
Abstract
Background
Multimodality magnetic resonance imaging (MRI) is an imaging technology that is used to integrate the structural and functional information of lesions. MRI can determine the staging of endometrial carcinoma, provide guidance for selection of surgical treatment and postoperative prognostic assessment, and has an important role in improving the survival of patients with endometrial carcinoma.
Purpose
To evaluate multimodality MRI staging accuracy for endometrial carcinoma based on the International Federation of Gynecology and Obstetrics (FIGO 2009) staging system.
Material and Methods
This is a retrospective study of the complete clinical and surgical pathology data from 83 patients with endometrial carcinoma treated between June 2011 and August 2015. Using a blind design, the preoperative clinical staging according to the current FIGO2009 MRI-based staging for each endometrial carcinoma was analyzed and corrected by postoperative histopathological results, which served as the staging standard. The role of multimodality MRI on clinical staging accuracy for endometrial carcinoma was studied.
Results
Based on the pathological evaluation after surgery, the 83 endometrial carcinoma patients were staged according to the current FIGO2009 staging criteria as: stage I, n = 56; stage II, n = 17; stage III, n = 7; and stage IV, n = 3. The multimodality MRI staging accuracy for endometrial carcinoma stages I–IV by FIGO2009 were 91.6% (76/83), 91.6% (76/83), 92.8% (77/83), and 97.6% (81/83), respectively.
Conclusion
Multimodality MRI is an important imaging tool in the pre-operative clinical staging of endometrial carcinoma. The current FIGO staging system appears to be a concise, reasonable, and practical set of criteria for the clinical management of endometrial carcinoma.
Introduction
Endometrial carcinoma accounts for 20–30% of female reproductive malignant tumors (1). Prognosis and survival to endometrial carcinoma are closely related to the depth of myometrial invasion, histological grade, and clinical staging (2). Fractional diagnostic curettage, hysteroscopy, and transvaginal ultrasonography (TVS) play a role in the measurement of the depth of myometrial invasion, but these modalities are unable to determine the degree of myometrial invasion, surrounding tissue infiltration, and pelvic and para-aortic lymph node metastases.
Multimodality magnetic resonance imaging (MRI) can fully display the anatomic structures and signal characteristics of uterine and surrounding tissues. The degree of tumor infiltration is related to the tumor histopathological type and grade (3,4). MRI is able to demonstrate the functional metabolism of the tumor in relation to the histopathological type and grade (3,5).
There are a number of studies about preoperative MRI staging of endometrial carcinoma (6–8), but these studies are limited to results based on the 1988 or 2000 staging system. In May 2009, the International Federation of Gynecology and Obstetrics (FIGO) formally announced the current FIGO staging system (9). Therefore, previous results with previous staging systems need to be updated.
Therefore, the aim of this study was to assess the multimodality MRI features of 83 patients with endometrial carcinoma. Each MRI staging finding was compared with the postoperative histopathological results.
Material and Methods
Study design
This study involved 94 patients with endometrial carcinoma who underwent workups that included a preoperative multimodality MRI examination and a postoperative histopathological staging between June 2011 and August 2015 at our hospital. This study was approved by the local ethics committee. The need for individual consent was waived by the committee because of the retrospective nature of the study.
Patients
Exclusion criteria were: (i) any MRI examination contraindication; (ii) any contraindication to surgery; (iii) an incomplete MRI examination; or (iv) no available postoperative histological findings. Finally, 83 consecutive patients were included and retrospectively analyzed.
