
Abstract
Background
Inadequate neointimal coverage of stent struts is associated with late stent thrombosis.
Purpose
To demonstrate the extent of neointimal coverage and strut malapposition in titanium-nitride-oxide-coated bioactive stents (BAS) versus everolimus-eluting stents (EES) by optical coherence tomography (OCT) performed at 18-month follow-up.
Material and Methods
In the BASE-ACS trial, 827 patients presenting with acute coronary syndrome were randomized to receive either BAS or EES. Forty patients (20 BAS, 20 EES) underwent OCT at 18-month follow-up for evaluation of stent strut coverage, malapposition, and neointimal hyperplasia (NIH). Primary endpoint was binary stent strut coverage (ratio of covered struts to all analyzed struts multiplied by 100). Co-primary endpoint was the percentage of malapposed struts.
Results
We analyzed 3465 struts in 330 cross-sections of BAS and 3327 struts in 316 cross-sections of EES. Binary stent strut coverage, based on strut-level analysis, was higher with BAS versus EES (99.5% versus 94.2%, respectively; P < 0.001), the strut-level percentage of malapposed struts was lower with BAS (0.6% versus 2.5%, respectively; P < 0.001). Yet, the mean NIH thickness was greater with BAS (237 ± 125 versus 108 ± 62 µm, respectively; P < 0.001).
Conclusion
In the current post-hoc analysis with OCT performed at 18 months, binary strut coverage, based on strut-level analysis, was higher with BAS versus EES; strut-level malapposed struts were fewer with BAS; yet, BAS induced thicker NIH.
Keywords
Introduction
In autopsy studies, inadequate neointimal coverage of stent struts was the most powerful histopathological predictor of late stent thrombosis (ST) in patients who received first-generation drug-eluting stents (DES); the ratio of uncovered to total struts per cross-section was the morphometric parameter that best correlated with inadequate neointimal coverage (1,2). Neointimal healing response can be evaluated in vivo by invasive imaging techniques; in an animal model, optical coherence tomography (OCT) had a higher diagnostic accuracy compared with intravascular ultrasound for detection of small degrees of neointimal tissue over stent struts, taking histology as the “gold standard” (3). In vivo identification of stent strut coverage has been suggested as a surrogate endpoint for the assessment of stent safety profile. Both uncovered and malapposed struts detected by OCT were associated with late and very late ST; nevertheless, the relative importance of strut uncoverage and malapposition to the risk of ST varies with the length of follow-up (4,5).
In the BASE-ACS randomized controlled trial, titanium-nitride-oxide-coated bioactive stents (BAS) were non-inferior to everolimus-eluting stents (EES) for the primary endpoint of major adverse cardiac events in patients presenting with acute coronary syndrome (ACS), both at 1- and 2-year follow-up (6,7). In a post-hoc analysis of the BASE-ACS trial, OCT evaluation at 9-month follow-up demonstrated higher binary stent strut coverage, and a lower percentage of malapposed struts associated with BAS versus EES (8). We sought to demonstrate the extent of neointimal strut coverage, and strut malapposition associated with BAS versus EES by OCT performed at 18-month follow-up of the BASE-ACS trial.
Material and Methods
Patient selection and study design
The study was initiated by the investigators and conducted according to the ethical guidelines of the 1964 Declaration of Helsinki, as revised in 2013. Informed written consent was obtained from every patient after full explanation of the study protocol. Patients were asked about their willingness to come for evaluation by OCT at 18-month follow-up. Consecutive patients who accepted were scheduled for follow-up. The study protocol was approved by the ethics committees of the participating centers. The BASE-ACS trial is registered under ClinicalTrials.gov, with number NCT00819923, and the BASE-OCT substudy with number NCT01080859.
