
Abstract
Background
Until now, no valid alternative exists for predicting central venous pressure (CVP) with lower invasiveness than central venous catheter.
Purpose
To explore inferior vena cava diameter (IVCD) measurement accuracy by ultrasonography as a surrogate variable for determination of central venous pressure (CVP).
Material and Methods
A systematic review and meta-analysis of all published studies in PubMed, Scopus, Web of Knowledge, and Google Scholar were conducted from inception to July 2013. We used the STROBE checklist for quality assessment and meta-regression.
Results
Thirty-seven papers with 2843 cases were identified. The correlation coefficients between each one of IVCD, inspiratory IVC (iIVC), IVC collapsibility index (IVCCI), and expiratory IVC (eIVC) with CVP, were 0.68, 0.60, 0.54, and 0.44, respectively. There was no evidence of publication bias (P = 0.28). Based on meta-regression, male gender was an important source of heterogeneity (OR = 1.01; 95% confidence interval, 1–1.03), which resulted in a higher correlation between IVCD and CVP. The present study showed a higher strength of association with CVP pertaining to IVCD, iIVC, IVCCI, and eIVC, respectively, and they were higher in men.
Conclusion
This study does not support the measurement of IVCD by ultrasonography as an acceptable surrogate variable to determine CVP among critical patients.
Introduction
Right atrial (RA) pressure is important in both gauging central volume and calculating pulmonary pressure (1).
Is the role of inferior vena cava diameter (IVCD) only useful in assessing volume status (2), or in determining central venous pressure (CVP) in addition? As the first statement is accepted worldwide, in this meta-analysis we focused on quantifying the usefulness of IVCD for estimating CVP and its associated factors.
There are many technical variations and situational changes that make this technique less reliable, including respiratory changes of IVCD (3–5), factors affecting vascular resistance (6), positions and maneuvers (7), heat and cold stress (8,9), treatments (10), and experience of the technician (usually a radiologist). These points are also mentioned in many original studies. However, no single study has focused on these issues to determine the real source of heterogeneity. We expect that these factors will have an effect on estimating the means of both IVCD and CVP. However, the correlation coefficient between IVCD and CVP may be unbiased. This can be tested only by a meta-analysis.
Finding a correlation between these two indices could be important, particularly in geographic regions where we have no data at all. More interestingly, finding sources of heterogeneity between studies and focusing on the correlation between IVCD and CVP will help us to understand the factors that influence this correlation, as they could be considered as confounders in future confirmatory studies. In this study, first we focused on a meta-analysis of published studies which tested an association between IVCD and CVP. Then, the sources of heterogeneity between the studies were evaluated.
Material and Methods
Search strategy and selection of studies
We searched PubMed (784 papers), Scopus (960 papers), Web of Knowledge (950 papers), Cochrane Library (no prior meta-analysis in this field), TRIP database (no prior meta-analysis in this field), and Google Scholar (first 50 pages were searched), from inception to 9 July 2013. The search sentence was: (“central venous pressure” [MeSH Terms] OR “central venous pressure” [MeSH] OR (“central” [All Fields] AND “venous” [All Fields] AND “pressure” [All Fields]) OR “central venous pressure” [All Fields]) AND (“ultrasonography” [MeSH Terms] OR “ultrasonography” [Mesh] OR “ultrasonography” [All Fields] OR “sonography” [All Fields] OR “imaging” [All Fields]).
References within the original reports and review articles were checked. We also evaluated “related citations” of articles when we searched PubMed for additional studies. The primary search was not limited to studies using human participants or English language only; animal studies, studies on fetuses or infants, reviews, letters, or case reports were not excluded in this phase. In the final inclusion process, the eligibility criteria included all related studies with any association between IVC and CVP, except for animal studies, studies on fetuses or infants, reviews, letters, or case reports. The search strategy was designed to also include letters with new or revised information, however, no such letters were found.
Exclusion of non-related papers was made based on screening titles, abstracts, and full texts in three consecutive stages. Decision to include/exclude papers was made by two independent but matched (according to sessions with all other authors) reviewers. In cases with disagreement, the points of difference were discussed and if there was still disagreement, a third person was involved in determining whether the article was relevant.
Critical appraisal
Two independent, matched trained reviewers (AK, MM) read all papers and scored them according to the STROBE checklist (11) (Appendix 1). They entered into discussion when their score was different by more than one point on each paper. A third person participated in the sessions when a disagreement was not resolved.
Papers were categorized; without quality (score <2/10), low, moderate, and high quality (2–4, 5–7, and >7, respectively) from a total score of 10. We excluded papers without acceptable quality (score <2) from the meta-analysis. The analysis was run on all papers and also separately on papers with different qualities.
