
Abstract
Background
Chondromalacia patellae is a very common disorder. Although magnetic resonance imaging (MRI) is widely used to investigate patellar cartilage lesions, there is no descriptive MRI-based grading system for chondromalacia patellae.
Purpose
To propose a new MRI grading system for chondromalacia patellae with corresponding high resolution images which might be useful in precisely reporting and comparing knee examinations in routine daily practice and used in predicting natural course and clinical outcome of the patellar cartilage lesions.
Material and Methods
High resolution fat-saturated proton density (FS PD) images in the axial plane with corresponding T2 mapping images were reviewed. A detailed MRI grading system covering the deficiencies of the existing gradings has been set and presented on these images. Two experienced observers blinded to clinical data examined 44 knee MR images and evaluated patellar cartilage changes according to the proposed grading system. Inter- and intra-rater validity testing using kappa statistics were calculated.
Results
A descriptive and detailed grading system with corresponding FS PD and T2 mapping images has been presented. Inter-rater agreement was 0.80 (95% confidence interval [CI], 0.71–0.89). Intra-rater agreements were 0.83 (95% CI, 0.74–0.91) for observer A and 0.79 (95% CI, 0.70–0.88) for observer B (k-values).
Conclusion
We present a new MRI grading system for chondromalacia patellae with corresponding images and good inter- and intra-rater agreement which might be useful in reporting and comparing knee MRI examinations in daily practice and may also have the potential for using more precisely predicting prognosis and clinical outcome of the patients.
Introduction
Chondromalacia patellae is a very common disorder which is characterized by softening, swelling, fraying, fissuring, and erosion of hyaline cartilage overlying the patella (1). Patellar chondromalacia could be observed as a cause of patellofemoral pain, as well as in patients with osteoarthritis, in patients with knee trauma, or even in asymptomatic patients. Patellar chondromalacia could also be diagnosed in the vast majority of patients who underwent magnetic resonance imaging (MRI) examination of the knee regardless of clinical diagnosis. Although arthroscopy is generally considered as the gold standard for making the diagnosis, with the current field strength of MRI, developments in coil production, and software, MRI has become a powerful non-invasive tool to investigate patellar cartilage lesions (2). MRI is also used for monitoring the effects of therapies for cartilage lesions (3).
Grading systems for articular cartilage lesions.
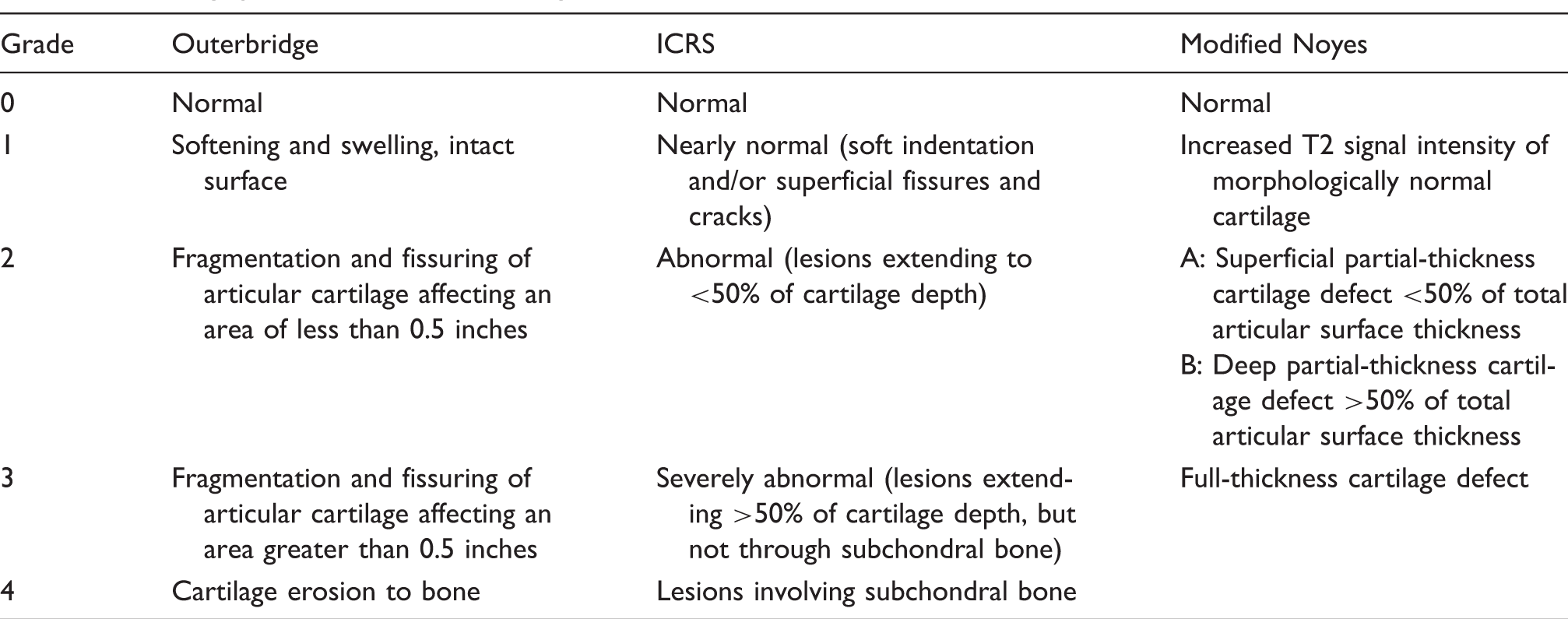
Although there have been many classifications used for articular cartilage injury, we believe all these systems have some deficiencies in describing and monitoring all cartilage lesions based on the current knowledge. First, very early intracartilaginous lesions with intact articular surface have not been managed as a separate entity and classified accordingly considering the area involved. Second, all these existing clinical and imaging grading systems largely depend on depth of the chondral defect. All types of defects with the same depth or area, such as fissures, flaps, and fibrillations, have been classified in the same grade as if they could be managed as a single entity and their natural course or response to any therapy would result in same outcome. Third, full thickness cartilage defects, with or without subchondral bony changes, have been classified in the same category. The objective of this study was to propose a new descriptive MRI grading system for chondromalacia patellae covering the deficiencies of the current systems, which might be useful in reporting, comparing, and monitoring patellar chondral lesions.
Material and Methods
This study was approved by the institutional ethics committee. Informed consent was obtained from all individual participants included in the study.
Patients
Forty-four knee MRI examinations of 41 adult consecutive patients (20 women, 21 men; mean age, 42 years; age range, 21–71 years) were included in this study. Clinical diagnosis was patellar chondromalacia in 21 (51%), non-specific pain in nine (22%), meniscopathy in eight (20%), and anterior cruciate ligament tear in three (7%) patients. Patellar cartilage of the patients was evaluated in FS PD images and corresponding T2 mapping images in the axial plane as explained in the imaging section. Images of the patients with any kind of artifacts that would prevent optimum interpretation were not included in the study.
