
Abstract
Background
Only few previous case reports have been found focusing on the imaging findings of adult Wilms’ tumor (WT).
Purpose
To characterize multislice computed tomography (MSCT), magnetic resonance imaging (MRI) characteristics, and follow-up results of adult WT.
Material and Methods
Sixteen patients with WT were studied retrospectively. MSCT and MRI were undertaken to investigate the tumor characteristics.
Results
Tumors (mean diameter, 13.1 ± 4.5 cm) exhibited an expansible appearance and disrupted the reniform contour (16/16), cystic components (16/16), curvilinear calcification (1/16), poorly marginated (2/16), hemorrhage (16/16), displacement of renal pelvis or calyx (13/16), and had lymph node or distal metastases (5/16). Attenuation of WT was less or equal compared to renal parenchyma on unenhanced CT (P > 0.05), while tumor enhancement after administration of a contrast agent was lower than that of normal renal parenchyma (P < 0.05). WT was isointense on T1-weighted (T1W) imaging, isointense or hypointense on T2-weighted (T2W) imaging. Tumor enhancement was less than normal renal cortex in all phases (P < 0.05). The number of tumor stages (grades I, II, III, and IV) was two, three, six, and five cases, respectively. Follow-up time was in the range of 19–123 months; six patients died within 3 years, six patients died within 5 years after the initial diagnosis, with the remaining patients still alive.
Conclusion
Adult WT tends to be a large tumor, isointense or hypointense on T2W imaging with enhancement less than normal renal parenchyma in all phases. The long-term follow-up results demonstrated the poor prognosis of the tumor.
Introduction
Wilms’ tumor (WT) is one of the commonest malignant tumors of childhood. Ninety-eight percent of cases occur in individuals aged less than 10 years, only 2% of reported cases have been adults (1). Most WTs in children are of low stage, have a favorable histology, and are associated with an excellent prognosis. A favorable outcome can be expected even among most neoplasms with small foci of anaplasia. However, most WTs in adults have a poor prognosis, and about two-thirds of patients die of their disease within 3 years of diagnosis in China (2). In routine clinical work, the rate of correct imaging diagnosis of WTs in adults by imaging is low. This is likely due to both a low incidence and a low level of awareness.
Although adult WTs have been relatively well described in pathology studies (3,4), imaging data are scanty. However, patients with adult WT have a different prognosis from other renal cell carcinoma (RCC) subtypes. A close collaboration between radiologists and oncological surgeons is essential to optimize imaging both for initial diagnosis, staging, and preoperative workup, as well as for follow-up during and after treatment. Furthermore, international protocols provide guidelines for imaging workup that allow an inter-institutional comparison for not only research, but also for second opinion statements as well as multi-center therapy evaluation (5). Therefore, an accurate diagnosing is important for guiding clinical treatment.
Material and Methods
Patients
This study was approved by the Institutional Research Ethics Committee. A search of pathology records and PACS system identified 16 patients (computed tomography [CT], n = 16; CT and magnetic resonance imaging [MRI], n = 13) with adult WTs who were hospitalized at Subei People’s Hospital, Yangzhou, PR China between 2001 and 2014. Details of the patients’ age, gender, tumor size, surgery or biopsy confirmation, metastasis, clinical symptoms, follow-up, and therapy were recorded.
CT and MRI technique
CT was performed with one of two clinical scanners: a 16-MSCT scanner, or a 64-MSCT scanner (GE Healthcare, Milwaukee, WI, USA). Scanning parameters were: 120 kVp; 200–300 mAs; section thickness, 3 mm; collimation, 0.6–2.5 mm; pitch, 1.0–1.4; reconstruction interval, 50%; field of view (FOV), 33 cm; rotation time, 0.5 s; reconstruction kernel, B40. Images were obtained with a renal mass protocol that included unenhanced images followed by nephrographic phase images 120 s after i.v. administration of non-ionic contrast medium (Iohexol 350 mgI/mL, Omnipaque, GE Healthcare, Cork, Ireland) at 3–4 mL/s and volume of 1.5 mL/kg followed by a 20-mL saline flush.
