
Abstract
Background
The physiological uptake of 18F-fluorodeoxyglucose (FDG) in the heart often interferes with the accurate diagnosis of inflammatory cardiac diseases (CDs). Unfractionated heparin (UFH) administration may suppress its uptake through the alteration of myocardial metabolism.
Purpose
To clarify the effectiveness of UFH administration to suppress the physiological FDG uptake in the heart.
Material and Methods
The physiological FDG uptake in the heart was compared among 178 patients who fasted less than 18 h, 37 patients who fasted more than 18 h, and 64 patients who fasted more than 18 h and were administered UFH (UFH-CD group) prior to FDG PET/CT. Free fatty acid (FFA), triglyceride, insulin, and blood glucose levels were measured after UFH administration. Myocardial FDG uptake was evaluated by visual assessment and on the basis of maximum standardized uptake value (SUVmax).
Results
In the UFH-CD group, the FFA level increased 15 min after UFH administration (P < 0.01). Blood glucose and insulin levels remained unchanged (P = NS). FDG physiological uptake was observed in 69% of the patients who fasted less than 18 h, 38% of the patients fasted more than 18 h, and 22% of the UFH-CD group (P < 0.01 for trend). SUVmax decreased in the UFH-CD group compared with the patients who fasted less than 18 h (P < 0.01) and the patients who fasted more than 18 h (P = 0.029).
Conclusion
UFH administration and fasting more than 18 h could effectively suppress FDG physiological uptake in the heart and can be a useful method of detecting inflammatory CDs and tumors.
Introduction
Positron emission tomography (PET) is significantly useful for the evaluation of inflammatory cardiac diseases (CDs) and tumors (1). 18F-fluorodeoxyglucose (FDG) is a useful tracer for detecting the presence of inflammatory CDs and tumors and determining the magnitude of disease activity. However, the physiological FDG uptake throughout the heart or in certain regions can make it difficult to evaluate the pathological FDG uptake in the heart. The prevalence of this non-pathological glucose uptake is observed in up to 68% of patients who have no CDs (2).
To reduce physiological FDG uptake in the heart, several methods have been used to shift cardiac metabolism from glucose to free fatty acids (FFA). A low-carbohydrate diet or a combination of a low-carbohydrate diet and a high-fat diet is widely used (3,4). Administration of unfractionated heparin (UFH) may be another effective method of reducing physiological FDG uptake associated with an increase in plasma FFA level (5–7). However, the effect of UFH on myocardial glucose metabolism has not been fully investigated.
We hypothesized that UFH could effectively suppress glucose metabolism in remote regions in patients with inflammatory CDs. The aim of this study was to clarify the clinical utility of UFH for the suppression of physiological FDG uptake in the myocardium.
Material and Methods
Study patients
We retrospectively enrolled consecutive patients who underwent FDG PET/CT between December 2008 and March 2013 and divided them into a group of non-CD patients (n = 300) and a group with suspected CDs and had UFH administration (UFH-CD group, n = 64). This study was approved by the institutional review board of Hokkaido University Hospital.
Patients with non-CDs were further divided into the long-fasting group (fasting more than 18 h) and the short-fasting group (fasting less than 18 h) (8). We excluded patients who: (i) were <20 years old; (ii) had blood glucose levels >150 mg/dl before FDG administration; (iii) showed abnormal findings in electrocardiography or chest X-ray examinations; (iv) were previously diagnosed as having CD; and (v) had an intrathoracic tumor or any metastatic lesion near the heart. Abnormal findings in electrocardiography included bradycardia (<50 beats per minute [bpm]), tachycardia (≥100 bpm), atrioventricular block, left bundle branch block, atrial fibrillation, and any ST change. Abnormal findings in chest X-ray examination included cardiomegaly (chest-thoracic ratio >50%) and pleural effusion. All patients were required to fill out an interview sheet that asked about the duration of fasting, past medical history, and drug allergies.
Patients in the UFH-CD group were instructed to fast for at least 18 h before FDG injection (8). We excluded patients who (i) were <20 years old; and (ii) had blood glucose higher than 150 mg/dl before FDG administration. We reviewed the medical reports of these patients for their medical history, findings in physical examination, electrocardiography, and coronary angiography, and history of other non-invasive cardiovascular interventions.
FDG PET/CT
All PET/CT images were obtained using a 64-slice PET/CT scanner (Biograph 64 TruePoint with TrueV, Siemens, Tokyo, Japan). A computed tomography (CT) scan in PET/CT was performed for attenuation correction. PET scanning was performed 45–60 min after FDG administration.