Imaging
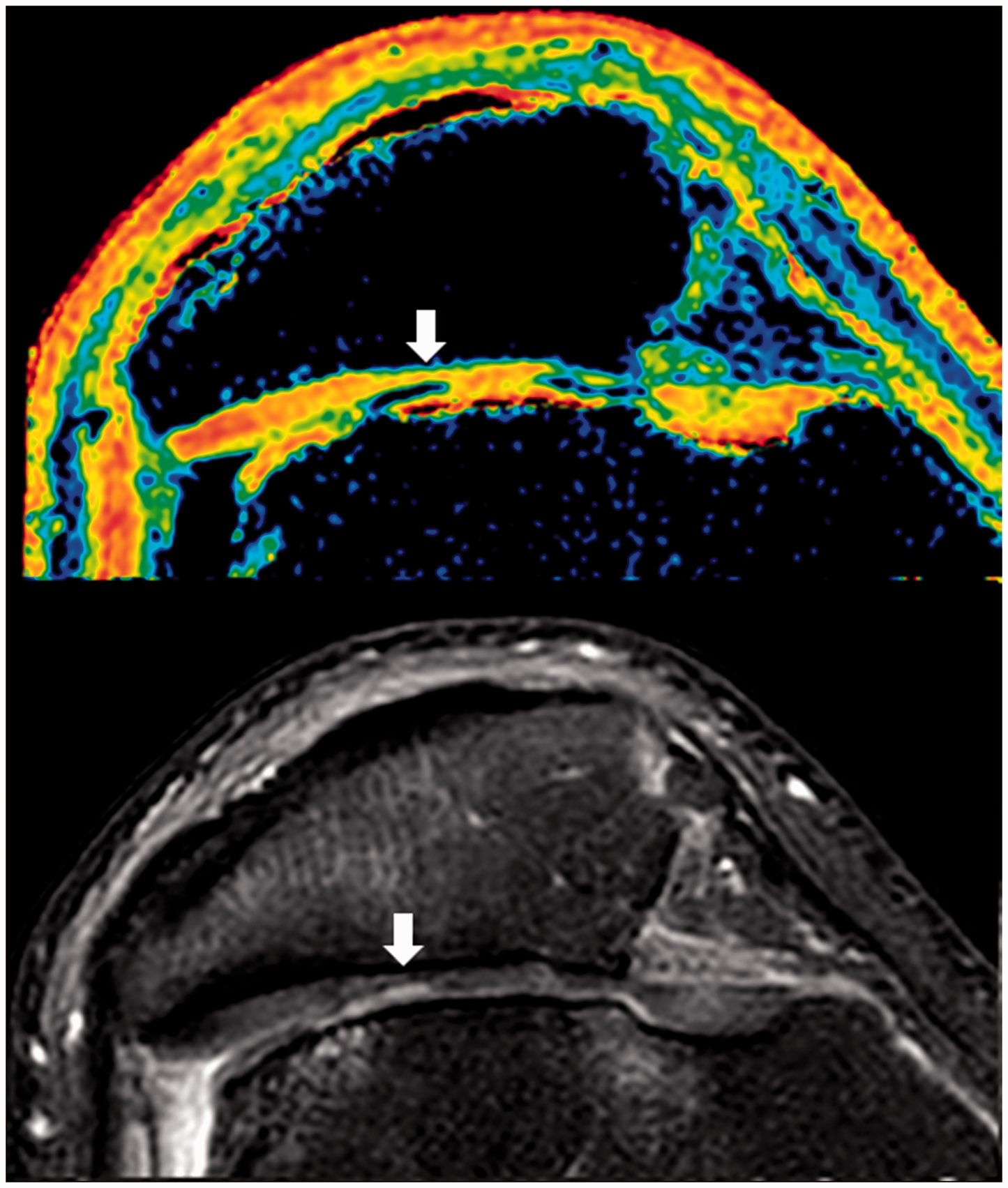
All images were obtained with a 3.0 T machine (Ingenia; Philips Medical Systems, Best, The Netherlands) using a 16-channel transmit/receive dedicated knee coil. FS PD images (TR 2000/TE 30) were obtained in the axial plane with two excitations. Slice thickness was 2 mm, resolution was 0.4 × 0.5 mm except for Fig. 12 which had a resolution of 0.3 × 0.3 mm. Field of view was 80 mm. Corresponding T2 mapping sequence (TR 2000/TE 13, 26, 39, 52, 65, 78) were obtained with the same slice thickness, 0.6 × 0.6 mm resolution, and with single excitation. In these images, the orange areas represent normal cartilage whereas the yellow, green, and blue areas represent cartilage lesions with higher water content in that order.
MRI grading
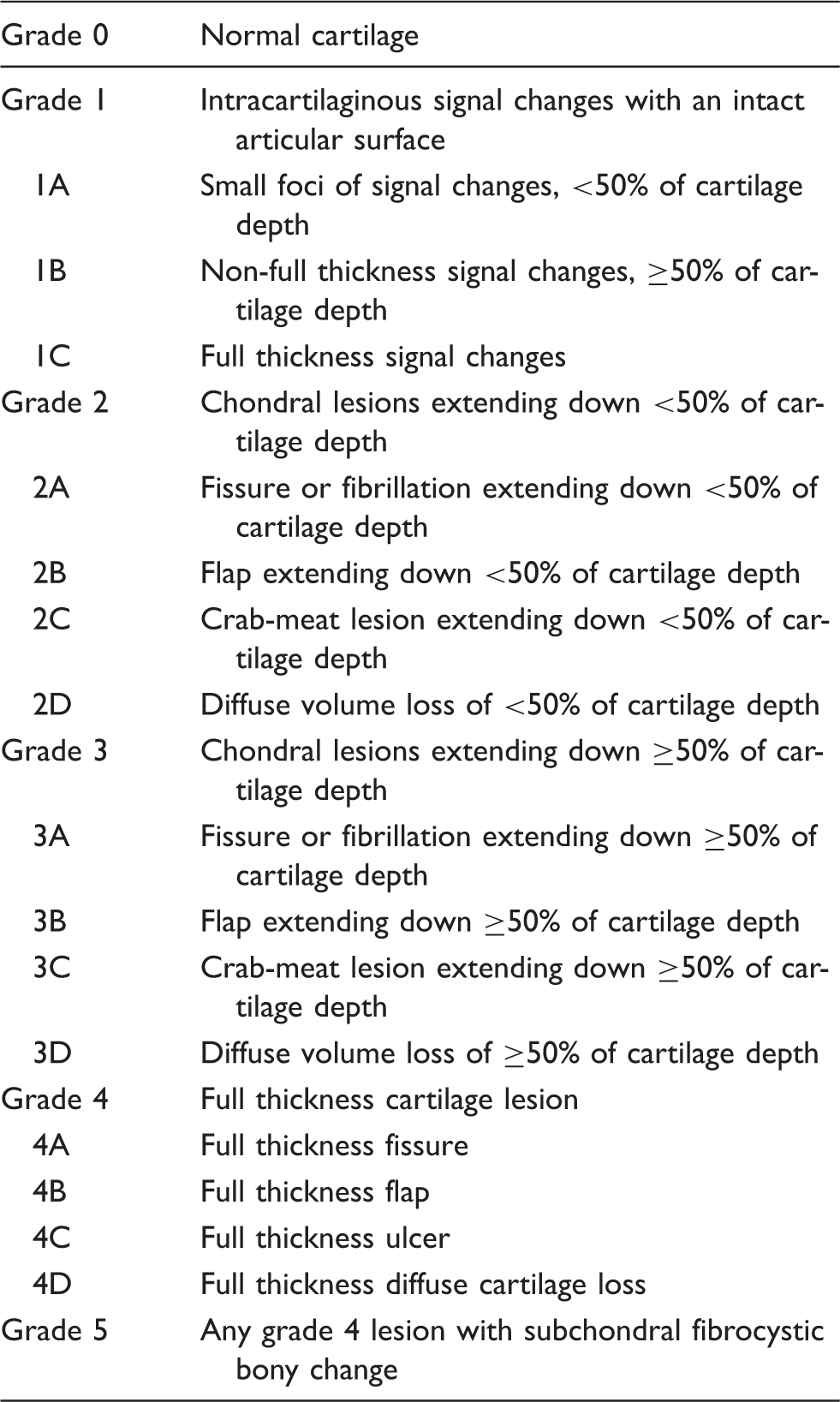
MRI grading of chondromalacia patellae.

T2 mapping (up) and corresponding FS PD (down) images of a normal appearing patellar cartilage. Note uniform homogenous signal from the cartilage both in FS PD and T2 mapping images. Relative thin appearance of medial aspect of the cartilage with green coding in T2 mapping is caused by partial volume artefact.
T2 mapping (up) and corresponding FS PD (down) images showing small foci of signal changes (arrows) representing grade 1A lesions.
