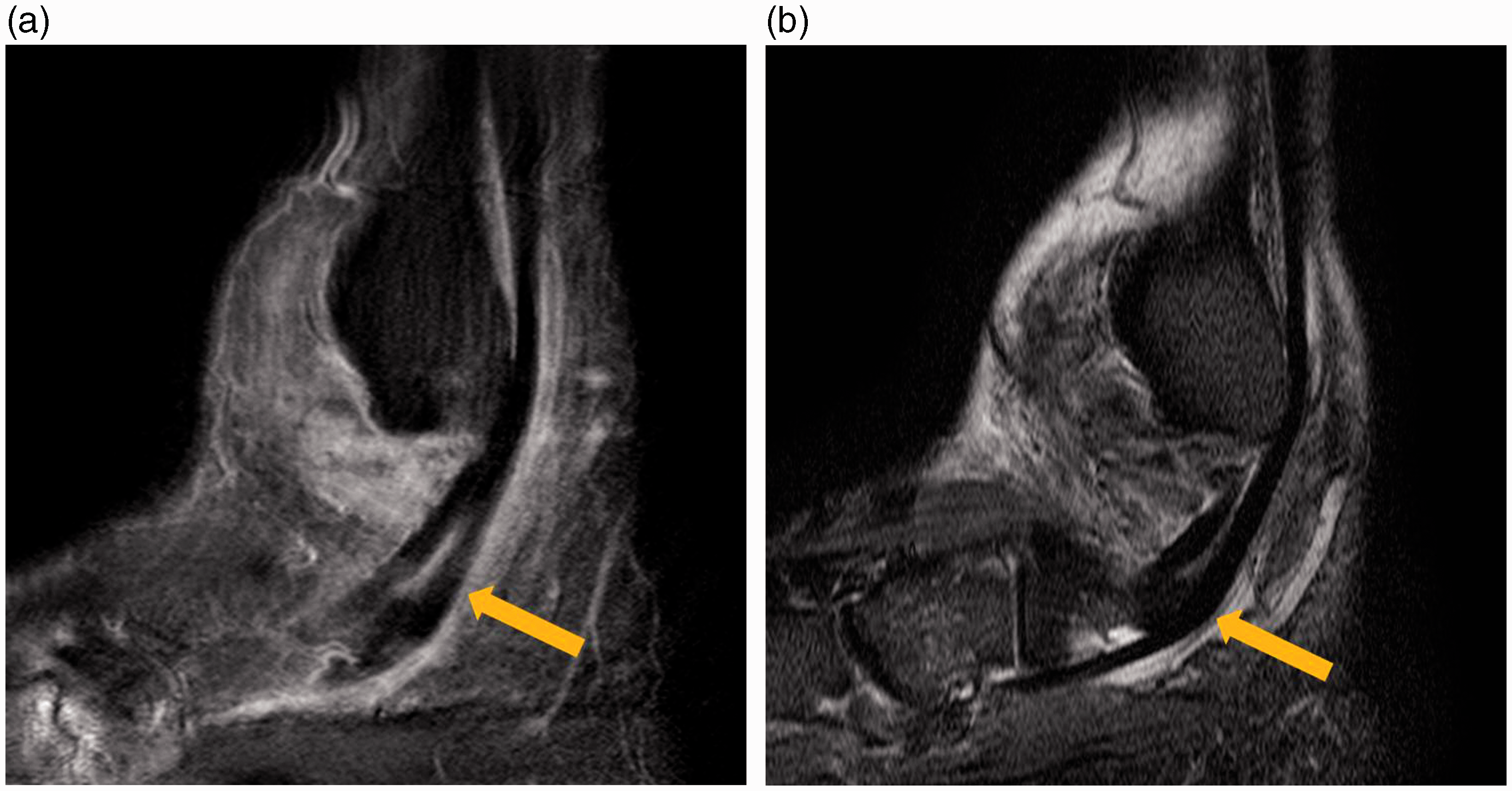
Statistical analysis
Anatomic identification on peroneal view and orthogonal sagittal views, as graded by the two radiologists, were compared. Inter-observer agreement between the readers was analyzed using an intra-class correlation coefficient (ICC) because the values were continuous variables. ICC values less than 0.40 were indicative of poor agreement, while ICC values in the range of 0.40–0.75 indicated fair-to-good agreement. ICC values which were greater than 0.75 indicated excellent agreement (13).Wilcoxon signed-rank tests were used to determine statistical significance of the anatomic identification score. With kappa statistics, we analyzed inter-observer agreement of diagnostic performance. The kappa value interpretation was as follows: poor (k < 0.1), slight (0.1 ≤ k ≤ 0.2), fair (0.2 < k ≤ 0.4), moderate (0.4 < k ≤ 0.6), substantial (0.6 < k ≤ 0.8), and nearly perfect (0.8 < k ≤ 1) (14). Diagnostic performance was evaluated using the sensitivity, specificity, and accuracy of peroneal tendon tear diagnosis as determined by the use of the peroneal and orthogonal sagittal views. The arthroscopic or clinical findings were used as the reference standard. The values of sensitivity, specificity, and accuracy were statistically analyzed using the McNemar test. Statistical analyses were performed using PASW software version 18.0 (IBM, Armonk, NY, USA), and P values ≤0.05 were considered to be statistically significant.
