
Abstract
Background
The number of computed tomography (CT) examinations is increasing and leading to an increase in total patient exposure. It is therefore important to optimize CT scan imaging conditions in order to reduce the radiation dose. The introduction of iterative reconstruction methods has enabled an improvement in image quality and a reduction in radiation dose.
Purpose
To investigate how image quality depends on reconstruction method and to discuss patient dose reduction resulting from the use of hybrid and model-based iterative reconstruction.
Material and Methods
An image quality phantom (Catphan® 600) and an anthropomorphic torso phantom were examined on a Philips Brilliance iCT. The image quality was evaluated in terms of CT numbers, noise, noise power spectra (NPS), contrast-to-noise ratio (CNR), low-contrast resolution, and spatial resolution for different scan parameters and dose levels. The images were reconstructed using filtered back projection (FBP) and different settings of hybrid (iDose4) and model-based (IMR) iterative reconstruction methods.
Results
iDose4 decreased the noise by 15–45% compared with FBP depending on the level of iDose4. The IMR reduced the noise even further, by 60–75% compared to FBP. The results are independent of dose. The NPS showed changes in the noise distribution for different reconstruction methods. The low-contrast resolution and CNR were improved with iDose4, and the improvement was even greater with IMR.
Conclusion
There is great potential to reduce noise and thereby improve image quality by using hybrid or, in particular, model-based iterative reconstruction methods, or to lower radiation dose and maintain image quality.
Introduction
The number of computed tomography (CT) examinations is increasing at radiology departments and, as a result, the collective effective dose received by patients is increasing. CT constituted 14% of radiological examinations and contributed 58% to the collective effective dose in Sweden in 2005 (1,2). Similar statistics are reported by the European Commission for the European population (3). Improving the image quality (e.g. reducing noise in the image) would enable a dose reduction for the most frequently used and highest dose CT procedures. Many steps have been taken to reduce the radiation dose in CT examinations, including improved detector sensitivity, an anti-scatter grid, and dose modulation (4). One important development in recent times has been the introduction of iterative reconstruction methods to replace the conventional filtered back projection (FBP) procedure. Several clinical studies have shown the potential of iterative reconstruction to improve image quality and thereby reduce the radiation dose while maintaining diagnostic acceptability (5–13).
Different CT manufacturers use different methods to reconstruct the images; statistical-based algorithms based on photon statistics and model-based algorithms that in addition attempt to model the system and the acquisition process (14,15). The iterative process can be performed on image data, projection (raw) data, or a combination of both (hybrid iterative reconstruction).
The main purpose of this study was to investigate variations in image quality parameters depending on the image reconstruction method and to discuss the possibility of lowering the patients’ total dose by using different iterative reconstruction models.
Material and Methods
Phantoms
Two different phantoms were used: an image quality phantom (Catphan® 600, The Phantom Laboratory, Greenwich, NY, USA) and an anthropomorphic torso phantom (CTU-41, Kyoto Kagaku Co., Ltd., Kyoto, Japan). The Catphan® phantom was scanned both with and without a 25–35 cm oval body annulus. The annulus was used to better simulate a patient’s shape and size.
Scan parameters
All phantom measurements were performed with a Brilliance iCT system (Philips Healthcare, Cleveland, OH, USA).
The Catphan® phantom was scanned in spiral mode using a body protocol with different dose levels (CTDIvol [32 cm phantom] = 25 mGy [100%], 17.5 mGy [70%], 10 mGy [40%], and 2.5 mGy [10%]). The collimation 128 × 0.625 and pitch of 0.6 were unchanged for all scans. The highest dose level was chosen to match the national reference dose level for an abdomen examination in Sweden (16). The 10 mGy level was chosen to match the clinical protocol used at the authors’ institution and the 2.5 mGy level resembles a low-dose protocol. Scanning was conducted with different tube voltages (80, 100, 120, and 140 kV). The dose modulation system was disabled.
The anthropomorphic phantom abdomen was scanned with a standard clinical abdomen protocol used at the authors’ institution. The settings were: 120 kV; 180 mAs; rotation time, 0.5 s; collimation, 128 × 0.6; and pitch, 0.993. The dose modulation system, Dose Right (ACS and Z-DOM), was activated. Acquisition was performed for different dose levels; first CTDIvol = 7.1 mGy (100%), and then mAs was lowered to 50% for a dose of 3.6 mGy. The third scan was a low-dose protocol at 100 kV, 57 mAs, with the other parameters identical to the standard protocol; this gave a dose of 30% or 2.3 mGy.
Reconstruction settings
Images of the Catphan® and the anthropomorphic phantom were reconstructed to 1, 3, and 5 mm slice thicknesses, increments of 1, 3, and 5 mm, and a 350 mm field of view. Filter B (soft) was used with FBP. Corresponding images were also reconstructed using the hybrid iterative reconstruction, iDose4 (SW version 3.2). The iDose4 reconstruction is available in seven different noise reduction levels. In the current study we used the lowest noise reduction level 1, and in addition two levels with stronger noise reduction, level 3, and 5, (iD L1, iD L3, and iD L5) (17). A soft reconstruction kernel, filter B, was used in all cases. Using an offline prototype system (release R07) located at site, images were also reconstructed with iterative model-based reconstruction (IMR) (18). On the prototype system several different reconstruction algorithms were available. For the Catphan® and for the abdominal reconstructions of the anthropomorphic phantom a soft tissue reconstruction algorithm was used to get optimal low-contrast. The algorithm is available with three different noise reduction levels: 1, 2, and 3, where level 3 is the highest noise reduction (IMR L1, IMR L2, and IMR L3). The IMR reconstruction time in the clinical system is claimed to be less than 3 min, dependent on the number of images. All levels were used and compared to iDose4 and FBP reconstructions.