Administration of UFH and blood biochemical analysis
UFH (Mochida Pharmaceutical Co. Ltd., Tokyo, Japan) was administrated 15 min before FDG administration in the UFH-CD group. The indication for UFH administration was decided before PET/CT study when the patient was suspected of having an inflammatory cardiac involvement. Blood samples were drawn immediately before, 15 min after, and 30 min after UFH administration at 50 units/kg body weight via intravenous infusion. Blood sample were drawn in the UFH-CD group for measurements including FFA levels, triglyceride levels, immunoreactive insulin levels (IRI), blood glucose levels, and activated partial thromboplastin time (APTT). Written informed consent was obtained from all the patients in the UFH-CD group.
Myocardial FDG uptake
FDG uptake in the myocardium was measured by visual analysis and on the basis of standardized uptake value (SUV). SUVmax in the myocardium was measured in a three-dimensional region of interest drawn on the LV wall. SUVmax was used to evaluate myocardial FDG uptake because it can delineate the disease activity with higher sensitivity (9,10).
In the UFH-CD group, the FDG uptake in the heart was evaluated independently by two nuclear medicine physicians. They were blind to the patients’ clinical information and other imaging data. Myocardial FDG uptake was assessed by referring to findings in myocardial perfusion imaging (MPI), late gadolinium enhancement cardiac magnetic resonance imaging (LGE-CMRI), and follow-up PET/CT scan. MPI and LGE-CMRI were carried out within 3 months before and after the initial FDG PET/CT scan. Pathological uptake was defined as positive when FDG uptake was observed in the perfusion defect region in MPI or in the LGE-positive region in CMRI. When the region had previously known ischemia, FDG uptake in this region was also defined as pathological. When such information was not available, the FDG uptake was described as undefinable. SUVmax was also measured in the regions that we established as physiological.
Statistical analysis
Continuous variables are expressed as mean values and standard deviations or median and interquartile range (IQR), whereas categorical variables are expressed as numbers and percentages. Comparisons of continuous variables were subjected to the Wilcoxon rank sum test. Comparisons of categorical variables were subjected to the chi-square test. The Cochran-Armitage trend test was performed for comparison among groups in the visual analysis of FDG physiological uptake. The Kruskal-Wallis test was performed for comparisons of more than three groups. In multiple comparisons, P values were adjusted by the Holm method. Multivariate logistic regression analysis was performed to estimate the risk of physiological FDG uptake. Variables included in the models were selected on the basis of baseline characteristics (age, sex, BMI, fasting blood glucose levels, UFH administration, and fasting time [binomial categories; ≥18 h or <18 h]). The variance inflation factor was used to check for multicollinearity. For all analyses, P values less than 0.05 were considered statistically significant. All statistical analyses were conducted using R version 3.0.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Patient characteristics.

P < 0.05 compared with short-fasting group.
P < 0.01 compared with short- and long-fasting groups.
FDG, 18F-fluorodeoxyglucose; UFH, unfractionated heparin; UFH-CD, unfractionated heparin with suspected cardiac disease.

Flow chart of study patients.
Effects of UFH on blood biochemical factors
Of the 64 patients enrolled in the UFH-CD group, patients who lacked blood biochemical serial data were excluded from analysis. Thirteen patients were excluded owing to lack of FFA, blood glucose levels, and IRI levels, 14 patients owing to lack of triglyceride levels, and 19 patients owing to lack of APTT. The plasma FFA level was highest 15 min after UFH administration (P < 0.01) (Fig. 2). Triglyceride levels decreased from baseline 15 and 30 min after UFH administration (P < 0.01). UFH did not affect blood glucose or IRI levels. APTT increased after UFH administration as expected. None of the patients experienced any adverse events such as hemorrhage or heparin-induced thrombocytopenia.
