
Abstract
Background
Metal artifacts often impair diagnostic accuracy in computed tomography (CT) imaging. Therefore, effective and workflow implemented metal artifact reduction algorithms are crucial to gain higher diagnostic image quality in patients with metallic hardware.
Purpose
To assess the clinical performance of a novel iterative metal artifact reduction (iMAR) algorithm for CT in patients with dental fillings.
Material and Methods
Thirty consecutive patients scheduled for CT imaging and dental fillings were included in the analysis. All patients underwent CT imaging using a second generation dual-source CT scanner (120 kV single-energy; 100/Sn140 kV in dual-energy, 219 mAs, gantry rotation time 0.28–1/s, collimation 0.6 mm) as part of their clinical work-up. Post-processing included standard kernel (B49) and an iterative MAR algorithm. Image quality and diagnostic value were assessed qualitatively (Likert scale) and quantitatively (HU ± SD) by two reviewers independently.
Results
All 30 patients were included in the analysis, with equal reconstruction times for iMAR and standard reconstruction (17 s ± 0.5 vs. 19 s ± 0.5; P > 0.05). Visual image quality was significantly higher for iMAR as compared with standard reconstruction (3.8 ± 0.5 vs. 2.6 ± 0.5; P < 0.0001, respectively) and showed improved evaluation of adjacent anatomical structures. Similarly, HU-based measurements of degree of artifacts were significantly lower in the iMAR reconstructions as compared with the standard reconstruction (0.9 ± 1.6 vs. –20 ± 47; P < 0.05, respectively).
Conclusion
The tested iterative, raw-data based reconstruction MAR algorithm allows for a significant reduction of metal artifacts and improved evaluation of adjacent anatomical structures in the head and neck area in patients with dental hardware.
Introduction
Metal artifacts have limited diagnostic evaluation of computed tomography (CT) images since the early days (1). At the same time, the prevalence of metallic implants such as dental fillings and implants, orthopedic prostheses and cardiac devices is increasing, particularly in elderly patients (2,3). This poses a particular challenge to the oral cavity, in which artifacts caused by non-removable dental implants and fillings are affecting a large area of the palatine and the root of the tongue (4).
The main underlying mechanisms responsible for causing these artifacts are beam hardening and photon starvation, due to the high-density metallic material of the implants (5). This often leads to impaired image quality of the adjacent tissue as well as of the metallic implant itself, since relevant anatomic structures are often completely obscured by artifacts, bearing the potential risk of missing relevant findings (6,7).
In recent years, a number of attempts have been undertaken in order to reduce metallic artifacts in CT imaging. Increased tube current at lower kV only or the use of higher kV energy may improve image quality in terms of noise reduction and better image contrast, but is accompanied by increased radiation dose levels (1,8). Dual-energy CT is another recently introduced method that significantly can reduce metallic artifacts using two different absorption spectra (9,10). Also, approaches including filtered back projection (FBP) (11,12), sinogram inpainting (13,14), or iterative methods (6,15,16) have been evaluated. However, while some of these methods may substantially reduce artifacts, none of these have made their way to clinical routine yet, also due to time-consuming reconstruction times and missing implementation in clinical workflows.
The purpose of this study was to assess the impact of an iterative metal artifact reduction (iMAR) algorithm on diagnostic image quality implemented in a clinical workflow in consecutive participants undergoing oncological head and neck CT imaging. Our hypothesis was that such an algorithm allows for improved diagnostic image quality by reducing the degree of metal artifacts due to dental implants and fillings.
Material and Methods
Patient population
Patient demographics and scan parameters of 30 participants included in this study.

