
Abstract
Background
Scapholunate interosseous ligament (SLIL) injuries can often be difficult to detect using magnetic resonance imaging (MRI), especially with older 1.0 and 1.5 Tesla magnets. Wrist arthroscopy is the gold standard for diagnosis of SLIL injuries, but is an invasive procedure with associated risks.
Purpose
To assess whether SLIL injuries can be more accurately detected using axial MRI sequences instead of coronal sequences.
Material and Methods
An institutional review board approved retrospective analysis of arthroscopic wrist surgeries performed at our institution. Patients that had a preoperative MRI performed at our university center using a 1.5 Tesla scanner with a dedicated wrist coil were included in the study. Three fellowship-trained musculoskeletal radiologists reviewed the axial sequences and coronal sequences independently. The accuracy of the coronal and axial sequences was compared with the arthroscopic/surgical findings.
Result
Twenty-six patients met the inclusion criteria. The sensitivity for SLIL tears was 79% and 65% for the axial and coronal sequences, respectively. The specificity was 82% for the axial and 69% for the coronal sequences, respectively. The positive and negative predictive values for the axial sequences were 76% and 84% respectively, compared to 68% and 71% for the coronal sequences, a statistically significant difference.
Conclusion
SLIL tears are more readily detectable on axial MRI sequences than coronal. Clinically, patients with radial-sided wrist pain and suspicion for SLIL tears should have the axial sequences scrutinized carefully. An otherwise normal study with the axial sequence being degraded by motion or other MRI artifacts might need repeat imaging.
Introduction
Ligamentous injuries of the wrist are a common problem, which can lead to clinically significant progressive instability and weakening if the diagnosis is delayed (1). These injuries most frequently involve the scapholunate interosseous (SLIL) and lunotriquetral interosseous (LTIL) ligaments, and a SLIL tear is one of the most common causes of carpal instability (2). Thus, precise prompt preoperative diagnosis is the key to guide definitive surgical management (3).
The SLIL ligament is a C-shaped structure divided anatomically into three portions: volar, membranous (or proximal), and dorsal components (4). The dorsal and palmar portions of the SLIL are true ligamentous structures, whereas the membranous portion is thin and structurally irrelevant from a clinical standpoint because tears of the membranous portion rarely occur in isolation and are not addressed surgically (4). Biomechanically, the three portions of the SLIL have distinctive physical properties, with the dorsal portion of the ligament having the maximum load capacity.
Cadaveric studies of ligament splitting have demonstrated the SLIL to be the principal ligament accountable for stabilization of the scapholunate (SL) joint (5–9). Yet, routine posteroanterior (PA) radiographs after wrist injury are not suitable to completely exclude ligamentous injury (10,11). Even a complete tear of the SLIL may show no static increase in the SL gap or a change in the lateral SL angle radiographically (12).
Early diagnosis is critical in the subtle occult and dynamic stages of SLIL injury, during which there is a small time window during which the ligament can be successfully repaired. Rohman et al. concluded that more preferable outcomes were obtained if acute intervention occurred within 6 weeks of the injury (13). Clinically, the classic “scaphoid shift test” has been shown to be falsely positive in up to one-third of patients and is usually only present in more severe SLIL injuries, with sensitivity and specificity of 69% and 66%, respectively (14,15). Additionally, radiographs in both the non-stress and stress positions may be negative in these early stages.
Wrist arthroscopy is widely regarded as the gold standard for the diagnosis of SLIL injury (16). Arthroscopy yields both important functional and anatomic information for the orthopedic surgeon; in addition, combination with fluoroscopy can offer kinematic information as well (15). Arthroscopy, however, is an invasive surgical procedure with attendant risks.