MRI
All images were reviewed from the PACS system by two radiologists experienced in pelvic MRI (YW and XQ) and blinded to the histopathological staging; in case of discordance, the radiologist-in-chief (LD) was consulted. Multimodality MRI was performed with a 1.5 T magnet (MAGNETOM Avanto; Siemens, Erlangen, Germany) using a phased array coil. For all examinations, patients were placed in the supine position with a partially full bladder. The parameters of non-contrast enhancement images were: body coils; field of view (FOV), 320 × 320 mm; matrix, 256 × 256; and slice thickness, 3–5 mm with a gap of 20% slice thickness. In each examination, spin echo (SE) T1-weighted (T1W) imaging (TR/TE repetition time/echo time, 400/11 ms) and turbo spin echo (TSE) T2-weighted (T2W) imaging (TR/TE, 6500/90 ms) were performed in the axial and sagittal planes parallel to the longitudinal axis of the uterus. Blade sequence T2W imaging with respiratory gating and fat saturation imaging was obtained in the sagittal planes with TR/TE 3600/86 ms and 1 excitation. Diffusion-weighted imaging (DWI) was added in the sagittal planes with b = 0 and 1000 s/mm2, and 3 excitations. The values of apparent diffusion coefficient (ADC) were measured. A multiple voxel 1H-MRS (MR spectroscopy) was performed with TR 1800 ms, TE 35 ms, and an 18-channel phase-array body coil. The values of chemical compound peaks, including choline (3.2 ppm), monounsaturated fatty acid (2.0 ppm), triglycerides-CH2 (1.3 ppm), and -CH3 (0.9 ppm) were obtained with the MRI workstation. Dynamic contrast-enhanced (DCE) MRI was obtained in the sagittal plane. DCE MRI was performed using a gradient-echo sequence (fast low angle shot technique with three-dimensional volume interpolated gradient echo with a fat-suppressed angiographic sequence [FLASH-3D-VIBE-FS] technique), with: TR/TE, 4.74/2.38 ms; flip angle, 10°; FOV, 320 × 320 mm; matrix, 256 × 256; 1 excitation; slab thickness, 72 mm; slice thickness, 3 mm; and slice gap, 20% slice thickness before and after a bolus injection of contrast medium. After pre-contrast enhancement images, gadopentetate dimeglumine (Gd-DTPA) (Beijing Beilu Pharmaceutical Co. Ltd., Beijing, PR China) (0.1 mmol/kg; total, 20 mL; flow rate, 3 mL/s) was administered via the antecubital vein with a high pressure injector (MEDRAD Spectris Solaris EP MR Injection system; Medrad Inc., Indianola, PA, USA); 20 mL of saline solution was administered. The beginning of the contrast medium injection was taken as point zero. DCE MRI was performed with an automatic trigger scan after injections at 30, 60, 90, 120, and 180 s. The whole multimodality protocol takes about 28 min, including 16 min for structural imaging and 12 min for functional imaging.
Surgery
The current FIGO 2009 staging criteria for endometrial carcinoma.

Statistical analysis
According to current FIGO staging criteria, the multimodality MRI sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) for assessing stage of endometrial carcinoma were calculated, using pathology as a gold standard. SPSS 19.0 (IBM, Armonk, NY, USA) was used for statistical analysis. Two-sided P values <0.05 were considered statistically significant.
Results
Patient characteristics
Characteristics of the patients with endometrial carcinoma (n = 83).
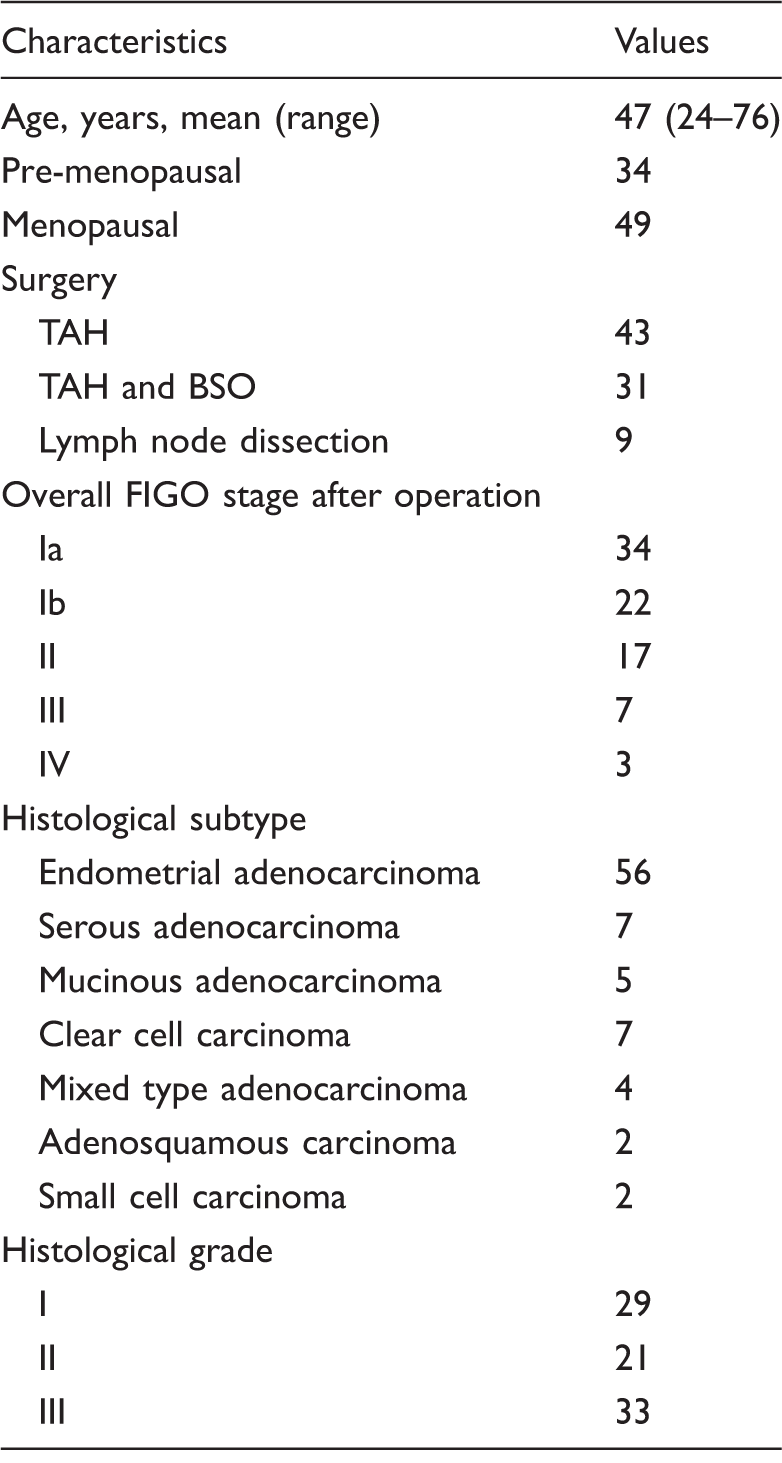
BSO, bilateral salpingo-oophorectomy; TAH, total abdominal hysterectomy.
Histopathological staging results
Multimodality MRI accuracy for endometrial carcinoma based on the current FIGO 2009 staging system.
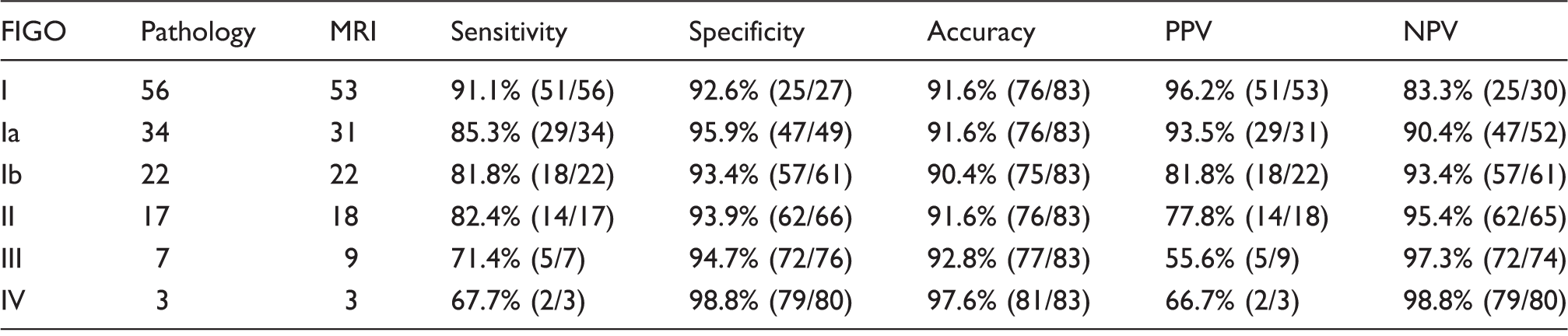
NPV, negative predictive value; PPV, positive predictive value.