CT image acquisition
All examinations were performed using a standard single-energy/dual-energy imaging protocol on a second generation Dual Source CT scanner (Somatom Defintion Flash, Siemens Healthcare, Forchheim, Germany). Acquisition parameters were as follows: tube voltage of 120 kV in single-energy acquisition; in dual-energy we used standard DE tube ratio of 100/Sn140 kV. The 120 kV equivalent mixed images were reconstructed using 0.5 ratio of higher and lower energy spectra. Tube current varied (CareDose) with an average of 219 mAs, gantry rotation time 0.28–1/s, and collimation 0.6 mm. For further acquisition parameters, see Table 1.
CT image reconstruction
From the acquired CT raw data, two axial series were reconstructed using similar kernel and slice thickness (medium hard kernel, B49, slice thickness: 1.5 mm: (i) Standard reconstruction with Advanced Modeled Iterative Reconstruction (ADMIRE) algorithm (non-iMAR); and (ii) Reconstruction applying an iterative Metal Artifact Reduction (iMAR) algorithm (Siemens Healthcare) which combines the recently introduced frequency-split metal artifact reduction technique (FSMAR) and the normalized metal artifact reduction approach (NMAR) as described in detail elsewhere (11,17,18). Briefly, the FSMAR algorithm preserves the valid edge information of the uncorrected images, given that this information is often impaired when using pure sinogram inpainting methods. The NMAR algorithm avoids the formation of new artifacts tangentially to high contrast objects, commonly observed in sinogram inpainting approaches. By combining both methods, the tested iMAR algorithm repeatedly performs frequency-split operations and normalized sinogram interpolations. The result of each iteration serves as input for the next iteration to further reduce the remaining artifacts and thus subsequently improves image quality. Depending on the density and location of the metallic hardware preprogrammed algorithm adjustments (different number of iterative cycles) can be selected by the operator, such as dental hardware, cardiac devices, or orthopedic prosthesis for optimal artifact reduction. The reconstruction process is executed similar to the standard AMDIRE reconstruction without specific operator education.
CT image analysis
Qualitative image analysis: All reconstructed CT images were reviewed on a workstation (SyngoVia VA30A; Siemens Healthcare) by two observers (radiologist JW with 2 years of experience in oncological CT imaging and CS with 5 years of experience in oncological CT imaging), blinded to the type of reconstruction applied. Per study subject, all readings were performed on the axial images which were the most and the least affected by metal artifacts. The qualitative reading comprised two aspects. First, overall image quality was rated on a 5-point Likert scale (1, non-diagnostic; 2, poor; 3, fair; 4, good; 5, excellent). Second, artifact severity and ability of evaluating adjacent soft tissue of the palatine or root of the tongue and the distant para/retropharyngeal soft tissue was graded, again using a 5-point Likert scale (1, major streak artifacts, no depiction of anatomical structures; 2, marked artifacts, no depiction of surrounding tissue and considerably impaired image quality of distant soft tissue; 3, moderate artifacts, non-diagnostic in the surrounding tissue but fair diagnostic image quality of distant soft tissue; 4, minor artifacts with good image quality; 5, no artifacts, full diagnostic image).
Quantitative image analysis: In order to obtain objective measures of the degree of artifacts, mean CT attenuation values (Hounsfield Units [HU]) and standard deviation (SD) were measured on the axial reconstruction of the image most affected by metal artifacts. A subjective consensus reading was performed in order to select the CT reconstruction with the most severe artifacts. The corresponding imaging of the second reconstruction with the less pronounced artifact was used to evaluate the impact on the artifact reduction. As such, per patient a total of six regions of interest (ROIs) were placed on each reconstruction (iMAR and standard reconstructions). The ROIs included the following regions: ROI1, darkest area of the artifact; ROI2/3, left and right masseter muscle; ROI4/5, left and right posterior cervical muscles; ROI6, tongue. Location and diameter of the ROIs (1.5 cm2) were kept constant in all patients with muscle adapted oval shaping of ROI2–5. To ensure identical positioning of the ROIs in iMAR and non-iMAR reconstructions in each patient, ROI size and position was copied from iMAR to non-iMAR images. An exemplary image of ROI size and placement is provided in (Fig. 1). Hereafter, ROI1–3/6 are summarized as adjacent tissue and ROI4/5 as distant soft tissue.