Biochemical changes before and after administration of unfractionated heparin. Serial changes in free fatty acid (n = 51), triglyceride (n = 50), blood glucose (n = 51), and IRI (n = 51) levels and activated partial thromboplastin time (APTT; n = 45) are shown. *P < 0.01 compared with baseline.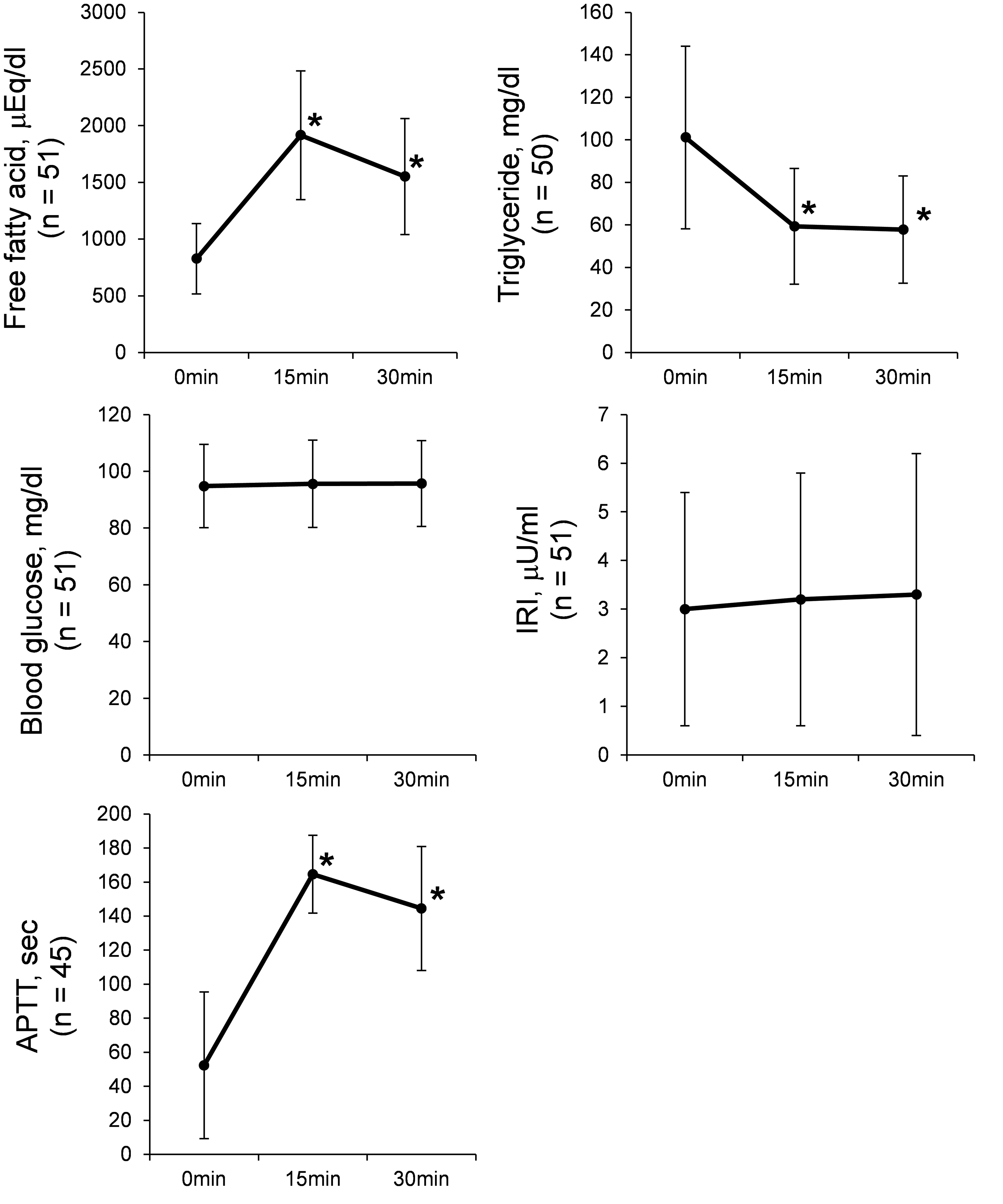
Physiological FDG uptake in myocardium
The prevalence of FDG uptake was significantly different among the three groups (P < 0.01) (Fig. 3). The prevalence of positive physiological uptake was lowest in the UFH-CD group (P < 0.01 for trend). Four patients (6%) in the UFH-CD group showed borderline findings. The prevalences of pathological and physiological FDG uptakes in patients who underwent other examination modalities are shown in Table 2. In the short-fasting and long-fasting groups, physiological uptake was more frequent in the basal region (60%) than in the mid and apical regions (42% and 39%, respectively, P < 0.001). LVEF was not significantly different between patients with physiological uptake and those without it (42.5 ± 14.0% vs. 45.8 ± 19.9%, P = 0.50).
