
Abstract
Background
Arterial dissections during transcatheter arterial chemoembolization (TACE) procedures are not rare and can limit the successful treatment of unresectable hepatocellular carcinoma (HCC).
Purpose
To evaluate the incidence of arterial dissections during TACE procedures, the rate of spontaneous lumen recovery, and the predictive factors of dissecting stenosis during follow-up.
Material and Methods
Based on 69,651 TACE procedures from 1997 to 2016, patients who had procedure-related arterial dissections were identified by procedure report search. More than two months after the date of dissection, dissecting stenosis was evaluated using a three-grade scale: subclinical narrowing with diameter loss under 30%, overt stenosis with diameter loss over 30%, and occlusion. Pearson Chi-square and two-sample t-test were used to assess potential prognostic markers for dissecting stenosis.
Results
Eighty-four arterial dissections directly related to TACE were identified in 83 patients, resulting in an incidence of 0.12% (84/69651). After more than two months, normal or subclinical narrowing, overt stenosis, occlusion, and doubling were seen in 39 (46.4%), 26 (31.0%), 13 (15.5%), and one (1.2%) patients, respectively. No follow-up images were obtained for five (6.0%) patients. On univariate analysis, the dissection ratio (the ratio of the length to the diameter of the dissection) alone was related to dissecting stenosis (P = 0.035).
Conclusion
The incidence of iatrogenic dissection during TACE was approximately 0.12%. Less than 50% of the iatrogenic dissections showed normal or subclinical narrowing during follow-up of at least two months. The dissection ratio alone was the predictive factor for dissecting stenosis during follow-up.
Keywords
Introduction
Transcatheter arterial chemoembolization (TACE) is the standard treatment for unresectable hepatocellular carcinoma (HCC) without distant metastasis (1,2). Since patients with HCC often require repeated TACE procedures for a residual viable tumor or local recurrence, hepatic artery injury associated with TACE may interfere with catheterization, thereby compromising treatment success and clinical outcome (3). In addition, knowledge of the changes in the hepatic artery can help in devising the optimal treatment plan and in understanding patient prognosis.
Although arterial dissections are well-known complications following TACE, the incidence, technical success rate of TACE with feeding artery dissection, and detailed follow-up data, together with an analysis of the prognostic factors of their future patency, such as dissecting stenosis, occlusion, or patent lumen recovery, have not been thoroughly reported (4–6). The purpose of this study was to evaluate the incidence of arterial dissections occurring during TACE procedures, rate of spontaneous lumen recovery, and predictive factors for stenosis or occlusion of the dissection during follow-up.
Material and Methods
Patient characteristics
From January 1997 to February 2016, a total of 69,651 TACE procedures were performed at our hospital. Our institutional review board approved the current study and waived the requirement for patient consent for this retrospective review.
To evaluate the occurrence of arterial dissections during the TACE procedures, the words, “dissection,” “dissections,” “dissect,” and “dissected” were used for an electronic search of all reports on TACE procedure during the study period. Subsequently, dissections of the celiac trunk, common hepatic artery and its branches, left gastric artery, superior mesenteric artery, and inferior phrenic artery and their branches were singled out with reference to TACE images. Dissections of the femoral arteries were not included in this study.
TACE procedures
HCC was diagnosed on the basis of findings on computed tomography (CT) or magnetic resonance image (MRI), along with laboratory findings or pathologic confirmation. Subsequently, the unresectable HCCs were referred to us for TACE treatment.
A 5-french (F) RH, Yashiro, or Cobra catheter (Cook, Bloomington, IN, USA) and a 0.035-inch guidewire (Terumo, Tokyo, Japan) were used for cannulation of the celiac trunk or the common hepatic artery with/without the superior mesenteric artery.
Selective catheterization of the feeding artery was performed using a 2.0- to 2.8-F micro-catheter (Terumo, Boston Scientific, or Cook) and a 0.014- to 0.018-in. micro-guidewire (Terumo, Boston Scientific, or Cook).