Image quality assessment
Evaluation of the Catphan® images was performed using AutoQA Lite™ software (v. 2.3 2007 Iris QA, LLC, Frederick, MD, USA) and ImageJ software (v. 1.46 r, National Institutes of Health, Bethesda, MD, USA, http://imagej.nih.gov/ij/). CT numbers (Hounsfield unit, HU), noise, noise power spectra (NPS), low-contrast resolution, and spatial resolution (modulation transfer function, MTF) were determined. In addition to the objective measurements, a subjective evaluation of the low-contrast resolution was performed by three observers. All observers were medical physicists with 7–12 years of experience in evaluating this type of CT image.
The attenuation (HU) was measured for different materials in the Catphan® phantom using AutoQA Lite™. The HU value for each material was compared for the different reconstruction methods. The influence of the reconstruction method on the HU value was evaluated.
The image noise was determined as the standard deviation (SD) and was measured in the uniform module of the Catphan® phantom using a centrally placed region of interest (ROI) by AutoQA Lite™. The image noise was evaluated for all dose levels and for different reconstruction settings.
In addition, the NPS was calculated from the uniform module of the Catphan® phantom as

For the anthropomorphic phantom, the image noise was measured at different dose levels in the upper abdomen. The noise was measured in a ROI in the liver for different reconstruction methods.
The low-contrast resolution was assessed in two steps using the low-contrast module of the Catphan® phantom. The module contains three sets of outer supra-slice cylinders with a z-axis dimension of 40 mm, which (according to the manufacturer) have nominal contrasts of 1.0%, 0.5%, and 0.3% corresponding to a difference in HU value of 10, 5, and 3. Each set consists of nine cylinders with diameters in the range of 2–15 mm. The objective assessment was performed by measuring CT numbers (HU) and noise (SD) in identical ROIs placed in the largest cylinder in each of the three sets, as well as in the background (center of the phantom). The contrast-to-noise ratios (CNR) were calculated using the formula

A subjective assessment of all reconstructions was conducted in consensus by the same three observers as above. Two image quality criteria were assessed separately for each of the three sets of supra-slice cylinders: (i) smallest discernible cylinder, and (ii) smallest sharply defined cylinder. The images were presented individually in randomized order on a PACS workstation using the viewing and scoring software ViewDEX v2.0 (Viewer for Digital Evaluation of X-ray images) (20). As the absolute CT numbers varied slightly between reconstructions, the window level was adjusted for each reconstruction to match the mean attenuation in the homogenous background, while the window width was fixed at 80 HU.
For the anthropomorphic phantom, the CNR was calculated for the liver/vessel. A ROI was placed in the homogenous part of the liver in the same slice for all reconstructions, and a background ROI was placed in a vessel structure in the same slice of the phantom. The CNR was calculated for the liver/vessel for the 5 mm slices at different dose levels. These calculations were performed for the different reconstruction methods and noise reduction levels.
The spatial resolution was evaluated visually by determining the number of visible line pairs and, in addition, the MTF was determined for the wire insert in the Catphan® using AutoQA Lite™.
Results
CT numbers
Measured CT numbers (HU) in Catphan® for filtered back projection (FBP), iDose4 level 3 (iD L3), and iterative model reconstruction level 2 (IMR L2) at 120 kV. The maximum deviation was 2.7% between IMR and FBP, and 0.5% between iDose4 and FBP.

LDPE, Low-density polyethylene; PMP, polymethylpentene.
For the anthropomorphic phantom, the CT numbers were specified as follows: liver 70 HU, vena cava 40 HU, and soft tissue 8 HU (21). The measured CT numbers for the liver were 79/79/81 HU (FBP/iD L3/IMR L2), for the vena cava 39/39/40 HU, and for soft tissue 4/4/5 HU. These data showed no difference in CT number between FBP and iDose4, and a negligible difference compared to IMR. The difference between the measured and specified CT numbers could have been caused by the filtration of the X-ray beam and the reconstruction kernel.
Noise
Data for 120 kV were analyzed and the results for different dose levels (CTDIvol = 2.5, 10, 17.5, and 25 mGy) are given in Fig. 1. The data for all reconstruction methods are included. Compared to FBP, the noise was decreased by 10% for iDose4 level 1, 22% for level 3, and 35% for level 5. IMR decreased the image noise further compared to FBP; IMR level 1 reduced the noise by 60%, and levels 2 and 3 by 68% and 75%, respectively. The results were independent of dose.
Noise measured centrally in Catphan® at 120 kV for different dose levels (CTDIvol): 2.5, 10, 17.5, and 25 mGy. Images were reconstructed with filtered back projection (FBP); iDose4 levels 1, 3, and 5 (iD L1-5); and iterative model reconstruction levels 1, 2, and 3 (IMR L1-3).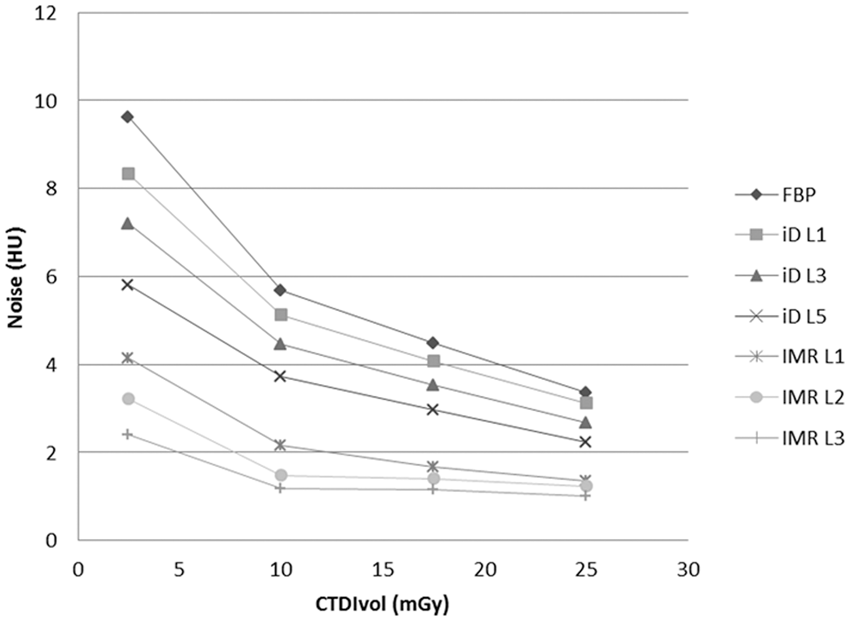
Scanning the Catphan® with the body annulus resulted in generally much noisier images than scanning without the annulus. For the lowest doses and for 80 kV, artifacts from the body annulus were seen in the images in some cases. The noise reduction for the 120 kV scans for the Catphan® with body annulus followed the same pattern as occurred when scanning the phantom without annulus. The noise reduction for the phantom with and without annulus by IMR was similar (data not shown).