Physiological uptake of FDG in myocardium. The rate of negative physiological uptake is shown by a black bar, positive uptake by a white bar, and undefinable uptake by a gray bar. UFH-CD, unfractionated heparin with suspected cardiac disease. Prevalences of pathological and physiological FDG uptakes in UFH-CD group. FDG, 18F-fluorodeoxyglucose; LGE-CMRI, late gadolinium enhancement cardiac magnetic resonance imaging; MPI, myocardial perfusion imaging; PET/CT, positron emission tomography/computed tomography; UFH-CD, unfractionated heparin with suspected cardiac disease.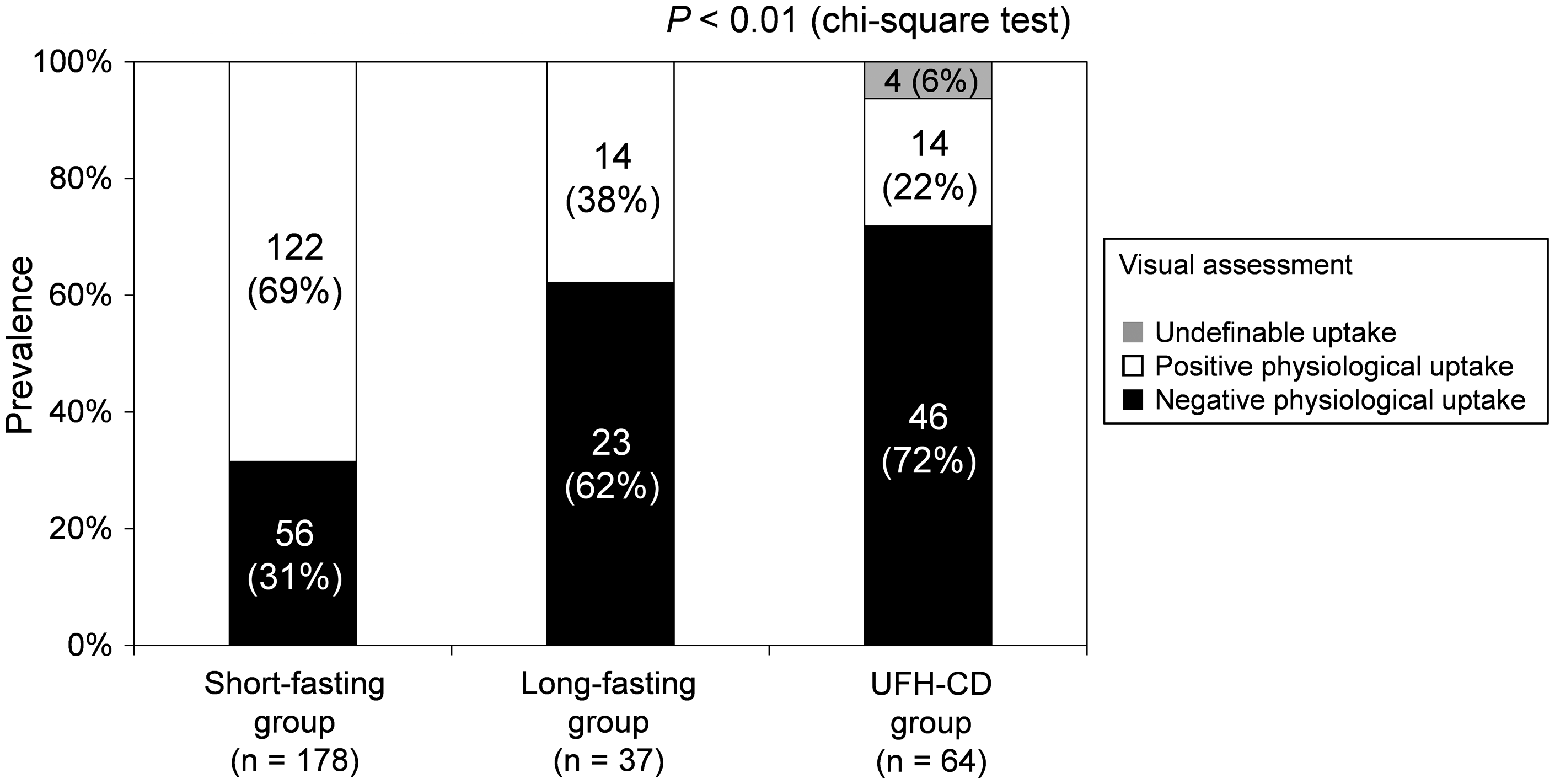