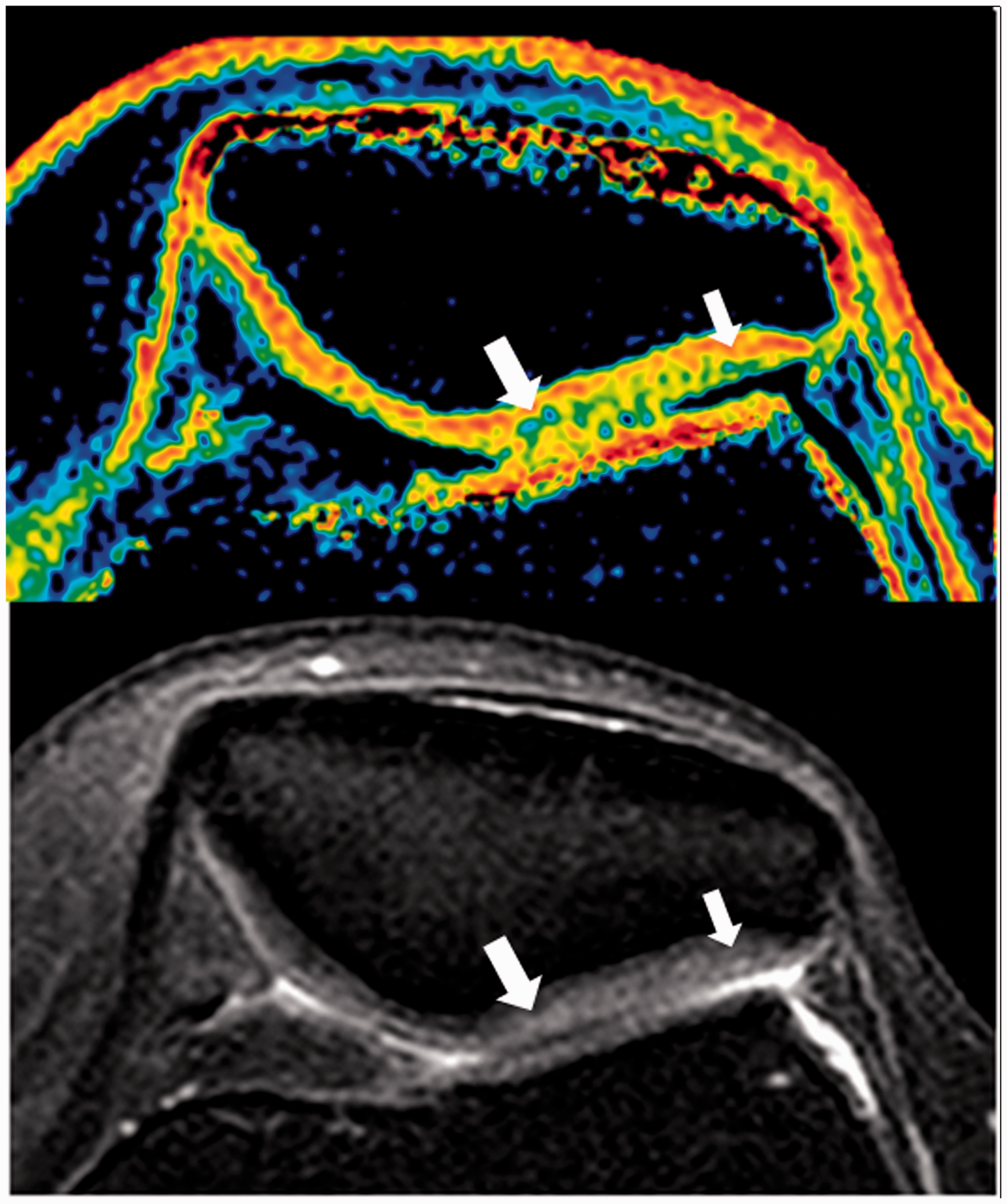
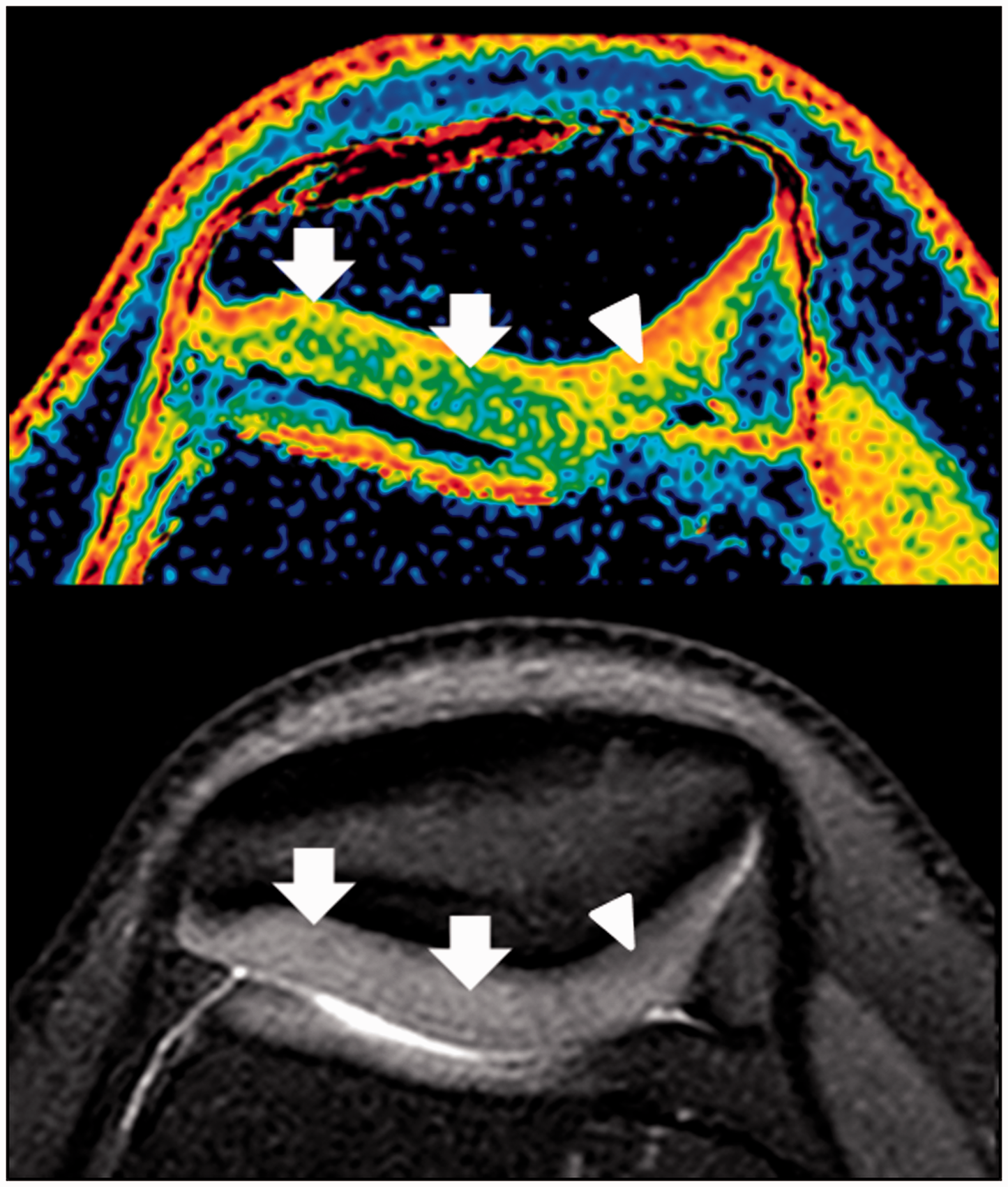
T2 mapping (up) and corresponding FS PD (down) images showing signal changes of articular cartilage (arrows) representing grade 1B lesions. Note there is swelling (arrowheads) of the cartilage which could be noted by arthroscopy whereas the other lesion is located deeply and might not be detected.
