
Abstract
Background
The anatomical lung volume is conventionally measured by computed tomography (CT). However, chest radiographs could be considered as an alternative method with low cost and low radiation.
Purpose
To predict the anatomical lung volume using planimetric measurements of chest radiographs.
Material and Methods
In total, 119 participants (M:F ratio = 66:53; age, 53.7 ± 9.6 years) who underwent chest CT for lung cancer screening were enrolled. The lung volume on CT was measured as a reference for the anatomical lung volume. To eliminate the bias from the degree of inspiration, virtual chest radiographs (posterior–anterior view and lateral view) were generated from the CT images using the thick multiplanar technique, and the lung area (cm2) was measured in the right (P), left (Q), and lateral (R) lungs according to the planimetric method. A regression equation predicting the anatomical lung volume from the planimetric measurements was generated. The correlation between the measured and estimated lung volumes was evaluated. The percentage error rate (%) was calculated and the equation was validated internally and externally.
Results
The equation predicting the anatomical lung volume (mL) was 9.6*S–1367, where the summed lung area (S) was defined as (P + Q + R). The measured and estimated lung volumes were highly correlated (R = 0.941, P < 0.001). The absolute error rate was 5.7 ± 4.9%. The root mean square error of the equation was 290.2. The root mean square errors on internal and external validation were 300.4 and 267.0.
Conclusion
The anatomical lung volume may be feasibly and accurately predicted from planimetric measurements of chest radiographs.
Introduction
Anatomical lung volume is a useful parameter in various clinical situations including chronic obstructive pulmonary disease (COPD), lung volume reduction surgery, and lung transplantation (1–6). Volumetric data from multi-detector computed tomography (MDCT) can be used to accurately calculate the anatomical lung volume (1,7). However, the utility of CT can be limited by several factors such as the clinical condition, radiation dose, and economic restrictions. Donors, before lung transplantation, do not have chest CT taken routinely. Repeated chest CT scans for volume change might be inappropriate due to radiation and cost. Chest radiography is a simple, inexpensive, and more accessible imaging modality than CT. If anatomical lung volume could be measured by chest radiography, it would be possible to measure and compare the lung volume repeatedly. Pratt et al. (8) described a simple and accurate planimetric method of predicting the functional lung volume using chest radiographs. Therefore, we surmised that planimetric measurements on chest radiographs could accurately predict the anatomical lung volume as well as functional lung volume. In this study, we aimed to construct a new equation for predicting the anatomical lung volume from chest radiographs using CT lung volume as a reference.
Material and Methods
Study population
A total of 131 consecutive healthy participants who underwent chest CT for lung cancer screening from January to April 2014 were retrospectively enrolled, and their CT images and medical records were reviewed. Twelve participants who previously underwent pulmonary surgery or had abnormalities on chest CT images, such as tumor, infection, emphysema, fibrosis, or pulmonary effusion, were excluded. Finally, 119 participants were included in the analysis. An additional 85 participants were used for external validation of the equation. This study was approved by the institutional review board. The CT images and clinical data were retrospectively obtained; therefore, the requirement for informed consent was waived.
Computed tomography protocol
Low-dose CT was performed using a 64-slice MDCT scanner (Brilliance CT 64-slice; Philips Healthcare, Best, The Netherlands). Subjects were scanned in the supine position from the lung apex to the adrenal glands during breath-holding at the end of inspiration. After acquisition of a scout image to determine the field of view (FOV), low-dose CT was performed using a helical technique and a mediastinal window setting with the following exposure parameters: 120 kVp; 50 mA; slice thickness, 1 mm; and reconstruction interval, 1 mm. Images were reconstructed on the scanner’s workstation. All CT images were retrieved using a picture archiving and communication system (PACS; Centricity™ 2.0; GE Healthcare, Mt. Prospect, IL, USA) and analyzed.
CT image analysis
All CT images were reviewed by two radiologists who each had over 10 years of experience in chest CT interpretation. Images were excluded if abnormal features, including tumors, infection, emphysema, fibrosis, or pleural effusion, were found. Eligible axial CT images were transferred to a commercially available reconstruction program for three-dimensional (3D) reconstruction and measurement (Aquarius iNtuition™ Ver.4.4.6 TeraRecon, Foster City, CA, USA). The CT lung volume was measured semi-automatically as the reference anatomical lung volume using a threshold-based 3D auto-segmentation technique at a default range from –200 to –1024 HU (7,9) (Fig. 1).