Cisplatin (Cisplan; Dong-A Pharmaceutical, Seosan, Republic of Korea) or Adriamycin (Ildong Pharmaceutical, Seoul, Republic of Korea) was used as the chemotherapeutic agent with an emulsion of iodized oil (Lipiodol Ultra-Fluide; Laboratoire Guerbet, Aulnay-sous-Bois, France), and absorbable gelatin sponge (Gelfoam; Upjohn, Kalamazoo, MI, USA) or polyvinyl alcohol particle (Contour; Boston Scientific) were used as embolic materials.
An additional TACE procedure was considered based on post-treatment CT scan obtained one month after a previous TACE and was performed when the condition of the patients was stable. CT scans were obtained using a helical CT (GE Light Speed VCTXT, GE Healthcare, Milwaukee, WI, USA) with a four-phase (precontrast, arterial, portal, and delayed phases) technique.
Image analysis
All images were reviewed and a consensus was reached by two interventional radiologists (with over 14 and 3 years of experience in interventional suites, respectively).
The location of the dissection was determined as the most proximal artery where the dissection began. Moreover, we calculated the dissection ratio, which was defined as the ratio of the length to the diameter based on digital subtraction angiographic (DSA) or fluoroscopic images obtained in the anteroposterior (AP) view. The length was measured as the total length of the dissection and the diameter was measured as the mean diameter of the proximal and distal normal arteries adjacent to the dissection.
To evaluate the treatment results, technical success was evaluated twice each for the TACE session during which the dissection developed and for the next TACE session. Technical success was defined as unimpeded treatment via the route of the original or collateral feeding artery.
Follow-up
DSA images, fluoroscopic images, or CT scans obtained at least two months after development of the dissection were subsequently reviewed. Because of the ease of comparison, DSA images or fluoroscopic images were reviewed first when both angiography and CT images were available.
To observe the change in dissected arteries and evaluate the prognostic factors for progression to overt stenosis or occlusion, the change in dissections during follow-up was evaluated using a three-grade scale, i.e. (i) normal or subclinical narrowing with a diameter loss less than 30%; (ii) overt stenosis with a diameter loss greater than 30%; and (iii) occlusion.
Statistical analysis
Mean dissection ratio and other values were reported as mean ± standard deviation (SD) unless otherwise specified. Prognostic factors for dissecting stenosis were obtained by evaluating the location and dissection ratio of the dissected arteries as well as the patient’s age, sex, and the presence of medication for diabetes mellitus and hypertension. Pearson Chi-square and the two-sample t-test were used for statistical analyses (SPSS version 15.0. SPSS Inc., Chicago, IL, USA).
Results
Of 69,651 TACE procedures, 84 arterial dissections directly related to TACE procedures were identified in 83 patients, with an incidence of 0.12% (84/69651). These patients included 59 men and 25 women (mean age, 58.05 ± 8.04 years; age range, 39–75 years).
The sites of the 84 dissections were as follows: the celiac artery (n = 7), the common hepatic artery (n = 11), the proper hepatic artery (n = 8), the right hepatic artery (n = 14), the replaced right hepatic artery from the superior mesenteric artery (n = 12), the left hepatic artery (n = 8), the replaced left hepatic artery from the left gastric artery (n = 10), the intra-hepatic segmental artery (n = 7), and the right inferior phrenic artery having a blood supply to HCC (n = 7).
The dissection ratio was available in 53 dissections in 52 patients, while the ratio could not be obtained in 31 patients because images of the dissections were not available. The mean dissection ratio was 8.30 ± 5.73. The dissection ratio is shown in Fig. 1, and the dissection ratio between 2 and 4 comprised the largest group of patients (n = 15, 28.3%).