MR examination was performed with either a 1.5 T or a 3.0 T MR scanner (Vision or Symphony, Siemens Medical Solutions, Iselin, NJ, USA; or Excite Twin Speed, GE Healthcare, Waukesha, WI, USA). All sequences were acquired with anterior and posterior saturation bands. Axial T1-weighted (T1W) and T2-weighted (T2W) MR images were obtained during breath-hold. The transverse planes covered the entire area of the kidneys. The following sequences were obtained: (i) coronal T2W half Fourier single-shot fast spin-echo; (ii) axial dual-echo T1W in-phase and opposed-phase gradient-echo; and (iii) coronal and sagittal three-dimensional (3D) frequency-selective fat-saturated T1W spoiled gradient-echo. Coronal 3D T1W gradient-echo acquisitions were obtained dynamically in the cortical, medullary, and delayed phases after administration of a bolus of 0.1 mmol/kg gadolinium-DTPA (Magnevist; Berlex Laboratories, Wayne, NJ, USA) at a rate of 2 mL/s followed by a 20-mL saline flush. The first pass was timed to the cortical phase by using a test bolus of 2 mL of contrast agent, and the nephrographic phase was initiated 20 s after the cortical phase. The timing bolus was administered following the initial precontrast phase acquisition.
Pathologic examination
Pathological specimens were observed by light microscopy and immunohistochemical analysis. All renal tumors were confirmed to be WT by pathology and immunohistology.
Imaging and statistical analysis
Imaging characteristics were retrospectively analyzed by two genitourinary radiologists with more than 10 years of experience each. The evaluated parameters included tumor calcification, cystic components, and hemorrhage. Retroperitoneal lymph nodes or distal metastasis, perinephric stranding, hydronephrosis, and renal tissue invasion were also documented.
The presence of an expansile or infiltrative pattern of growth was assessed, as well as which pattern predominated in each case. Expansile growth was characterized by well-marginated bulging tumor margins that displace normal parenchyma, whereas infiltrative growth on CT or MRI was characterized by poorly marginated borders between the tumor and normal renal parenchyma.
The tumor percentage signal intensity (SI) and tumor-to-cortex enhancement index change were assessed. Percentage SI changes were calculated for the tumor and the renal cortex on enhanced phase images as follows: ([SIpost—Sipre]/Sipre) × 100, where SIpost is the SI of the ROI on the contrast-enhanced phase images and SIpre is the SI of the ROI on the image obtained before administration of the contrast agent. The relative enhancement of the tumor with respect to the renal cortex in the same patient (tumor-to-cortex enhancement index) was calculated for cortical, medullary, and delayed phase images as the percentage SI change of the tumor divided by the percentage SI change of the renal cortex.
Statistical analyses were undertaken using SPSS 17.0 statistical software (SPSS Inc, Chicago, IL, USA). Numeric data were expressed as mean ± standard deviation and categorical data were expressed as percentages. Evaluated characteristics were compared using analysis of variance (ANOVA) or independent-samples t test. P values < 0.05 were considered statistically significant.
Results
Clinical, CT, and MRI appearances in adult WT
The study included 16 patients (8 men, 8 women) with WT. The mean age at diagnosis was 32.7 ± 11.8 years (age range, 18–57 years). Presenting symptoms of WT included flank pain (n = 6), hematuria (n = 13), and palpable mass (n = 12).