Less invasive diagnostic tools include magnetic resonance imaging (MRI), MR arthrography, and computed tomography (CT) arthrography. The diagnostic usefulness of CT arthrography has only been investigated in a few prior studies (17). MR arthrography is minimally invasive and can be moderately painful for the patient, with added minor potential risks of infection and hemorrhage. MRI is the least invasive tool in evaluating SLIL injuries, but has historical diagnostic variability in detecting tears (18). Ultrasound has also been studied in diagnostic evaluation of the SLIL, with sensitivity in detecting dorsal band tearing, in the range of 46–100% (19).
The goal of this study was to examine how diagnostic performance in evaluating SLIL tears with MRI can be improved. Our hypothesis was that the axial plane may yield improved information compared with use of the coronal plane only. Since Berger’s study in 1994, which suggested that the coronal sequence was superior in evaluating the SLIL, many musculoskeletal radiologists have relied heavily on the coronal plane (20). Advances in MR technology have vastly improved during this time, and the advent of 3 Tesla MR has demonstrated superior evaluation of the SLIL compared with 1.5 Tesla (21). However, high-resolution 3 Tesla scanners are not yet as widely available as the 1.5 Tesla scanners.
In the current study, we compare the diagnostic performance in detecting scapholunate ligament tears with 1.5 T MRI in the axial versus coronal planes.
Material and Methods
Patients
After approval by the institutional review board (IRB), we retrospectively reviewed MRI studies of 26 wrists in patients who fulfilled the following criteria: (i) preoperative wrist MRI at our institution; (ii) the patients subsequently underwent arthroscopy and/or wrist surgery for radial sided wrist pain; and (iii) the surgical report provided description of the SLIL.
MRI
All MRI studies were performed on a GE Signa HDx 1.5T Optima Ed. (GE Healthcare, Waukesha, WI, USA), utilizing software release Rel. 23 (discovery interface), and a dedicated 8-channel phased-array extremity coil (Precision 8 wrist array coil, GE Healthcare) with 12 cm maximum field of view. The wrist imaging protocol at our institution includes acquisition of coronal, axial, and sagittal planes. For the axial planes we obtain two proton density fast spin echo (FSE) images (TR/TE, 2500/28 ms; matrix, 282 × 512; gap, 0.00; flip angle, 180°): one that is fat saturated and one that is not. For the coronal planes we obtain: a T2 3D (TR/TE, 46/25 ms; matrix, 320 × 320; gap, 0.00; flip angle, 7°); T2 inversion recovery (IR) FSE (TR/TE, 3500/14 ms; relaxation time (TI), 130 ms; matrix, 202 × 448; gap, 0.00; flip angle, 180°); and a proton density fast spin echo (FSE) (TR/TE, 4000/33 ms; matrix, 282 × 512; gap, 0.00; flip angle, 150°). Imaging parameters included a slice thickness of 2.5 mm for coronal plane images, with the exception of 3D coronal images at 1.0 mm thickness. Axial images were performed at 2.5–3.0 mm slice thickness.
Analysis of MR images
Three independent observers (identified as observers A, B, and C), blinded to the arthroscopic and/or surgical results and any clinical information about the participants, evaluated the images. All three observers were fellowship trained in musculoskeletal imaging, with 10, 20, and 20 years of experience, respectively. The coronal and axial sequences for each patient were evaluated independently from each other one at a time in a randomized order. The morphologic appearance of the three components of the SLIL (dorsal, volar, and membranous) was assessed independently in each plane. As in previous studies, complete tears were classified by the presence of fluid through the ligament, and indistinctness, discontinuity, or disruption of the ligament, up to the point of absence of the entire ligament (22,23). Partial tears of the SLIL were diagnosed by the presence of fluid through a portion of the ligament, i.e. not spanning the entire synovial to synovial width, excessive T2 hyperintensity and any altered morphology, such as the thickness of the ligament. Data were recorded on individual worksheets.
As part of our retrospective review, we compared the original preoperative MRI reports with the final arthroscopy and/or surgical reports, to detect errors in our initial diagnosis of SLIL injuries at the time of the patients’ first presentation.