Multimodality MRI staging findings for stage I
Of the 83 patients with endometrial carcinoma, 67.5% were confirmed to be with pathologically confirmed stage I (56/83). The multimodality MRI sensitivity, specificity, and accuracy for FIGO2009 stage I were 91.1% (51/56), 92.6% (25/27), and 91.6% (76/83), respectively. Of the 34 patients who were pathologically-confirmed as stage Ia, five were over-staged by MRI, including two as stage Ib, two as stage II, and one as stage III. Of the 22 patients who were pathologically confirmed as stage Ib, two were under-staged as stage Ia and two were over-staged by MRI (i.e. one as stage II and one case as stage IIIa). Multimodality MRI sensitivity for the FIGO2009 stage Ia and Ib were 85.3% (29/34) and 81.8% (18/22), respectively.
Multimodality MRI staging findings for stage II
Among the 17 stage II patients, multimodality MRI showed the correct staging in 14 patients, while two patients were over-staged and one was under-staged. One patient was over-staged as stage II was because of her age and atrophy of the uterus led to blurred margin between cervical mucosal glands and cervical stroma.
Multimodality MRI staging findings for stage III and IV
Five out of seven stage III patients were accurately staged by MRI. Two patients were under-evaluated. One patient was mis-staged as Ib and pelvic lymph node metastases were found at surgery. The sensitivity, specificity, and accuracy of MRI for stage III cancer were 71.4% (5/7), 94.7% (72/76), and 92.8% (77/83). The sensitivity, specificity, and accuracy of MRI for stage IV cancer were 67.7%, 98.8%, and 97.6%.
Overall multimodality MRI staging findings