With iDose4, the noise reduction with level 1 and 3 was more pronounced with annulus than without annulus. This might be due to the artifacts in these cases, therefore the accuracy of the data is reduced and the results are uncertain.
The image noise measured in the liver of the anthropomorphic phantom was significantly decreased with the iDose4 reconstruction compared to FBP (Fig. 2). Measurements of the image noise show that the thinner slices with IMR result in lower noise than the thicker slices with iDose4. IMR provides only a small reduction in noise when thicker slices are used; this reduction is less for higher levels of IMR. There was a pronounced decrease in noise with IMR. For both the 5 and 1 mm slices, the noise level was decreased to levels below 10 HU (data for the 1 mm slice thickness are not shown).
Noise measured in liver left panel in anthropomorphic phantom at 120 kV for different dose levels (CTDIvol): 2.3, 3.6, and 7.1 mGy. Images of 5 mm were reconstructed with filtered back projection (FBP); iDose4 levels 1, 3, and 5 (iD L1-5); and iterative model reconstruction levels 1, 2, and 3 (IMR L1-3).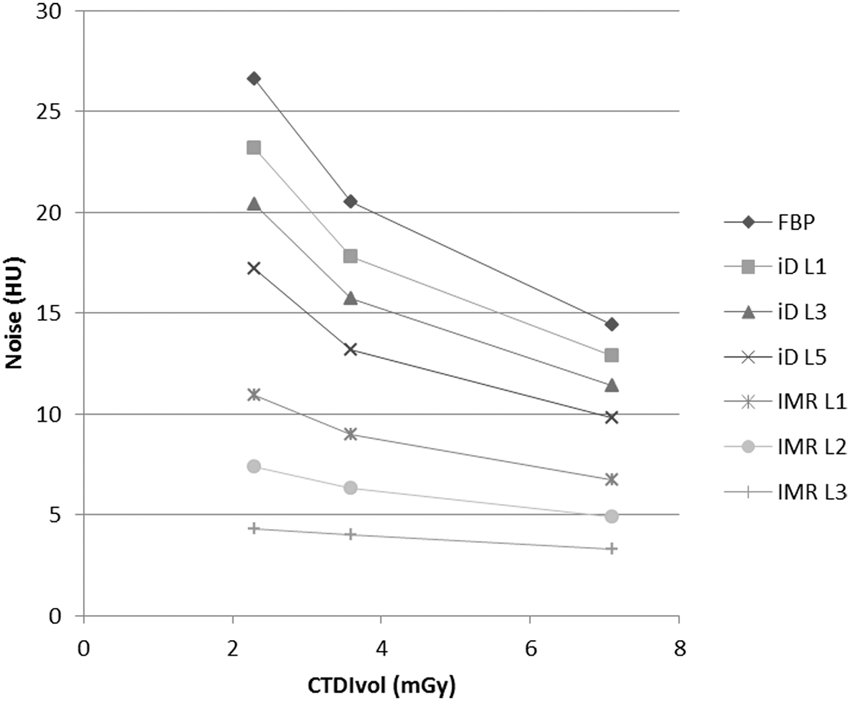
Noise power spectrum
The NPS for FBP, iDose4 level 3, and IMR level 2 at 120 kV and 10 mGy are shown in Fig. 3. The amplitude of the curve is related to the amount of noise, and the shape of the curve illustrates the characteristics of the image noise. The NPS for iDose4 has a similar shape as the one for FBP. The NPS of IMR was lower and the shape of the curve differs from that for iDose4 and FBP.