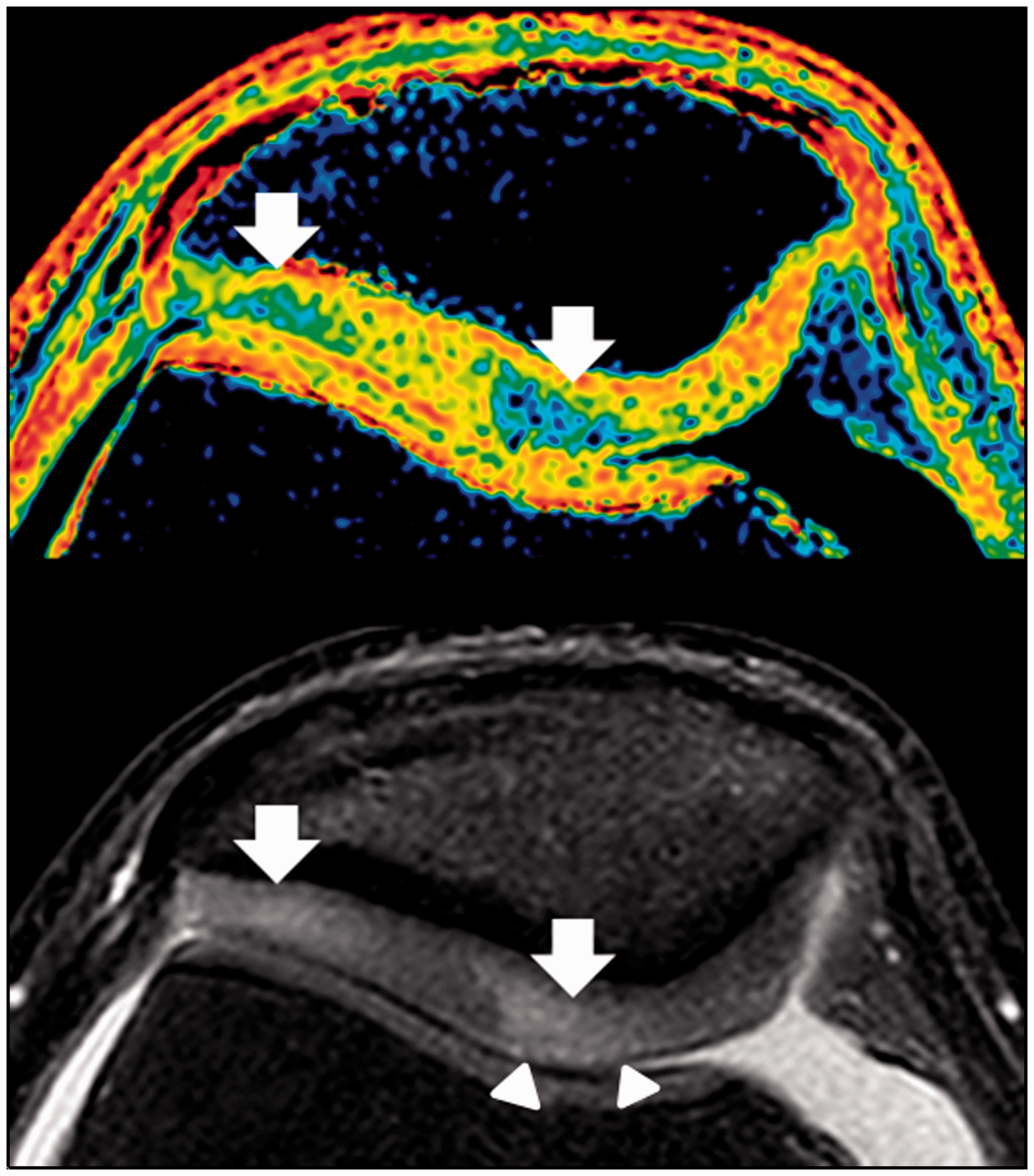
T2 mapping (up) and corresponding FS PD (down) images showing diffuse signal changes of articular cartilage (arrows) in the lateral facet representing grade 1C lesion. Note there is also a grade 1B lesion (arrowhead) in the medial facet of the patellae.
Grade 2 is reserved for chondral lesions extending down <50% of the cartilage depth. Grade 2A represents isolated fissures or fibrillations (Fig. 5), grade 2B represents flaps (Fig. 6), grade 2C represents a crab-meat appearance, multiple fissures, or fibrillations side by side (Fig. 7), and grade 2D represents a diffuse cartilage volume loss, which width of the lesion is more than its depth.
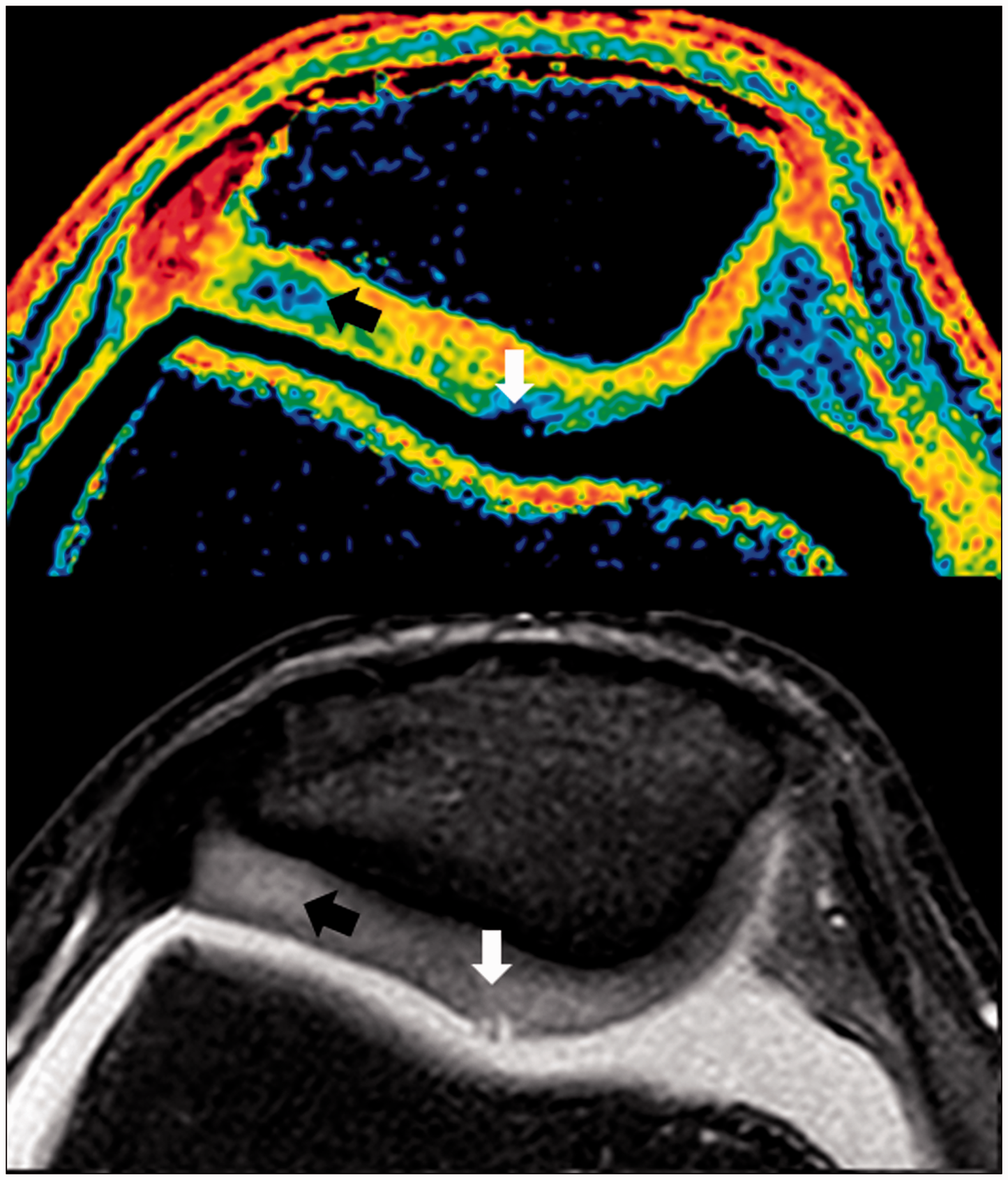
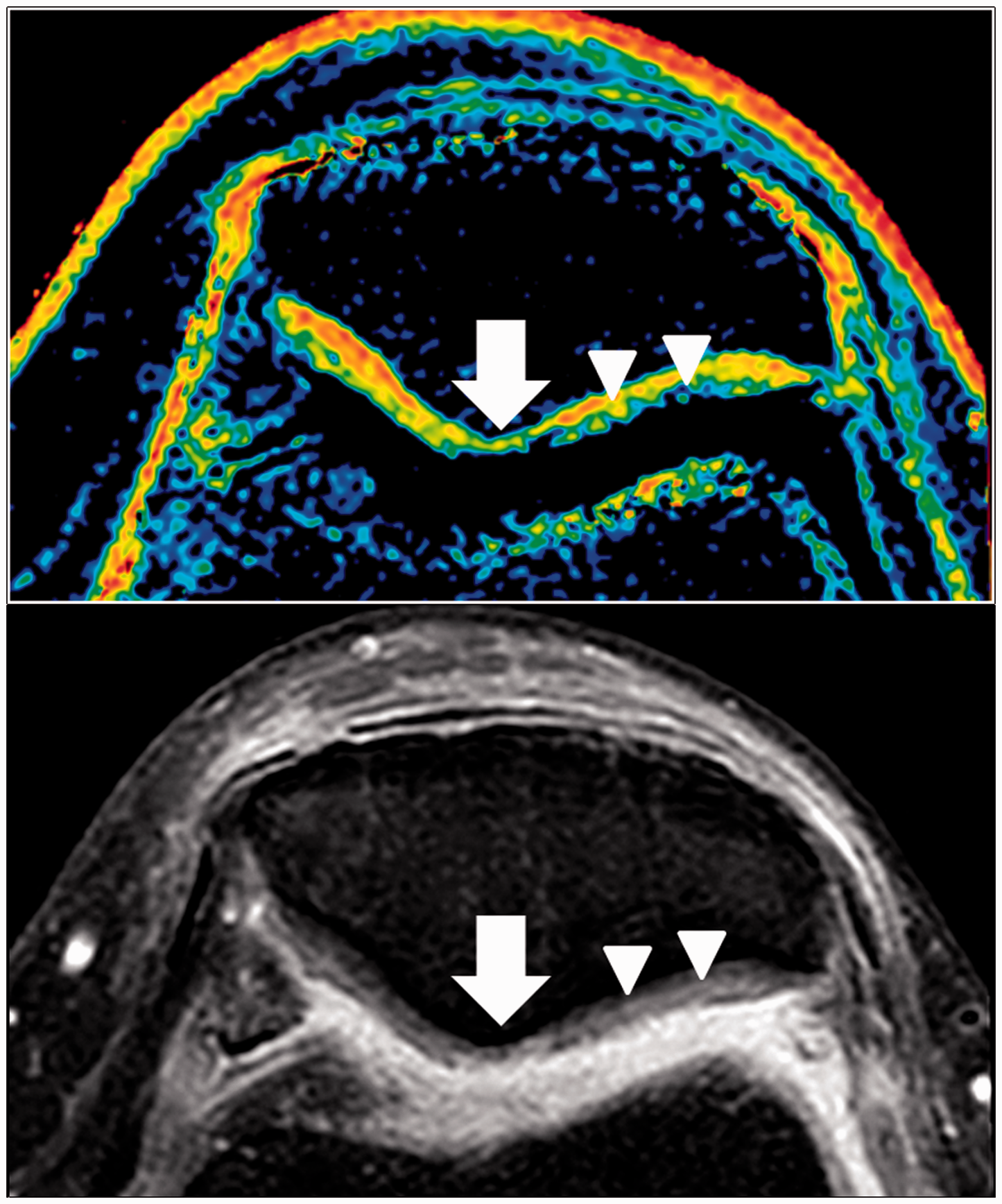