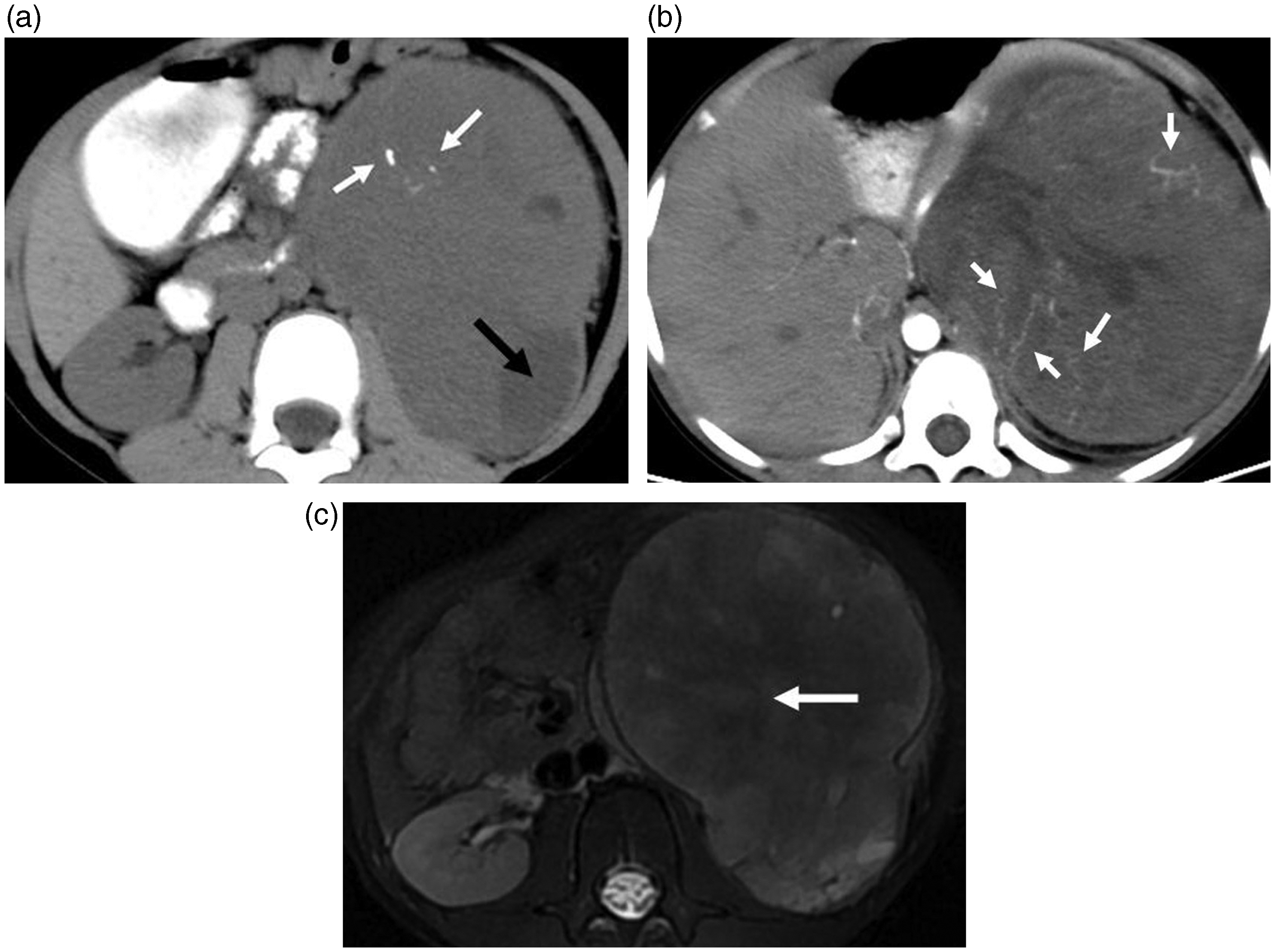
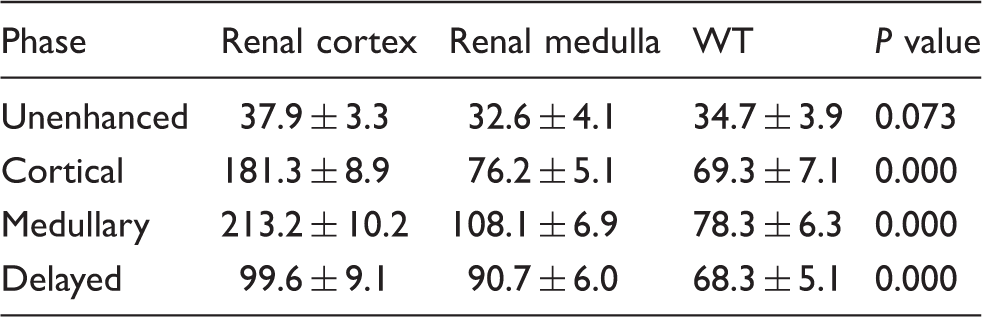
Sixteen patients with WT (mean diameter, 13.1 ± 4.5 cm) exhibited an expansible appearance and disrupted the reniform contour (16/16, Figs 1–3), cystic components (16/16), poorly marginated (2/16), hemorrhage (16/16, Fig. 2b), calcification (1/16, Fig. 3a), displacement of renal pelvis or calyx (13/16), invasion into renal vein, inferior vena cava or ureter (3/16), and had lymph node or distal metastases (5/16). Attenuation of WT was less or equal compared to renal cortex or medulla on unenhanced CT (35.9 ± 4.7 vs. 38.7 ± 3.9 or 33.1 ± 4.6, P = 0.073) (Table 1). On dynamic contrast-enhanced CT scan, the CT attenuation of WT was less than normal renal cortex and medulla during all phases (P = 0.000, 0.000, 0.000, respectively, Table 1).
WT of right kidney in a 57-year-old-man. (a) Unenhanced CT scan showed a clearly marginated mass (diameter, 6 cm), exhibited an expansible appearance and disrupted the reniform contour. (b) Contrast-enhanced CT scan