Data extraction and data synthesis
Two independent matched reviewers (AK, MM) extracted data from papers based on the checklist provided by all of the authors. First, five papers were read by both reviewers in the same place to produce higher agreement. Disagreements were solved by discussion. Data about quality assessment score, continent, country, district, type of study, year of study, publication year, sample size, sampled population, male percentage, mean age, age range, IVCD detection method, CVP detection method, mean IVCD, mean inspiratory IVC (iIVC), mean expiratory IVC (eIVC), IVC collapsibility index (IVCCI), patient position in which the indices were measured, and their standard deviation (SD), standard error (SE), or 95% confidence interval (CI), as well as their P values were also extracted from studies whenever possible.
Statistical analysis
All analyses were performed with Excel, StatsDirects version 2.8.0 and Stata 11.0 software (STATA Corp. LP, College Station, TX, USA). Quantitative variables were expressed as mean and 95% CI. For assessment of heterogeneity between the studies, we used the Cochrane’s Q test. Quantitative value of the heterogeneity was expressed using I2. We used the DerSimonian and Laired method (random effect analysis) for heterogeneous indices and the inverse variance method (fixed effect analysis) when they were not heterogeneous.
For assessment of publication bias, the Egger, Begg, and Funnel plot was used. The trim and fill method was also used for correction of publication bias when there was evidence of bias.
Meta-regression was used to either explore the most important variables affecting the correlation between IVCD and CVP or to quantify heterogeneity explained by the available covariates in the study. The significance level was set at 0.05 for all statistical tests except for heterogeneity and publication bias, which were 0.1.
Results
Search strategy findings
There were 2694 papers with 1420 duplications (indicative of a high sensitivity search strategy). After screening the titles, 189 papers remained. Screening abstracts and full-text papers resulted in 110 excluded abstracts and 42 excluded full-text papers. One paper was a duplicate of another study without any new content and two others were clinical commentaries (Suppl. Fig. 1). Forward-backward citation added three related papers. We