The original trial design was previously described (6). Briefly, the BASE-ACS is a prospective multi-center randomized controlled trial that evaluated non-inferiority for clinical outcome of BAS (Titan2®, Hexacath, Paris, France) versus EES (Xience V®, Abbott Vascular, Santa Clara, CA, USA) in patients presenting with ACS. The study enrolled 827 patients with ACS and at least one significant de novo lesion (≥50% diameter stenosis) in a native coronary artery or coronary bypass graft. Main exclusion criteria were unprotected left main disease or aorto-ostial lesions, intolerance to the study medications, planned surgery within 12 months of the index procedure, and life expectancy less than 12 months. Enrolled patients were randomly assigned in a 1:1 fashion to receive either BAS or EES. We enrolled consecutive patients who accepted to come for evaluation by OCT at 18-month follow-up and had a lesion(s) successfully treated during the index procedure. The main exclusion criterion was a second de novo stenosis ≥50% in the stented vessel observed during follow-up angiography. Forty-six patients accepted to come for 18-month follow-up, six withdrew consent to participate in the 18-month OCT substudy; ultimately, 40 patients (20 in each group) were enrolled for the current analysis. The patients enrolled in the current 18-month OCT follow-up constitute a discrete cohort separate from that enrolled for 9-month OCT follow-up (8).
Optical coherence tomography image acquisition
OCT images were obtained 18 months after the index procedure, immediately after follow-up angiography, with the C7Xr frequency-domain system (LightLab Imaging Inc., Westford, MA, USA) employing the non-occlusive technique via radial or femoral approach. A 0.014-inch guide-wire was introduced into the vessel using a 6F guiding catheter. An imaging catheter (Dragonfly, LightLab Imaging Inc.) was positioned distal to the stent and automated motorized pullback was performed at 20 mm/s during flush of 4–6 mL/s iso-osmolar contrast. A segment length of 54 mm was visualized and images were stored digitally for subsequent offline analysis.
Optical coherence tomography image analysis
Offline OCT analysis was performed independently by two investigators blinded to patient characteristics and the stent used. Proprietary software (LightLab Imaging Inc.) was used to analyze cross-sections at 1-mm intervals (every five frames) within the stented segment. Stent cross-sectional area (CSA) and lumen CSA were traced semi-automatically. Neointimal hyperplasia (NIH) area was calculated by subtracting lumen CSA from stent CSA. The percent NIH area was calculated as the ratio of NIH area to the stent CSA, multiplied by 100. In each cross-section, the number of struts was counted. Struts were classified as uncovered if any part of the strut was visibly exposed to the lumen or covered if a layer of tissue was visible all over the reflecting surfaces (Fig. 1a–d). The percentage of uncovered struts was calculated as the ratio of uncovered struts to all analyzed struts multiplied by 100. In covered struts, NIH thickness was measured from the strut marker to the endoluminal edge of the tissue coverage, following a straight line connecting the marker with the center of gravity of the vessel (9). Apposition was assessed by measuring the distance between the strut marker and the lumen contour following a straight line connecting the marker with the center of gravity of the vessel. A margin of 18 µm was added as a correction for half the blooming. Struts with distance to lumen contour greater than the sum of strut thickness + polymer thickness (in case of EES) + 18 µm were considered malapposed. Given a coated strut thickness of 91 µm, we adopted a malapposition threshold of 110 µm for BAS (91 µm + 0 µm + 18 µm = 109 µm). Similarly, given a strut thickness of 79 µm and a polymer thickness of 16 µm, we adopted the same malapposition threshold (110 µm) for EES (79 µm + 16 µm + 18 = 113 µm). Struts located at the ostium of a side branch were classified as non-apposed side branch struts and were excluded from the analysis. Non-apposed side branch struts were excluded from analysis, since we considered that this specific category of struts might have different healing characteristics as they are not in close contact with the vessel wall, compared with struts facing the vessel wall; and therefore, inclusion in the analysis would be confusing when we report the comparative healing characteristics of different stent designs. Thrombus was defined as an irregular high- or low-backscattering (red or white thrombus) mass protruding into the lumen discontinuous from the surface.