Noise power spectra (NPS) after scanning the Catphan® phantom with body annulus at 120 kV and 10 mGy, and reconstructing the images with filtered back projection (FBP), iDose4 level 3 (iD L3), and iterative model reconstruction level 2 (IMR L2). The curve form represents the distribution of noise (y-axis) as a function of spatial frequency (x-axis). Higher curves imply more noise.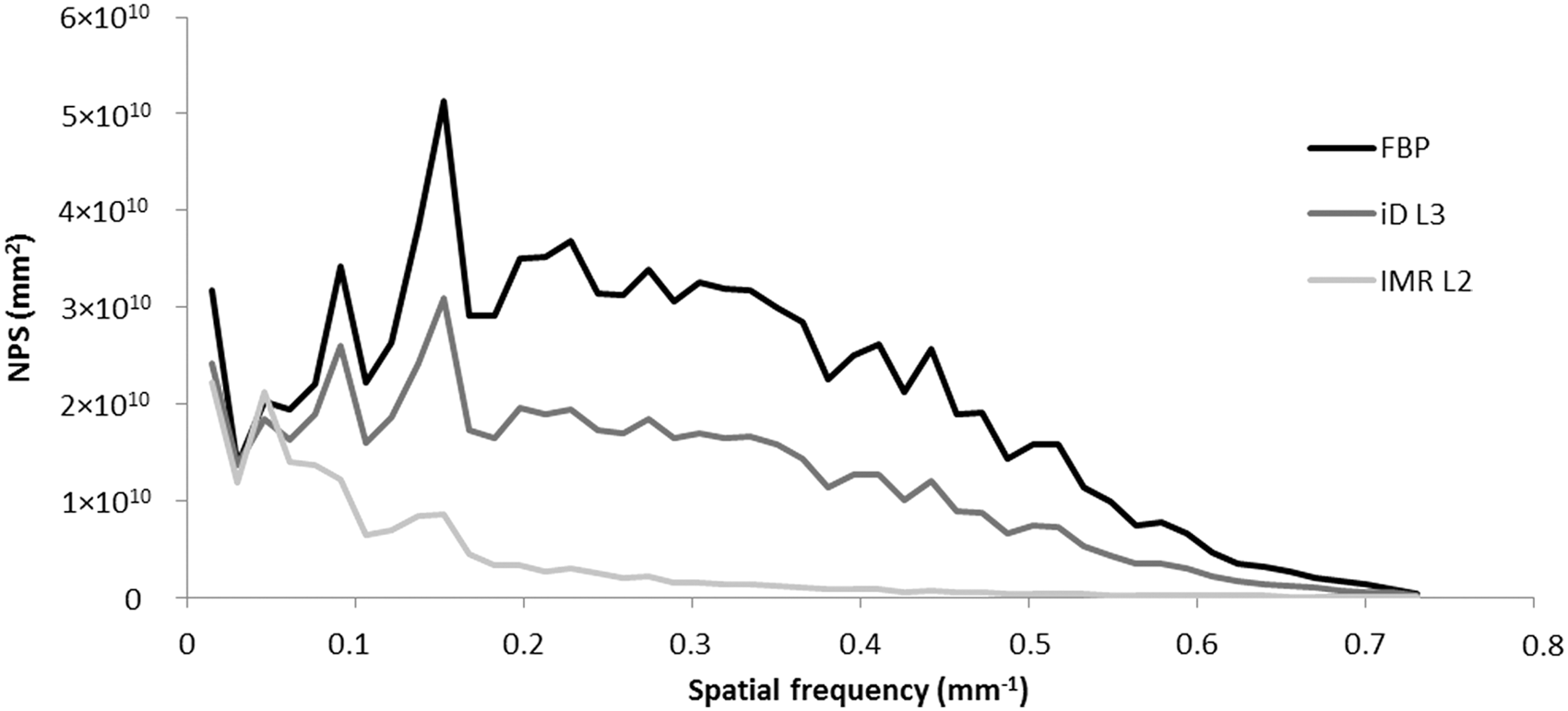
The shape of the NPS was dependent on the IMR level. The largest difference between FBP and IMR was at level 3, which also had the most noise reduction. The difference in these characteristics is also seen in images of the anthropomorphic phantom (Fig. 4). FBP and iDose4 images have a coarse graininess and IMR images are smoother.
Anthropomorphic phantom reconstructed with different reconstruction methods. (a) filtered back projection (FBP), (b) iDose4 level 3 (iD L3), (c) iterative model-based reconstruction level 2 (IMR L2), (d) IMR L3.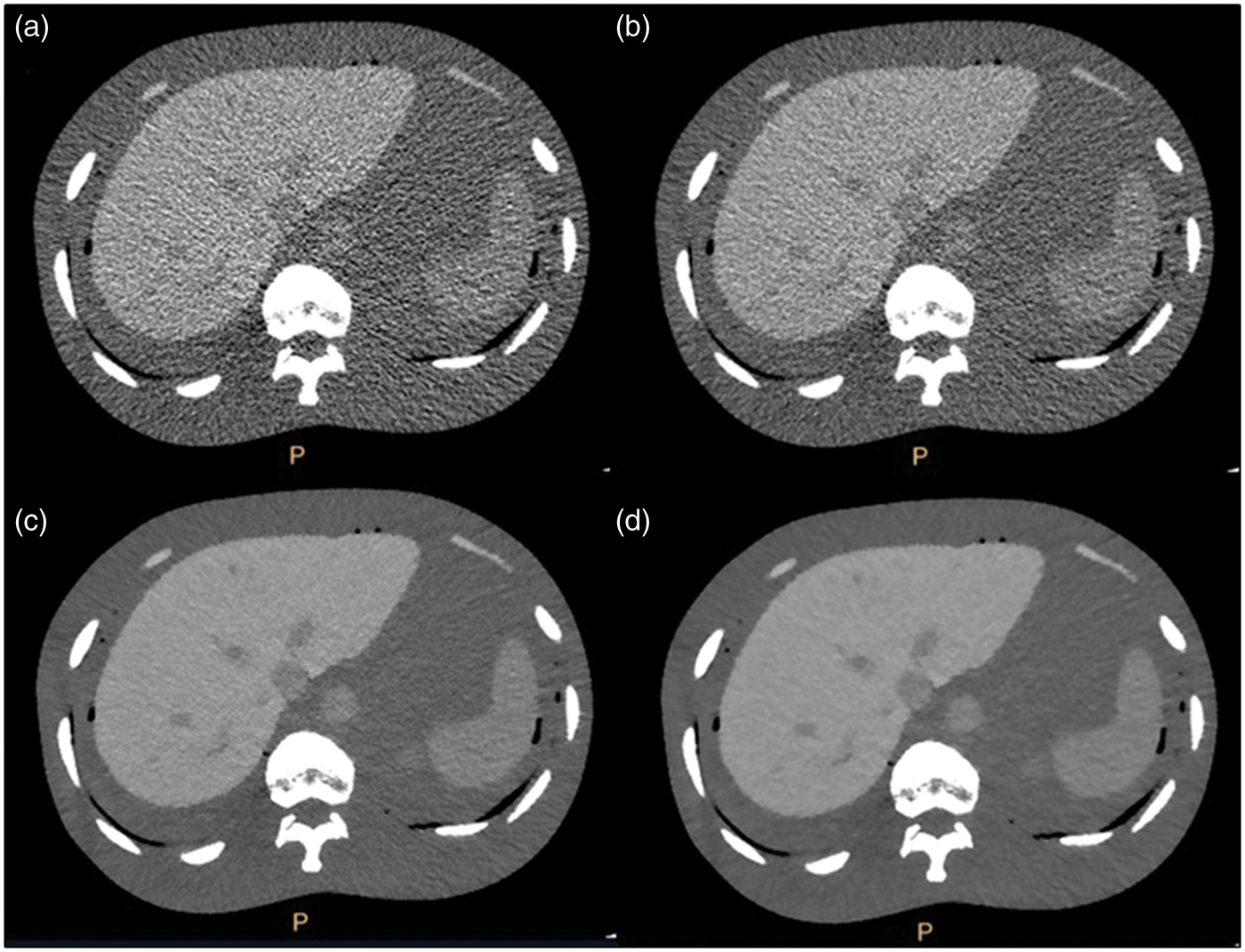
Objective low-contrast resolution
