
Abstract
Background
Hepatic venous outflow is important for graft survival in living donor liver transplantation (LDLT). If hepatic venous outflow obstruction occurs, hepatic vein stenting is considered to restore the patency.
Purpose
To retrospectively evaluate the efficacy and patency of primary hepatic vein stenting for hepatic venous outflow obstruction (HVOO) after LDLT.
Material and Methods
Percutaneous interventions, including hepatic vein stent placement with or without balloon angioplasty, were performed in 21 patients who had undergone LDLT and had HVOO confirmed through hepatic venography or manometry, including the patients who had a structural abnormality. Two stents each were inserted in four patients; therefore, the total number of treated anastomoses was 25. Technical success, patency rates, and pressure gradients between hepatic veins and the right atrium were evaluated in 19 patients each.
Results
Technical success was achieved in 25 of 26 vessels (96%). The mean interval between operation and stenting was 43 days. After the procedure, the follow-up period was a mean 530 days. The mean pressure gradient decreased from 8.5 mmHg to 2.1 mmHg after treatment (P < 0.01). The patency rates of the 25 vessels were 80% at 1, 2, and 3 years after stent placement. However, middle hepatic vein stenting revealed a low patency rate (all were 36%). Three of seven stents (43%) in the middle hepatic vein occluded during follow-up.
Conclusion
Percutaneous primary hepatic vein stent replacement is an effective treatment for HVOO after LDLT.
Introduction
Living donor liver transplantation (LDLT) is a therapeutic option for liver disease, mainly for hepatocelluar carcinoma or terminal liver cirrhosis from any cause (hepatitis B, hepatitis C/non-A, non-B, alcoholic, autoimmune, and others), and is a method for overcoming graft shortage in adult patients. However, there are some difficulties in LDLT because of multiple anastomoses, including in the hepatic veins. The patency of hepatic venous outflow is important to graft survival. Reported incidences of hepatic venous outflow obstruction (HVOO) after LDLT are in the range of 3.9–16.6% (1–4). Clinical manifestations of HVOO are non-specific but may include abnormal liver function, hepatomegaly, ascites, pleural effusion, and lower-extremity edema (1,4,5). In the immediate postoperative period, HVOO can be devastating and result in loss of graft and the patient’s life.
Percutaneous intervention has been recently accepted as the initial treatment for various liver transplant-related complications such as HVOO (6–11). Moreover, it has been reported that percutaneous intervention is safe and effective (1,5,6). Primary stent placement may be an effective treatment modality with an acceptable long-term patency to manage early post-transplant HVOO (12). However, there have been few reports on the outcomes of primary hepatic vein stenting for HVOO after LDLT, based on computed tomography (CT) findings, after LDLT in early-onset (≤28 days) or late-onset (>28 days) HVOO.
Our study aimed to assess the efficacy and patency of primary hepatic venous stent placement for HVOO after LDLT. CT was used to diagnose HVOO and perform follow-up evaluations after hepatic vein stenting.
Material and Methods
Patient population
Between October 2010 and December 2013, liver transplantation was performed at our institution in 131 adult patients (age >18 years), among which were 79 LDLT patients. Routine CT was performed every week during hospitalization and at 1, 3, 6, and 12 months after discharge. Of these 79 patients, 27 were suspected to have HVOO during the postoperative follow-up period based on CT findings of a non-opacified hepatic vein or focal luminal narrowing >50% at the hepatic vein’s anastomotic site compared with the adjacent normal hepatic venous diameter (11). A decreased, mottled, reticulated, or mosaic pattern of parenchymal contrast enhancement, especially in the periphery, was defined as abnormal. The CT images were evaluated in consensus by two abdominal radiologists, JWL and TUK, who had 20 and 5 years of experience, respectively. HVOO was confirmed by hepatic venography and manometry and was defined as stasis of the contrast medium from anastomotic obstruction on venography or a pressure gradient across the stenosis between the distal hepatic vein and the right atrium that was >5 mmHg. In this way, 22 of 27 patients were confirmed to have HVOO and received right liver lobes. However, in one patient, intraoperative stenting was performed first because of selection failure resulting from a thrombotic occlusion, and as a result, this patient was excluded, and 21 patients were included in the study’s final cohort. Two cases (not related to this study cohort) of significant portal vein stenosis (>50%) occurred in donors of LDLT (n = 79), but they were treated successfully by balloon angioplasty alone or stenting. The demographic data of these 21 patients are summarized in Table 1. The inclusion criteria are shown in Fig. 1.