Representative optical coherence tomography images of titanium-nitride-oxide-coated stents (a, b) and everolimus-eluting stents (c, d) at 18-month follow-up: (a) struts covered with a neointimal layer of varying thickness seen around the contour, (b) thick neointimal layer over some struts measuring 740 µm at 9 o’clock, (c) struts covered with a thin neointimal layer seen around the contour, (d) uncovered struts from 5 to 9 o’clock.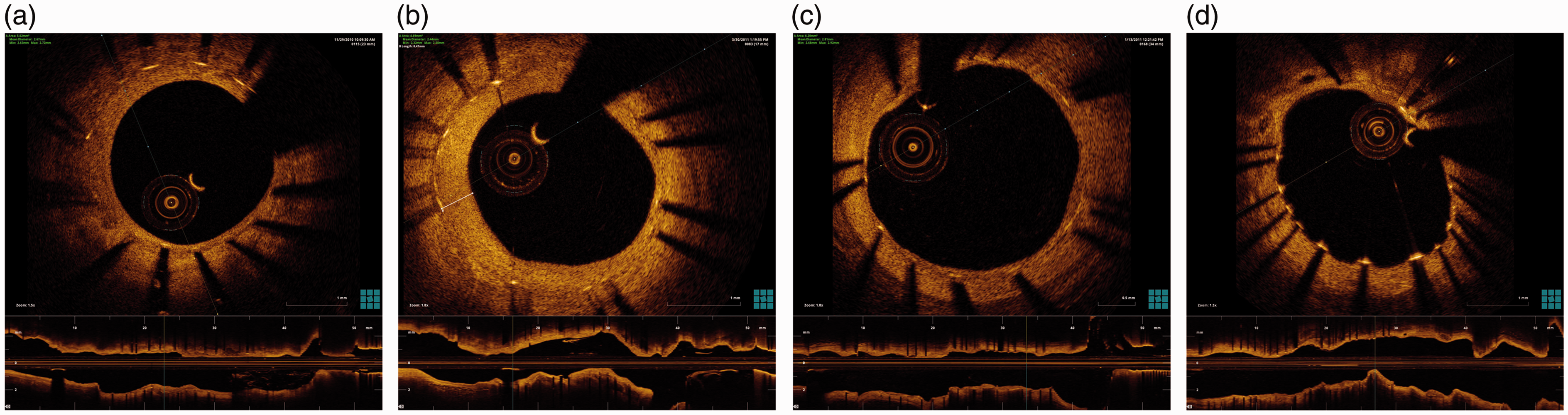
Statistical analysis
The primary endpoint of the current study was binary stent strut coverage (the ratio of covered struts to all analyzed struts multiplied by 100) in BAS versus EES. It was assumed that an average of 150 struts per patient would be analyzed; and therefore, we calculated that inclusion of 12 patients in each group would identify a 5% difference in binary stent strut coverage between BAS and EES (power 80%, two-sided type I error of 0.5). Co-primary endpoint was the percentage of malapposed struts in BAS versus EES. Categorical variables were described with absolute and relative frequencies (percentage), whereas continuous variables were reported as mean ± standard deviation. Pearson χ2 test, Fisher’s exact test, unpaired t test, Mann–Whitney test, or Spearman test were used for comparison between the two groups, as appropriate. Binary stent strut coverage and the percentage of malapposed struts were analyzed at strut level and comparison between the two groups was performed using the Mann–Whitney test, since these variables were not normally distributed. Statistical analysis was performed using SPSS statistical software (SPSS v. 16.0.1, SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics of the OCT subgroup
Baseline clinical characteristics of the two individual study groups.

Continuous variables are presented as mean ± SD, whereas categorical variables are presented as frequency (percentage).
ACEI, angiotensin converting enzyme inhibitors; ACS, acute coronary syndrome; ARB, angiotensin II receptor blockers; BAS, bioactive stents; EES, everolimus-eluting stents; NSTEMI, non-ST-elevation acute coronary syndrome; STEMI, ST-elevation myocardial infarction.
Lesion and procedural characteristics of the two individual study groups.