Axial CT images of a 46-year-old patient with melanoma: non-iMAR (a) and iMAR (b) reconstruction in the image least affected by metallic artifacts and exemplary size and placement of ROI1–6.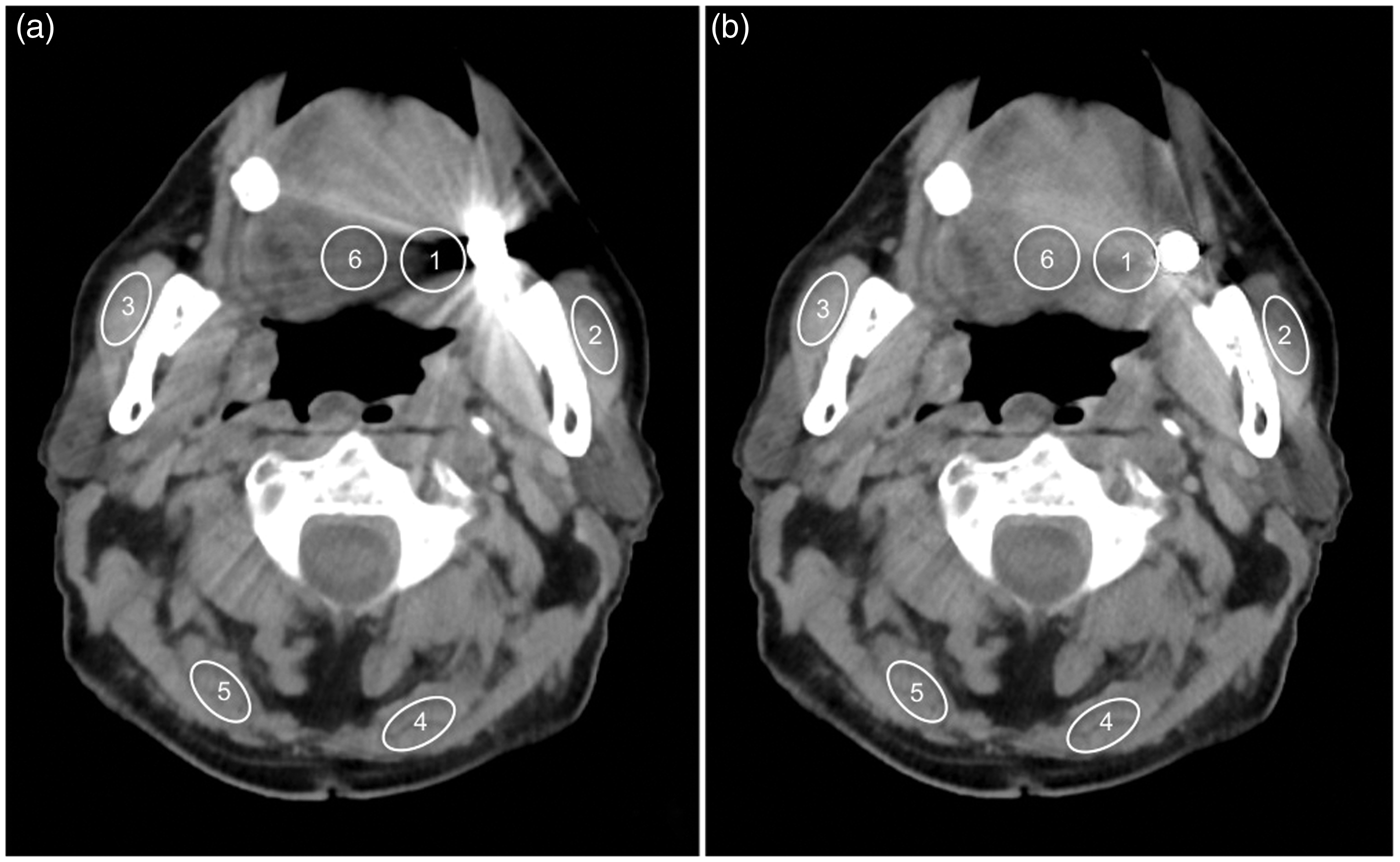
Statistical analysis
Descriptive statistics are provided as mean ± standard deviation for continuous and n (%) for categorical variables. To determine differences of the artifacts and diagnostic image quality score (quantitative) as well as absolute and relative measurements to address the clustered data structure (several measurements per participants), repeated measure analysis was performed. As such, we fitted linear models in SAS Proc Mixed (SAS Institute, Cary, NC, USA) by assuming a standard variance components pattern of covariance.