showed mild enhancement which was less than that of the cortex in the cortical phase, and the blood vessel within the tumor was noted (white arrow). WT of right kidney in a 24-year-old-man. (a) Unenhanced CT scan showed a clearly marginated mass (diameter, 12 cm), exhibited an expansible appearance together with cystic components (black arrow) and hemorrhage (white arrows). (b, c) The hemorrhage within tumors was hyperintense on T1W imaging (b, arrow), hypointense on T2W imaging (c, arrow). (d) Contrast-enhanced MR scan showed mild heterogeneous enhancement (arrow). WT of left kidney in a 27-year-old-woman. (a) Unenhanced CT scan showed a clearly marginated hypodense mass (diameter, 13 cm), exhibited an expansible appearance together with curvilinear calcifications (white arrow) and cystic components (black arrow). (b) Contrast-enhanced CT scan showed mild heterogeneous enhancement which was less than that of the cortex in the cortical phase. The tumor distorted and displaced the collecting system and the blood vessel within the tumor was shown (white arrow). (c) The WT was hypointense on T2W imaging (arrow). The CT values of adults with Wilms’ tumor (n = 16), normal renal cortex, and medulla.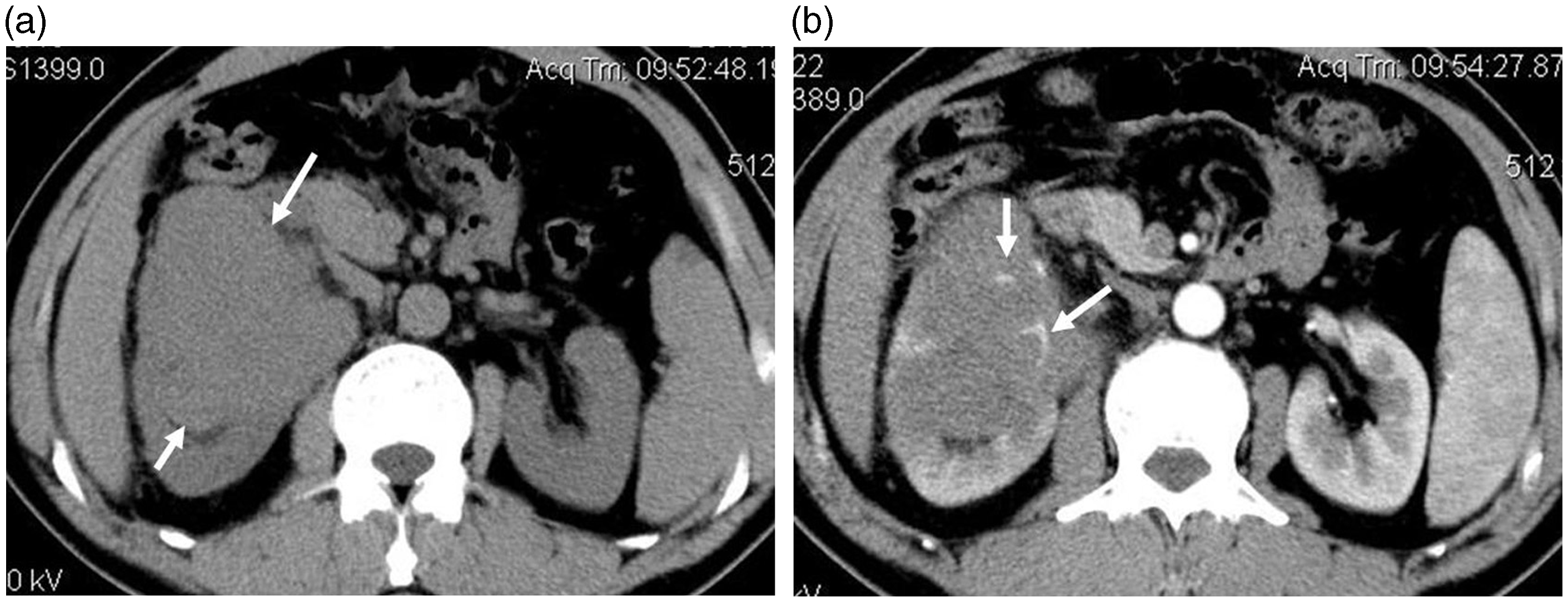
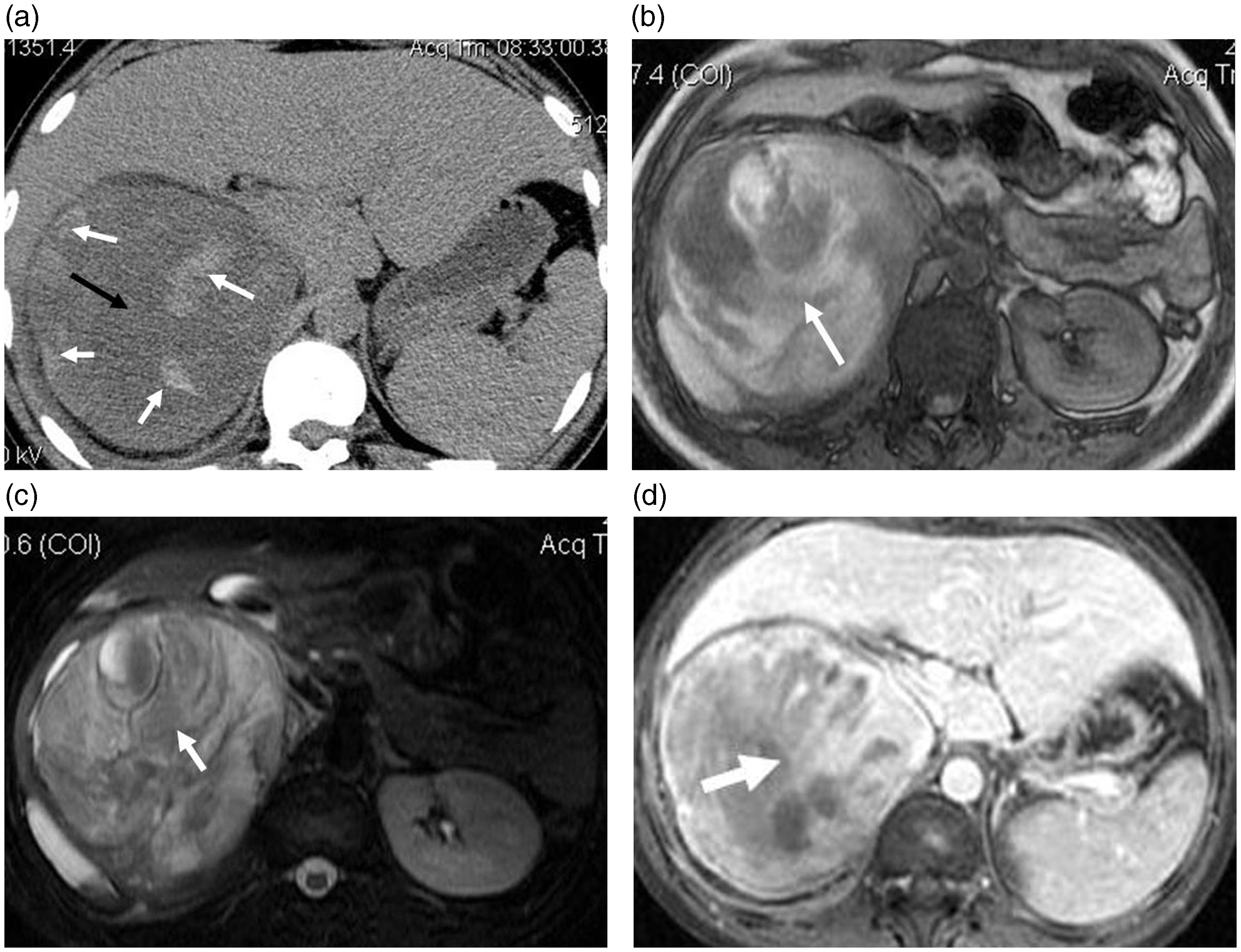
WT was isointense on T1W imaging, isointense or hypointense on T2W imaging. The hemorrhage within tumors was hyperintense on T1W imaging, hypointense on T2W imaging (Figs 2c and 3c). On cortical, medullary, and delayed phases, WTs showed less signal intensity changes ([127.1 ± 8.3]%, [156.6 ± 11.8]% and [138.6 ± 11.1]% than the renal cortex [296.6 ± 40.3]%, [258.3 ± 51.2]% and [230.3 ± 31.7]%, respectively, P = 0.000). The tumor-to-cortex enhancement index during the cortical, medullary, and delayed phases was 0.49 ± 0.19, 0.69 ± 0.31, and 0.56 ± 0.23, respectively. WT enhanced less than renal cortex during all phases.
Therapy and follow-up
General and follow-up data of adults with Wilms’ tumor (n = 16).

C, chemotherapy; F, female; M, male; NED, no evidence of disease; R, radiotherapy; S, surgery.
Microscopic findings
Microscopic analysis indicated that the blastemal cells of WT are small, closely packed, and mitotically active rounded or oval cells with scant cytoplasm, and overlapping nuclei containing evenly distributed, slightly coarse chromatin, and small nucleoli. Hemorrhage, or hemosiderin deposition were found in all 16 cases. Immunochemistry staining demonstrated vimentin, neuron specific enolase (NSE), WT-1 in 13 cases (+++), 13 cases (++), and 15 cases (++), respectively.
Discussion
WT is one of the commonest malignant tumors of childhood. It appears mainly in the first 5 years of life. Pediatric WTs are typically large (average diameter, 12 cm) and spherical. On CT scan, pediatric WT appears heterogeneous and attenuation is usually slightly lower than the uninvolved kidney on unenhanced scans. On MR scan, tumor demonstrates a heterogeneous hypointense signal on T1W sequences and heterogeneous hypo- or isointense signal relative to renal cortex with hyperintense necrotic or cystic areas on T2W sequences (5).