did not have access to the full text of five papers. The abstract of one of these papers was not available and the abstract of another was not informative. As Supplementary Fig. 1 and Table 1 show, 35 papers were included in meta-analysis (1,3), (Suppl. ref. 1–35). However, we had some dependent variables like IVCD, eIVCD, and iIVCD. Six of these 35 papers had information about IVCD. Another 22 studies had information about eIVCD. Another 31 studies had data about CVP (Table 1). These studies had some overlap but not completely match with each other. As a whole, there were 35 papers that we could use their data in different parts of our meta-analysis.
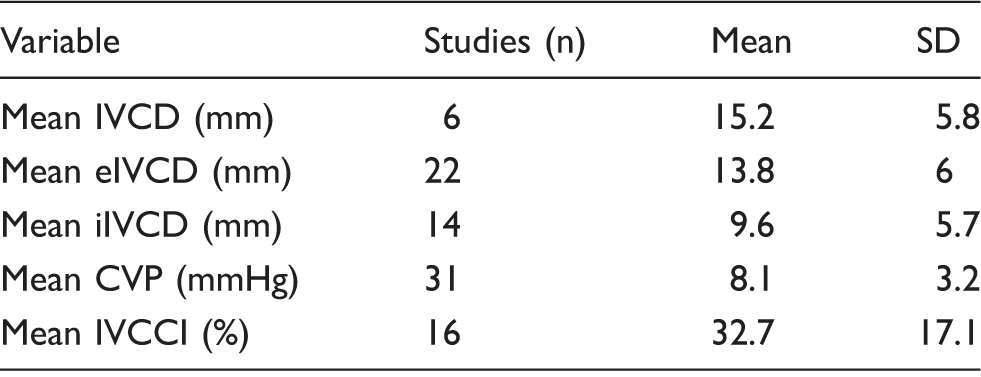
Results of searching the literature to assess the correlation between inferior vena cava diameter and central venous pressure Basic characteristics of included study in assessment of association between IVCD and CVP. CVP, central venous pressure; eIVCD, end-expiratory inferior vena cava diameter; iIVCD, end-inspiratory inferior vena cava diameter; IVCCI, inferior vena cava collapsibility index; IVCD, inferior vena cava diameter; SD, standard deviation.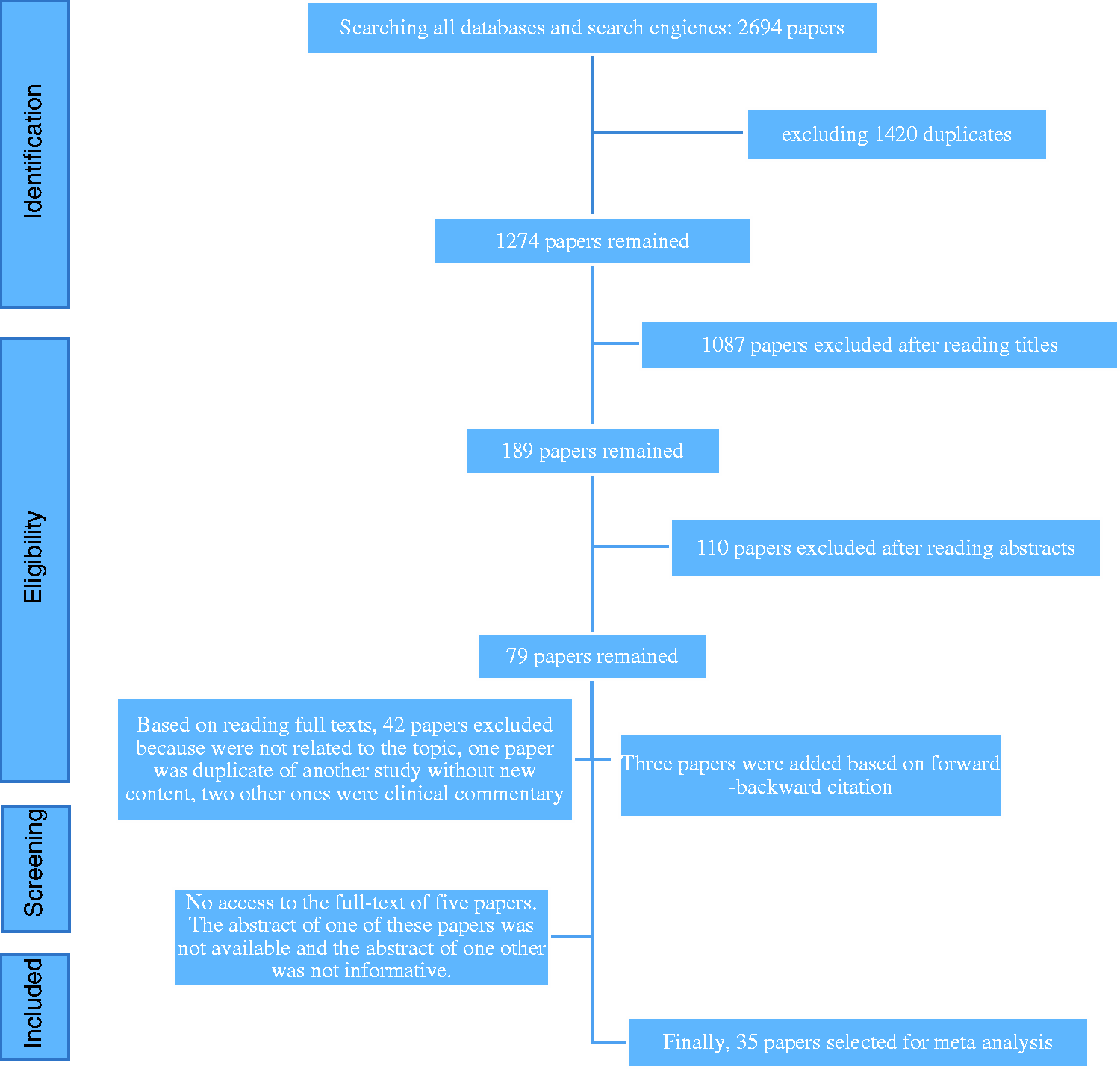
Description of included studies
In total, 2843 cases were included in this meta-analysis. Their mean (SD) age was 53.2 (+/–17.4) years (range, 6 months–97 years). Of these, male percentage was mentioned in 31 studies with a mean age of 59.5 ± 13.8%. The quality of 23 studies was high and in 13 studies intermediate. Mean IVCD and CVP were 15.2 mm and 8.1 mmHg, respectively (Table 1).
Correlation between IVC, IVCCI, iIVC or eIVC, and CVP
Some studies mentioned correlation coefficients according to their different sub-samples, resulting in more than one correlation coefficient from some studies. Twelve studies mentioned correlations between IVCD and CVP in the range of 0.27–0.92, and the mean was 0.68 (95% CI, 0.58–0.77). This index was heterogeneous between studies (Q test: P = 0.005, I2 = 54.5%). This correlation was slightly higher in Europe than in the USA, and was lowest in Asian countries (Suppl. Fig. 2). Meta-regression showed that this difference was not significant (P = 0.308). An interesting finding was that the date studies were started in this field in the USA was older than European and Asian publications, which were started in recent years (Suppl. Fig. 2).