Measurement of lung volume on CT using an auto-segmentation technique. The anatomical lung volume was measured semi-automatically by volumetric CT to serve as the reference using a threshold-based 3D auto-segmentation technique with a default range from –200 to –1024 HU. In this case, the lung volume was 5007 cm3.
Planimetric measurement of virtual chest radiographs
To eliminate bias from the degree of inspiration, virtual chest radiographs (posterior–anterior [P-A] and lateral views) were generated from the axial CT images using the thick multiplanar technique (Fig. 2a and b). Lung area was measured on the virtual chest radiographs using an electronic caliper according to the planimetric method described by Pratt et al. (8,10,11,12) (Fig. 2c and d). Three lung areas (cm2) were measured as follows: P, the right lung area on the virtual chest P-A view; Q, the left lung area on the virtual chest P-A view; and R, the lateral lung area on the virtual lateral view. The sum of these three areas (S) was calculated as follows: S = P + Q + R.
Measurement of lung area using the planimetric method. Virtual chest radiographs (posterior–anterior and lateral views) were generated by the thick multiplanar technique from axial CT images (a, b). The lung area was measured on the virtual chest radiographs using electronic calipers according to the planimetric method described by Harris et al. (12) (c, d). On the PA film, a line is drawn along the cardiac and mediastinal shadow, hemi-diaphragm, and pleural surface of the chest wall, joining at the apex of the lung. On the lateral film a line is drawn along the internal surface of the sternum, midway between the two hemi-diaphragmatic shadows, at the posterior margin of the vertebral bodies, joining at the apex of the lung.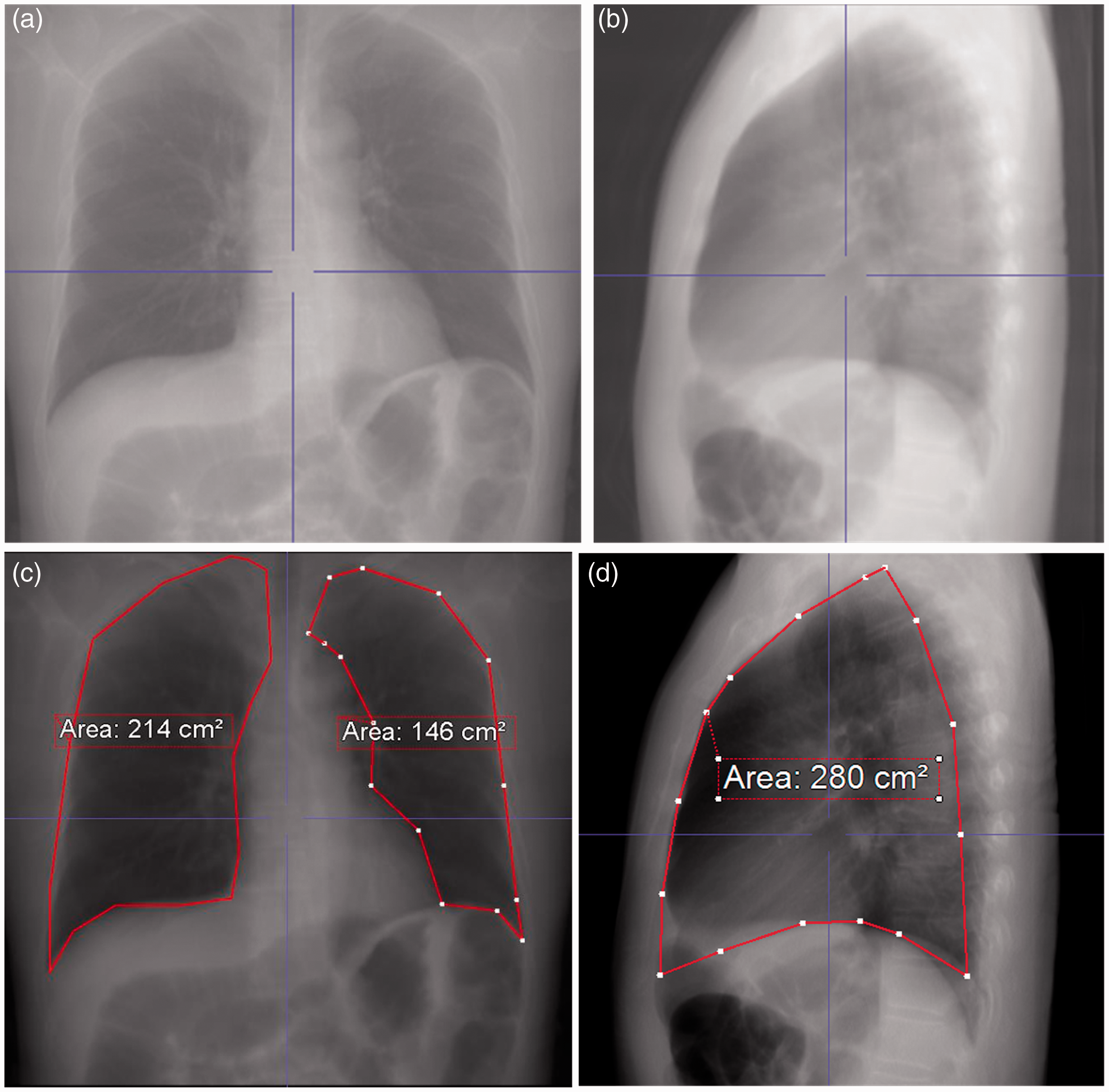