Inter-reader agreement of qualitative image analysis was evaluated by Cohen’s kappa.
All statistical analyses were performed using the SAS system for Windows, version 9.2 (SAS Institute), and statistical significance was defined as p < 0.05.
Results
Overall, 30 consecutive patients were included in the analysis (mean age, 62.8 ± 12.2 years; 50% men). The reconstruction time was equal for iMAR and the standard reconstruction (17 s ± 0.5 vs. 19 s ± 0.5; p > 0.05) and all reconstructions from all patients were included in the final analysis. The average dose length product (DLP) was 767.8 mGy*cm (average CT dose index (CTDIvol) was 12.39 mGy) for the whole-body staging CT protocol applied. Detailed patient and scan parameters are summarized in Table 1.
Qualitative image analysis: In the standard reconstructed images, the diagnostic image quality was rated 2.6 ± 0.5 in the image most affected by metal artifacts and 3.6 ± 0.8 in the image the least affected by metal artifacts. Compared to the standard reconstruction, the diagnostic imaging quality was rated significantly higher on iMAR reconstructions in the image most affected by metal artifacts (3.8 ± 0.5) as well as in the image the least affected by metal artifacts (4.8 ± 0.4, p < 0.01). Image examples and further results are provided in Figs. 1–3 and Table 2.
Axial CT images of a 62-year-old patient with breast cancer: non-iMAR (a) and iMAR (b) reconstruction in the image most affected by metallic artifacts demonstrating the effectiveness of artifact reduction (circle). Axial CT images of a 35-year-old patient with an abscess located in the left mucosal space. Lesion detection (circle) is clearly improved with iMAR reconstruction (b) as compared to non-iMAR reconstruction (a). Observed diagnostic image quality and extent of artifacts between standard and iMAR reconstructions.


The absolute and relative difference in diagnostic image quality was higher for images most affected by metal artifacts as compared with images the least affected by metal artifacts (Absolute: 1.15 ± 0.58 vs. 1.19 ± 0.77; p > 0.05; and relative: 29.6 ± 14.2% vs. 24.3 ± 18.5%; p < 0.05). In addition, the diagnostic image quality was significantly higher for both adjacent and distant soft tissue on the iMAR reconstructions in the images with least artifacts as compared with standard reconstructions (4.0 ± 0.5 vs. 4.7 ± 0.4; adjacent vs. distant image quality). In contrast, in the image with most severe metal artifacts, the adjacent soft tissue remained non-diagnostic in both reconstructions, whereas the depiction of the para/retropharyngeal distant tissue improved significantly (2.6 ± 0.8 vs. 3.6 ± 0.7; p < 0.0001 for adjacent vs. distant image quality) with consecutively improved lesion detection. Examples are presented in Figs. 1–3.
Inter-reader agreement for qualitative image analysis was high (all κ > 0.71).