The correlation between IVCD and CVP was independent of mean IVCD (P = 0.811), mean CVP (P = 0.312), mean age (P = 0.52), position of the patients during measurements (P = 0.369), quality of the study (P = 0.725), and sample size (P = 0.105). Despite such non-significant associations, when we adjusted each one of these variables separately in our meta-regression, the male percentage no longer had a significant effect on the correlation between IVCD and CVP. Based on the meta-regression, the male percentage had a significant effect on the correlation between IVCD and CVP (OR = 1.01; 95% CI, 1–1.03; t: 2.79; P = 0.049). Tau-square of this meta-regression was 0.005, percentage of residual variation due to heterogeneity (I-square residual) was 13.3%, and adjusted r-squared was 84.1%. Completion year/publication year did not have any significant effect on the correlation between IVCD and CVP during the last decades.
Mean (95% CI) absolute value (without considering the direction of the association) of the correlation between IVCCI and CVP in 14 studies was 0.54 (0.44–0.65), which was heterogeneous (P < 0.001, I2 = 64.9%) (Suppl. Fig. 3). When we considered the main values mean (95% CI) of the correlation coefficient, it was 0.15 (–0.12–0.41), which was heterogeneous (P < 0.001, I2 = 95%). The correlation between iIVC and CVP was 0.60 (0.51–0.68) in 10 studies, which was not heterogeneous (P = 0.6, I2 = 0%) (Suppl. Fig. 4); however, between eIVC and CVP this was 0.44 (0.35–0.54) in nine studies and again it was not heterogeneous (P = 0.14, I2 = 34.8%). (Suppl. Fig. 5)
We compared correlation coefficients between each one of the IVC, IVCCI, iIVC, or eIVC and CVP in different quartiles of quality score of the studies. There was no pattern.
Publication bias
Egger test for evaluation of publication bias in assessing the correlation between inferior vena cava diameter (IVCD), IVC collapsibility index (IVCCI), inspiratory IVC (iIVC), or expiratory IVC (eIVC) and central venous pressure (CVP).

CVP, central venous pressure; eIVCD, end-expiratory inferior vena cava diameter; iIVCD, end-inspiratory inferior vena cava diameter; IVCCI, inferior vena cava collapsibility index; IVCD, inferior vena cava diameter.
Discussion
This study showed that IVCD measurement by ultrasonography is an acceptable surrogate variable for determination of CVP. Also, this study showed a moderate correlation between IVCD and CVP. Other indices, such as iIVC, IVCCI, and eIVC, also had moderate but lower strength of correlation than IVCD with CVP, respectively.
According to our meta-regression, none of the factors, such as continent, year of the study’s completion or publishing, age, position of the patients during measurements, quality of the study, and sample size, were known sources of heterogeneity.
Although there was no analysis of different sexes in 35 studies of our meta-analysis, we conducted a meta-regression that included male percentage as an independent variable. This analysis showed that studies with higher percentages of male gender had a higher correlation between IVCD and CVP. Every one-unit increase in male percentage will cause this correlation coefficient to be multiplied by 1.01. Therefore, we can consider sex as an effect modifier in this association. Based on this finding, we suggest that subgroup analysis be carried out in future studies in order to assess the correlation between IVCD and CVP.
One paper with a sufficient sample size in the subgroups showed that the correlation between CVP and IVC index is highly dependent on the status of the patients (Suppl. ref. 19). In this study, non-ventilated patients (n = 133) had the highest Pearson’s correlation (r = 0.97) in comparison with ventilated cases (n = 344, r = 0.59) and patients with right ventricle (RV) enlargement (n = 78, r = 0.39) (Suppl. ref. 19). Other studies also showed that this correlation was significant in cases with spontaneous breathing; but, not in patients with mechanical ventilation (Suppl. ref. 9, 14, 15). Moreover, one study showed that normalized, IVC diameter for body weight (BW), body surface area (BSA), and even body length (BL) had a lower correlation coefficient with CVP (Suppl. ref. 15). On the other hand, some studies like Brennan et al. (Suppl. ref. 11) showed that adjustment of the IVC size for BSA did not significantly improve the accuracy of CVP prediction. Furthermore, another study expressed a better correlation in patients with depressed right ventricle function (RVF) in comparison with cases by normal RVF (Suppl. ref. 2). As a future research-oriented focus, we need to consider the situations that affect this association.