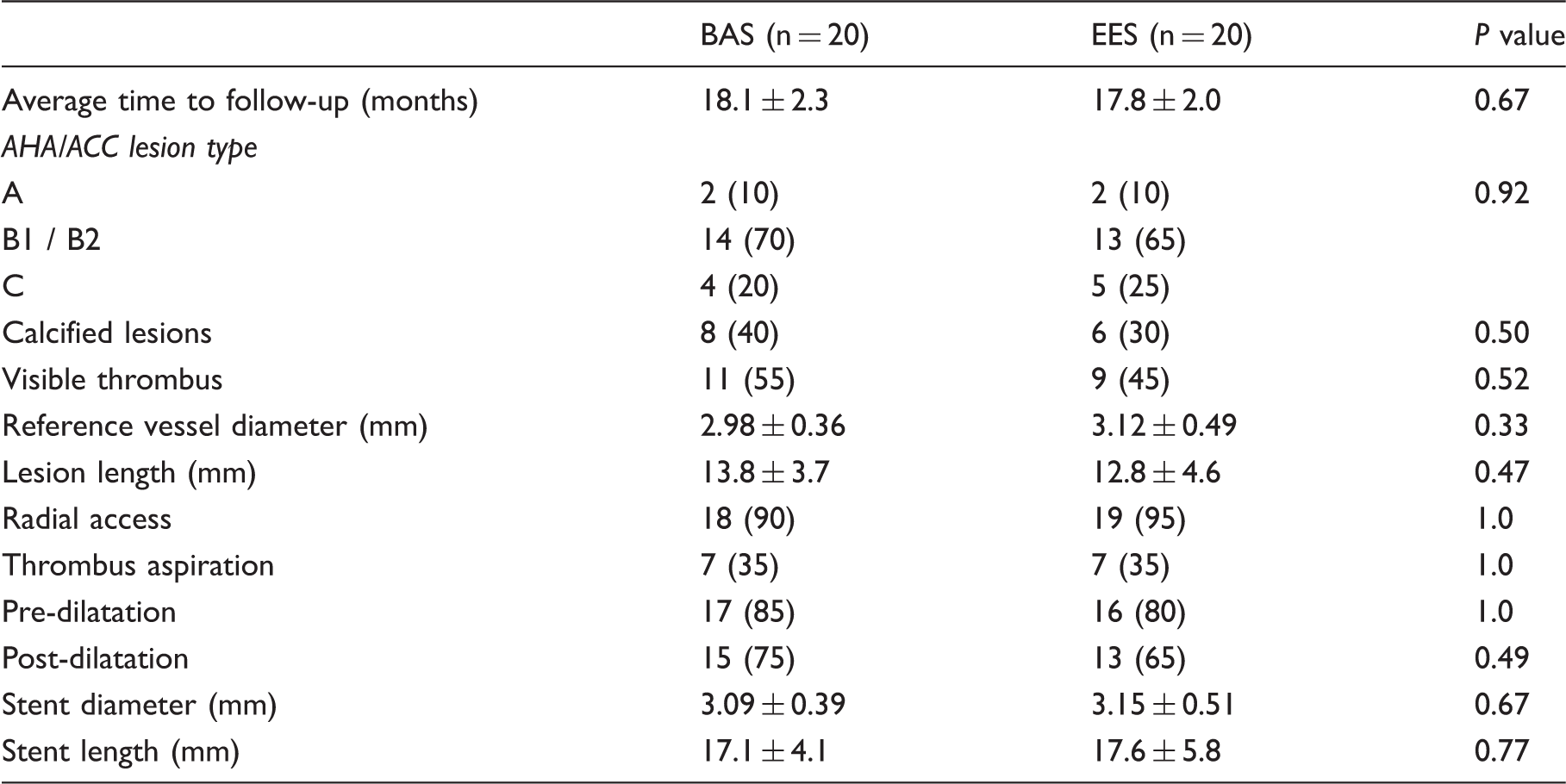
Continuous variables are presented as mean ± SD, whereas categorical variables are presented as frequency (percentage).
