
Abstract
Background
Parathyroid carcinomas (PTC) are very rare. There have been a few studies on the contribution of ultrasound (US) in the diagnosis of PTC compared with parathyroid adenomas (PTA).
Purpose
To identify the differences between US findings of PTC and PTA in patients with primary hyperparathyroidism (PHPT).
Material and Methods
We enrolled seven patients with PTC and 32 consecutive patients with PTA whose diagnoses were confirmed by surgery at our institution between March 1994 and June 2015. We retrospectively compared the US features of the two groups, as well as the demographic, clinical, and biochemical characteristics (age, gender, palpability, and serum ionized calcium and parathyroid hormone [PTH] levels).
Results
The patients with PTC and PTA did not exhibit significant differences in terms of mean age (59.0 years versus 51.1 years; P = 0.2063), sex distribution (male:female, 4:3 versus 1:3; P = 0.1716), mean PTH levels (2855.0 pg/mL versus 1821.5 pg/mL; P = 0.2067), and mean ionized calcium levels (1.7 mMol/L versus 1.5 mMol/L; P = 0.1585) except palpability (P < 0.0001). On US images, the PTCs were significantly larger (3.5 cm versus 1.9 cm; P = 0.0133) and exhibited higher incidences of heterogeneous echotexture (P = 0.0002), irregular shape (P < 0.0001), non-circumscribed margin (P < 0.0001), intra-nodular calcifications (P = 0.014), and local invasion (P = 0.0004) compared to the PTAs.
Conclusion
In preoperative patients with PHPT, PTCs are differentiated from PTAs by their palpability and significant US features: large size, heterogeneous echotexture, irregular shape, non-circumscribed margin, intra-nodular calcifications, and local invasion.
Introduction
Parathyroid carcinoma (PTC) is a rare malignant neoplasm which affects 0.5–5.0% of the patients with primary hyperparathyroidism (PHPT) (1). Although patients with PTC have a long duration of survival, they undergo several operations because of the high rates of recurrence and surgical complications associated with the disease (2). Complete surgical extirpation is the only known curative modality, and the outcome of PTC strongly depends on the surgical approach during initial surgery (3,4). In order to avoid local recurrence, the lesion must be removed en bloc with safe margins (5). Bilateral parathyroid exploration was the standard method for parathyroid surgery until the introduction of the minimally invasive and focused parathyroidectomy. Due to its critical effect on the surgical outcome, the need for accurate preoperative diagnosis of parathyroid pathology has increased (6,7). When a lesion is excised without ascertaining its non-malignancy, there might be a greater likelihood of its re-implantation and recurrence (8).
Ultrasonography (US) and radionuclide (99mTc-sestamibi) imaging are the most widely used tools for detecting parathyroid abnormalities in patients with PHPT (6,7). Although US plays a major role in the pre-surgical localization of parathyroid masses, US has shown low specificity for differentiating PTC from its benign entities, such as adenoma or hyperplasia (7,9,10).
The most common cause of PHPT is solitary parathyroid adenoma (PTA), which accounts for 85–90% of PHPT cases (11,12). Therefore, the differentiation of PTC from PTA is important when determining the operative strategy as well as predicting the clinical outcome (13). Many studies have reported the preoperative localization of PHPT lesions on the basis of biochemical data and scintigraphy findings (6,7,9,14–16). Some studies have shown the role of US in assisting preoperative differentiation of PTC and PTA of PHPT (10,17,18). In these studies, well-known aggressive features such as large size and marginal irregularity with local tissue invasion were more common in PTC than in PTA. However, these studies did not review the US features in conjunction with the biochemical data of the patients. The performance of US has markedly improved in the last years with the development of high-frequency and high-resolution probes. In this study, we attempted to identify the differences between PTC and PTA in the preoperative analysis of patients with PHPT, in terms of US findings, as well as demographic, clinical, and biochemical characteristics.
Material and Methods
Patients
This retrospective study was approved by our institutional review board and the need for informed consent from the patients was waived. Of the 263 patients who underwent surgery for the excision of parathyroid masses at the same institute between March 1994 and June 2015, seven (2.7%) were diagnosed with PTC and 256 (97.3%) with PTA or parathyroid hyperplasia. We enrolled 38 consecutive patients who were diagnosed with PTAs after surgery between June 2014 and May 2015 at our institution as the control group; of these 38 patients, three with secondary hyperparathyroidism and three with negative US findings were excluded. The study group consisted of 39 patients (27 women, 12 men) with PTC (n = 7) and PTA (n = 32), with mean ages of 59 years (age range, 39–73 years) and 51 years (age range, 28–75 years), respectively.