Cumulative CNR results for all three contrast levels (0.3%, 0.5%, and 1.0%) and for 10 mGy and all combinations of kV and reconstruction algorithm are shown in Fig. 5. The results showed that increasing the iDose4 level improved the low-contrast resolution; additional improvement was achieved with IMR. Equivalent results with a higher level of iDose4 and IMR were found when scanning with the body annulus. The highest cumulative CNR was achieved at 120 kV.
Objective evaluation of low-contrast resolution in Catphan® with body annulus. Cumulative contrast-to-noise ratios (CNRs) from all three contrast levels (0.3%, 0.5%, and 1.0%), for 10 mGy and all combinations of kV and reconstruction algorithms: filtered back projection (FBP); iDose4 levels 1, 3, and 5 (iD L1-5); and iterative model reconstruction levels 1, 2, and 3 (IMR L1-3).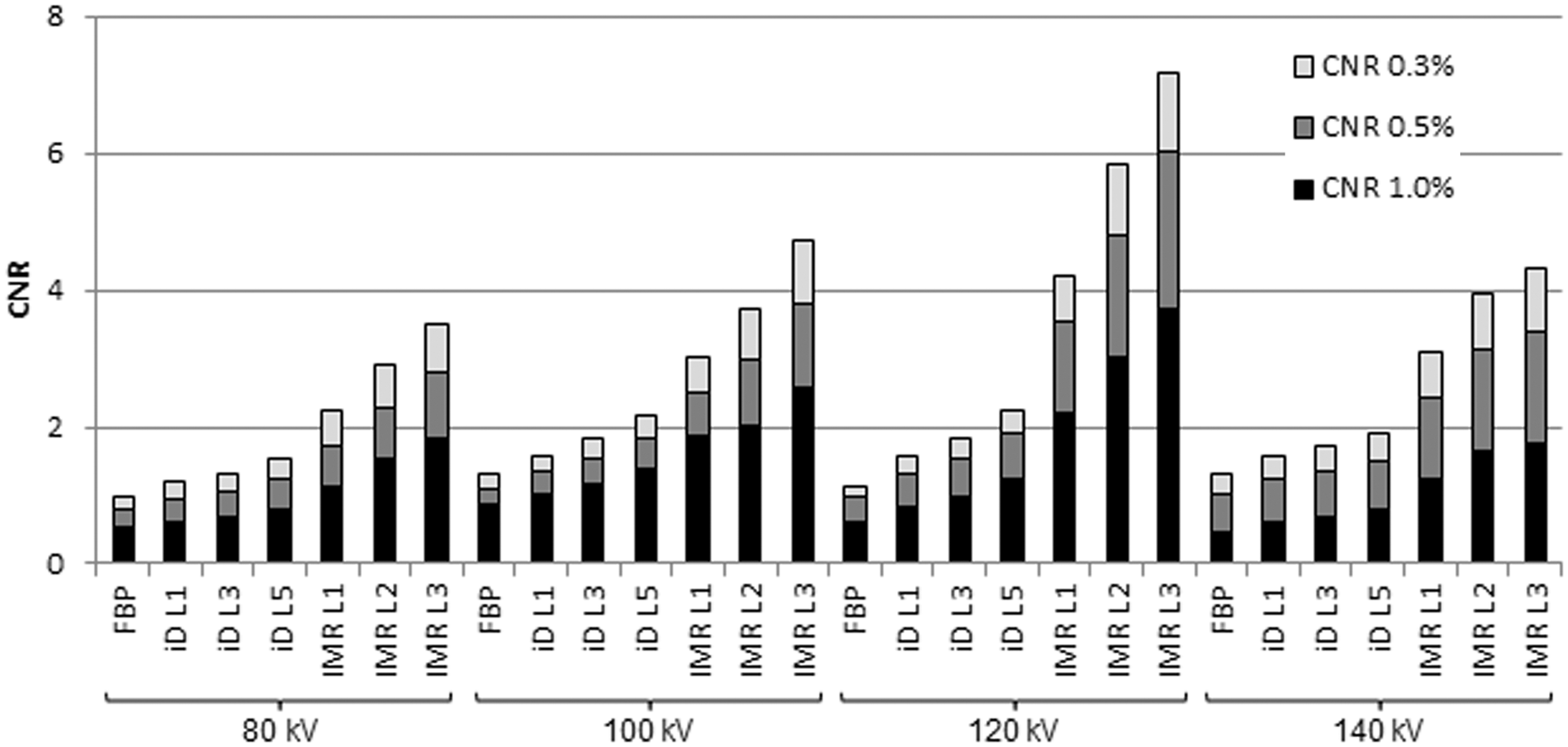
The CNR of liver/vessel in the anthropomorphic phantom for 5 mm slices is presented in Fig. 6. For IMR at the highest level of noise reduction (IMR L3), the CNR was about four times higher than for FBP, and about three times higher than for iDose4 level 2. An even higher improvement in the CNR of IMR compared to both iDose4 and FBP was seen with thin 1 mm slices (data not shown). The same trend was seen for all dose levels.