BAS, bioactive stents; EES, everolimus-eluting stents.
Optical coherence tomography data
OCT measurements in the two individual study groups.
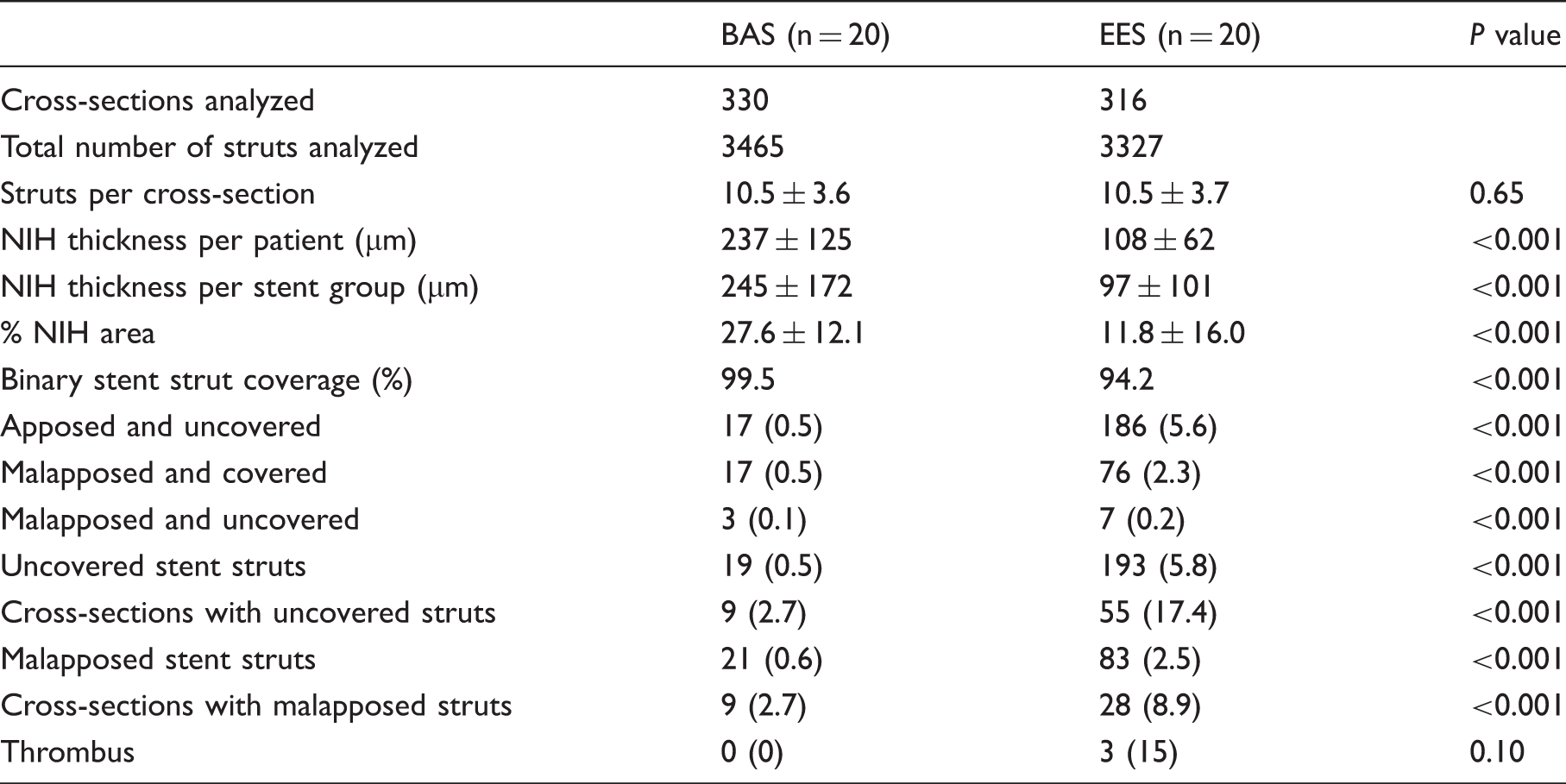
Continuous variables are presented as mean ± SD, whereas categorical variables are presented as frequency (percentage).