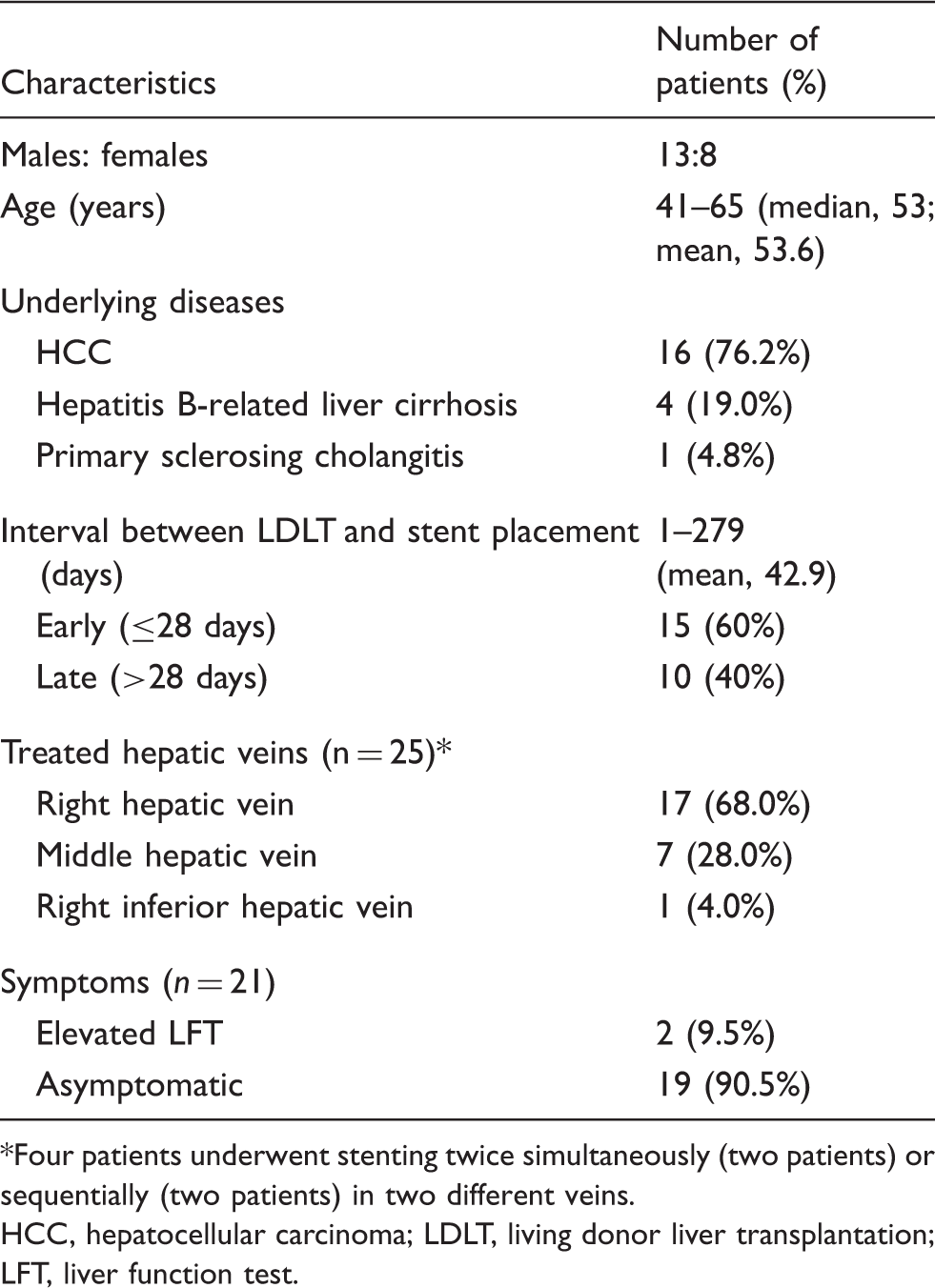
Inclusion criteria of patients. 1)A non-opacified hepatic vein or focal luminal narrowing >50% at the hepatic vein’s anastomotic site compared with the adjacent normal hepatic venous diameter on CT; 2)stasis of the contrast medium from anastomotic obstruction or complete thrombotic occlusion on venography; 3)pressure gradient across the stenosis between the distal hepatic vein and the right atrium that was >5 mmHg on manometry; 4)structural abnormality such as vascular kinking or extrinsic compression from enlarged graft, but pressure gradient was ≤5 mmHg; 5)no abnormal finding on hepatic venography or manometry and no structural abnormality. CT, computed tomography; HVOO, hepatic venous outflow obstruction; intraop., intraoperative; LDLT, living donor liver transplantation; LT, liver transplantation; pts, patients. Demographic data of 21 patients. Four patients underwent stenting twice simultaneously (two patients) or sequentially (two patients) in two different veins. HCC, hepatocellular carcinoma; LDLT, living donor liver transplantation; LFT, liver function test.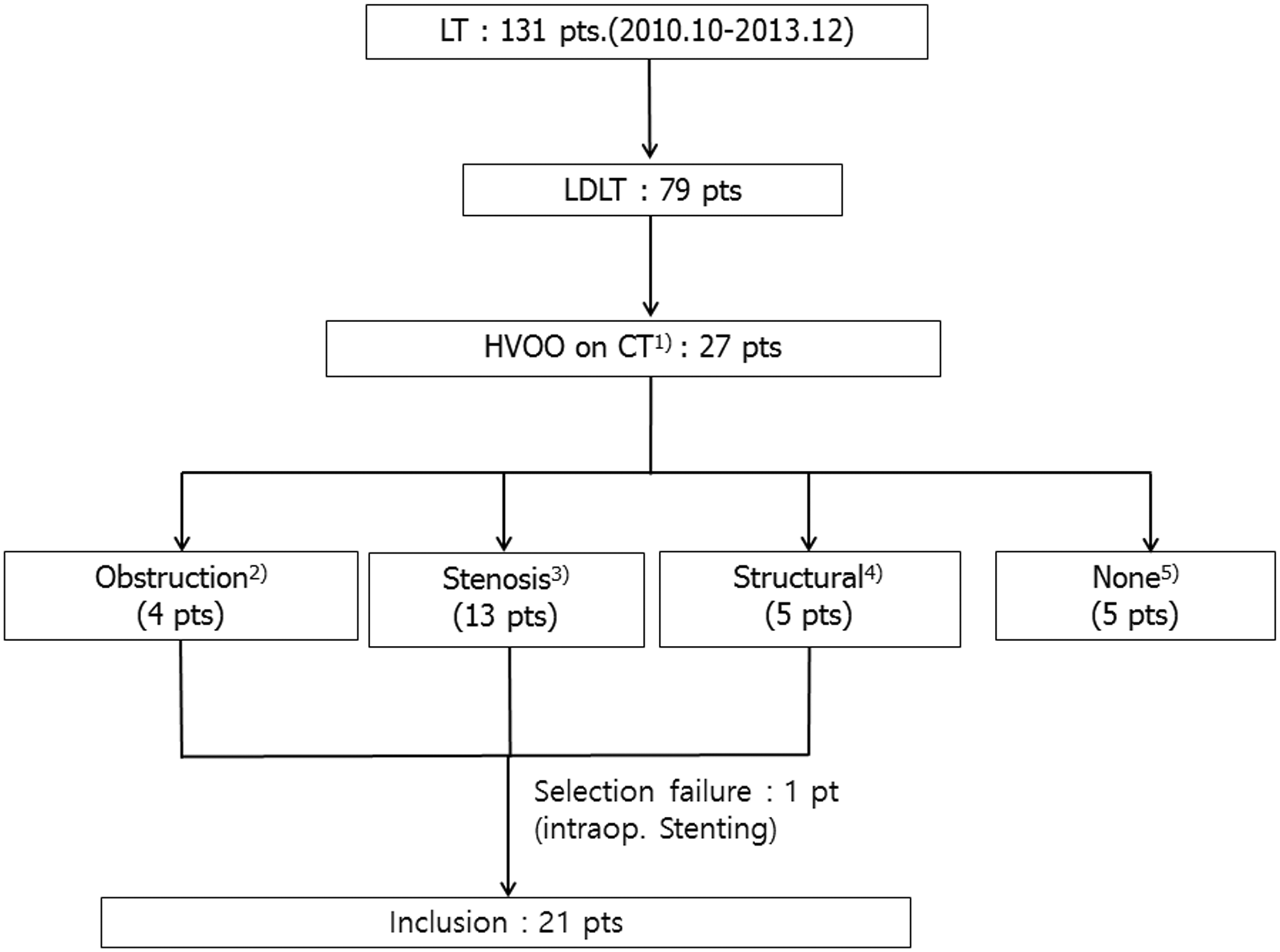
All 21 patients underwent primary hepatic vein stenting with or without balloon angioplasty. Of the 21 patients, four underwent stenting twice simultaneously (two patients) or sequentially (two patients) in two different veins. As a result, 25 anastomoses were treated. The mean interval between the LDLT and the stenting ranged from 43 days (range, 1–279 days). Fifteen of 25 vessels were in the early stage (≤28 days) when the stents were placed.