T2 mapping (up) and corresponding FS PD (down) images showing a superficial fissure (arrow) representing grade 2A lesion. T2 mapping (up) and corresponding FS PD (down) images showing a superficial flap (white arrow) representing grade 2B lesion which could be easily seen by arthroscopy. Note there is also a deep grade 1B lesion (black arrow) which might be undetected by visual inspection at arthroscopy. T2 mapping (up) and corresponding FS PD (down) images showing crab-meat appearance representing grade 2C lesion (arrowheads) and grade 3C (arrow) lesion.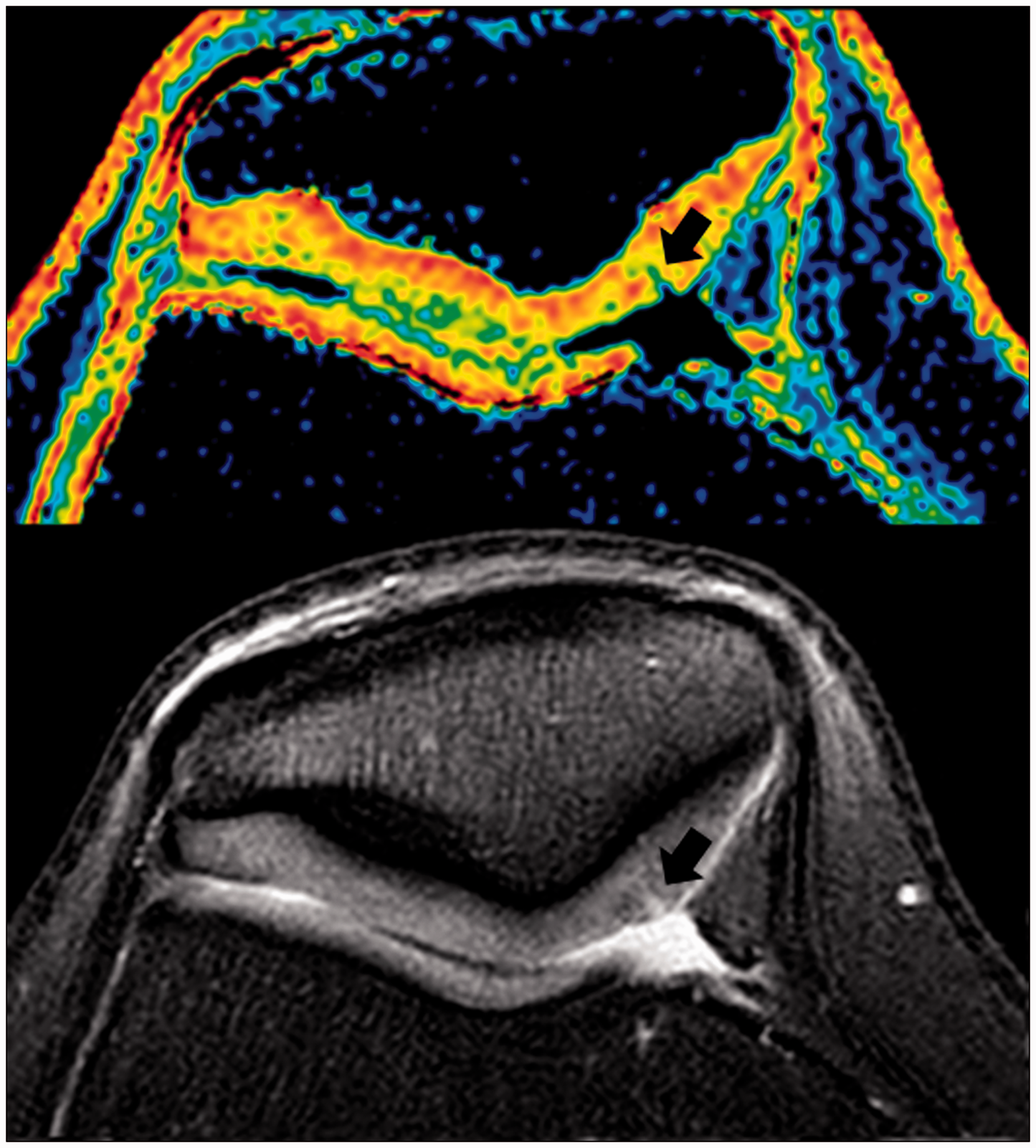
Grade 3 is reserved for chondral lesions extending down 50% or more of the cartilage depth but not reaching the subchondral bone. Like grade 2 lesions, grade 3A represents isolated fissures or fibrillations, grade 3B represents flaps (Fig. 8), grade 3C represents a crab-meat appearance (Fig. 7), and grade 3D represents diffuse chondral volume loss (Fig. 9).