Results
Mean scores for anatomic peroneus tendon identification.
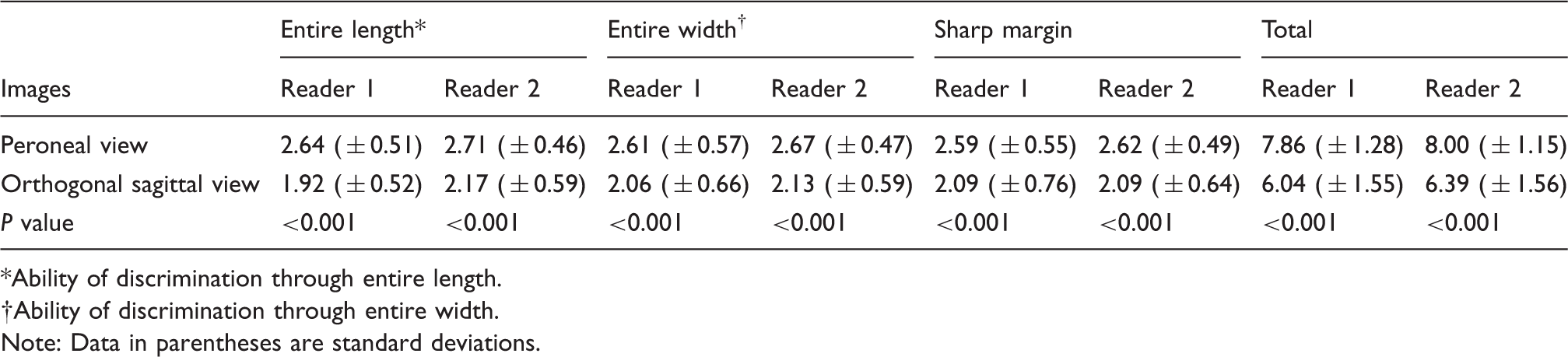
Ability of discrimination through entire length.
Ability of discrimination through entire width.
Note: Data in parentheses are standard deviations.
Intra-class correlation coefficients of anatomic identification scores between readers.

Ability of discrimination through entire length.
Ability of discrimination through entire width.
Data: Numbers in parentheses are 95% confidence intervals.
Sensitivity, specificity, and accuracy of the peroneal view and orthogonal view in diagnosing peroneal tendon injuries (%).