Procedures
One author with 8 years of experience in interventional radiology (UBJ) performed the procedures. Percutaneous interventions were performed using local anesthesia in all patients. Selective hepatic venography and stent placement were performed from the right internal jugular vein in all patients (n = 25). A 0.035-inch hydrophilic guide wire (Terumo, Tokyo, Japan) and a 5F Cobra catheter (Cook, Bloomington, IN, USA) were used to select each hepatic vein. The pressure gradient across the anastomosis was obtained in most patients, but if the venogram exhibited definite hepatic vein stenosis with flow stasis or an obviously normal hepatic vein without flow disturbance, measurement of the venous pressure gradient was omitted, except for those with thrombotic occlusion or definite stagnation of contrast medium. Primary stent placement was then performed with a Zilver (Cook), Smart (Cordis, Miami Lakes, FL, USA), Hercules (S&G Biotech Inc., Seongnam, Republic of Korea), Complete SE (Medtronic Inc., Minneapolis, MN, USA), Protégé (Covidien, St. Paul, MN, USA), or Epic (Boston Scientific, Natick, MA, USA) stent. The stents were 8–16 mm in diameter and 3–12 cm long. To minimize the risk of migration, the stent diameter in each case was intentionally oversized at approximately 1–2 mm with respect to the measured normal hepatic vein diameter adjacent to the stenosis. Following stent placement, a repeat hepatic venogram and pressure gradient were obtained. In 10 cases, immediate balloon angioplasty was performed following stent placement because of underexpanded stents that were <50% of their normal diameter or because the pressure gradient across the stenosis was >5 mmHg. In one case, a stent was immediately replaced in the same vein because the first one had migrated. Anticoagulants were not administered to any patients during or following the procedures.
Procedures were considered an immediate technical success when the hepatic venogram revealed alleviation of the hepatic venous anastomotic stenosis with fluent flow of contrast medium through the hepatic venous anastomosis and the pressure gradient across the stenosis was <5 mmHg.
Follow-up
Patient follow-up examinations were performed using CT in all cases (n = 21). Patients usually underwent CT within 1 week after stent placement and then at 1-, 2-, and 3-month intervals after discharge. According to clinician discretion, however, the follow-up schedule could be altered. The first follow-up CT examination was performed a mean 11.6 days (range, 0–54 days) after the procedure. In addition, hepatic venography was performed when CT showed suspected HVOO. The mean follow-up duration was 530 days (range, 4–1146 days). The following parameters were documented retrospectively: technical success, pressure gradient across the stenosis before and after the procedure, and the duration of stent patency.