All measurements were performed independently by two radiologists, and the inter-observer variability was examined.
Statistical analysis, regression equation generation, and validation
Continuous variables are expressed as the mean ± standard deviation (SD), and categorical variables are expressed as the frequency or percentage. The intraclass correlation coefficient was used to evaluate the inter-observer reproducibility of the measured lung volume and planimetric lung area. An equation predicting the lung volume using S was generated by simple linear regression analysis. The correlation between the lung volume measured by CT and the estimated lung volume calculated using the equation was evaluated using Pearson correlation analysis. The percentage error rate (%) of the generated equation was calculated as follows: ([Estimated lung volume – Measured lung volume]/Measured lung volume × 100). The reliability of the predictive model was internally validated using the five-fold cross-validation method. The differences between the predicted and measured lung volumes were used to calculate the root mean square error (RMSE). External validation was performed using an additional 85 healthy participants. All data were analyzed using SAS® version 9.1.3 statistical software (SAS Institute Inc., Cary, NC, USA), and P < 0.05 was considered statistically significant.
Results
Demographic characteristics in 119 healthy participants used for the predictive equation and 85 healthy participants used for external validation.
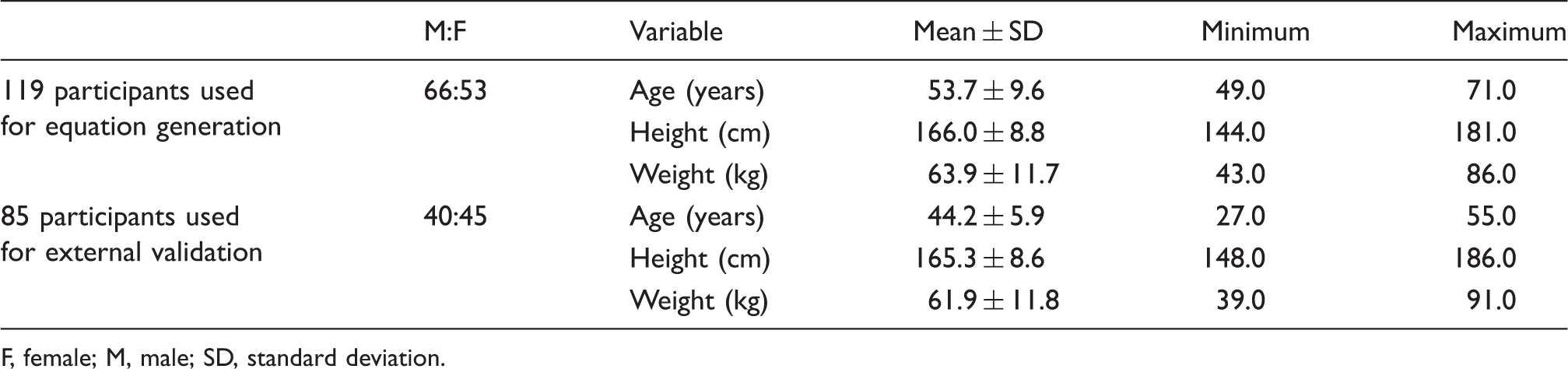
F, female; M, male; SD, standard deviation.