Distribution of the dissection ratio, defined as the ratio of the length of the dissected artery to its diameter.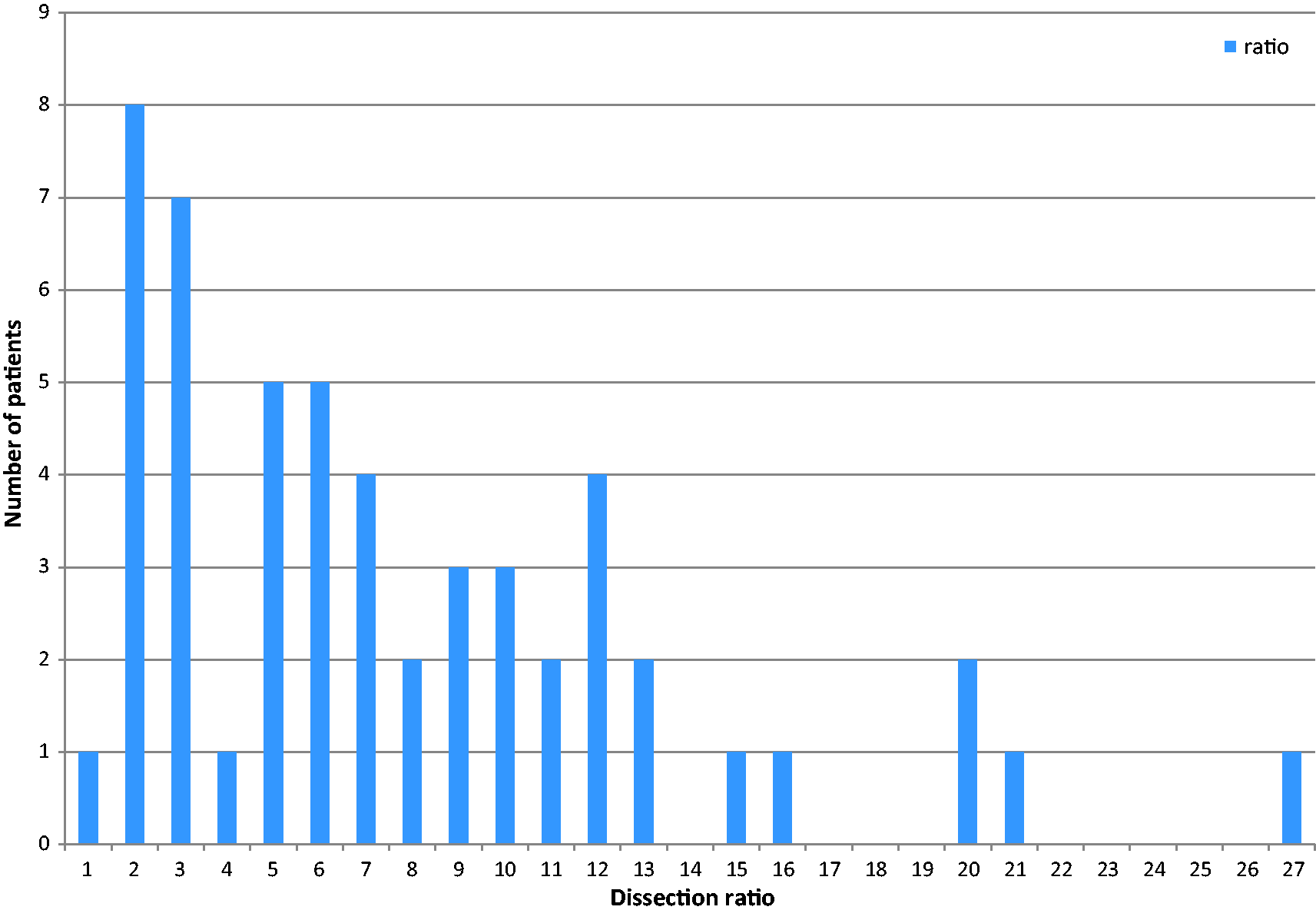
In the TACE session during which the dissection developed, excluding ten patients in whom chemoembolization via the dissected artery was not performed, the technical success rate was 48.6% (36/74); 27 and nine patients were treated via the original artery and the collateral feeding artery, respectively. Incomplete treatment due to failed selection of the original or collateral feeding artery occurred in 15 patients (20.3%). The remaining 23 patients (31.1%) could not undergo TACE at that time because of the dissection.