Statistical analysis
Cumulative primary stent patency rates of stent-inserted hepatic veins (total and early- vs. late-onset HVOO) were calculated using the Kaplan–Meier method. A log-rank test was used to compare patency rates between patients with early- and late-onset HVOO. The Wilcoxon rank test was used to compare the pre- and postprocedural pressure gradients across the hepatic vein stenosis on hepatic venography. Sensitivity and positive predictive value of CT for HVOO were calculated. Values of P < 0.01 were considered statistically significant. SPSS version 18.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
Results
Twenty-six stents were successfully placed in 25 vessels in 21 patients (two vessels each in four patients). In one patient, the first stent was placed successfully across the stenosis. However, stent migration into the distal vessel occurred simultaneously in one patient; therefore, a second stent was placed to overlap the first stent and anastomosis. After second stent placement, hepatic venous outflow was improved and the pressure gradient decreased to 2 mmHg. In one patient, intraoperative stenting was performed first because of selection failure that resulted from a thrombotic occlusion (previously mentioned in materials and methods section). Thus, technical success was achieved in 25 of 26 vessels (96%). There were no procedure-related complications.
The pressure gradient was measured in 19 vessels but not in those with thrombotic occlusion (n = 4) or definite stagnation of contrast medium before the procedure (n = 2). Postprocedural pressure gradient was measured in 19 anastomoses but not in those patients with definite relief of stagnation. The preprocedural and