Planimetric measurements in virtual chest radiographs and measured CT lung volume in 119 participants.

CT, computed tomography; SD, standard deviation.

Comparison of measured CT lung volume and estimated lung volume. The correlation between the measured CT lung volume and the lung volume estimated using planimetric measurements is very high (R = 0.941, P < 0.001).
Calculated regression equation and validation results.

RMSE, root mean square error; S, summed lung area using planimetric measurements; SE, standard error.
Discussion
A new equation was made in the present study to predict the anatomical lung volume (mL) by using planimetric measurements on chest radiographs. The resulting equation was simple (9.6*S–1367) and predicted the anatomical lung volume with a low absolute error rate.
Historically, there has been many efforts to estimate lung volume from plain radiographs, and two methods are primarily used to predict the functional lung volume. In 1966, Loyd et al. (10) described a modified ellipsoid method for predicting the total lung capacity (pTLC) from chest radiographs. This method can predict the TLC measured by plethysmography with high accuracy and reproducibility. However, the measurement is complex, as the volumes of the five ellipsoid lung compartments are calculated using various diameters and heights (11). In 1971, Harris et al. (12) described a simpler planimetric method for TLC prediction. The resulting equation for pTLC was as follows: 8.5*S – 1200, where S is the summed surface area (cm2) of the right, left, and lateral lungs on chest radiography. The planimetric method for calculating the functional lung volume was simple and feasible in healthy participants and patients (11–13). The anatomical lung volume is an important parameter in addition to functional lung volume, and it correlates well with the functional lung volume (14). Gollogly et al. (2) reported that the anatomical lung volume could serve as a supplementary tool in pulmonary function testing. In patients undergoing lung transplantation, the anatomical lung volume can be used in size-matching (15), which is critical as size mismatches between donor lungs and recipient thorax can result in numerous complications and poor prognosis (16–18). In COPD patients, the anatomical lung volume and its change during inspiration and expiration reflect disease severity (3,19,20). After lung volume reduction surgery, the change in anatomical lung volume can indicate the effectiveness of surgery (4). MDCT can accurately measure lung volume (21), however, CT may be limited under certain conditions depending on the clinical condition of the transplantation donor, increases in radiation dose with repeated scans, and economic restrictions. Estimation of anatomical lung volume from chest radiographs could replace MDCT with less cost and lower radiation, while maintaining high accuracy. However, no studies have predicted the anatomical lung volume using chest radiographs. By using our simple equation, anatomical lung volume could be measured easily and repeatedly in patients with various conditions, including lung transplantation, COPD and lung volume reduction surgery.
In this study, we aimed to predict the anatomical lung volume using planimetric measurements from chest radiographs. This new equation for anatomical lung volume is as simple as the Harris equation, and the absolute error rate was low at 5.7%. The correlation between the measured and estimated lung volume was very high (R = 0.94, R2 = 0.90). On the internal and external validation, the RMSEs were similar to that of the equation, confirming the fitness of the equation. The equation presented on this study is different from the equation by Harris et al. (12) in that our equation was designed to predict the anatomical lung volume at the same inspiration level of chest radiographs.
There are several limitations in our study. First, this study was performed at a single center with a small number of participants. However, both internal and external validations were performed. Second, the radiological lung volume may potentially be affected by the depth of inspiration during imaging; however, we used virtual radiographs generated from CT images to minimize the effect of inspiration. The inter-observer reproducibility for measuring the CT lung volume and planimetric lung areas was very high because of the semi-automatic measurement method and clear guidelines for performing the planimetric measurements.
In conclusion, a new, simple regression equation was generated using planimetric measurements from chest radiographs and could be a feasible method for estimating the anatomical lung volume.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.