T2 mapping (up) and corresponding FS PD (down) images showing a flap (arrow) reaching 50% of cartilage thickness representing grade 3B lesion. T2 mapping (up) and corresponding FS PD (down) images showing a diffuse volume loss of more than 50% of articular cartilage (arrows) representing grade 3D lesion.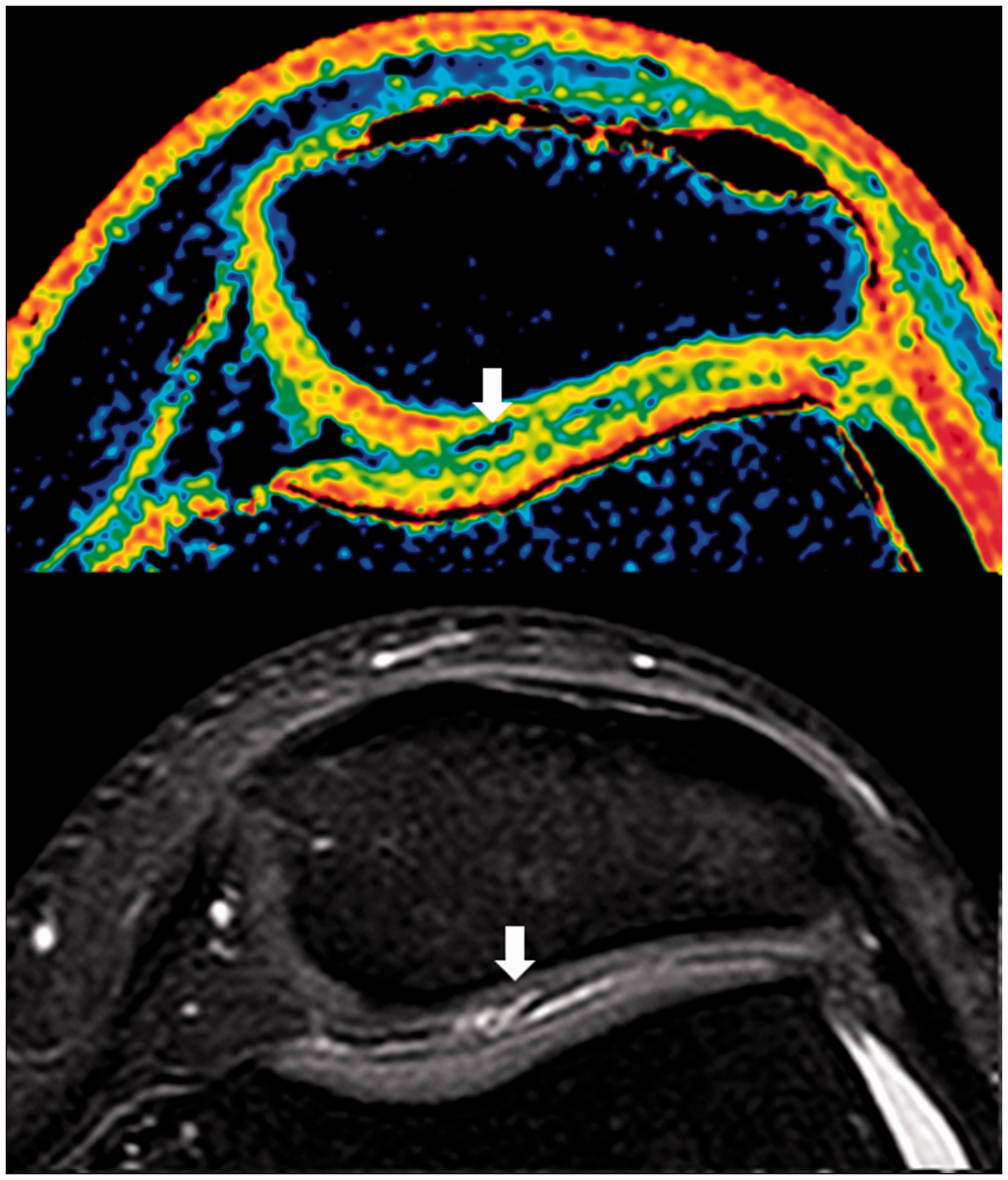
Grade 4 is reserved for full thickness cartilage defects. Grade 4A represents a full thickness fissure, grade 4B represents a full thickness flap (Fig. 10), grade 4C represents a full thickness ulcer, and grade 4D represents full thickness diffuse cartilage volume loss. Grade 5 is reserved for any grade 4 lesion with subchondral fibrocystic change in the underlying bone (Fig. 11).
T2 mapping (up) and corresponding FS PD (down) images showing a full thickness flap (arrow) representing grade 4B lesion. (a) FS PD image showing full thickness articular cartilage loss with subchondral changes (arrows), (b) FS PD image showing full thickness fissure with subchondral changes (arrows) representing grade 5 lesions. Very high resolution (0.3 × 0.3 mm) axial FS PD image of the patellae of a volunteer. Anatomic zones of the cartilage are not delineated in normal or chondromalacic appearing area of the articular hyaline cartilage.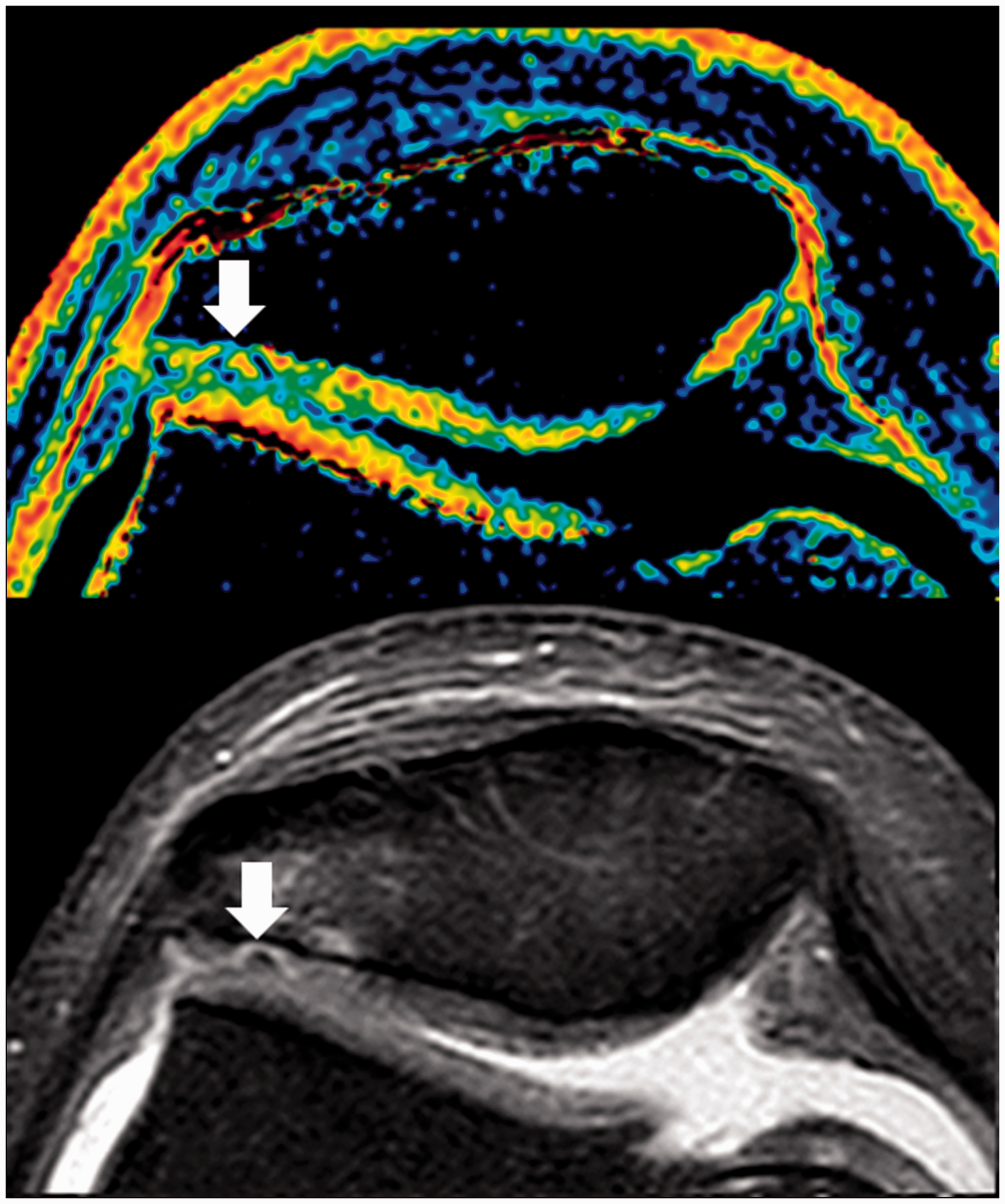