BAS, bioactive stents; EES, everolimus-eluting stents; NIH, neointimal hyperplasia.
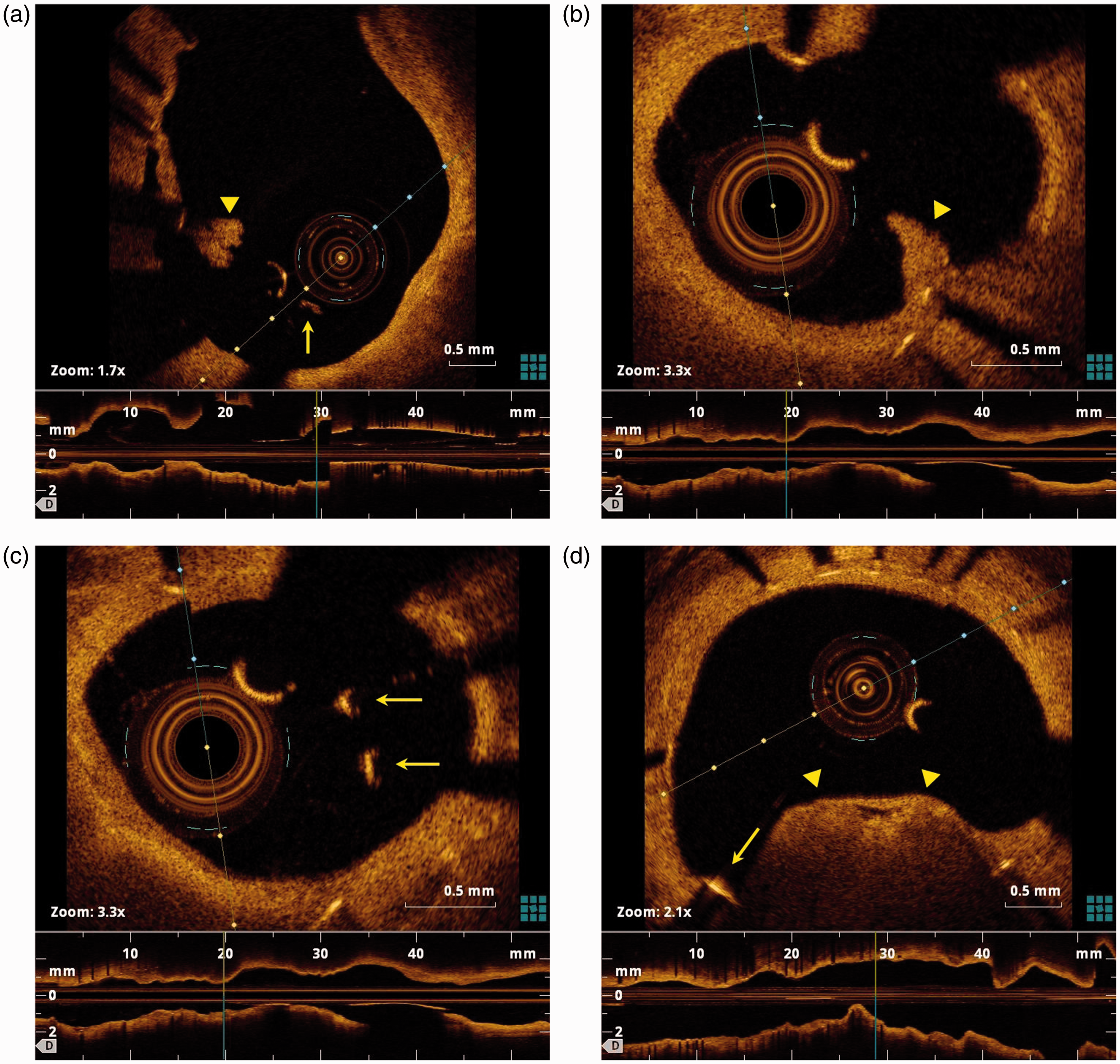
Intra-stent thrombus observed during follow-up optical coherence tomography in three patients who received everolimus-eluting stents: (a) patient 1, arrowhead = white thrombus, arrow = malapposed strut; (b) patient 2, arrowhead = white thrombus; (c) patient 2, arrows = malapposed struts; (d) patient 3, arrowheads = red thrombus, arrow = uncovered strut.