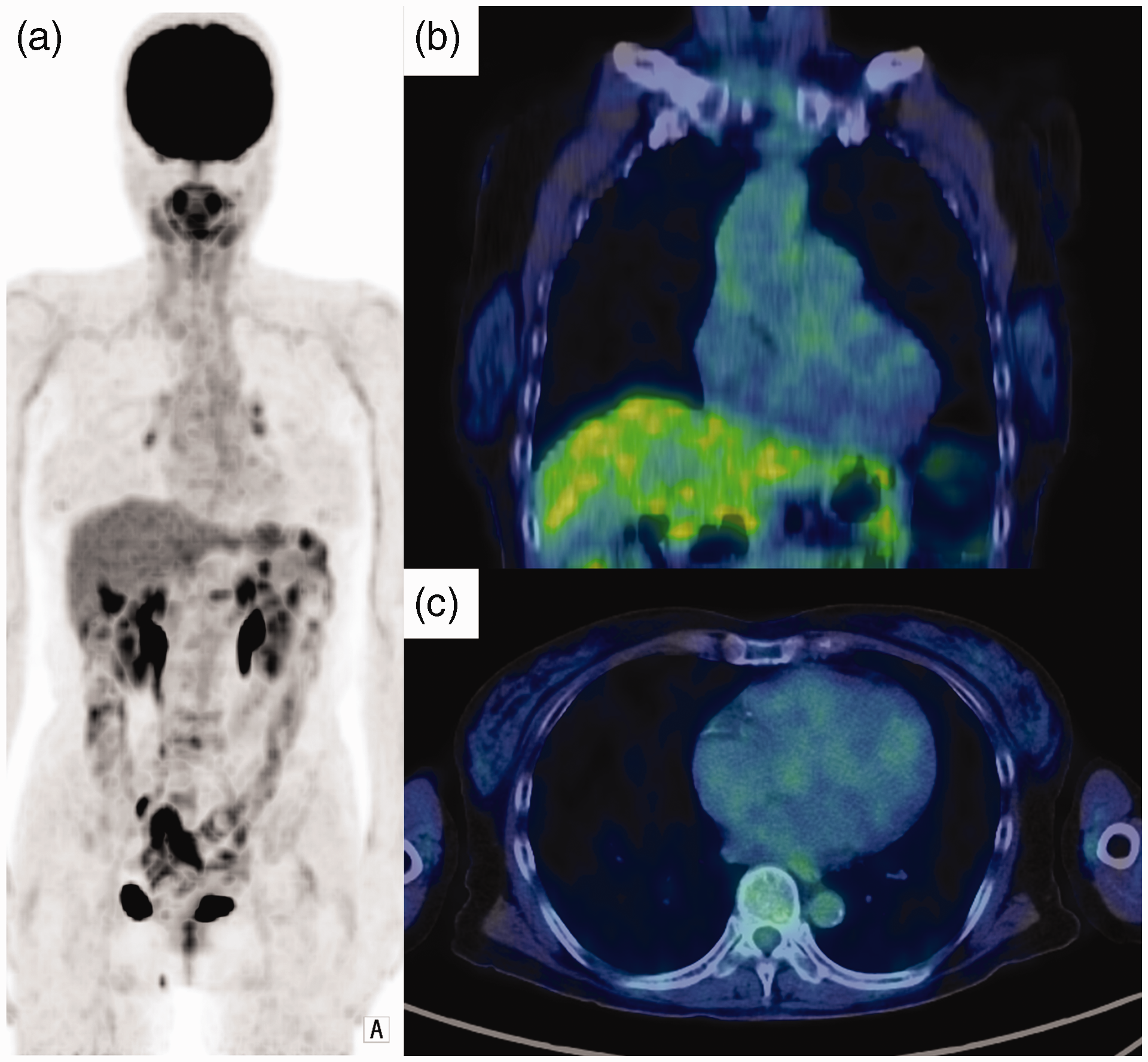
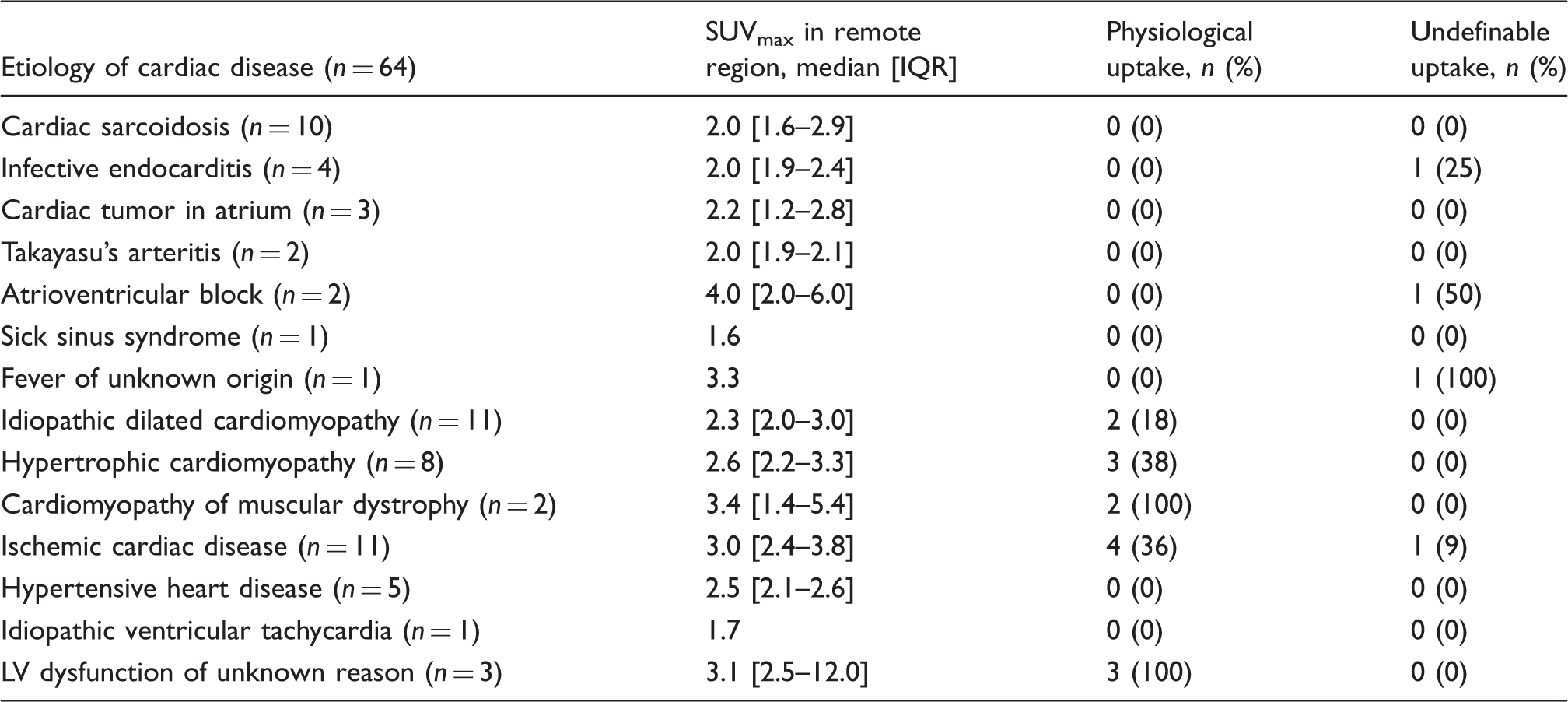
SUVmax was 4.2 (interquartile range [IQR], 2.7–8.1) in the short-fasting group, 2.7 (IQR, 2.3–3.7) in the long-fasting group, and 2.4 (IQR, 1.9–3.2) in the UFH-CD group (Fig. 4). The prevalence of physiological FDG uptake varied among CDs (Table 3). SUVmax was the lowest in the UFH-CD group (P < 0.01 vs. short-fasting group and P = 0.029 vs. long-fasting group). The SUVmax in the LV blood pool was 2.2 (IQR, 1.8–2.6) and did not correlate with either FFA levels or insulin resistance. A representative case in which UFH administration sufficiently suppressed myocardial FDG uptake is shown in Fig. 5.