Among the 83 patients with endometrial carcinoma, 68 patients were accurately staged by multimodality MRI, nine were under-evaluated, and six patients were over-evaluated. According to the latest FIGO2009 standard, the total sensitivity of MRI for endometrial carcinoma staging was 81.9% (68/83).
Representative cases and error analysis
Two concordant cases are presented (Figs. 1 and 2).
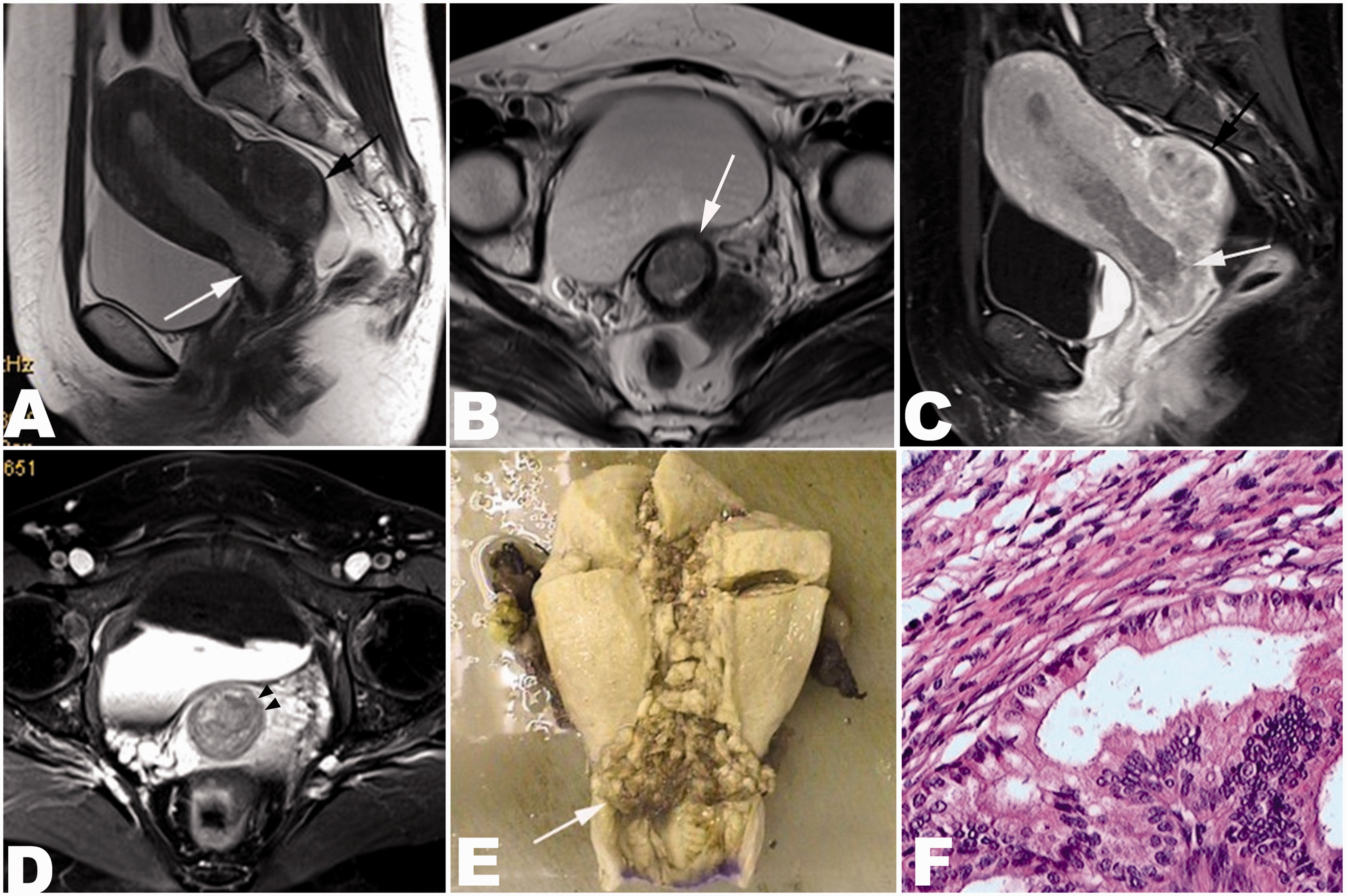
Stage I endometrial carcinoma of the diffuse type, with deep muscular layer being invaded. Multimodality MRI result was concordance with histopathology. (a) Transverse axial T1W image showing that the isointensity of the diffused tumor was detected in the entire uterine cavity, which was hardly distinguishable from uterine wall (white arrow). (b) Transverse axial T2W image showing that the tumor with isointense signal invaded the left anterior wall of the uterine. The detailed depth of invasion was unclear (white arrow). (c) Sagittal image of multimodality MRI with blade sequences and fat suppression. (d) Transverse DWI image (b = 1000). (e) ADC transverse axial image. (f) T1W dynamic enhanced sagittal image with FLASH-3D-VIBE-FS sequence indicated that the diffuse tumor invaded the whole uterine cavity. The left anterior wall of uterus was topically invaded. The junction area was interrupted, with the deep muscular layer being infiltrated (black and white arrows). (g) Pathological specimen showing the diffused thickening of endometrium, which occupied the entire uterine cavity. The cauliflower-like tumor was observed at the left anterior wall of uterine, dark red and soft, and the deep muscular layer was invaded (white arrow). (h) H&E staining (×200). The invasive growth of the tumor was in the shape of sieve, papillary, tubular, or solid nests, and the deep muscular layer was invaded. Stage II endometrial carcinoma