Quantitative image analysis: On the standard reconstructions, the mean CT attenuation in the image most affected by metal artifacts was lowest in the ROI adjacent to the dental hardware (ROI1) and highest in the distant (mean of ROI4/5) soft tissue (–20 ± 47 vs. 5.5 ± 1.8 for ROI1 vs. mean of ROI4/5, p < 0.01, respectively). Similarly, on the iMAR reconstructions, the mean CT attenuation in the image most affected by metal artifacts was lower in the ROI adjacent to the dental hardware (ROI1) as compared to the ROI in distant (mean of ROI4/5) soft tissue (0.9 ± 1.6 vs. 5.1 ± 1.6 for ROI1 vs. mean of ROI4/5, p < 0.0001, respectively). Results are also presented in Table 2.
Discussion
In this study we demonstrated that a workflow integrated iterative metal artifact reduction algorithm significantly improves overall and diagnostic image quality and reduces artifacts caused by dental hardware in patients undergoing standard head and neck oncologic CT imaging. While this effect is most pronounced in distant soft tissue, e.g. posterior cervical muscles, improvements are also observed in the tissue directly adjacent to the metal implants, although a fully diagnostic image quality is not achieved in these regions even with the iMAR reconstruction algorithm.
Despite many substantial research efforts over the last years, metal artifacts still pose a challenge for CT imaging. The main reason for this is that easily applicable methods to reduce metal artifacts, such as using higher kV energy or increased tube current, result in a significant increase of the radiation dose exposure of the patient (1,5). Other approaches like dual-energy CT or FBP-algorithms showed promising results in reducing artifacts, however, required specialized equipment or lengthy complex calculations that are not automated as well as producing new artifacts are significant drawbacks, and thus, these techniques never gained widespread clinical acceptance (10,11,19,20).
For instance, Meinel et al. introduced a special adjusted protocol and reconstruction algorithm using dual-energy CT that could significantly reduce metal artifacts and improve diagnostic image quality. However, the developed protocol was specifically tailored to MAR in patients referred for CT due to musculoskeletal indications without the administration of iodine contrast. Also, due to the dual-energy-based extrapolation, the degree of iodine enhancement is similarly attenuated in the images, which may limit the diagnostic value of the approach, particularly in oncological settings (10). Morsbach et al. (16) evaluated an iterative and linear interpolated MAR algorithm compared to FBP-reconstruction. They also demonstrated excellent results concerning artifact reduction and image quality, however, for post-processing additional image transfer to a dedicated work-station with a special reconstruction software was needed and thus an implementation in clinical workflow was not possible.
In our analysis we could demonstrate the advantage of the tested novel iterative MAR algorithm as an effective tool for artifact reduction and significantly improved diagnostic image quality. However, it is important to note that other iterative metal artifact algorithms such as the Metal Deletion Technique (MDT) and Selective Algebraic Reconstruction Technique (SART) have been developed to allow for reduction of dental hardware artifacts with promising results (21,22). Therefore, further research, including comparison of different iterative metal artifact reduction techniques with respect to impact on image quality, diagnostic accuracy and reconstruction time are required.
Some limitations of the study must be acknowledged. First, we had no further information about the type (metallic hardware such as amalgam or gold) and volume (single tooth to total prosthesis) of the dental hardware of our patients prior to the CT scan and thus correlation to image quality was not possible. Second, only one patient of the collective had a parapharyngeal abscess at the time of examination and no patient suffered from cancer manifestation in the observed area. However, our results indicated that using this MAR algorithm provides additional diagnostic information, and this might be of special importance in patients with oro-pharyngeal pathologies. In addition, the quantitative image analysis did not comprise the palatine as separate ROI given that there was no constant area for consistent ROI placement in the reconstructions most affected by artifacts in all participants. Further, more focused research may be necessary. Also, we did not specifically assess the impact of iMAR on image noise. However, there was no visible difference during the subjective assessment of image quality.
In conclusion, the tested novel iterative metal artifact reduction algorithm significantly reduces metal artifacts caused by dental hardware and consecutively improves image quality and diagnostic performance of anatomic structures in the head and neck area.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by an unrestricted research grant by Siemens Healthcare (Forchheim, Germany).