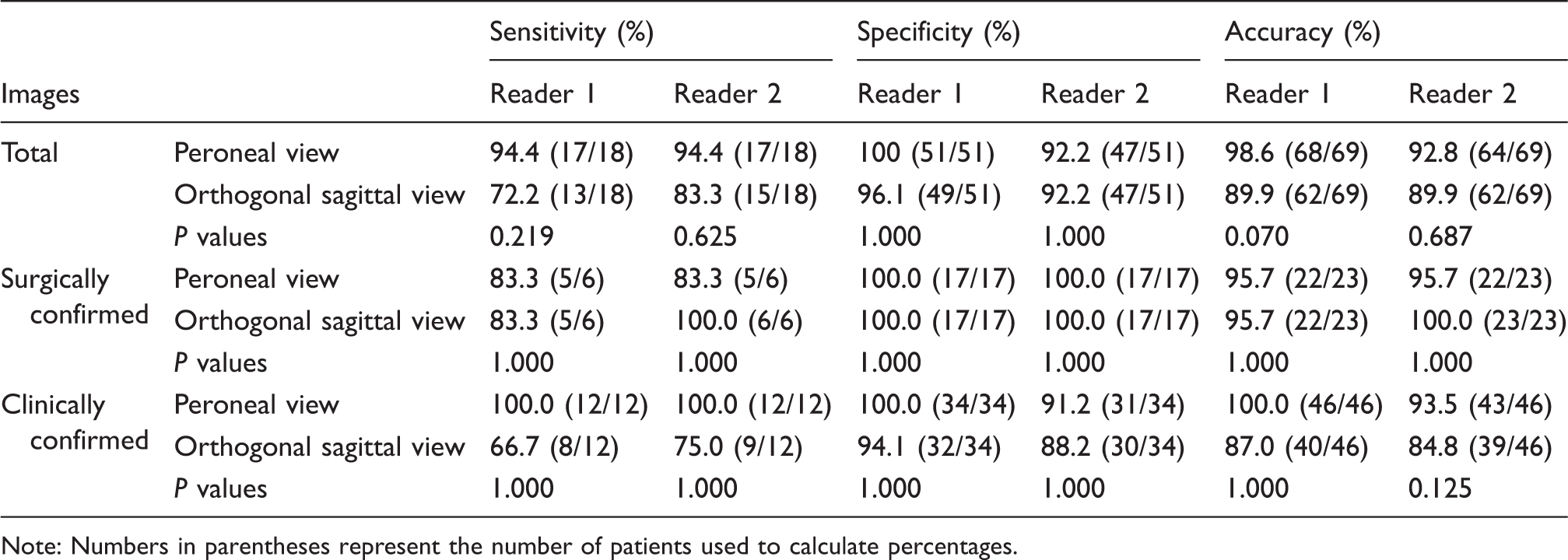
Note: Numbers in parentheses represent the number of patients used to calculate percentages.
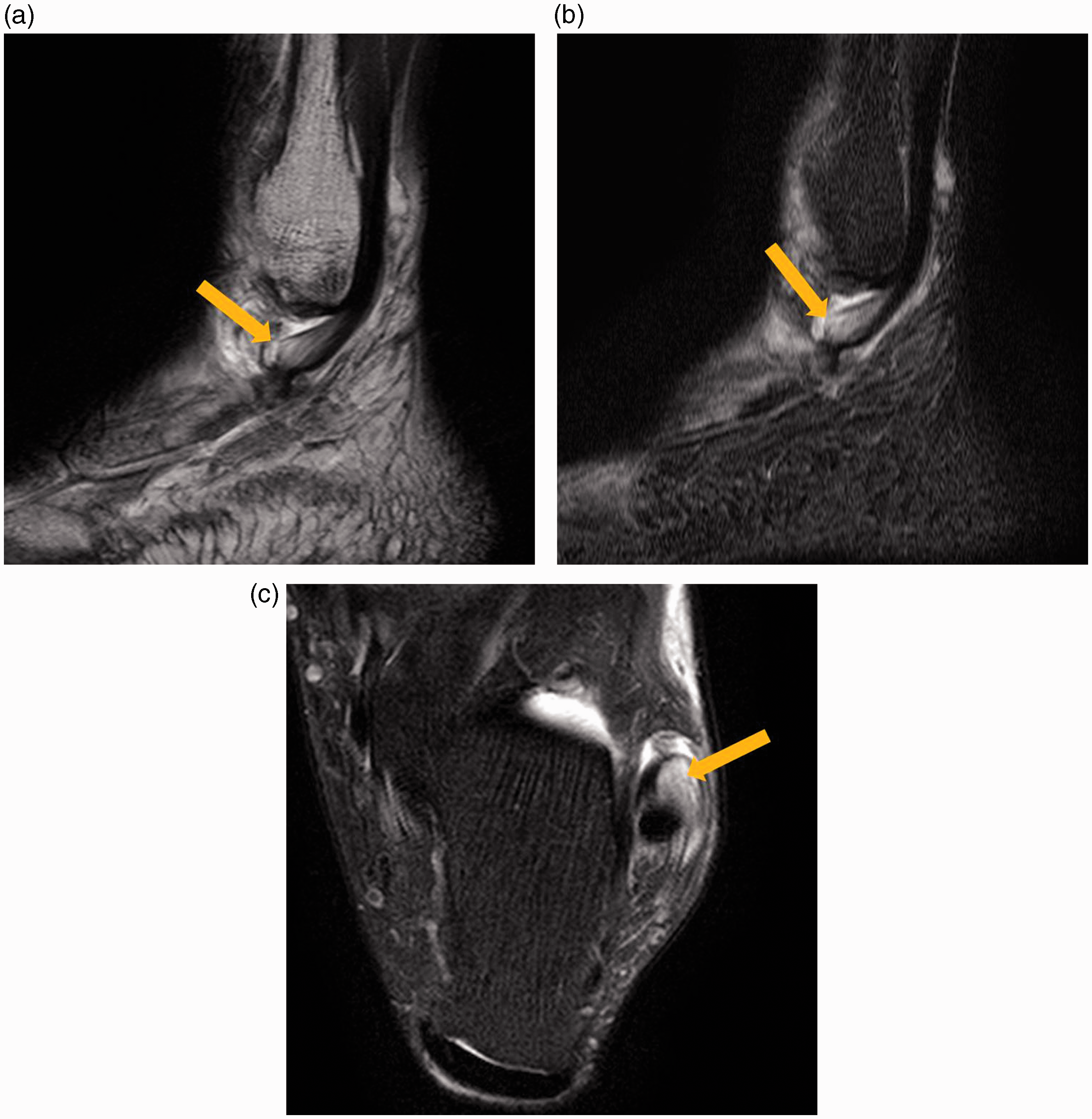
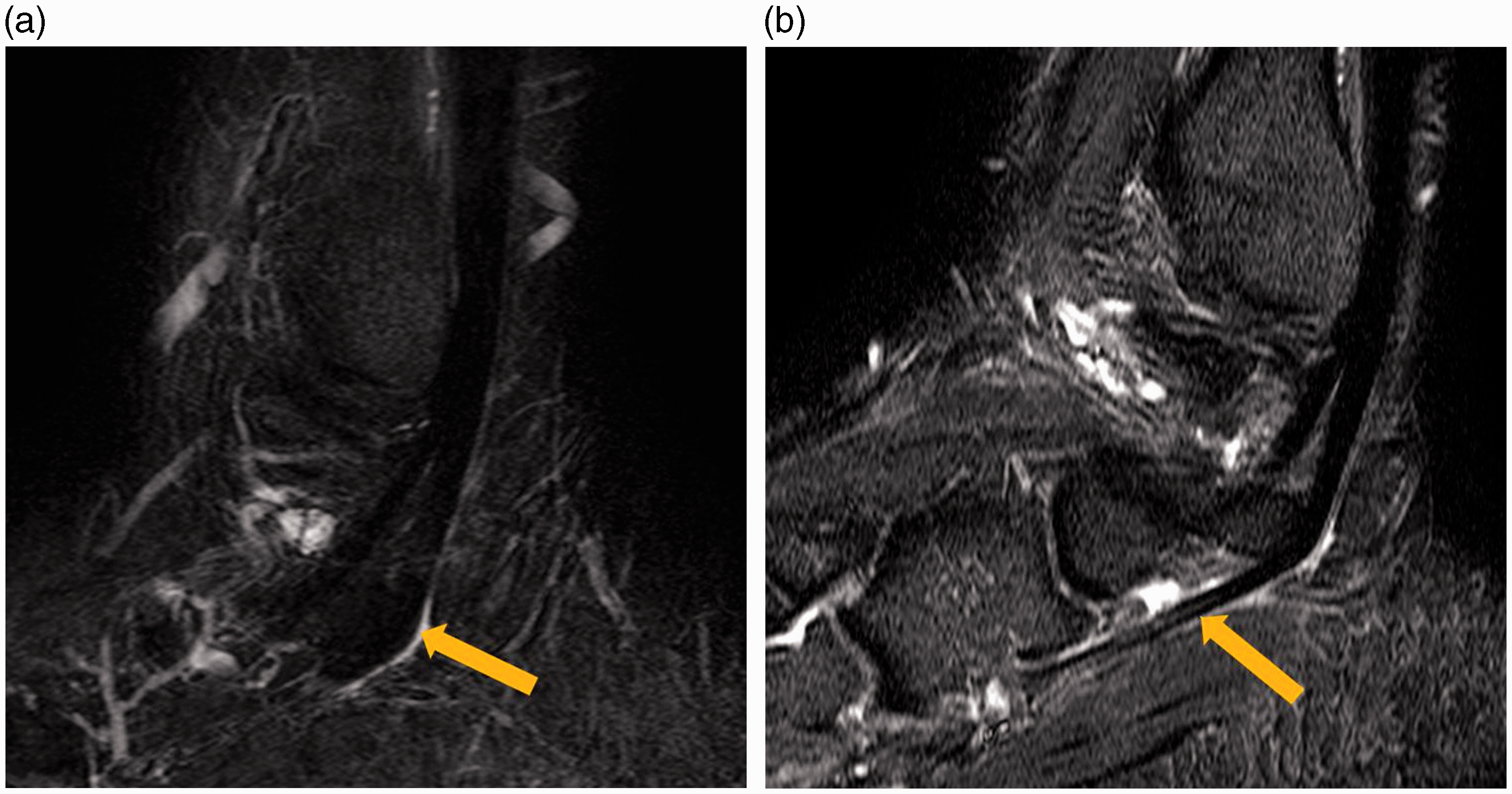
A 52-year-old woman with ankle pain for 1 month. (a) Sagittal T2W MR image (TR/TE, 3800/80) reveals prominent tendon disruption (arrow). (b) Peroneal view (TR/TE, 2000/60) also revealed tendon split (arrow). The diagnosis was a peroneus brevis tendon split, which was confirmed upon surgery. (c) Axial fat-saturated T2W MR image (TR/TE, 3200/70) shows splitting of the peroneus brevis tendon (arrow).