Discussion
In the current post-hoc analysis, binary stent strut coverage, based on strut-level analysis, was higher with BAS versus EES by OCT performed at 18-month follow-up; the strut-level percentage of malapposed struts was lower with BAS; yet, BAS induced thicker NIH. To the best of the authors’ knowledge, this is the longest-term OCT follow-up of titanium-nitride-oxide-coated stents reported to date.
Vascular healing is a key concern after coronary stent implantation. Impaired neointimal healing was common in autopsy analysis of patients who died of late ST from a registry of human coronary stents (10). The best histologic morphometric predictor of late ST was the ratio of uncovered to total stent struts (1). So far, however, no clinically relevant cutoff value of the percentage of uncovered struts was identified as a reliable predictor of late ST. Yet, the length of segment with uncovered struts by OCT independently predicted late and very late ST (median follow-up, 615 days: range, 172–1836 days) (4). However, the relative contribution of uncovered struts to the occurrence of late ST appears to decrease with longer duration of follow-up (5). The percentage of uncovered struts tends to decrease progressively with time due to progressive neointimal growth/healing (11–13). The strut-level percentage of uncovered struts associated with BAS in the current 18-month evaluation was similar to that reported for a separate cohort in the same stent group evaluated at 9 months (0.5% and 0.6%, respectively) (8). In two prior OCT studies of unselected patients who received BAS, the percentage of uncovered struts was 3.7% and 2.8%, at 2- and 4-week follow-up, respectively (14,15). Unfortunately, no immediate post-procedural OCT was performed in the BASE-ACS trial. On the other hand, the percentage of uncovered struts associated with EES decreased from 10.8% at 9 months to 5.8% at 18 months (8). The latter percentage was similar to that reported in the EES arm of the RESOLUTE All Comers trial (5.8% uncovered struts) with OCT performed at 13-month follow-up (16). Comparably, Choi et al. reported a prevalence of 4.4% uncovered struts by OCT 9 months after EES implantation (17); the prevalence reported at the same time point of follow-up was 2.26% in a recently published study (18). Moreover, in serial OCT assessment, Kim et al. observed that the percentage of uncovered struts associated with EES decreased from 6.9% at 3 months to 1.3% at 12 months (19). In another study, OCT performed at an average follow-up of 24.9 months demonstrated 1.9% uncovered struts in the EES group (20). In contrast, a single study reported a percentage of 0.6% uncovered struts both 12 and 24 months following EES implantation (21). In two separate studies, the percentage of uncovered struts associated with another second-generation DES (Resolute® zotarolimus-eluting stent) was 4.4% and 7.4% at 9-month and 13-month follow-up, respectively (16,22). In another study by Kim et al., serial OCT assessment of a biolimus-eluting stent with a biodegradable polymer (BiomatrixFlix®) revealed 14.7% uncovered struts at 3-month follow-up; that percentage decreased to 8.6% at 12-month follow-up (23). Yet, in a substudy of the LEADERS trial, the same stent type was associated with 0.6% uncovered struts with OCT performed at 9 months (24). Divergence between studies reporting on the same stent type might be explained by differences in the study population characteristics, different time points of follow-up, different OCT systems used for evaluation, as well as inter-study and inter-observer variability.