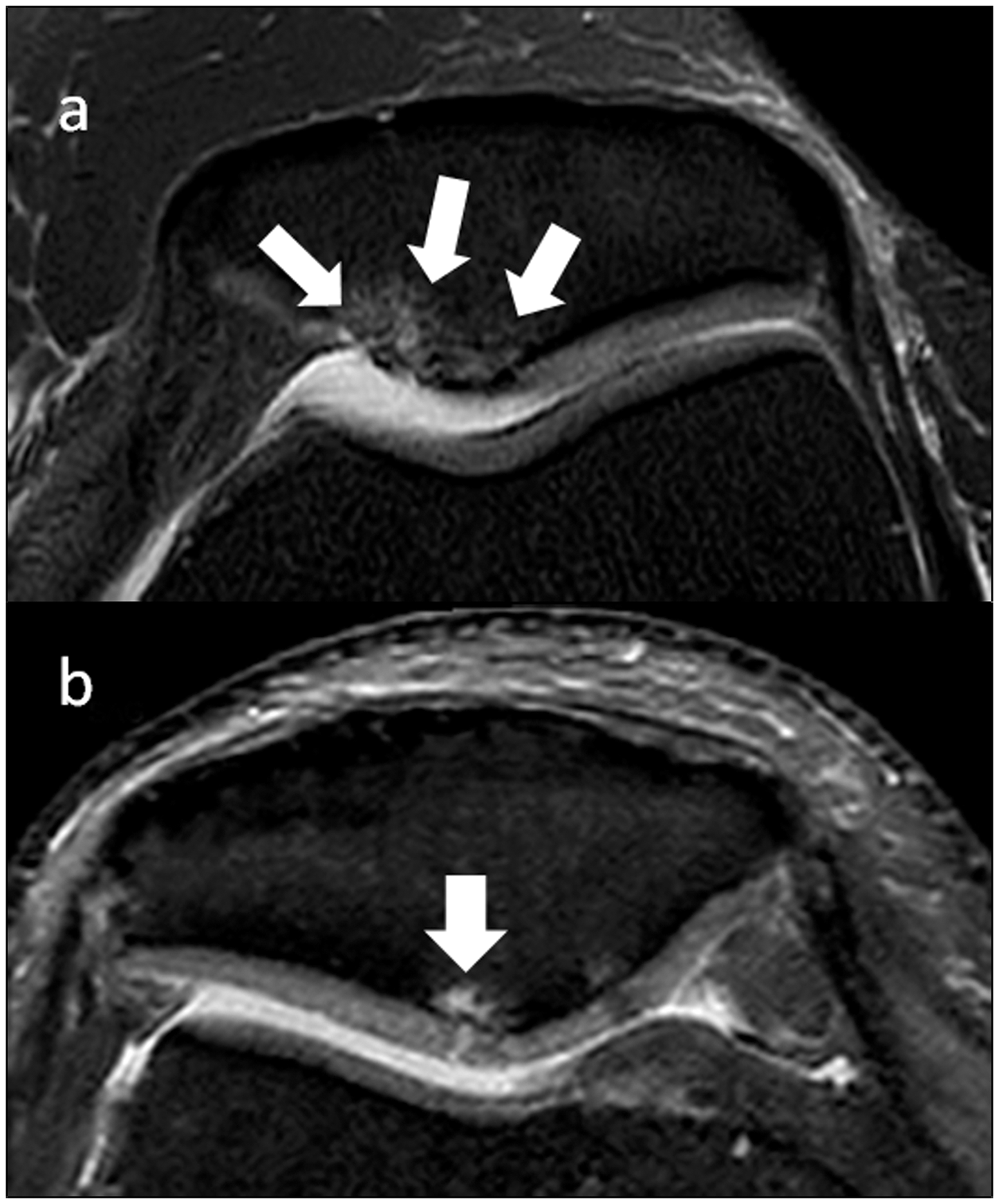
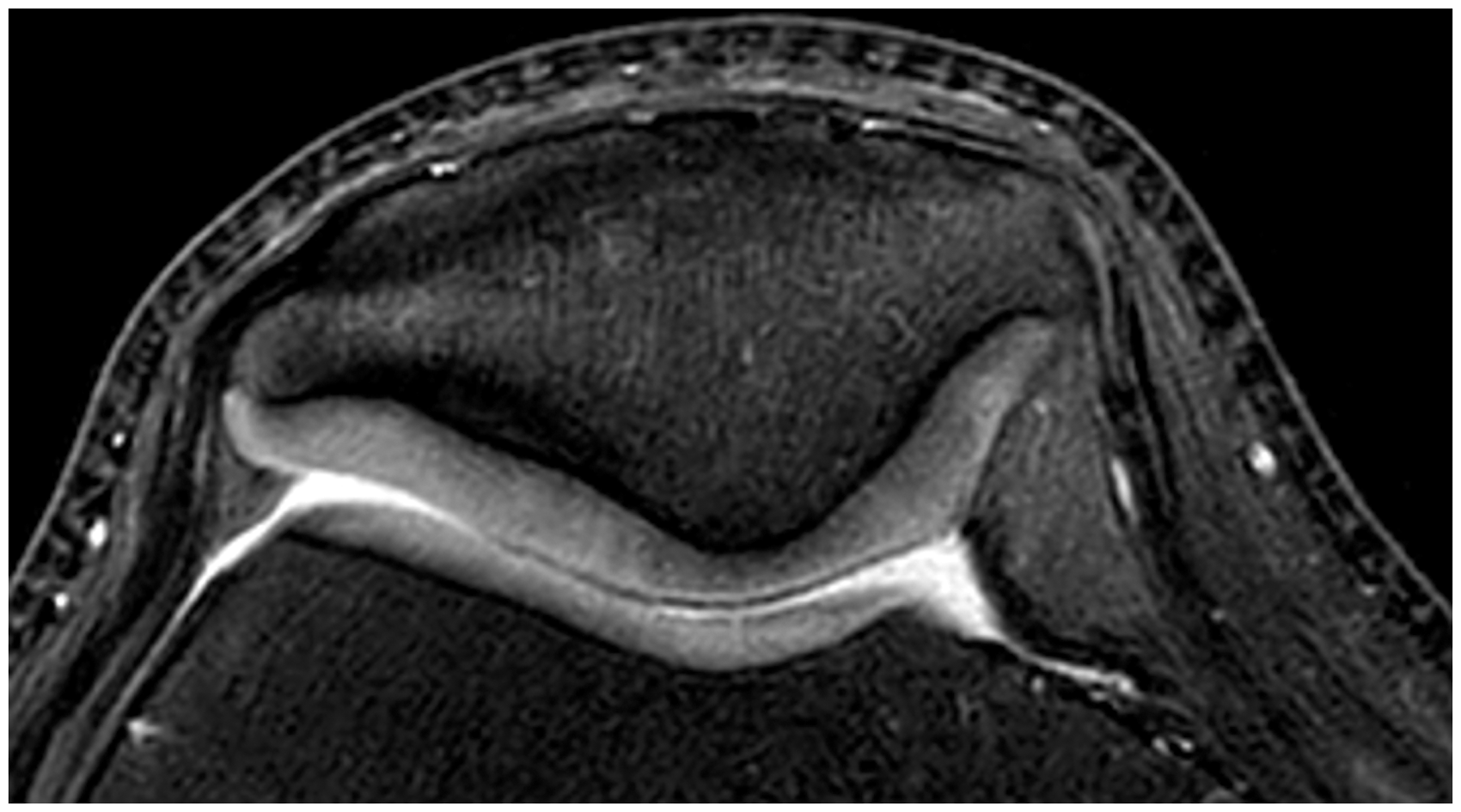
Image review
All images were reviewed and graded by two radiologists blinded to the clinical data. Observer A was a general radiologist with 16 years of experience and observer B was a musculoskeletal radiologist with 10 years of experience. Final grading of patellar chondromalacia was made with mutual agreement. For each patella, medial facet, lateral facet, and junctional area were separately evaluated and graded. Therefore, each rater did perform 132 gradings in 44 knee examinations.
Statistical analysis
We performed inter- and intra-rater validity testing using Cohen’s unweighted kappa statistics with SPSS 20 software (SPSS Inc., Chicago, IL, USA). To assess inter-rater agreement, two radiologists blinded to the clinical data examined 44 knee MRI examinations of 41 adult patients. To assess intra-rater agreement, observers A and B re-evaluated the same patients after at least a 3-week period. Kappa values were defined based on Altman’s Kappa Benchmark Scale (Table 2). A Kappa value <0.20 indicates a poor agreement level, a value of 0.21–0.40 indicates a fair agreement level, a value of 0.41–0.60 indicates a moderate agreement level, while ranges of values 0.61–0.80 and 0.81–1.00 indicate good and very good agreement levels, respectively (15).