postprocedural pressure gradients across stenoses were 3–15 mmHg (mean, 8.5 ± 3.8) and 1–5 mmHg (mean, 2.1 ± 0.9), respectively (P < 0.001). The preprocedural pressure gradient was <6 mmHg in five cases; however, these patients also underwent stent placement prophylactically because of kinking at the anastomotic sites on coronal CT images.
The mean follow-up period was 530 days (range, 4–1146 days), and the mean duration of stent patency was 440 days (range, 4–1146 days). The cumulative patency rates of the 25 stent-inserted hepatic veins are shown in Fig. 2. The overall 1-, 2-, and 3-year patency rates were 80%. The initial decrease in patency rates occurred within 1 year after stent placement, and no further decrease in patency rates occurred during the long-term follow-up period. A low patency rate was seen in patients with middle hepatic vein (MHV) stenting: four of seven stents (57%) in the MHV occluded during follow-up (Fig. 3). Notably, there were four cases of initially occluded hepatic veins in this study, but this patient group was too small for statistical analysis. Also, a comparison of the patency among patients with early-onset (≤28 days, n = 15) onset and late-onset (>28 days, n = 10) HVOO was performed, and the overall 1-, 2-, and 3-year patency rates of early- vs. late-onset HVOO were 87.5% and 70%, respectively (Fig. 2). There were no statistically significant differences in patency of the stents between the two groups (log-rank test, P = 0.18).
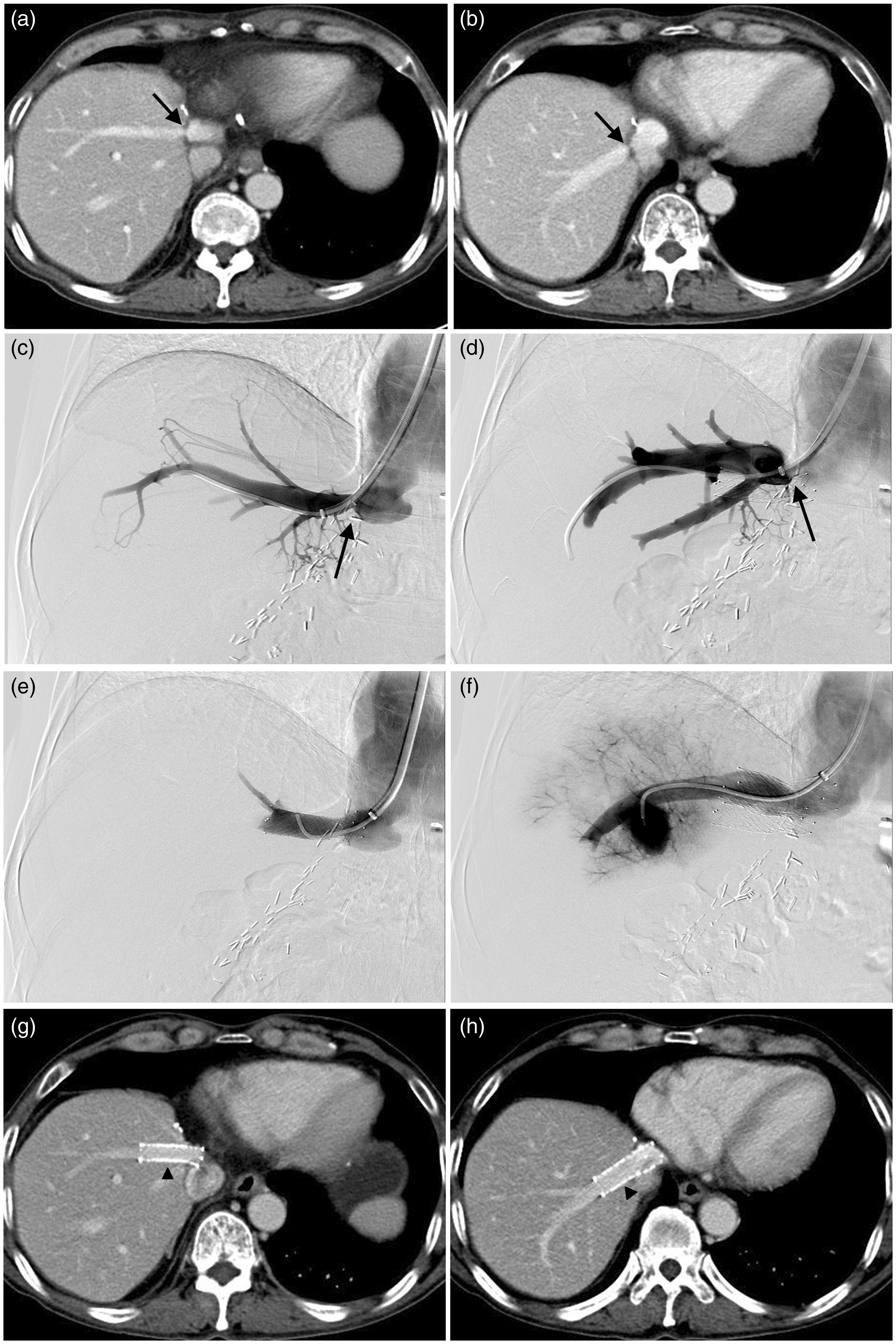