Statistical analysis
Each SLIL was classified as having either a complete full-thickness tear (a tear involving all three portions of the ligament with complete disassociation between the scaphoid and lunate), a focal full-thickness tear (a focal tear involving one, two, or all three portions of the ligament with incomplete disassociation between the scaphoid and lunate), a partial thickness tear (a tear that only involved a portion of the thickness of the ligament), or lastly, an intact ligament. Diagnostic accuracy, including sensitivity, specificity, accuracy, negative predictive value, and positive predictive value, was determined for each sequence and each observer for the diagnosis of tears of the SLIL. All percentages were calculated with 95% confidence interval (CI) (24).
Results
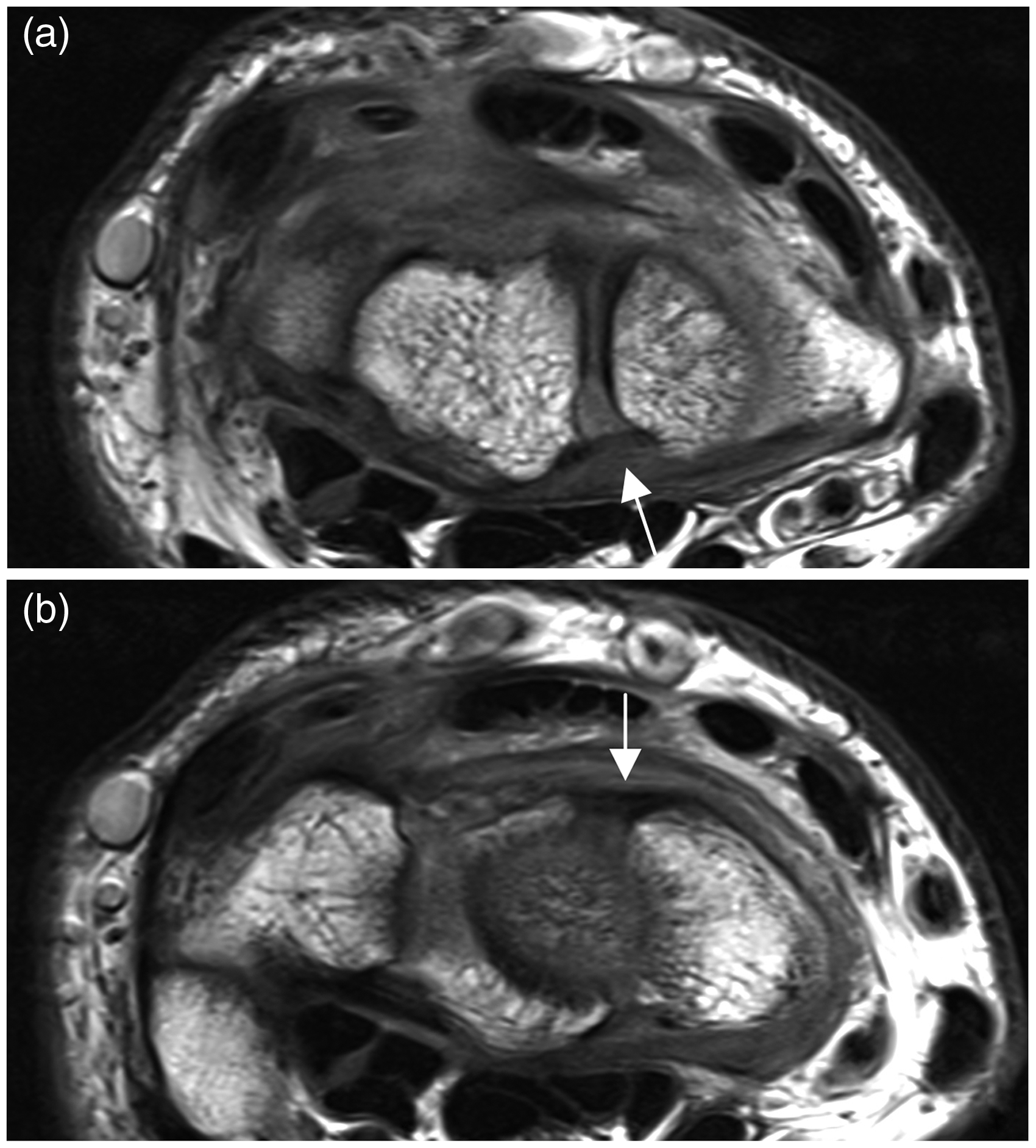
A total of 98 patients were enrolled in the study; however, after review only 26 patients met our inclusion criteria. Of those 26 participants, 13 were men and 13 women. Their mean age was 38 years (age range, 18–65 years). Eleven patients demonstrated complete, focal, or partial thickness tears of the SLIL, and 15 were enrolled as normal subjects (demonstrating either mild