Objective contrast-to-noise ratio (CNR) for liver/vessel in the anthropomorphic phantom for 5 mm slices and for different reconstruction methods and noise reduction levels. Data are shown for the three different dose levels (CTDIvol of mGy) used in the abdominal scan and all combinations of reconstruction algorithms: filtered back-projection (FBP); iDose4 levels 1, 3, and 5 (iD L1-5); and iterative model reconstruction levels 1, 2, and 3 (IMR L1-3).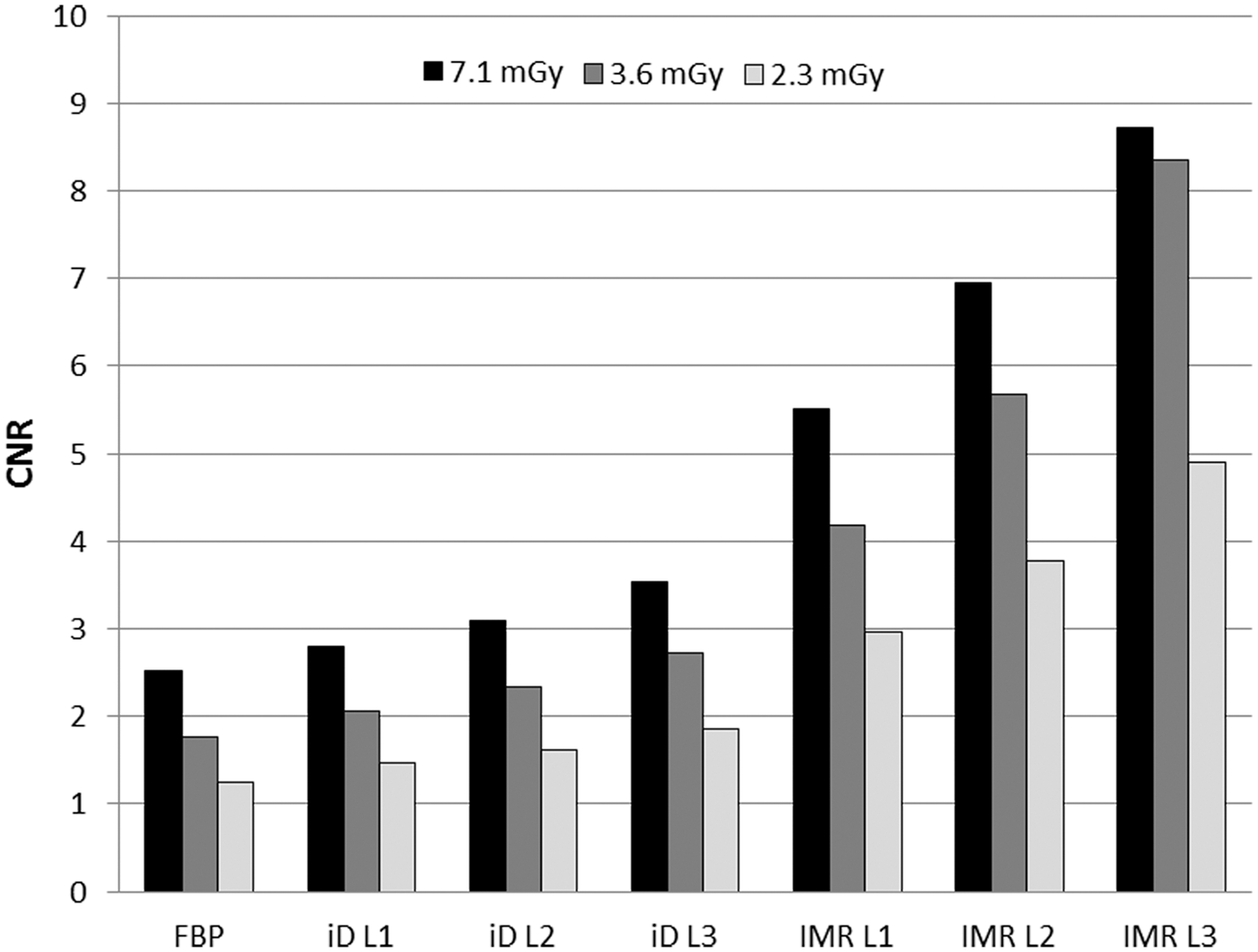
Subjective low-contrast resolution
The cumulative representation of the number of sharply defined and discernible cylinders at three nominal contrast levels is presented in Fig. 7. The trend shows that the subjective visibility increased with radiation dose up to 17.5 mGy and with higher levels of iDose4 and IMR. There was also a trend that IMR reproduced more sharply defined and discernible objects at the same dose level compared to iDose4. There was no further increase in the number of sharply defined and discernible objects at 25 mGy compared to images with lower doses.