In the next TACE session, excluding 31 patients who did not undergo chemoembolization via the dissected artery, the technical success rate was 84.9% (45/53), and 36 and nine patients were treated via the original artery and the collateral feeding artery, respectively. Incomplete treatment because of failed selection of the original or collateral feeding artery occurred in five patients (9.4%). The remaining three patients (5.7%) could not undergo TACE because of the obstructive change in the dissection. No patient developed hepatic ischemia during follow-up.
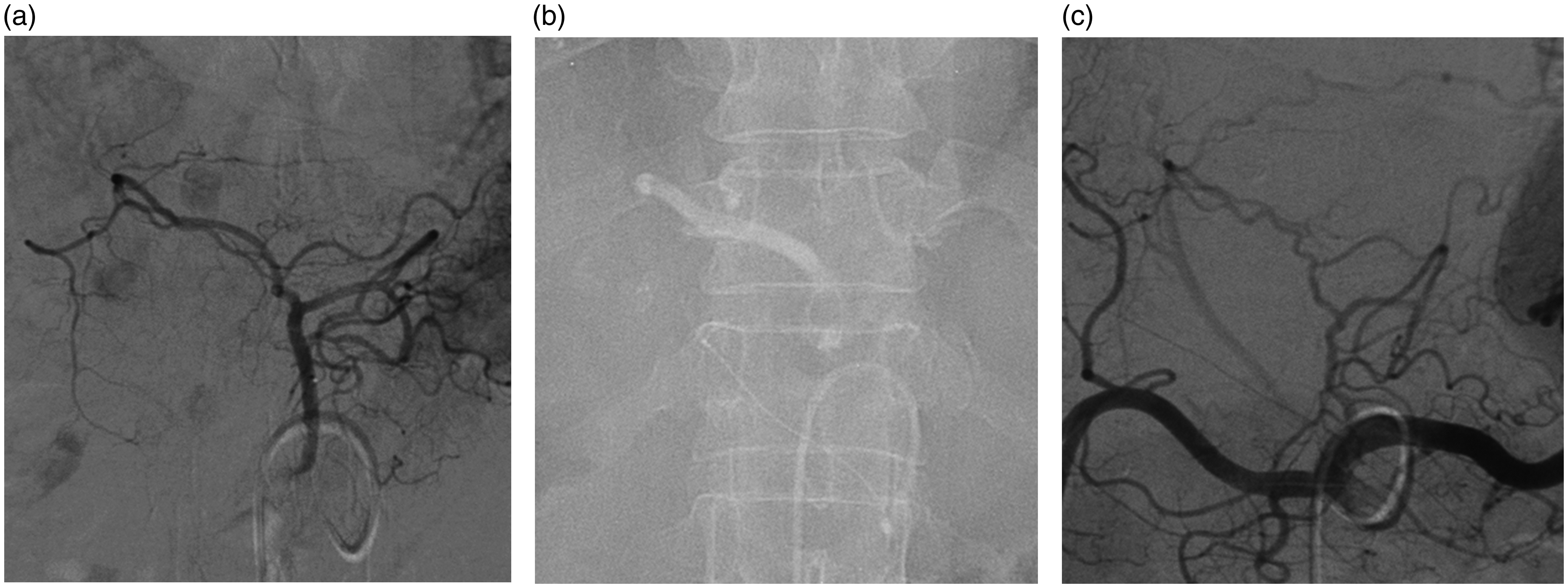
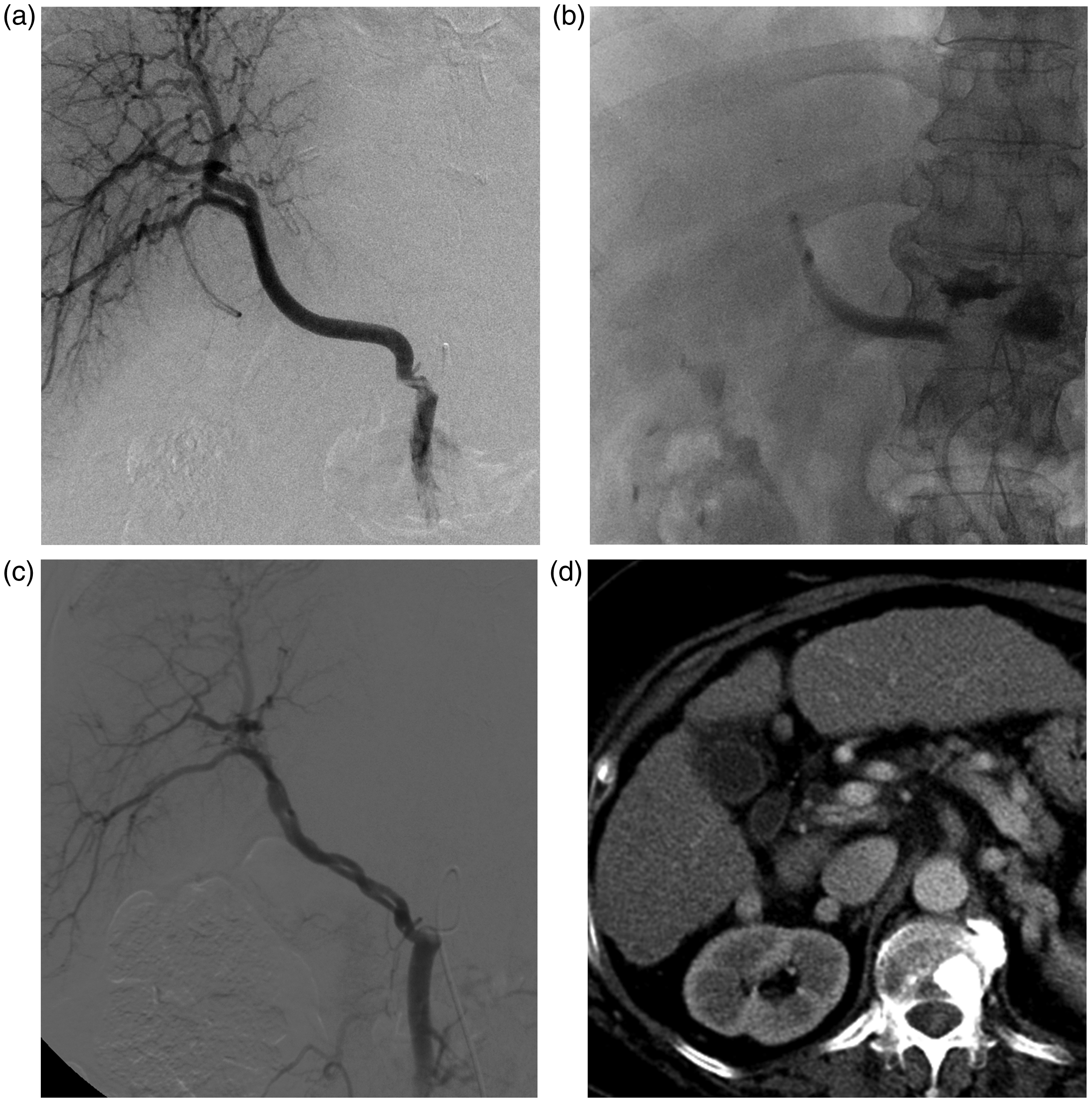
There were 84 dissection changes after more than two months. Of these, 39 (46.4%) had complete lumen recovery or subclinical stenosis (Fig. 2), 26 (31.0%) had overt stenosis (Fig. 3), 13 (15.5%) had occlusions, one (1.2%) had doubling (Fig. 4), and a follow-up image was not available for five (6.0%). Doubling was noted in the dissection at the replaced right hepatic artery from the superior mesenteric artery and that showed separated double lumens on the follow-up image.