Incidental examples of adult WT have been described in the literature (about 2% of all described cases) (6,7). Kilton (8) have applied six rigid diagnostic criteria for adult WT, which still remain in use: (i) primary renal neoplasm; (ii) primary blastematous spindle- or round-cell component; (iii) formation of abortive or embryonal, tubular epithelial, or glomeruloid structure; (iv) no areas of tumor diagnostic of renal cell carcinoma; (v) pictorial confirmation of histology; and (vi) age >15 years. According to these strict diagnostic criteria, only about 300 cases of adult WT have been reported in the English literature to date.
Most RCCs grow by radial expansion with displacement of the normal parenchyma, focal bulging of the renal contour, and pseudocapsule formation (9,10). Infiltrative growth was a less common pattern (11), which differ from those of cortical clear cell RCCs (12), the most common subtype, exhibit an expansible appearance with exophytic growth that disrupts the reniform contour (13). WTs exhibited an expansible appearance that disrupted the reniform contour (14). In our study, 16 patients with WTs had an expansible appearance that disrupted the reniform contour.
In our MR cases, isointense or hypointense signal on T2W imaging were observed, which was thought to be due to hemosiderin deposition (15,16). This is in distinction to many renal tumors that are hyperintense on T2W imaging, such as clear cell RCCs (17), some cystic renal tumors, and cysts. Larger clear cell RCCs tend to have a heterogeneous, hyperintense signal on T2W MRI, separating them from WT (18,19).
Perlman (20) reported that calcification within the tumors often suggested RCC subtypes. RCCs >3 cm often contain intratumoral necrosis, hemorrhage, cystic components, and calcifications, and are usually of the clear cell variety. In our study, there was evidence of calcification in only one patient, which was curvilinear compared with the stippled calcification seen in neuroblastoma.
In our study, enhancement was lower in WTs than in renal cortex in all phases. This enhancement pattern is atypical of hypervascular tumors such as clear cell RCCs, renal medullary carcinomas, renal angiomyolipomas, and renal angiomas. For example, the degree of enhancement of clear cell RCC is commonly similar or higher than renal cortex (21). Therefore, one may distinguish between WTs and tumors with hypervascularity on the basis of differences in enhancement.
In common with WTs, collecting duct carcinomas, chromophobe RCCs, and renal lymphomas are hypovascular compared to renal parenchyma on enhanced CT imaging. Medullary involvement and an infiltrative appearance are common findings on CT imaging and may suggest the diagnosis of collecting duct carcinomas (22). Papillary RCCs may be multifocal and bilateral, and tend to be less than 2 cm in size at diagnosis (23,24).
Lymph node or distal metastasis was noted in five cases and inferior vena cava or ureter in three cases of WT. Others have reported metastasis associated with this tumor occurring in adult (25). However, pediatric WT extension of tumor thrombus into the renal vein and inferior vena cava has been reported in up to 10% of cases, with possible extension into the right atrium. In comparison, clear cell RCC is associated with renal vein infiltration (26).
Information regarding the clinical behavior of adult WT is limited due to the rare incidence (27). Although the clinical course of these patients are rather indolent, routine follow-up is still mandatory (28). The correct distinction of WTs from other tumors can lead to better understanding of their clinicopathologic differences, which should aid in developing individualized management plans (29).
The present study had certain limitations. First, a small number of patients were included owing to the rarity of adult WT; and second, 81% (13/16) of patients with adult WT were diagnosed by pathology. Therefore, further multicenter cooperation on the radiological diagnosis of adult WT is required.
In conclusion, adult WT is a rare subtype of renal tumor with special pathologic features. Imaging features of adult WT include a large tumor, isointense or hypointense on T2W imaging with enhancement less than the normal renal parenchyma in all phases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received National Natural Science Foundation of China: 81401384.