One study showed that IVCCI had the best predictive value (both highest area under the curve [AUC] and Youden index) in determining cases with increased CVP in comparison with maximum, minimum or expiratory and inspiratory IVCD solely (Suppl. ref. 15).
IVCCI and AUC had a higher accuracy in comparison with iIVC and eIVC for the prediction of CVP. However, its correlation with CVP was lower than the two other variables (Suppl. ref. 11). Another study showed a higher correlation for IVCCI in comparison with iIVC, IVCD, and eIVC (Suppl. ref. 31). Our meta-analysis showed that the correlation between IVCCI and CVP was lower than IVCD and iIVC, but higher than eIVC.
There were obvious mistakes in some of the papers assessed; for instance, in De Lorenzo et al., in which the mean IVCD was lower than minimum IVCD in their study (Suppl. ref. 12). Another smaller issue was that nearly all of the studies which assessed the correlation between CVP and IVCD quantitatively used a Pearson’s correlation coefficient; however, some studies had a very low sample size, specifically in their subgroups, and it seems that they should have used a Spearman’s or Kendall’s correlation coefficient.
Maybe one important rational for observing the weak correlation between IVCD and CVP in some studies is the different situations observed in these studies. Several studies have evaluated this association in spontaneous breathing cases, while others investigated mechanically ventilated patients. Some evaluated CVP by invasive methods and others by non-invasive methods. There were those that evaluated IVC as total and others as maximum and minimum IVCD at end-expiration or end-inspiration. One study, which evaluated IVC from different radiological views (longitudinal or transverse subxiphoid, midpoint, and suprailiac), showed a wide range of correlation coefficients in the range of 0.34–0.67 (Suppl. ref. 12). Another study showed a higher correlation coefficient (r = 0.86) when IVCD was measured at the cavo-atrial junction (Suppl. ref. 2). Closer anatomic placement to the right atrium for measurement of IVCD may cause higher correlation coefficient because cavo-atrial junction is closer to right atrium (actual place of CVP assessment) and measurement of IVCD at this point has caused higher correlation coefficient between IVCD and CVP. As a result, all of these factors explain some sources of heterogeneity, which should be considered when reporting results.
It has also been shown that one other source of heterogeneity in these studies is due to the ultrasonographic methodology (M-mode or 2-dimensional echocardiogram) used and the timing of measurement during the cardiac cycle (Suppl. ref. 4).
Most of the studies which evaluated the indices in greater detail focused only on IVCD in inspiration (minimum) and expiration (maximum), but one Iranian study which also evaluated CVP in both inspiration and expiration showed higher, although not significant, differences in expiration as compared to inspiration (Suppl. ref. 22).
One of the limitations of some of these studies was that the IVCD and hemodynamic status were not evaluated simultaneously. Therefore, the previously mentioned correlation between these indices could have been confounded by this issue. Another limitation was that there was no point concerning the correlation between IVCD and CVP according to the sexes in any of the included studies. The strength of this association is different in each sex. As a result, we suggest that this relationship is analyzed according to sex in future or even in previously published papers, because we believe that they contain such data.
In conclusion, our results showed only moderate correlation between IVCD, IVCCI, iIVC, or eIVC and CVP, and do not support the measurement of IVCD by ultrasonography as an acceptable surrogate variable to determine CVP among critical patients. However, the validity of this index for predicting CVP is still under question.
Supplemental Material
sj-pdf-1-acr-10.1177_0284185116663045 - Supplemental material for Ultrasonography of inferior vena cava to determine central venous pressure: a meta-analysis and meta-regression
Supplemental material, sj-pdf-1-acr-10.1177_0284185116663045 for Ultrasonography of inferior vena cava to determine central venous pressure: a meta-analysis and meta-regression by Mostafa Alavi-Moghaddam, Ali Kabir, Majid Shojaee, Mohammad Manouchehrifar and Mehrdad Moghimi in Acta Radiologica
Supplemental Material
sj-pdf-2-acr-10.1177_0284185116663045 - Supplemental material for Ultrasonography of inferior vena cava to determine central venous pressure: a meta-analysis and meta-regression
Supplemental material, sj-pdf-2-acr-10.1177_0284185116663045 for Ultrasonography of inferior vena cava to determine central venous pressure: a meta-analysis and meta-regression by Mostafa Alavi-Moghaddam, Ali Kabir, Majid Shojaee, Mohammad Manouchehrifar and Mehrdad Moghimi in Acta Radiologica
Footnotes
Supplementary material
Supplementary material is available at: acr.sagepub.com/supplemental.
Acknowledgements
We would like to thank all of our colleagues and authors who cooperated with us by preparing the full text of the papers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.