Preoperative US examination and data analysis
All of the patients were subjected to preoperative US examinations with either the HDI 5000 or iU22 scanners (Philips Medical Systems, Bothell, WA, USA) or the Logiq 700 scanner (GE Healthcare, Little Chalfont, UK) equipped with a 7–12 MHz linear transducer. Anterior neck scanning was performed from the mandibular angle (or above the carotid bifurcation) to the sternal notch to cover the possibilities of ectopic parathyroid location, by experienced radiologists, and both longitudinal and transverse images were acquired.
The US findings were retrospectively reviewed in consensus by two radiologists with 8 and 15 years of experience in thyroid imaging. They analyzed the US findings to evaluate the following factors: echogenicity (hypoechoic, isoechoic, or hyperechoic compared to the thyroid), echo-texture of the solid portion (homogeneous or heterogeneous), size (width and depth on the transverse scan and the longest diameter in the three dimensional view), shape (round to oval or irregular), margin (circumscribed or non-circumscribed), presence of calcifications in the mass, existence of suspicious lymph nodes in the central and lateral regions of the neck, presence of local infiltration, and location of the masses. The mass sizes had been measured in three planes and recorded by the initial observers; the depth and width of the masses were measured again on the transverse images by the reviewers in the present study in order to obtain the depth/width (D/W) ratios. The D/W ratio were calculated as proposed by Hara et al. in order to evaluate their efficacy for differentiating malignancies from benign masses (17).
The preoperative levels of serum ionized calcium (Ca) and parathyroid hormone (PTH) measured by the ion-selective electrode method and chemiluminescent immunoassay, respectively, were recorded. The palpability of masses and demographic data of the patients were recorded, including the age and sex.
Statistical analysis
The US findings of PTC and PTA were compared by univariate logistic regression analysis. Comparison of the distribution of the sexes, echotexture, shape, margins, echogenicity, presence of calcifications in the masses, existence of suspicious lymph nodes, presence of local infiltration, palpability, and the location of masses between the two groups was performed using the Fisher’s exact test or Chi-square test. Statistical analyses of the differences between the two groups in terms of the patient age at the time of surgery, levels of the serum ionized Ca and PTH, D/W ratios, and longest dimension of the masses were performed using the Wilcoxon Mann–Whitney test. A P value <0.05 was considered as indicating statistical significance. We evaluated 64 combinations of six selected parameters with P values <0.05 and calculated their diagnostic performance values and accuracy using the Fisher’s exact test. The analyses were executed using the SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and the R 3.2.1 (Vienna, Austria; http://www.R-project.org) software.
Results
Comparison of the demographic, clinical, and biochemical characteristics of the patients with parathyroid carcinomas (PTC) and adenomas (PTA).
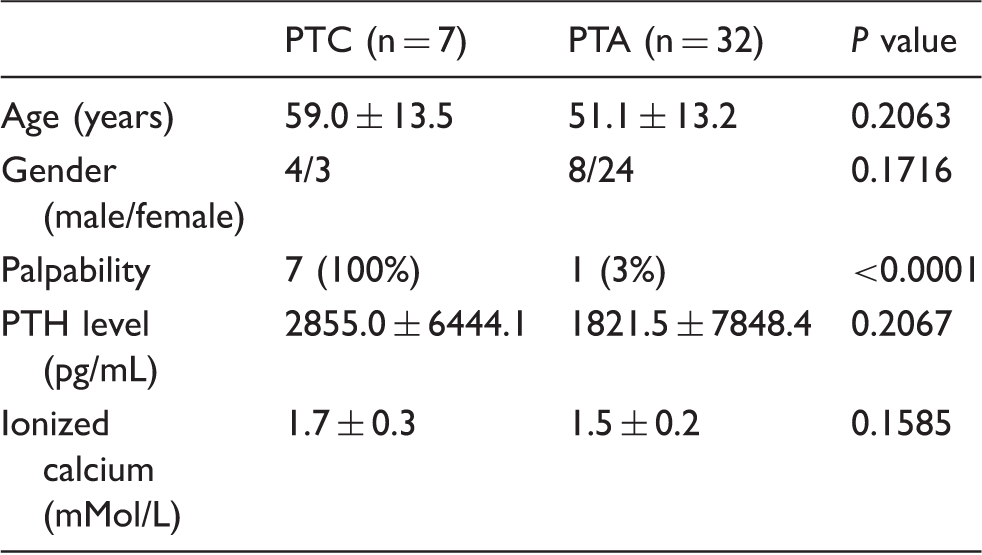
Values are presented as mean ± SD or n (%).