of the diffuse type, with the cervix being infiltrated. Multimodality MRI result was concordance with histopathology. (a) T2W sagittal image and (b) T2W transverse image showing the downward growth of the tumor protruding to the cervix (white arrow). The hypointense signal was detected and interrupted at the cervical stroma area. A fibroid was found on the posterior uterine wall (A: black arrow). (c) T1W sagittal image and (d) T1W transverse image with fat suppression showing that the uterine and cervical tumor were present as uniform intensity with interruption at the cervical stroma area (white arrow and black arrow heads), but the outside of the uterus was not invaded. (e) Pathological specimen showing the cauliflower-like tumor that filled up the entire uterine cavity. The downward growth of the tumor protruding to cervix was observed (white arrow). (f) H&E staining (×200) showing that the tumor cells were arranged in papillary, tubular, and sieve-like structures with squamous metaplasia, infiltrating into the superficial layer of the uterine muscle and cervical mucosa.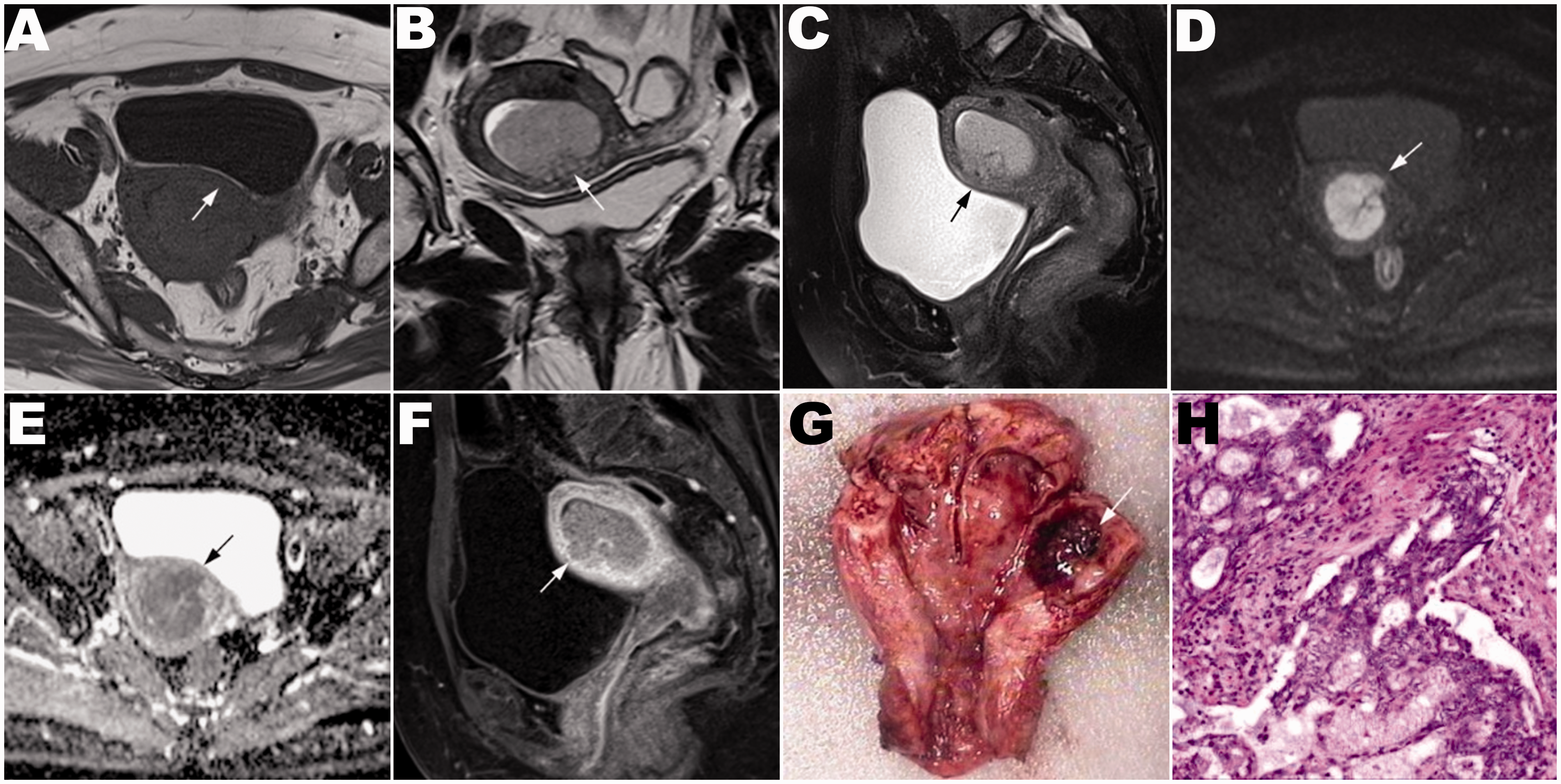
Misdiagnosis analysis of multimodality MRI staging findings compared with histopathological results.
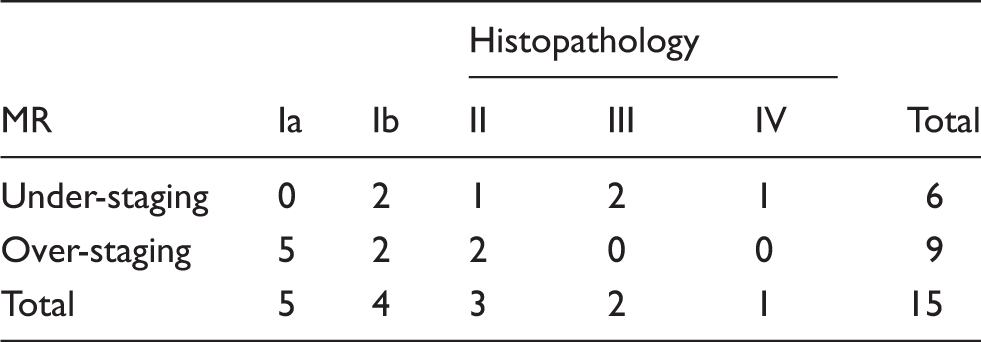
Five patients at stage Ia were mis-staged to stages Ib, IIa, and III, including two postmenopausal patients that were over-staged to stage Ib due to the unclear junction band of the endometrium; two patients were over-staged to stage IIa due to the unclear boundary between endometrium and cervical stroma; and one patient was over-staged to stage III due to the tumor located at the anterior wall of uterus and close to uterine isthmus, and complicated with pelvic inflammation and adhesion.