Maximal standardized uptake values in myocardium (SUVmax) in short-fasting, long-fasting, and UFH-CD groups. UFH-CD, unfractionated heparin with suspected cardiac disease. Case presentation. A 64-year-old woman was diagnosed as having inactive-phase Takayasu’s arteritis. She fasted more than 18 h and was administrated UFH (50 units/kg body weight via intravenous infusion) 15 min before FDG administration. The physiological FDG uptake in the heart was sufficiently suppressed and the entire left ventricular SUVmax was 1.38. The free fatty acid level increased (from 658 μEq/dl at baseline to 1782 μEq/dl 15 min after) whereas the triglyceride level decreased significantly (from 125 mg/dl at baseline to 87 mg/dl 15 min after). On the other hand, changes in blood glucose and IRI levels were not statistically significantly different. (a) Frontal view of coronal maximum intensity projection. PET/CT fusion images in coronal (b) and axial (c) views. SUVmax in remote region and prevalence of FDG uptake in UFH-CD group.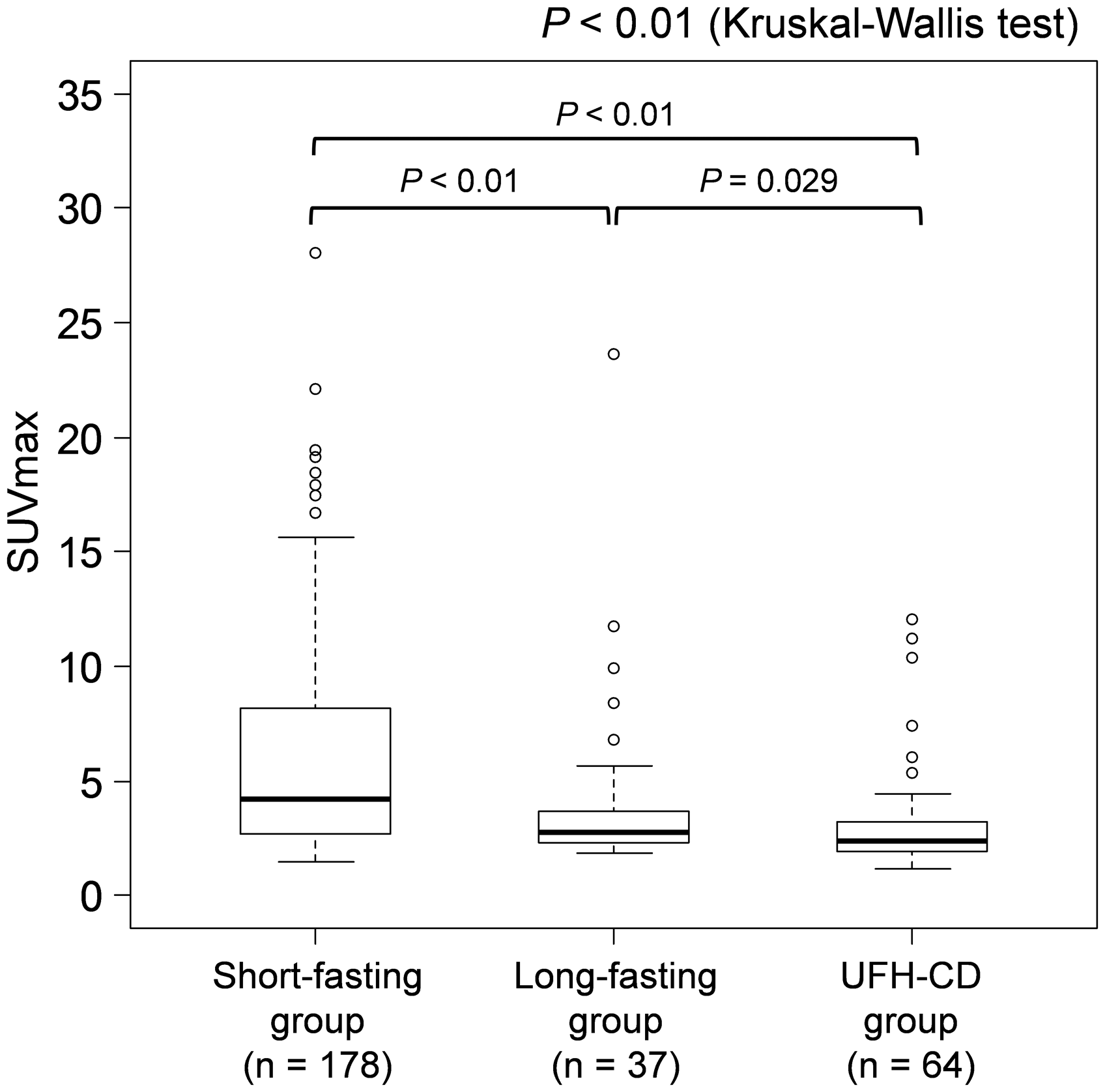
Predictors of physiological FDG uptake in heart.
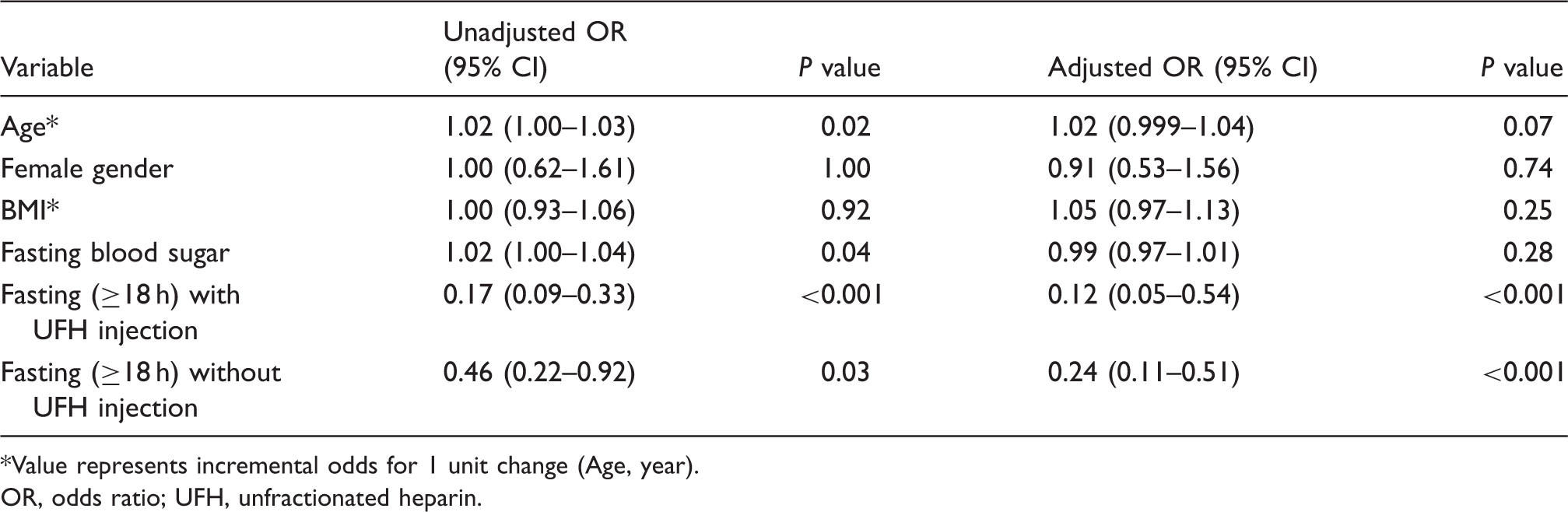
Value represents incremental odds for 1 unit change (Age, year).