PTH, parathyroid hormone.
Comparison of the ultrasonographic (US) features of the patients with parathyroid carcinomas (PTC) and adenomas (PTA).
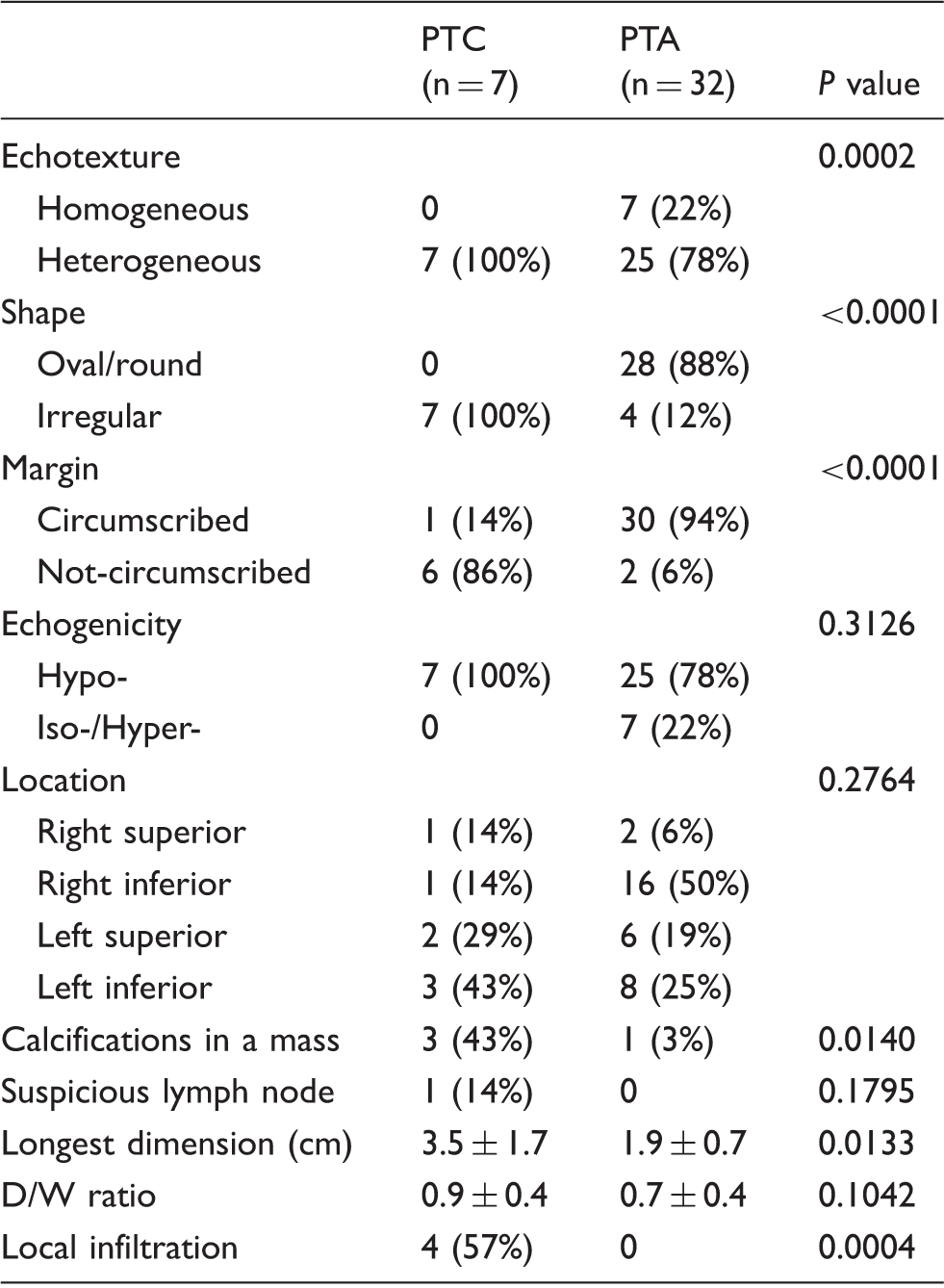
Values are presented as mean ± SD or n (%).
D/W ratio, depth/width ratio on the transverse scanning images.