Results
Grading results
There were 76 grade 1 lesions (58%), 14 grade 2 lesions (11%), five grade 3 lesions (4%), four grade 4 lesions (3%), and nine grade 5 lesions (7%) in 132 separate areas of 44 patellae examined. There was no patient whose patellar cartilage was interpreted as normal in all areas.
Inter- and intra-rater variability
Inter-rater agreement for grading was 0.80 (95% confidence interval [CI], 0.71–0.89) (k-values with 95% CI in parentheses). Of 18 disagreements, 12 of them were in between the same grade; seven for grade 1 lesions, three for grade 2 lesions, and two for grade 3 lesion. There was no inter-rater disagreement in evaluating grade 4 and 5 lesions.
Intra-rater agreements for grading were 0.83 (95% CI, 0.74–0.91) for observer A and 0.79 (95% CI, 0.70–0.88) for observer B (k-values with 95% CI in parentheses). Of 37 total disagreements, 18 for observer A and 19 for observer B, 27 were in between the same grade; 19 for grade 1 lesions, five for grade 2 lesions, and three for grade 3 lesions. There was no intra-rater disagreement in evaluating grade 4 and 5 lesions.
Discussion
In this study, we propose a new and detailed MRI grading system for chondromalacia patellae with corresponding high resolution FS PD and T2 mapping images, which might be useful in reporting and comparing knee MRI examinations in routine daily practice. We also present good inter-rater and good to very good intra-rater agreements when using this system. Naturally, multiple lesions could be observed in the same patella and we suggest each lesion to be graded separately.
Hyaline cartilage is divided into four somewhat arbitrary zones (16,17). The superficial zone makes up 3–12% of the cartilage thickness. The intermediate zone is thicker than the superficial zone. The deep zone is the thickest and represents over 50% of the cartilage thickness. The zone of calcified cartilage overlies the subchondral bone. However, with current MRI technology these zones are not well delineated even with very high resolution images in clinical practice (Fig. 12). Therefore, the value of 50% of the cartilage depth has been generally considered a practical landmark in chondromalacia grading systems both arthroscopically and radiologically.
Although many sequences have been used in MRI of the patellar cartilage and the optimal pulse sequence is controversial, FS PD images have been considered very valuable to evaluate patellar cartilage with high spatial resolution and good contrast-to-noise ratio in a reasonable scan time (2,3). T2 mapping, a sequence sensitive to T2 prolongation induced by cartilage degeneration, has been considered as effective in detecting very early patellar cartilage lesions although the technique is time consuming and has lower resolution (2,3,6,17). We currently use these two sequences in our daily practice for imaging of the patellar cartilage. There have been researches for revealing optimum sequence in detecting cartilage defects and for increasing the ability of MRI to detect very early patellar cartilage degeneration (5,6,18,19).
Early signs of patellar cartilage degeneration may be observed as hyperintense areas within the cartilage in FS T2-weighted (T2W) or FS PD images (2,3). Since T2 relaxation time is very sensitive to the integrity of collagen network, collagen content, and water content, these areas could be detected in T2 mapping sequence to a greater extent (3,5,14,18,20,21). Although T2 mapping is very sensitive in detecting cartilage lesions, due to its lower spatial resolution, type and depth of a lesion might not be well documented in comparison to FS PD images. There have been ongoing studies investigating this finding as an early indicator of knee osteoarthritis (20,21). Extent of these very early changes could not be determined in arthroscopy although some might be felt as softening in arthroscopic probing. On the other hand, in current MRI grading systems, any degree of intracartilaginous signal change is classified as a grade 1 lesion. However, percentage of early cartilage degeneration may be relevant in natural outcome or response to any therapy (21). Therefore, further subclassifying this finding based on percentage of the cartilage depth, as proposed in this study, may be helpful in comparing MRI examinations, monitoring therapy, and natural prognosis.
Current clinical and MRI grading systems for mild to moderate patellar chondromalacia are based on only depth of the chondral defect. Studies investigating natural course of the patellar chondromalacia and outcomes of different therapeutic approaches have been based on these basic gradings (13,14,22). Although most of the cartilage lesions remain in the same grade over a certain period of time or progress to a higher grade, natural course and response to various therapeutic approaches of mild and moderate patellar cartilage lesions based on current grading systems could not be well predicted (13,14). We believe that lack of specific definition of the chondral lesions in current grading systems may at least be one of the reasons not being able to exactly predict the prognosis. Type of the chondral lesion, which has been generally ignored in grading, might play a role in natural prognosis or response to any treatment as well as depth of the lesion might. For example, a chondral fissure might result in a different outcome than a chondral flap or defect with the same depth. Therefore, subclassifying patellar cartilage defects may enable us to make a more definitive diagnosis of patellar chondral lesions, and more precisely predict prognosis and clinical outcome of the patients. Likewise, full thickness cartilage defects with or without subchondral bony changes are generally classified in the same grade. However, presence or absence of subchondral fibrocystic changes may have an impact on response to any therapeutic interventional approach (23). Therefore, separating these full thickness defects into different grades might also help us more precisely classifying and monitoring these lesions.
Inter- and intra-observer reliability is a main feature of any grading system. Previous studies regarding reproducibility of MRI in detecting cartilage lesions revealed moderate to good degree of agreement (5,6,14,19,20). In comparison with the studies about reproducibility of the arthroscopical grading of chondral lesions, MRI based gradings result in better inter- and intra-observer reliability (24–26). In this study, we present good inter-rater and good to very good intra-rater reliability in grading cartilage lesions based on the proposed system. Use of high resolution images might have helped in reaching a high degree of inter- and intra-observer agreement. Getting used to this grading system may also further increase reliability.
There are several limitations of this study. Although, MRI is the best imaging method currently available for articular cartilage lesions and may also provide some biochemical information about the cartilage, arthroscopy is generally considered as the gold standard for making the diagnosis of patellar chondromalacia. Therefore, the main limitation of this study seems to be the lack of specific arthroscopical verification of MRI findings using this system. However, it is questionable for us that arthroscopy was superior to MRI in detecting and classifying all chondral lesions. Macroscopic appearance of the articular cartilage is evaluated in arthroscopy but it is insensitive to intrinsic degeneration that is not visible at the articular surface (21). Grade 1A and 1B lesions, as presented in this study, might not be detected by arthroscopic probing unless they were located superficially. Deeply located grade 1A and 1B lesions may represent grossly normal appearing patellar cartilage with histological degeneration those naturally have not been included in arthroscopy-based gradings (11,14,21). Therefore, arthroscopic grade 0 may not represent healthy cartilage and T2 mapping may be more valuable in the detection of very early cartilage degeneration. We believe that proper classification of grade 1 lesions could be possible only by MRI and by histological examination as the reference gold standard. Grade 2–4 lesions are very well detected by arthroscopy while MRI has also been proven to be accurate in detecting such lesions (5,6,14,20). Although grade 2 and 3 lesions are easily detected by arthroscopic examination, since the actual thickness of the cartilage could not be detected by arthroscopy in some patients and grading depends on the percentage of depth of the lesion, there might be some challenge in differentiating grade 2 lesions from grade 3 lesions solely by arthroscopy. High resolution MR images might provide a better differentiation between these lesions. Meanwhile, extent and nature of subchondral changes observed in grade 5 lesions could be better delineated with MRI than with arthroscopy. Therefore, superiority of arthroscopy over MRI in detecting and classifying all patellar chondral lesions might be questioned. We believe main limitation of this study is the lack of histological examination as the reference gold standard. Spatial resolution of T2 mapping in this study is relatively low due to its nature. However, a T2 mapping sequence with equally high resolution would last approximately 20 min and would not be practical in routine daily imaging. This study also lacks T1rho imaging which is also a sensitive method in detecting early cartilage changes (3). The limited number of patients evaluated in assessing reliability and reproducibility of this system and lack of correlation with physical examination are also limitations of the study. Further studies with large number of subjects verified with arthroscopy or preferably with histological examinations would be needed to investigate the reliability of the proposed grading system, its clinical relevance, and its ability to predict prognosis.
In conclusion, we present an MRI grading system for chondromalacia patellae with corresponding images which might be useful in reporting and comparing knee MRI examinations in routine daily practice and may also have the potential for using more precisely predicting prognosis and clinical outcome of the patients. Main differences of this grading that sets apart from the current clinical and MRI-based systems are its descriptive nature, distinct separation and subclassification of cartilage lesions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.