Subjective evaluation of low-contrast resolution in Catphan® without body annulus. Cumulative representation of the number of (a) sharply defined and (b) discernible cylinders at three nominal contrast levels (0.3%, 0.5%, and 1.0%), at four radiation dose levels (CTDIvol of mGy) at 120 Kv, and all combinations of reconstruction algorithms: filtered back-projection (FBP); iDose4 levels 1, 3, and 5 (iD L1-5); and iterative model reconstruction levels 1, 2, and 3 (IMR L1-3).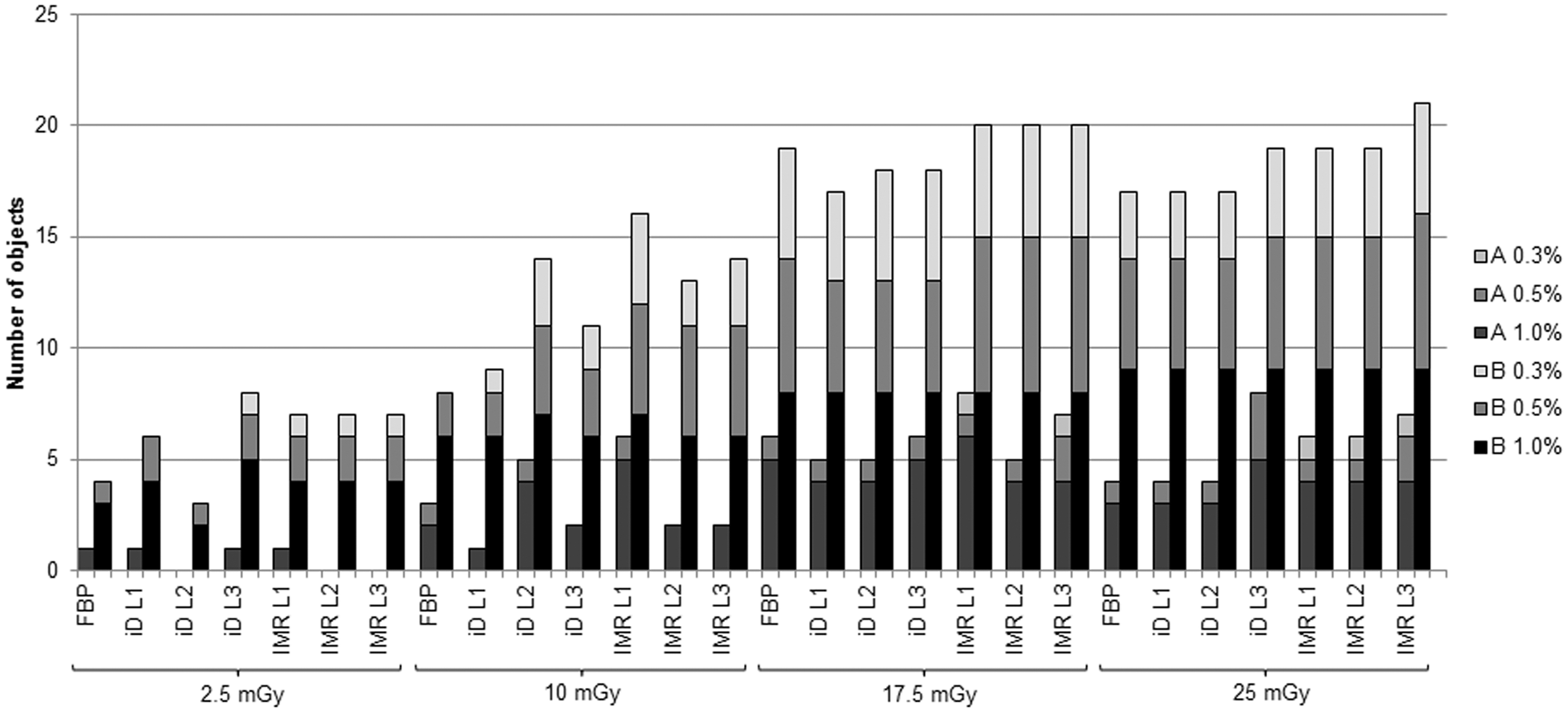
Spatial resolution
The spatial resolution was evaluated for the Catphan® phantom with and without body annulus. Visual inspection and analysis of the images showed that the iDose4 reconstruction did not change the resolution compared to FBP. With IMR, the resolution was improved.
Spatial resolution characterized as a modulation transfer function (MTF 10%) for the different reconstruction methods at 120 kV at 10 mGy, using the Catphan® phantom with and without body annulus. Values represent frequency (lp/cm), and higher values indicate improved spatial resolution.
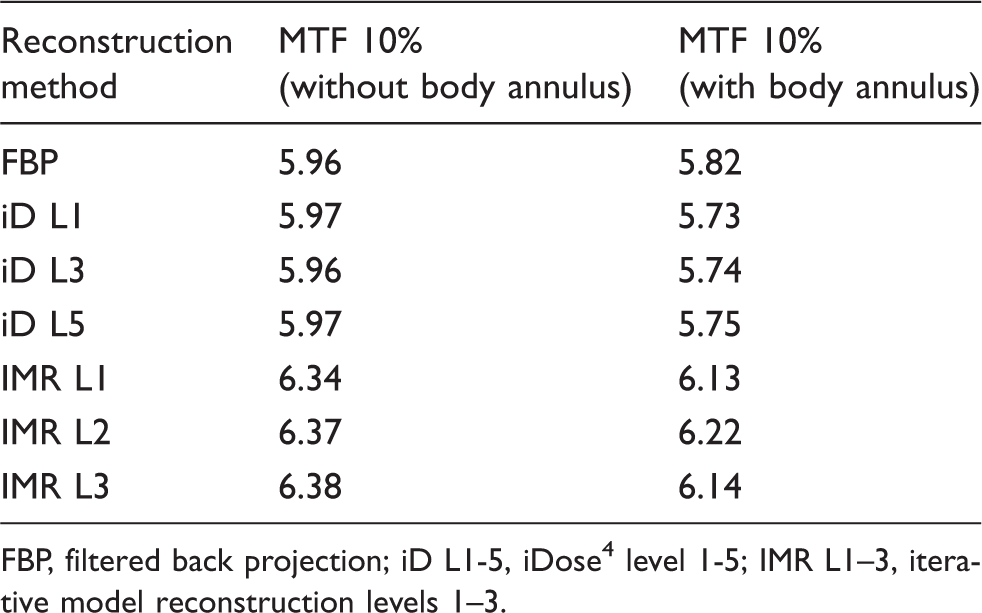
FBP, filtered back projection; iD L1-5, iDose4 level 1-5; IMR L1–3, iterative model reconstruction levels 1–3.