Four patients at stage Ib were mis-staged, including two patients that were under-staged to stage Ia because of seniority, uterine atrophy, unclear boundary between the deep and superficial muscular layers, and adenomyosis; one patient was over-staged to stage II because of tumor downward growth infiltrating the cervical glands and complicated with cervical Nabothian cyst, resulting in unclear boundary between cervical mucosal glands and cervical stroma; and one patient was over-staged to stage III because of tumor invasion into the deep muscle layer and complicated with hysteromyoma and pelvic effusion leading to the mistaken for the tumor invasion into the serous layer.
Three patients at stage II were mis-staged, including one patient that was under-staged to Ib due to the unclear boundary between the cervical mucous gland and the cervical stroma; one patient was over-staged to stage III due to the protruding of cervical tumor to vagina; and another patient was over-staged to stage IV due to peritonitis-related lymphadenopathy.
Two patients at stage III were under-staged to Ib and II, including one patient that was under-staged to Ib due to the pelvic inflammatory and pelvic hematocele; and the other patient was under-staged because pelvic lymph nodes metastasis were found postoperatively (IIIc), however, the preoperative estimation by MRI only showed the cervical stromal invasion.
One patient at stage IV was under-staged to stage III, because the unclear boundary between uterus and rectum caused by the tumor serosa invasion was mistaken as pelvic inflammation and adhesion, which was classified into stage III; however, it was found by postoperative examination that the rectal wall was affected by the tumor, which should be classified into stage IV.
Discussion
The prognosis of patients with endometrial cancer is closely related to the stage of the tumor (10,11). MRI is currently considered the most accurate imaging technique for staging endometrial carcinoma (10–14). MRI staging accuracy is high, at 78–92%, and is consistent with pathological staging (7). In the present study, the overall sensitivity and accuracy of MRI for the staging of endometrial carcinoma according to FIGO2009 were 91.9% (68/74) and 81.9% (68/83), respectively. These results are supported by a study by Haldorsen et al. (13).
In the present study, among the 34 stage Ia cases, five were over-staged by multimodality MRI. Some reasons could explain this over-staging such as age and the presence of inflammation or benign lesions. In addition, the interface of the endometrium and myometrium is usually unclear and irregular. Finally, it is not easy to pathologically diagnose stages Ia, especially tumors limited to the endometrium (9,15).
The rate of involvement of lymph nodes ranges from 3% for stage Ia to 46% for stage Ib (12,15,16). The depth of invasion to the muscle layer determines whether lymph node resection is needed. When invasion to the muscle is less than half the thickness, the chance of invasion of lymph nodes is low; but when invasion to the muscle is greater than half the thickness, the tumor will possibly migrate through lymph nodes in the deep muscle layer. In contrast, when determining the depth of invasion to the muscle layer, the accuracy is affected by the thinness and partial absence of the junction zone, unclear borderline to the muscle layer, endometrial polyps, adenomyosis, multiple leiomyomas compressing a thin myometrium, poor signal contrast between tumor border and muscle layer, and tumor expansion to the uterine horn. Therefore, the sensitivity and accuracy are low for determining stage I (Ia, Ib, and Ic) by MRI. Moreover, no significant prognostic difference has been observed between tumor invasion of the endometrium and the shallow muscle layer in patients with endometrial carcinoma (15,17,18).