Kaplan–Meier results on cumulative primary stent patency rates of total vessels (middle line, n = 25), early (≤28 days, upper line, n = 15) and late onset (>28 days, lower line, n = 10) HVOO, requiring endovascular treatment. An initial decrease in patency rates occurred within 1 year after stent placement. Further decreases in patency rates did not occur during the long-term follow-up period. There were no statistically significant differences in patency of the stents between the two groups (early- vs. late-onset HVOO, log-rank test, P = 0.18). A 60-year-old man underwent right lobe living donor liver transplantation. The axial computed tomography images on postoperative day 65 reveal middle (a) and right (b) hepatic venous anastomotic stenosis (arrow). Three days later, the venograms in the middle (c) and right (d) hepatic veins showed definite focal stenosis at the anastomotic site (arrow). Just after the stent insertion, venograms demonstrated relief of anastomotic stenosis at the middle (e) and right (f) hepatic veins. Axial CT obtained 31 months after stent placement still revealed the patent stent in the middle (g) and right (h) hepatic veins (arrowhead).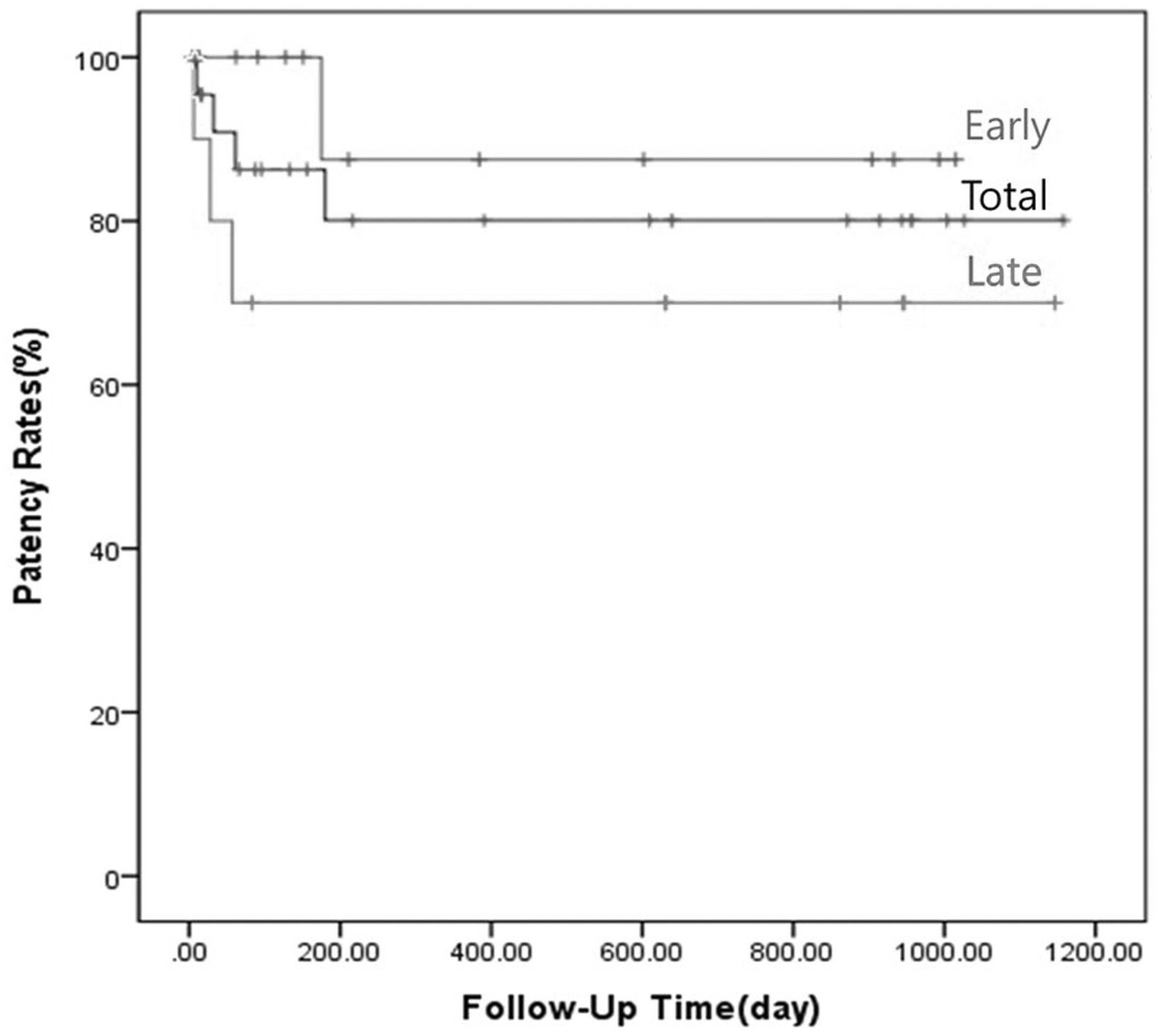
There was no patient with HVOO without positive findings on CT. The sensitivity and positive predictive value of abdominal CT were 100% (22/22) and 81% (22/27), respectively. Abdominal CT of 10 cases showed a decreased, mottled, reticulated, or mosaic pattern of parenchymal contrast enhancement on portal venous phase, which disappeared after stenting during the follow-up despite four occluded stents. During the follow-up period, 19 of 21 patients were alive at the time this manuscript was completed. One patient died of spontaneous intracranial hematoma 11 days after the procedure, despite successful stent insertion. The other patient died of a necrotizing liver infection 91 days after the procedure.