Stent segments with acute strut malapposition early after implantation portend a higher risk of delayed strut coverage and late malapposition, compared with well-apposed segments (25). The relative importance of strut malapposition to the occurrence of late ST appears to increase with longer follow-up; malapposition was the most frequent finding in a series of patients presenting with very late ST (median follow-up, 4.7 years; interquartile range, 3.1–7.5 years) (5). The strut-level percentage of malapposed struts associated with BAS in the current 18-month evaluation, was slightly higher than that reported for a separate cohort in the same stent group evaluated at 9 months (0.6% and 0.2%, respectively) (8). This can be viewed in light of the trial population presenting with ACS (nearly 40% acute ST segment elevation myocardial infarction, visible thrombus in 46.3% in the BAS arm). In such patients, thrombus dissolution and plaque regression underneath the stent could possibly result in late acquired strut malapposition (26). On the other hand, the percentage of malapposed struts associated with EES decreased from 4.6% at 9 months to 2.5% at 18 months (8). With progressive neointimal healing, previously malapposed struts ultimately become completely integrated into the vessel wall (25). Comparably, the percentage of malapposed struts in the EES arm of the RESOLUTE All Comers trial was 1.4% with OCT performed at 13-month follow-up (16). Nevertheless, three prior studies reported lower percentages of malapposed struts associated with EES (0.4% at 9 months, 0.11% at 9 months, and 0.1% at 2 years) (17,18,20). Two other studies reported similarly low percentages of malapposed struts associated with the Resolute® zotarolimus-eluting stent (0.1% and 1.8%) at 9- and 13-month follow-up, respectively (16,22). Yet, in the LEADERS trial, biolimus-eluting stents were associated with 0.2% malapposed struts, with OCT performed at 9 months (24). In the two OCT follow-up reports of the BASE-ACS trial, the percentage of malapposed struts associated with BAS was lower than that associated with EES, both at 9 and 18 months (data not serial), but was similar to those associated with other second-generation DES at similar time points of follow-up (8,22,24).
Expectedly, the mean NIH thickness was greater with BAS versus EES at both 9- and 18-month follow-up (8). The mean NIH thickness previously reported for BAS with OCT performed at 2- and 4-week follow-up was 71 and 109 µm, respectively (14,15). The slightly lower NIH thickness associated with BAS at 18-month follow-up, compared with that reported from the trial patients at 9-month follow-up (237 and 274 µm, respectively) remains unclear (data not serial). The NIH thickness associated with BAS at both 9- and 18-month follow-up was similar to that reported for the Endeavor® zotarolimus-eluting stent in two previous studies at earlier time points of follow-up (251 µm at 9 months and 332 µm at 6 months) (27,28). Yet, the NIH thickness reported for the Resolute® zotarolimus-eluting stent was less (116 µm at 13 months and 166 µm at 9 months) (16,22). On the other hand, the mean NIH thickness associated with EES at both time points (100 µm at 9 months and 108 µm at 18 months) was similar to those reported previously for EES at various time points of follow-up (142 µm at 13 months, 115 µm at 9 months, 93 µm at 9 months, and 109 µm at 2 years) (16–18,20).
The current study was based on a relatively small sample size and therefore the results should be taken with caution. An important limitation of the current study is reporting the binary stent strut coverage and the percentage of malapposed struts based on strut-level analysis. It is well acknowledged that OCT datasets are characterized by hierarchical distribution of data: stent struts nested within individual lesions are not independent. Therefore, the multi-level and aggregated analysis methods are more appropriate for lesion-level analysis. Moreover, the current OCT technology cannot detect neointimal coverage of less than 10 µm thickness; therefore, it cannot identify very thin layers of neointimal coverage. Another limitation is that OCT was not performed before and immediately after the index procedure. Additionally, no independent core lab was involved in data analysis. Finally, the current post-hoc analysis was underpowered to correlate OCT findings with clinical endpoints; hence, larger studies are needed to address the clinical implication of these findings.
In conclusion, in the current post-hoc analysis, with OCT performed at 18 months, binary stent strut coverage based on strut-level analysis was higher with BAS versus EES; strut-level malapposed struts were fewer with BAS; yet, BAS induced thicker NIH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.