In the FIGO2009 staging system, tumors limited to the endometrium and the depth of invasion to the muscle layer less than half the thickness are stage Ia, and the depth of invasion to the muscle layer greater than half the thickness is stage Ib, which simplifies the classification for the depth of invasion to the muscle layer, and makes it easier to evaluate the degree of invasion before surgery. It is important to evaluate the depth of invasion to the muscle layer before surgery to avoid errors in judgment and increase the diagnostic accuracy (86–91%) (15,19,20). In the present study, applying the current FIGO staging standard for endometrial carcinoma based on multimodality MRI, the sensitivity, specificity, and accuracy were 91.1%, 92.6%, and 91.6%, respectively, which is in agreement with previous studies (12,20). Nevertheless, over-staging (five cases for stage Ia, two cases for stage Ib) and under-staging (two cases for stage Ib) still occurred. Indeed, the contrast between tumor and muscle layer is often low, and when T2W imaging is low in contrast, applying a FLASH 3D dynamic enhanced scan increases the contrast. When the tumor invades the uterine horn, it is not easy to determine the depth of invasion because the muscle layer is thin. In addition, because of the combination of tumor and endometrioma, and compression of multiple uterine fibroids, errors in judgment may happen.
In the FIGO2009 staging system, stage II is only limited to tumor invasion to the cervical stroma without spreading outside of the uterine body. This makes the staging of stage II easier and more accurate. As a result, the accuracy for determining stage II by MRI is greatly improved (12,15,20,21). To judge the invasion to the cervical stroma, MRI is the first choice apart from pathology. MRI cannot only differentiate invasion to cervical glands with precision, but also determines the depth of invasion to intermediates and differentiates polyps of the cervix and Nabothian cysts. If cervical stroma involvement is suggested by MRI preoperatively, a biopsy is necessary to determine whether or not broad curettage of the uterus is needed.
In the present study, the accuracy of MRI was high (92.8–97.6%) for stage III and IV patients according to the current FIGO2009 staging standards, but because of the small number of stages III and IV patients, and because there is no further sub-staging, the efficiency of the MRI was low, and additional studies are needed for further investigation and evaluation.
Though there was 18.1% of mis-staging by preoperative multimodality MRI, the consistency between preoperative MRI staging and postoperative pathological examination was observed in 81.9% of tumors. For instance, the diffused tumor from a 63-year old postmenopausal patient was presented as an iso-intense signal on T1W/T2W imaging sequence, the muscle layer of anterior uterine wall was invaded with the invasion depth and boundary poorly defined (Fig. 1a–h). However, the present study showed that multimodality MRI scanning is able to display tumor diffusely invading the muscle layer of anterior uterine wall with the junction band interrupted. MRI could also clearly display if the depth of invasion was more than half of the depth of the muscle layer, either on DWI and ADC sequences or on dynamic enhanced FLASH-3D-VIBE-FS sequence. The postoperative pathological examination indicated the diffused thickening of endometrium and the papillary or cribriform-like invasive growth of cauliflower-like tumor, invasion into the deep muscular layer. The stage Ib was accurately determined by both preoperative MRI and postoperative pathological examination. Similarly, for tumor at stage II, the significant difference could be discriminated between the cervical mucosal glands with obviously enhanced intensity and the cervical stroma with moderate enhanced intensity on dynamic enhanced sequence by multimodality MRI; therefore, the downward growth of uterine tumor and the tumor invasion into cervix leading to the interruption of cervical stroma could be clearly visualized by MRI. And the tumor invasion into the superficial layer of uterine muscle and cervical stroma was also clearly indicated by histology study (Fig. 2a–f). Therefore, the high consistency with respects to the tumor staging was demonstrated between preoperative MRI and postoperative pathological examination.
The present study is not without limitations. Indeed, the sample size was small and from a single center. Most patients treated at our center during the study period (186/280) did not undergo MRI, and 11 of those who did had incomplete MRI data. In addition, its retrospective nature prevented examining other factors that were not part of the original investigations. A previous study revealed differences between imaging protocols (22) and to examine different combinations of protocols could be interesting. MRI could also be combined with other imaging modalities such as positron emission tomography (23). Additional studies are necessary to examine the role of MRI in the preoperative staging of endometrial cancer.
In conclusion, multimodality MRI is an important imaging tool in the pre-operative clinical staging of endometrial carcinoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shenzhen science and technology R & D funds (grant no. JCYJ20140415093749223) and Shenzhen health and family planning system of scientific research project (key project) (grant no. 201401102).