fraying or a completely normal ligament at arthroscopy). Figs. 1 and 2 demonstrate the normal appearance of the SLIL in both the coronal and axial planes, respectively. Only one participant demonstrated a complete full-thickness tear of the SLIL. Of the remaining patients, two demonstrated focal full-thickness tears and eight demonstrated partial thickness tears of portions of the SLIL (Table 1).
Normal scapholunate interosseous ligament anatomy on coronal MRI. Normal coronal anatomy of the scapholunate interosseous ligament: three portions. T2 3D (TE, 25; TR, 46; slice thickness, 1.0 mm). S = scaphoid bone, L = lunate bone. (a) T2 3D coronal image of the wrist, the volar portion of the ligament is trapezoidal and intermediate signal (arrow). (b) T2 3D coronal image of the wrist, the membranous portion of the ligament is lower in signal than the volar portion and triangular in configuration (arrow). (c) T2 3D coronal image of the wrist. The dorsal portion has “fan” morphology and is lower in signal (arrow). Normal scapholunate interosseous ligament anatomy on axial MRI. Normal axial anatomy of the scapholunate interosseous ligament. Proton density fast spin echo (TE, 28; TR, 2500; slice thickness, 3.0 mm). (a) Demonstrates normal appearing volar (arrow) and interosseous portions of the ligament. (b) Demonstrates a thick, normal appearing dorsal portion (arrow) of the ligament. Scapholunate interosseous ligament positive cases at arthroscopy and surgery.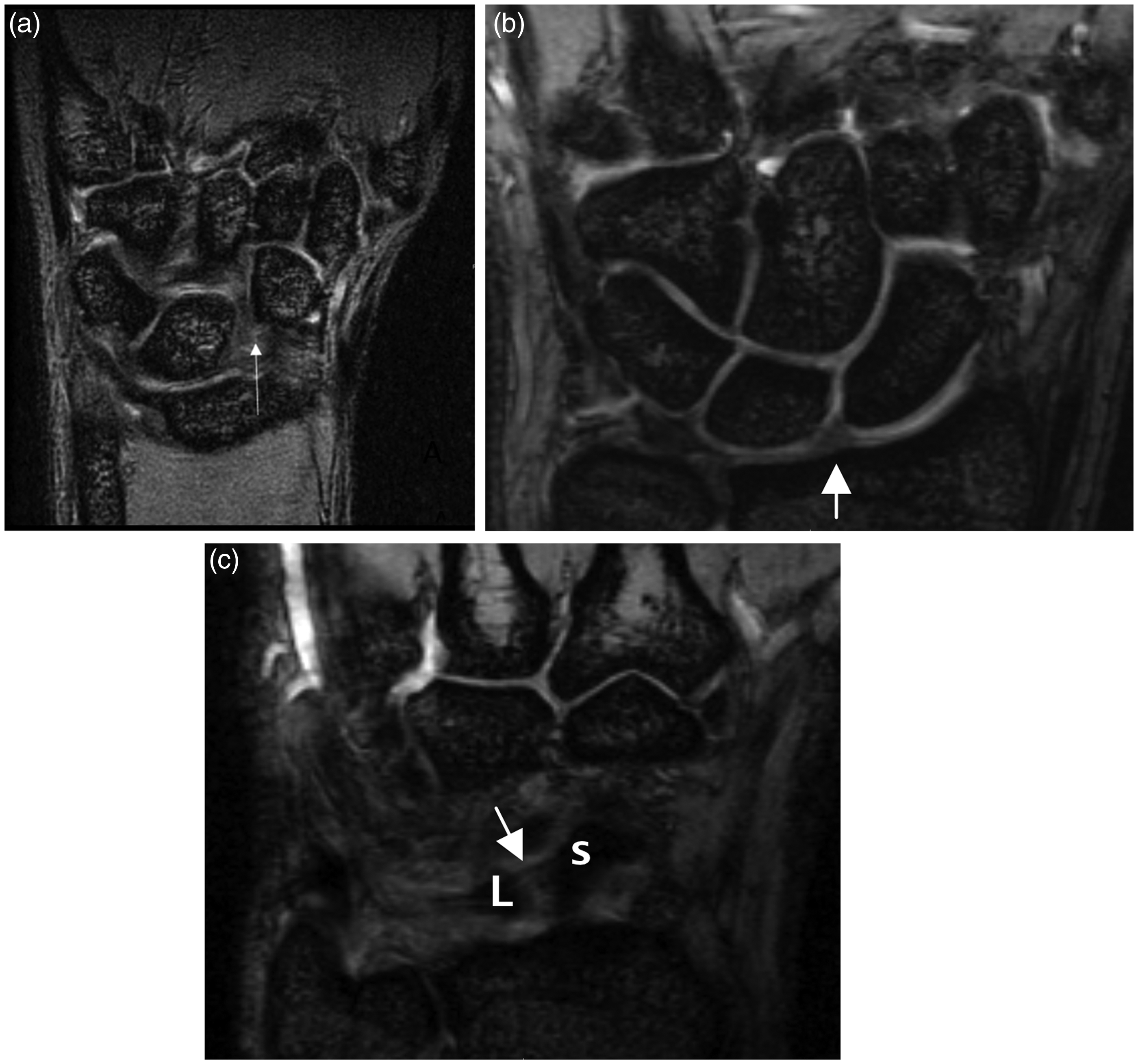

Diagnostic statistical performance of axial plane on MRI.

Diagnostic statistical performance of coronal plane on MRI.

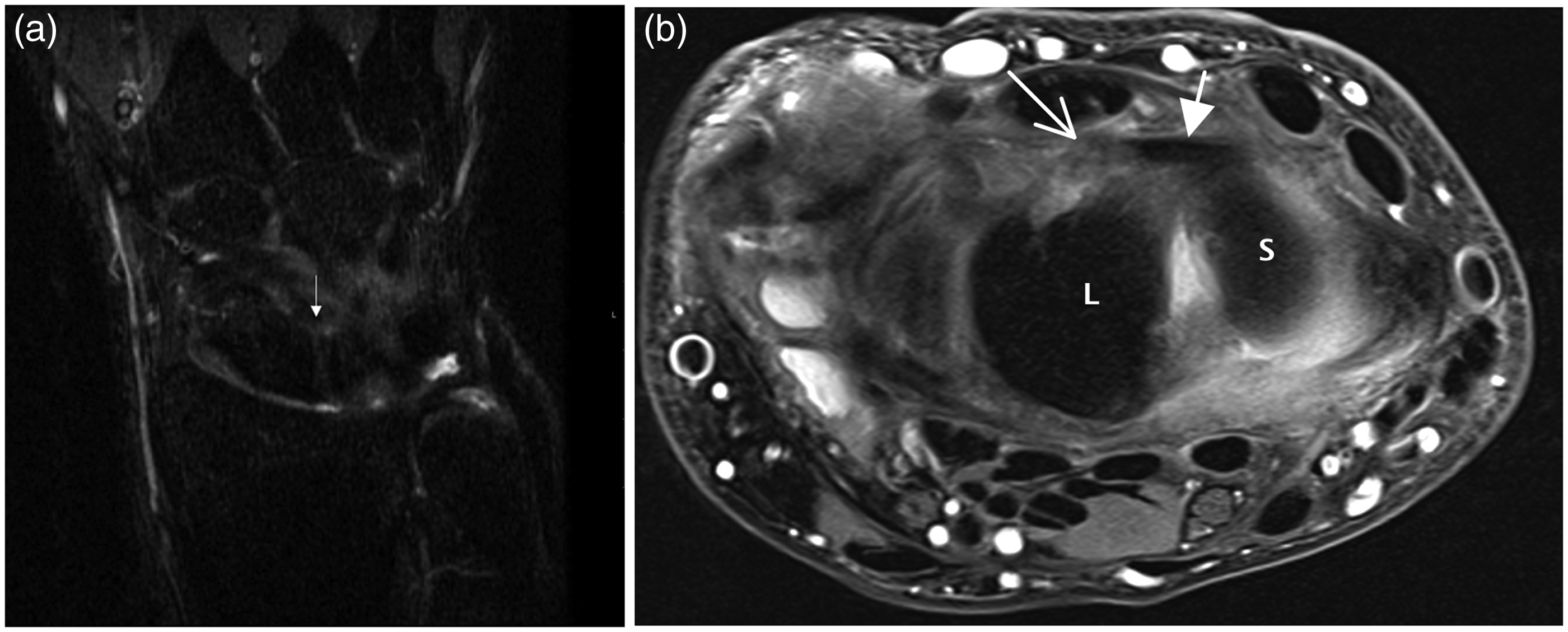
The retrospective nature of the study allowed us to review the original preoperative MRI report to detect errors in our initial diagnosis of SLIL injuries. It was found that in many instances false positive diagnoses were made of SLIL tears based on the coronal sequence (Fig. 3). In addition, we also found instances where initial reports falsely suggested the absence of a complete SLIL tear based on the coronal sequences alone. In Fig. 4, the initial MRI reported the dorsal portion of the ligament as “intact”. However, careful scrutiny of the axial plane demonstrates avulsion of the dorsal portion of ligament from its lunate attachment, a finding that correlates precisely with the subsequent surgical report.