OR, odds ratio; UFH, unfractionated heparin.
Discussion
This study demonstrated that fasting for more than 18 h together with UFH administration significantly increased FFA levels by up to three-fold, which was associated with a significant reduction in physiological FDG uptake, as determined by both visual and SUV assessments. This method is considered to be practical, safe, and reliable for assessing cardiac involvement in patients with inflammatory CDs and tumor. Importantly, this method may also be applicable to the detection of inflammation in atherosclerotic plaques.
In this study, FFA levels significantly increased whereas triglyceride levels decreased after UFH administration. FFAs are a major source of myocardial oxidative metabolism particularly in the fasting state, and high levels of FFAs inhibit glucose utilization (11–13). Nuutila et al. investigated the effect of elevation of FFA levels following UFH and intravenous lipid administration on glucose metabolism in the skeletal muscles and the heart (13). They concluded that elevation of FFAs levels effectively inhibits glucose metabolism in the heart. Several case reports also indicated the suppressive effect of UFH on FDG uptake in the heart (6,7). These reports were in accordance with our findings.
The physiological FDG uptake in the heart was effectively suppressed by the UFH administration combined with long (≥18 h) fasting. The prevalence of physiological FDG uptake in the heart in patients who fasted more than 18 h was lower (38%) than that in patients who fasted less than 18 h (69%). This finding is consistent with the report by Langar et al. that long fasting for more than 18 h suppressed myocardial FDG uptake more effectively than a shorter fasting period of less than 12 h (8). Our present study also showed that the physiological FDG uptake in the heart decreased from 38% to 22% following the UFH administration. These findings provide evidence that the UFH administration is an effective method of suppressing the physiological FDG uptake in the heart.
Other methods of suppressing the physiological FDG uptake have been reported. Wykrzykowska et al. (3) reported that the myocardial FDG uptake is effectively suppressed using a low-carbohydrate with high-fat diet preparation. The underlying concept in their method is to reduce glucose uptake in the heart by increasing FFA levels, which is the same as the concept in our method. However, we did not compare the effectiveness of reducing glucose uptake between UFH administration and those diet modification methods. Continuous UFH administration is also effective in suppressing the physiological FDG uptake in the heart (13).
UFH may have several adverse effects. Heparin-induced thrombocytopenia (HIT) is one of the most important complications of UFH. HIT occurs in < 0.1 to 5% of UFH-administered patients (14). Moreover, UFH may also cause hemorrhage owing to its potential anticoagulation effect. Hemorrhage was reported to occur in about 3.8–4% of patients who had intravenous UFH administration (15). In this study, none of the patients had hemorrhage or HIT. However, the patients’ history of hemorrhagic diseases, current anticoagulation therapy, and history of HIT need to be confirmed before UFH administration. UFH should not be used for patients with these features.
Our study has several limitations. First, UFH was administered only to patients with suspected CDs. We confirmed the presence of CDs using other modalities such as myocardial perfusion SPECT or LGE-CMRI. Although our study consisted of a heterogeneous population, we believe that this retrospective study of a consecutive cohort supports the generalizability of UFH administration in clinical settings. Second, UFH was administered only to patients who had fasted more than 18 h. Further study is needed to determine whether a similar effect of UFH could be obtained in patients who fasted for a shorter time. If UFH is effective even in patients with a short fasting time, this method of PET study could be more easily performed. Third, myocardial SUVmax was measured by setting the ROI such that it included the LV blood pool because it is difficult to distinguish the LV wall in patients with a low myocardial FDG uptake.
In conclusion, UFH administration together with fasting for more than 18 h could effectively suppress the physiological FDG uptake in the heart. This method can be reliable for evaluating the affected area and its magnitude in patients with cardiac inflammation and tumors by FDG PET/CT.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.