Complete lumen recovery of the dissected replaced right hepatic artery. (a) Superior mesenteric arteriogram shows the straight course of the replaced right hepatic artery from the superior mesenteric artery. (b) Arteriogram of the replaced right hepatic artery shows dissection, slight dilation of its proximal and middle portions, and flow limitation to its distal portion. (c) Fluoroscopy image after dissection shows the remaining contrast medium in the false lumen. (d) Twelve-month follow-up arteriogram shows normal caliber and patent lumen of the replaced right hepatic artery. Overt stenosis after the dissection of a replaced left hepatic artery. (a) Left gastric arteriogram shows the replaced left hepatic artery from the left gastric artery. (b) Fluoroscopy image after dissection shows the remaining contrast medium in the false lumen. (c) Six-month follow-up arteriogram shows the stenotic and tortuous change of the replaced left hepatic artery. Doubling of the lumen after the dissection of the replaced right hepatic artery. (a) Arteriogram shows the straight course of the replaced right hepatic artery from the superior mesenteric artery. (b) Fluoroscopy image after dissection shows the remaining contrast medium in the false lumen. (c) Six-month follow-up arteriogram shows the slightly tortuous course of the two separate lumens of the replaced right hepatic artery. (d) Eight-month follow-up CT image shows the two separate lumens of the replaced right hepatic artery crossing each other in the portocaval space.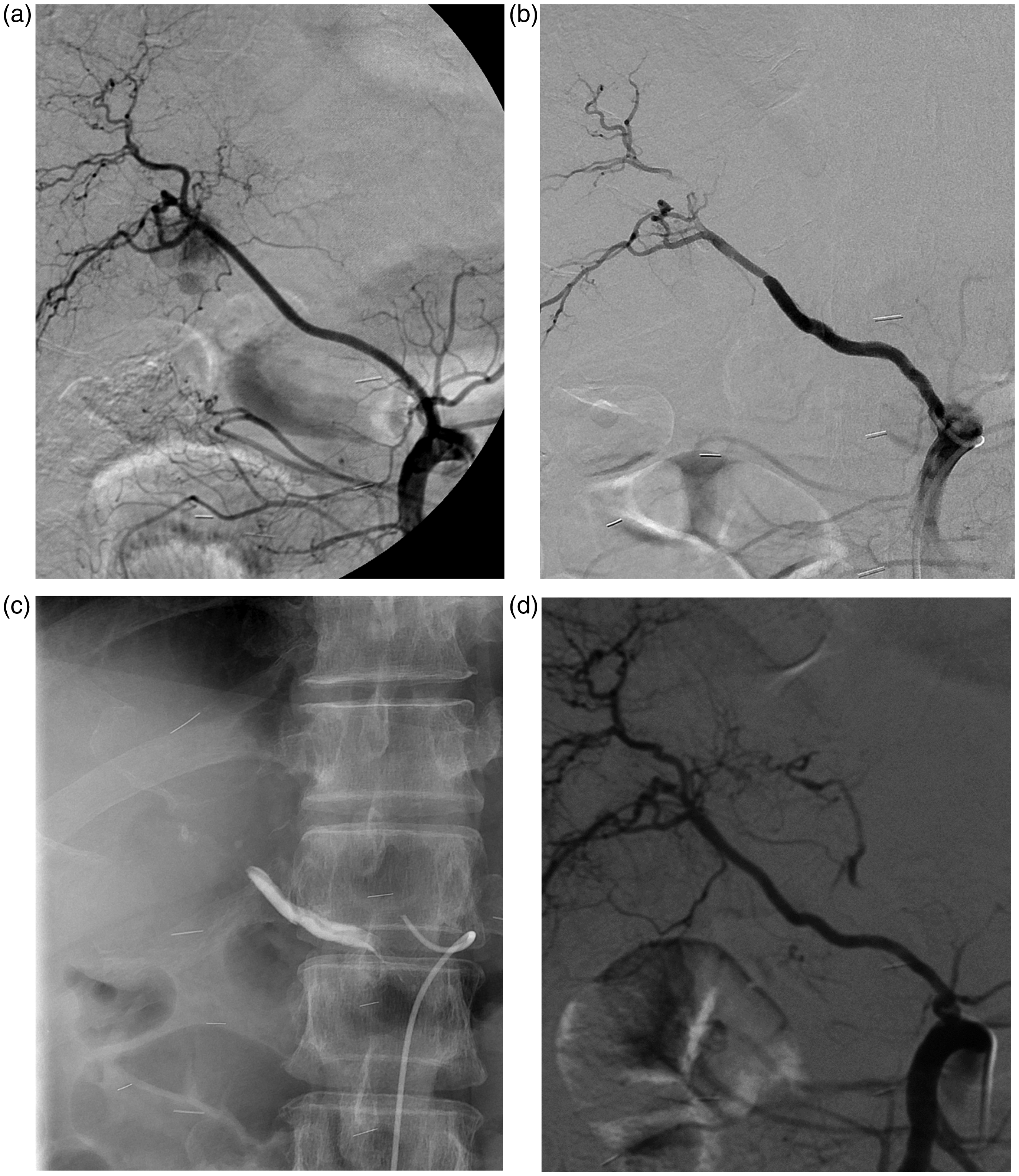
Factors influencing normalization and other changes of the dissections.