Retrospective mistake on original MRI report: false positive result. (a) Coronal T2 3D (TE, 25; TR, 46; thickness, 1.0 mm) and (b) axial proton density FSE fat-saturated (TE, 28; TR, 2500) images through the SLIL ligament. S = scaphoid bone, L = lunate bone. (a) The initial MRI report was read as a “full thickness tear of the dorsal portion based on the coronal sequence” (arrow). (b) Evaluation of the same patient, in the axial plane, demonstrates an intact ligament where both the dorsal (solid arrow) and volar (open arrow) portions of the ligament are normal and well demonstrated. Retrospective mistake on original MRI report: false negative result. (a) Coronal proton density fast spin echo (TE, 33; TR, 4000; slice thickness, 2.5 mm) and (b) axial proton density FSE fat-saturated images (TE, 28; TR, 2500; thickness, 3.0 mm). S = scaphoid bone, L = lunate bone. (a) Coronal slice through the dorsal ligament (arrow), this was read as “intact” in the original MRI report. (b) Axial slice through the dorsal ligament (solid arrow) shows a clear focal full-thickness tear where the ligament is avulsed from its lunate attachment (open arrow).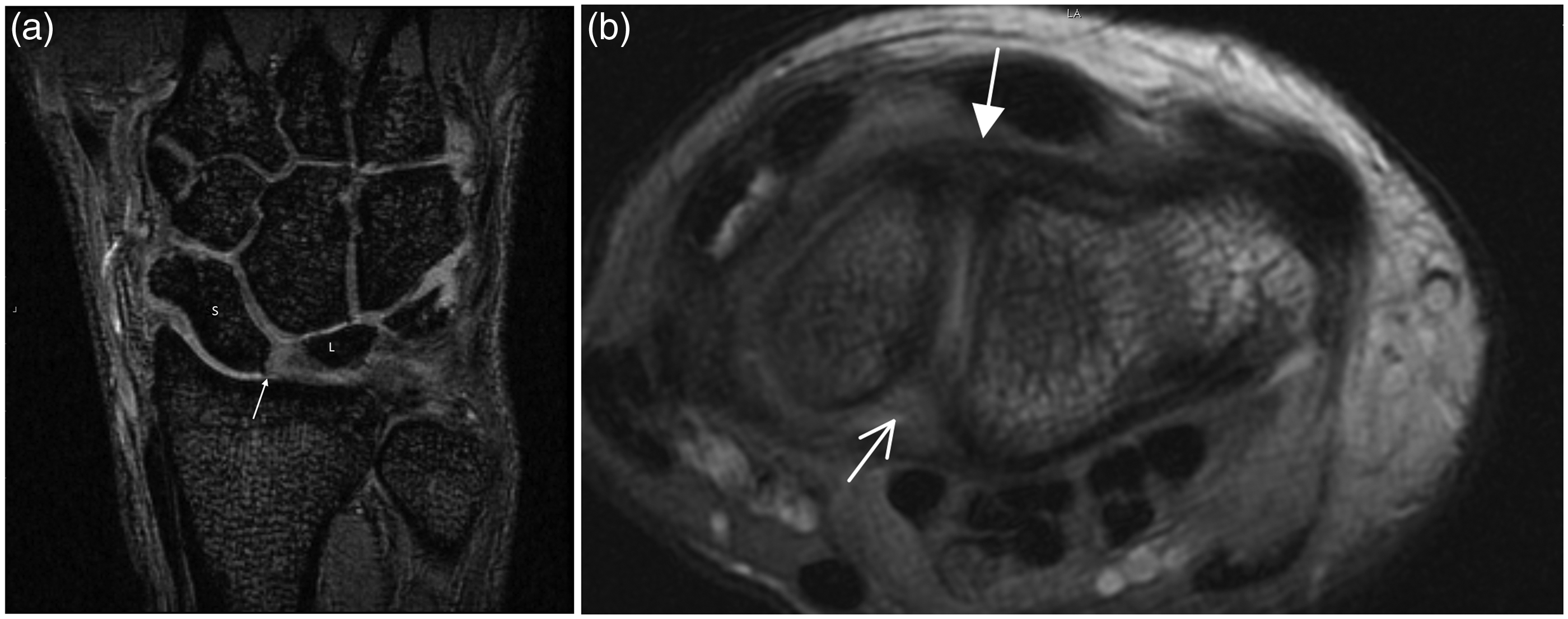
Discussion
The purpose of our study was to compare axial versus coronal sequences to discover the optimal plane to diagnose SLIL tears on MRI. Previous studies have evaluated the diagnostic accuracy of MRI with regards to SLIL tears (17). These studies have traditionally demonstrated a wide range of sensitivities, in the range of 38–88%. However, to date, no study has evaluated the diagnostic accuracy of MRI by comparing the axial and coronal planes.
Our results show that the axial plane is superior to the coronal plane with regards to the diagnostic accuracy of SLIL tears. The overall sensitivity was 79% for detecting SLIL tears in the axial plane versus 65% in the coronal plane. Although this number is not as high as the one reported by Potter et al. in 1997 (25), a more recent study by Moser et al. demonstrated only a combined sensitivity of 68% in two observers (26). Thus, our high sensitivity in only one plane demonstrates the possibility for higher sensitivity in diagnosing tears when both planes are used (as in normal clinical practice) without prejudice. Furthermore, all three observers demonstrated increased specificity, accuracy, negative predictive value, and positive predictive value when using the axial planes compared with the coronal planes.