Discussion
Because the peroneal tendons run on an oblique course, pathological diagnoses of tendon injuries can be difficult (2). The oblique course of the peroneal tendons does not permit sufficient evaluation in the orthogonal planes; thus, oblique imaging is recommended. The usefulness of oblique sagittal images in the evaluation of the other anatomic structures such as the anterior cruciate ligament has already been established (5). Studies have reported that signal changes, continuity, and contour can be seen more easily on oblique views (6).We expected that the peroneal view would allow similar evaluation of peroneal tendon pathology. This study used an anatomic identification scoring system that showed fair-to-good inter-observer agreement. The peroneal view was superior to the orthogonal sagittal view with regard to full width, full length, and margin sharpness (Table 2) for anatomically identifying peroneal tendon. Therefore, the peroneal view may be superior to the orthogonal views because it allows better tendon visualization. A previous study of the orthogonal MR images reported 84% sensitivity, 75% specificity, and 78% accuracy for diagnosing peroneal tendinopathy (2).Our study showed somewhat different results. The sensitivity of the orthogonal sagittal views was in the range of 72–83%, specificity was in the range of 92–96%, and accuracy was 90%. The difference in our results and the results from the previous studies might be due to differences in the strength of the magnet of the MRI machine. We used a 3.0-T MR scanner in this study, while Park et al. acquired images using a 1.5-T MR scanner (2). The diagnostic performance of the peroneal view was excellent (>92%), although the diagnostic performance of the orthogonal sagittal view was not bad (>72%). This result suggests that if we add a peroneal view to routine MR images, we can improve the sensitivity of equivocal case diagnoses. Actually, four cases of peroneal tendinitis were detected by reader 1 and two cases were detected by reader 2, but only with the peroneal view, and this diagnosis was not apparent on the orthogonal sagittal images. However, the results were not statistically significant. An operating surgeon and surgical team could acquire more useful information to establish a treatment plan from the radiologic report. Although we were unable to directly determine that the peroneal views improved the ability to diagnose peroneal tendon injury in general, this assessment could be very helpful in cases of diagnostic uncertainty.
Our study had some limitations. First, our study involved subjective analysis of the anatomic identification of peroneal tendons. We also used a scoring system that depended on the subjective opinion of a radiologist; nevertheless, the inter-observer agreement of the scores was high, which indicates that the scores were fairly reproducible. Second, our study lacked surgical confirmation of all peroneal tendon injuries. Only six of the 18 patients with peroneal tendon abnormalities needed surgical correction. Consequently, the results were based on a small number of surgically confirmed cases. Only 33% of all cases in this study underwent surgical procedures. However, we took great care to achieve the optimal possible standard of reference in the non-surgical cases using clinical and other MRI findings. Third, we could not blind the evaluators to the imaging technique because the peroneal views show slightly different anatomic plane. This awareness of the image nature might have influenced the results. Fourth, the peroneal views were obtained with a lower slice thickness (2 mm) and with a longer echo train length. These differences in parameter might contribute to make bias.
In conclusion, peroneal views provide better anatomic evaluation of the peroneal tendons itself, although cannot show significant superiority in the diagnostic performances. Peroneal views can be applied as a useful method for distinguishing equivocal cases of possible peroneal tendon injury, especially in the retromalleolar portion.
Footnotes
Acknowledgements
We represent special thanks to Da Hyun Park (Sookmyung Girl's high school, Seoul, South Korea) for manuscript correction.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.