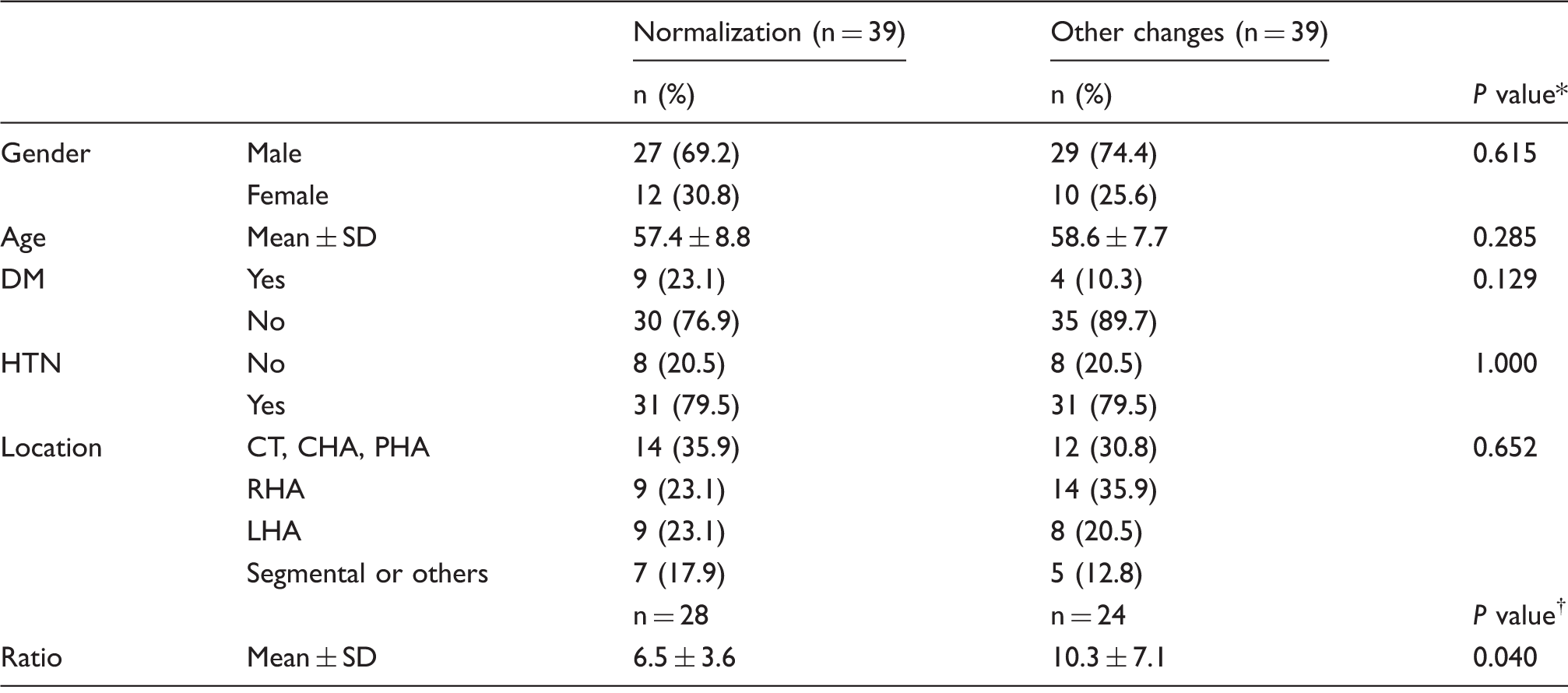
Pearson Chi-square test.