The main strength of our study was the high percentage of participants with intact ligaments or with only partial thickness tears, as these are the source of greatest consternation in radiologic diagnosis. Full-thickness tears of the SLIL are relatively easy to diagnose with MRI. Moser et al. demonstrated 100% sensitivity for two observers compared with their combined sensitivity of 59% for two observers in detecting partial tears of the SLIL ligament (26). Identifying partial tears of the SLIL is crucial for the development of treatment algorithms (27).
Diagnosis of partial ligament tears non-invasively by MRI can benefit the patient two-fold. In the acute stage, it can direct the surgeon to conservative treatment such as casting, splinting, non-steroidal anti-inflammatory drugs, and physical therapy (28). If conservative treatment fails and/or the patient complains of persistent pain, invasive arthroscopic debridement for partial SLIL tears has been reported with success by several orthopedic hand surgeons (29). Weiss et al. reported satisfactory improvement in 11 of 13 patients (85%) at a mean follow-up of 27 months (30). In addition, Ruch and Poehling reported satisfactory improvement in all seven patients with partial SLIL tears, with no progression to instability at a minimum follow-up time of 2 years (29).
Thermal shrinkage has also been used as an adjunct to arthroscopic debridement (30). Daris et al. reported substantial pain relief in 14 of 16 patients treated with arthroscopic debridement and thermal shrinkage (31). Of 16 patients, eight were completely pain-free and no patients demonstrated signs of arthritis or instability during the follow-up period. Thus, accurate diagnosis of partial tears by MRI is critical and, to date, our study demonstrates the highest sensitivity in diagnosing partial SLIL tears in the axial plane. We propose that radiologists and orthopedists pay particular scrutiny of the axial planes to detect partial tears of the SLIL.
Another strength of our study was the fact that our reviewers were completely blinded to any clinical information about the participants. Previous unblinded studies have found relatively high specificity and accuracy in diagnosing SLIL tears when the radiologist had access to clinical details and/or surgical results (19). Although our study is unrepresentative of usual clinical practice where the radiologist is informed of the patient’s clinical information (and allowed access to different planes of imaging) it is successful in removing potential bias in reporting.
In clinical practice, additional images with positional changes of the wrist may allow better visualization of the SLIL, such as imaging with radial or ulnar wrist deviation (32). However, patients with an SLIL tear may be unable to perform such maneuvers because of pain or a “tight fitting” wrist coil.
Traditionally, MR arthrography has been reported as the most sensitive imaging modality in detecting SLIL injuries (33). However, there are circumstances where non-invasive or non-contrast studies are preferable, such as in patients with contrast allergy, end-stage renal disease, or in immunocompromised patients who are at greater risk of infection from the invasive procedure.
There are several limitations in our study. Although statistically significant, the retrospective nature and small sample sizes inherently limits the generalization of these findings. Thus, it is our opinion that larger scale prospective studies in the future should be performed to increase the statistical power of the results. Another limitation is the use of a 1.5T scanner at our institution. While 3T scanners are preferred at many centers, they are not yet widely available at all institutions. 3T MRI has been shown in the literature to have higher sensitivity, specificity, and accuracy than 1.5T MRI in detecting SLIL tears (34). Therefore, we believe our conclusion that axial images are better than coronal images in detecting SLIL would stand with 3T images, and no additional sequences would be preferable (34,35).
In conclusion, our study showed that partial SLIL tears could be successfully detected non-invasively with 1.5 T MRI when particular attention is paid to the axial plane. Orthopedists and radiologists can maximize their diagnostic performance with careful scrutiny of the axial planes and thus early diagnosis and development of appropriate treatment algorithms. It is our opinion that an otherwise normal study in a symptomatic patient should be further scrutinized and possibly performed again, if the axial sequence is degraded by motion or other MR artifacts. Furthermore, abnormal MR findings involving the SLIL detected on axial sequences should be considered clinically significant even in the absence of signal abnormality on corresponding coronal sequences.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.