Discussion
In LDLT recipients, early post-transplant HVOO may induce liver function deterioration, graft failure, or even death resulting from the small size of the graft (13,14). A sufficiently long hepatic vein for reconstruction is not usually obtained during LDLT; this anatomic limitation is responsible for the development of HVOO (4,15). Such complications occurring in the early postoperative period (≤28 days) are thought to be caused by technical factors such as a tight suture line, donor–recipient size discrepancy, kinking of a redundant hepatic vein, and caval compression from a large graft (3,16). On the other hand, chronic (>28 days) obstructions are thought to result from fibrosis around the anastomotic site, intimal hyperplasia, or compression of the anastomosis from a hypertrophic graft (16).
In our series, primary stenting was selected for treatment instead of balloon angioplasty, which can induce rupture of the fresh anastomosis and may be ineffective in eliminating various etiologies of HVOO in the early stage (<28 days) (12). Further, balloon angioplasty performed alone is associated with a high incidence of relapse (17). In the current study, anastomotic disruption did not occur in any case, and the stent patency in patients with early onset of HVOO was slightly higher than that in patients with late onset of HVOO; however, no statistically significant difference in patency was observed. This result suggests that, irrespective of the procedure, once the procedure is successful, the stent patency is likely to be similar; however, further investigation is required.
Doppler ultrasound (US) is widely used to screen for HVOO after liver transplantation; however, multidetector CT is commonly used in patients with equivocal clinical and Doppler US findings because of its excellent spatial and temporal resolution. In addition, CT shows better sensitivity (97% vs. 87%) and specificity (86% vs. 68%) than Doppler US and allows the observation of parenchymal changes such as hypoattenuation during the portal venous phase or the delayed phase, which could suggest venous congestion (18). However, these parenchymal changes are not observed in all patients with HVOO after LDLT, as shown in our series (40%, 10/25). In six of 10 cases with parenchymal changes, stents remained patent until the end of the study, and parenchymal changes were resolved.
Pressure gradients have a key role in diagnosis, yet no consensus exists regarding gradient values and their correlation with significant stenosis. A pressure gradient of >5–6 mmHg is widely accepted as the threshold for induction of symptoms, yet pressure gradients of >3 mmHg also have the potential to be hemodynamically significant (19). Ko et al. (12) claimed that, in the presence of symptoms, stents should be implanted when even low gradients are observed, in an attempt to improve clinical characteristics and prevent obstruction. In our series, five patients with a pressure gradient of <6 mmHg (range, 3–5 mmHg) who exhibited structural abnormalities showed improvement in these abnormalities and a reduction in the pressure gradient (range, 1–2 mmHg) after stent placement. Therefore, although pressure gradients were sometimes low in patients with structural abnormalities, stent placement proved efficient. Further, we suggest that changes in the observed pressure measurements can be used to judge the success of stent placement.
A modified right lobe (MRL) graft with reconstruction of MHV tributaries (19–24) is commonly used to ensure donor safety in LDLT when performing a right lobe graft. Multiple MHV tributaries draining the segment 5 vein (V5) are commonly found in donor hepatectomy using conventional MRL grafts, and multiple anastomoses are inevitable. Graft congestion, caused by small-caliber MHV tributaries, can result in adverse effects on the regeneration of the graft and recovery of the recipient. In our series, MHVs treated with stents occluded during the follow-up period. Stents <10 mm in diameter were placed in five MHVs, four of which (80%) were occluded at the final follow-up. This result is in agreement with that of a previous study that showed that stent diameter was an independent factor associated with stent patency (12). Statistical significance between the obstruction rate and treated vessels was not analyzed because of an insufficient sample size. However, we observed a possible correlation in this study that warrants further research.
The main limitation of this study was its retrospective study design, with heterogeneous follow-up periods and heterogeneous stent types. In addition, CT was the only method used for the screening of HVOO. However, patency of hepatic vein stenting was shown to be relatively high, and CT exhibited both good sensitivity and positive predictive value for HVOO and additional parenchymal changes before and after stenting.
In conclusion, primary hepatic vein stenting is a useful treatment method for HVOO after LDLT, with acceptable patency observed. Additionally, we suggest that MHV stenting is more likely to be occluded during follow-up, which warrants further study in a larger population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.