The mean D/W ratios, which were calculated as proposed by Hara et al. (17) were not proven to be efficient predictors of PTC or PTA in our study (0.9 ± 0.4 versus 0.7 ± 0.4; P = 0.1042). However, the mean value of the longest dimension of the masses of the seven patients with PTC was significantly greater than that of the 32 patients with PTA (3.5 ± 1.7 cm versus 1.9 ± 0.8 cm; P = 0.0133).
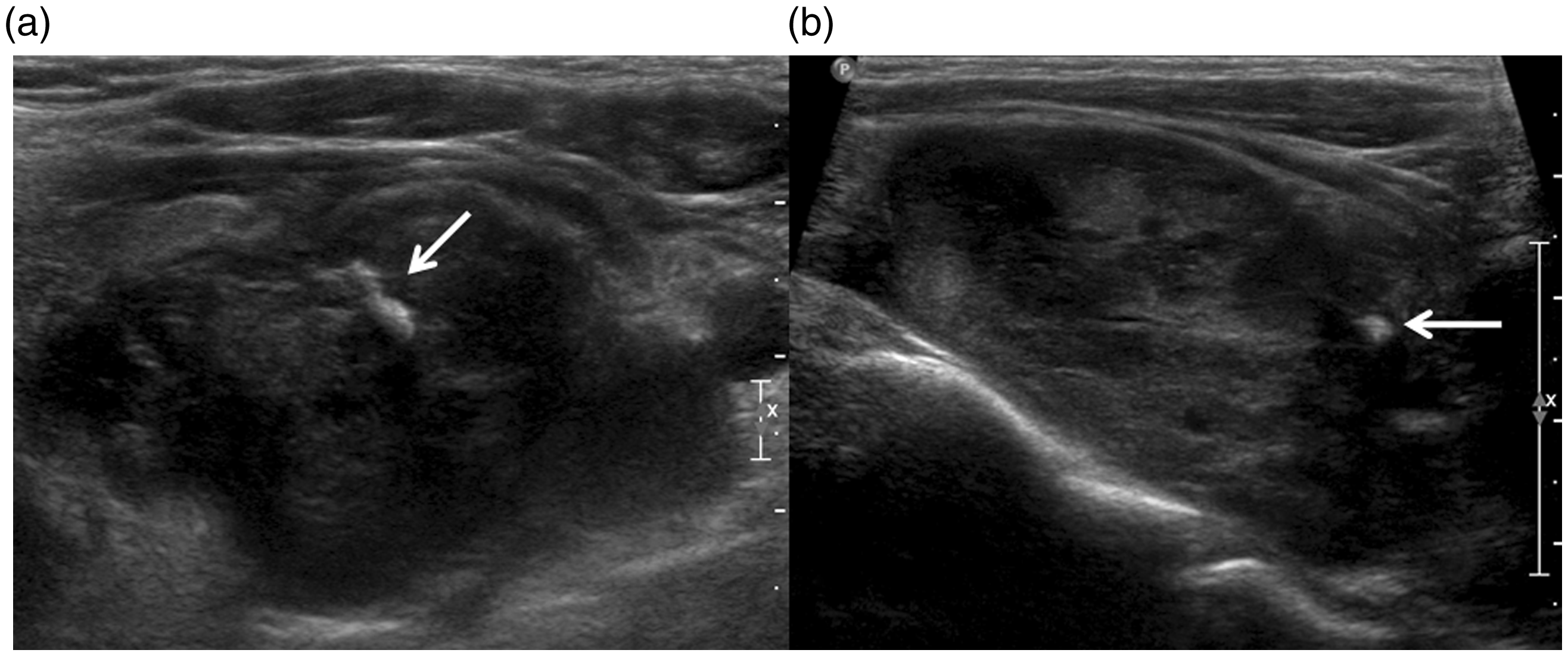
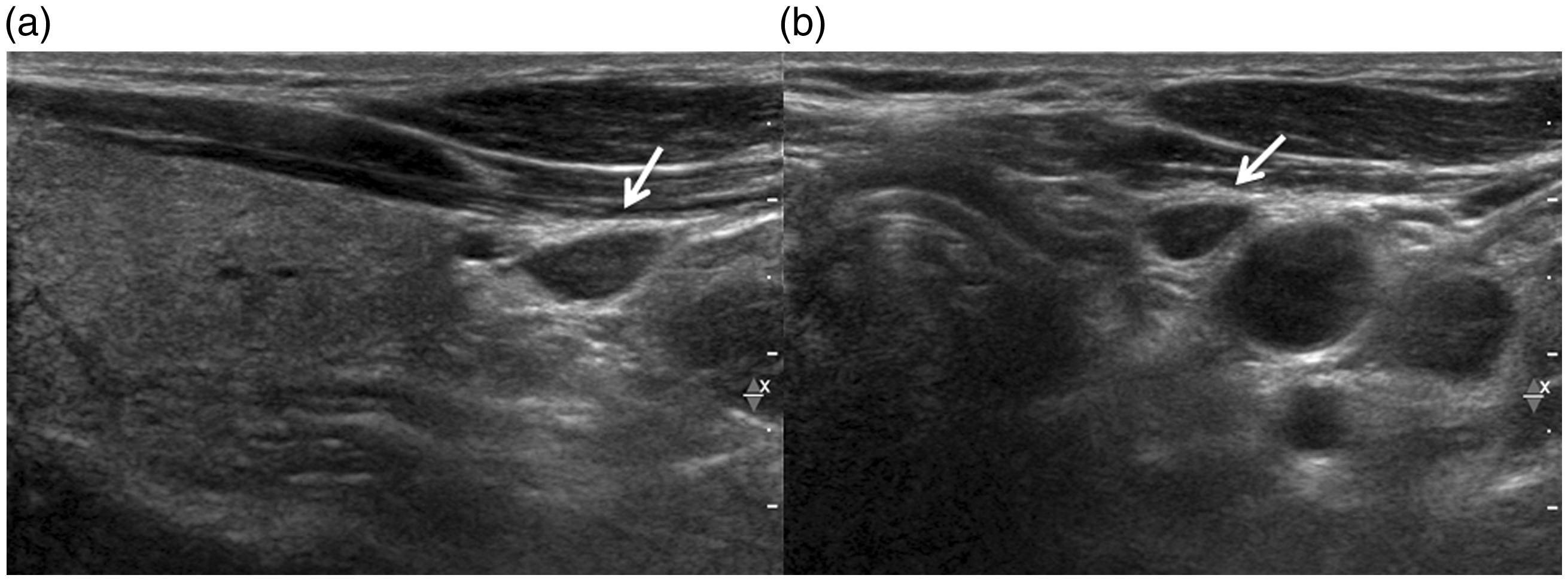
The analysis of the US findings revealed that, compared to the PTAs, a significantly greater number of PTCs presented heterogeneous echotexture of the solid portion (P = 0.0002), irregular shape (P < 0.0001), non-circumscribed margins (P < 0.0001), presence of calcifications in the masses (P = 0.014), and local infiltration (P = 0.0004) (Figs. 1 and 2). However, there were no significant differences between the two groups regarding the echogenicity (P = 0.3126), the location of the masses (P = 0.2764), and the presence of suspicious lymph nodes (P = 0.1795). Evaluation of the selected parameters in combination revealed that a mass with a homogeneous echotexture, oval or round shape, circumscribed margins, no calcifications, no palpability, no local invasion had a high probability of being a PTA (Fig. 3), whereas, a mass with a heterogeneous echotexture, irregular shape, non-circumscribed margins, calcifications, palpability, and