Discussion
Improvements to image quality, such as a reduction of noise, are a prerequisite for lowering a patient’s radiation dose. Other important parameters include low-contrast detectability and spatial resolution. The low-contrast resolution is a critical parameter, e.g. in brain and liver examinations, as it is vital for diagnosis and normally requires high doses. In the current study, image quality parameters were tested on two different phantoms: an image quality phantom and an anthropomorphic torso phantom. The image quality phantom gives an indication of how the image quality is affected by an iterative reconstruction method, and it provides the opportunity to measure any changes. Using an anthropomorphic phantom enables the scan and measurements to occur in a more patient-like situation. The anthropomorphic phantom corresponds to a rather small patient (a man of approximately 60 kg), and also affects the radiation dose for the standard abdomen protocol. The CTDIvol for the standard abdomen protocol is 10 mGy, and for the anthropomorphic phantom the dose was reduced to 7.1 mGy because automatic exposure control was used.
The hybrid and model-based iterative reconstructions did not affect the CT numbers. This is in agreement with published data (18).
The noise reduction obtained using iterative reconstruction is especially important in cases where it is desirable to reduce the dose to the patient. Our results are in good agreement with other studies performed in this field (5,8,13). Images reconstructed with thin slices and IMR result in lower noise than images using thicker slices with iDose4. IMR provides only a small noise reduction when thicker slices are used, and this reduction is less for higher levels of IMR. These results were also shown in a previous study (22).
For a more patient-like situation, simulated by Catphan® with body annulus, a major reduction in the noise occurred, resulting in clinically relevant noise levels even with a low dose protocol. There is considerable potential to reduce the noise and thereby improve the image quality using iterative reconstruction methods. This can be used to lower the radiation dose while maintaining image quality, or to maintain the radiation dose and improve image quality.
The shape of the NPS curve for iDose4 was similar to the shape of the NPS curve for FBP, although the amplitude was lower, demonstrating reduced noise. With a higher level of iDose4 the amplitude was further decreased. This explains the different expression that occurs with images at a high level of iDose4. The NPS curves for IMR differ from both FBP and iDose4. This can explain the “unnatural” image quality compared to FBP and iDose4. IMR and iDose4 also reduce image artifacts, such as streak artifacts that are common in images reconstructed with FBP. Due to the changes in NPS by the IMR, the perception of the image is influenced by the level of noise reduction (IMR level). With increasing noise reduction (higher noise reduction level) the NPS shift is more pronounced and this may initially affect the choice of noise reduction level. The images become smoother and may get a mottled appearance. An approach with stepwise introduction of dose reduction/noise reduction is recommended.
Our study showed that iterative reconstruction iDose4 improves the low-contrast resolution compared with FBP. With IMR a further improvement is seen. The most important gain with soft tissue IMR algorithm is the reduced noise and the improved low-contrast resolution. The main clinical improvement will be the possibility to reduce dose and improve low-contrast resolution in liver and abdominal scans as well as for other low-contrast scanning, such as brain scan. For the phantom used in the study, it was possible to reduce the dose from 25 mGy to 10 mGy while maintaining or even improving the low-contrast resolution.
The CNR of liver/vessel in the anthropomorphic phantom showed improvement in the CNR with IMR compared to both iDose4 and FBP. An even greater improvement was seen for the thin slices (1 mm). The same trend was seen at all dose levels. The same results for thinner slices have been shown in previous studies (22).
The subjective assessment of the low-contrast resolution revealed that IMR produced more sharply defined and discernible objects than iDose4 at the same dose level. The trend was that the visibility increased with radiation dose up to 17.5 mGy. At higher dose levels there was no further increase in visibility. This effect could be explained by the shape of the NPS curve, which shows that iDose4 and especially IMR have less high-frequency noise than FBP.
iDose4 did not affect the spatial resolution compared to FBP, whereas a small improvement was seen with IMR. If a sharper filter is used with iDose4, then the resolution can be improved as demonstrated in previous studies (23,24).
Some limitations of the study were that the phantom was only scanned once and that different reconstruction methods were applied to this scanned image set. This means that the uncertainty cannot be estimated based on the results. The ROI has the same size and is automatically placed at the same location in the images. We did not scan the phantoms multiple times with the same settings, which would have allowed us to estimate measurement uncertainties. The automatic evaluation of image quality used in this study generates identical results when applied repeatedly to the same raw data and images. Variations between repeated scans with identical parameters in modern CT systems are very small, and thus variations are caused by any inconsistency in the signal chain. This inconsistency would not be large enough to affect the relationship between the image quality parameters and the radiation dose. The current study is limited by the phantom size used, and further phantom or patient cases for different patient sizes needs to be included for a full understanding of the full potential with iterative reconstruction methods.
In conclusion, all image quality parameters were positively affected when using iterative reconstruction methods. Using IMR resulted in improvements in all image quality parameters compared to iDose4 and FBP. The decreased noise and increased low-contrast resolution by iDose4 and IMR may improve detectability in a clinical situation.
Footnotes
Acknowledgements
Professor Mats Nilsson, Skåne University Hospital for assistance with NPS evaluation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Ydström is a former employee of Philips Healthcare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Region Sk䭥 (Skane County Council's Research and Development Foundation).