Two-sample T-test.
CHA, common hepatic artery; CT, celiac trunk; DM, diabetes mellitus; HTN, hypertension; LHA, left hepatic artery; PHA, proper hepatic artery; RHA, right hepatic artery; SD, standard deviation.
Discussion
In this study, the incidence of arterial dissection directly related to TACE procedures was 0.12%. Although this incidence might be underestimated because of the inherent collection errors of an automatic search for the keywords of dissection, this study is the most recent and is based on a large number of patients. Yoon et al. reported the incidence of arterial dissection as 1.27% (61/4791) in 1995 (4) and Sakamoto et al. reported the incidence as 1.52% (35/2300) in 1998 (7). These two results are approximately ten times greater than our result. This may have been caused by the large time difference in data collection between the previous studies and our study. During such a large time span, many catheters, microcatheters, guidewires, and micro-guidewires of smaller size and higher component quality have been developed and superselective catheterization with minimal arterial injury has become the standard (1).
Variable hepatic arteries or other collateral arteries supplying a tumor can be dissected iatrogenically during TACE procedures. This could be done by direct trauma caused by a guidewire, the tip of the catheter, or the jet of contrast injection (4). In this study, the replaced right hepatic artery from the superior mesenteric artery was the most common site where dissection occurred. Considering the incidence of 12–22% of the replaced right hepatic artery having an anatomic variation (8–17), the true incidence of dissection of the replaced right hepatic artery seems quite high. This may be caused by the first downward course of the superior mesenteric artery and the next acute upward direction of the replaced right hepatic artery. The arteries with a more acute curve could have more injury caused by the catheters or wires used during TACE.
Technical success rates in the TACE session during which the dissection occurred decreased to as low as 48.6% (36/74). Fortunately, 36.5% (27/74) of the patients were treated via the original artery before the dissection developed. However, technical success rates in the subsequent TACE session increased to as high as 84.9% (45/53). Most patients (67.9%; 36/53) were treated via the original artery and others (17.0%; 9/53) were treated via the collateral feeding artery. A small number of patients (5.7%; 3/53) could not undergo TACE because of the obstructive change in the dissection.
As recanalization of the tumor vasculature is a prerequisite to subsequent TACE procedures (18), understanding the progression of the dissection is critical. We postulate that the dissection flap becomes attached to the wall over time, resulting in more lumen recovery, although whether true or false lumen recanalization occurs remains unclear.
In our study, the dissection ratio was the only significant prognostic factor for dissecting stenosis. If the dissection flap is relatively long compared to its diameter, the true or false lumen could be filled with more thrombus, resulting in stenosis or occlusion. Although partial recanalization occurs through the lumen, when the dissection flap is relatively short compared to its diameter, more overall lumen recanalization can occur.
“Doubling” was observed at the replaced right hepatic artery from the superior mesenteric artery in the follow-up images in one patient in this study. When the stenosis arises from the thrombosed occlusion of one of the true or false lumens, “doubling” may arise from the recanalization of both the true and false lumens with complex redistribution of the dissection flap to each lumen.
There were several limitations in our study. First, it was a retrospective study and therefore it is possible to have underestimated the incidence of arterial dissections. Moreover, part of the reported dissections was excluded in the analysis because of unavailable imaging data. Second, we could not analyze which catheter system or which action, such as catheter advance, wire manipulation, or contrast injection, was prone to dissection. Third, objective diameter and length of the dissection could not be measured in old images, which comprised over 50% of our study population.
In conclusion, the incidence of iatrogenic dissection during TACE was approximately 0.12%. Less than half of the iatrogenic dissections showed normal or subclinical dissection after at least two months. The dissection ratio was the only predictive factor for progression of the dissections during follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: this research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and future Planning (2014R1A2A2A01005857).