local invasion had a high probability of being a PTC; the diagnostic performance values of US for the differentiation of PTC and PTA were as follows: sensitivity 100% (7/7), specificity 96.9% (31/32), positive predictive value (PPV) 87.5% (7/8), negative predictive value (NPV) 100% (31/31) with the accuracy 97.4% (38/39). Of the seven patients with PTC, four (57.1%) experienced recurrence or metastasis: three occurred near the original site of the operation, and one was located in the contralateral neck. One of them died of air way obstruction due to recurred PTC, 6 months after the first operation. The mean follow-up period was 4.8 years (range, 0.6–11.5 years).
Parathyroid carcinoma in a 73-year-old man. Transverse (a) and longitudinal (b) ultrasonographic images show an irregular-shaped 3.5 × 2.0 × 1.5 cm palpable mass with heterogeneous echotexture, internal calcifications (arrow), and local infiltration. Parathyroid carcinoma in a 70-year-old man. Transverse (a) and longitudinal (b) ultrasonographic images show an irregular-shaped 7.5 × 5.0 × 4.5 cm palpable mass with heterogeneous hypoechoic echotexture, internal calcifications, and local infiltration (arrows). Parathyroid adenoma in a 50-year-old man. Transverse (a) and longitudinal (b) ultrasonographic images show a small, circumscribed, homogeneous, hypoechoic mass (arrows) in the left infrathyroid area.
Discussion
We analyzed the US features according to the currently accepted criteria for the diagnosis of PTC and attempted to identify the differences between PTC and PTA on the basis of the results of biochemical analysis. Several studies have reviewed the US features of PTC in comparison to its benign entity (1,10,17,18) and emphasized the value of preoperative US examination in patients with PHPT (6,7,16,19,20). Although there is no critical threshold for predicting PTC, the size of the lesions has been suggested to be its most reliable US feature thus far. Sidu et al. suggested that parathyroid masses larger than 15 mm on US images were predictive of PTC (10). O’Neal et al. reported that large parathyroid tumors weighing equal to or more than 2 g are at a higher risk of being atypical or carcinomas (13). However, the weight of the masses cannot be measured in a preoperative situation. Our study produced similar results regarding the size of the masses — the mean longest dimension of the PTCs was greater than that of the PTAs (3.5 ± 1.7 cm versus 1.9 ± 0.8 cm; P < 0.013). Unfortunately, because of the small sample size, we were unable to evaluate the cutoff value of the tumor size that can predict malignancy.
Hara et al. assessed the D/W ratios of 16 PTCs and 61 PTAs (17). In their study, the mean D/W ratios of the PTCs and PTAs were 1.21 (range, 0.91–2.5) and 0.64 (range, 0.33–1.47), respectively. The authors concluded that a D/W ratio ≥1 is likely to be indicative of malignancy and supported their results with previously reported similarities in the characteristics of malignant breast lesions (21). In our study, the mean D/W ratios were 0.9 in seven cases of PTC and 0.7 in 32 cases of PTA; the difference between the two groups was not statistically significant (P = 0.1042). The D/W ratio is a similar concept as the taller-than-wide feature of small masses that often grow against the plane of the normal thyroid or breast parenchyma. Our data did not indicate a similar growth pattern of PTC because we believed that the malignant masses were too large for the assessment of their ratios.
In this study, the characteristics of the evaluated PTCs in terms of the echotexture (P = 0.0002), shape (P < 0.0001), margins (P < 0.0001), calcifications in the masses (P = 0.014), and local infiltration (P = 0.0004) were found to be in accordance with the widely accepted US features of PTCs (17,18); however, the two groups showed no significant differences in the echogenicity (P = 0.3126), presence of suspicious lymph nodes (P =0.1795), and location of masses (P = 0.2764). Hypo-echogenicity of the masses was not a specific feature of the PTCs evaluated in our study; all of the PTCs, including the smallest mass, showed heterogeneous echotexture. It appears that the improvements in high-resolution US technology and skillful evaluation made possible the precise interpretation of the echogenicity and echo-texture of the masses in the present study. Therefore, we concluded that findings of large (mean size, 3.5 cm), irregular, non-circumscribed masses with heterogeneous echo-texture, accompanied by calcifications and local infiltration, on the preoperative US images of patients with PHPT were suggestive of PTC.
Parathyroid carcinomas are known to have an equal frequency of occurrence in both sexes and are usually diagnosed in the fifth decade of life (22); they are characterized by high levels of serum ionized Ca and PTH (14,22). In our study, there were no significant differences in the mean age and the distribution of sex between the two groups. The mean ages of both groups (PTC, 59.0 ± 13.5 years; PTA, 51.1 ± 13.2 years) in the present study were higher than those of the study populations in the previous studies. Several studies have reported that patients with PTC present with higher serum ionized Ca and PTH levels than do patients with PTA (8,23,24). In our study, there were no statistically significant differences in the intact PTH and ionized Ca levels between the patients of the PTC and PTA groups.
There are some limitations of this study. First, this was a retrospective study; a prospective analysis might provide more data to evaluate the value of US. Second, the sample size of each group was small because of the rarity of occurrence of PTC. Third, we did not include the findings of radionuclide scanning, which is one of the main diagnostic tools for parathyroid lesions, in our data analysis. Radionuclide scintigraphy would have been superior to US for the identification of ectopic parathyroid lesions. Fourth, the control group of PTA were examined with a new generation of US machine while two of seven patients with PTC were examined with an older machine. This difference of US generations could be a potential bias owing to different resolution. However, the influence of two generations of US machines in this study is probably limited.
In conclusion, PTCs are differentiated from PTAs by their US features and palpability in the preoperative evaluation of patients with PHPT. In our study, PTCs significantly presented as large palpable masses with heterogeneous echotexture, irregular shape, non-circumscribed margin, calcifications, and local invasion on the US images. In these patients, more aggressive surgical treatment is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.