
Abstract
Background
Metallic dental prostheses may degrade image quality on head and neck computed tomography (CT). However, there is little information available on the use of dual-energy CT (DECT) and metal artifact reduction software (MARS) in the head and neck regions to reduce metallic dental artifacts.
Purpose
To assess the usefulness of DECT with virtual monochromatic imaging and MARS to reduce metallic dental artifacts.
Material and Methods
DECT was performed using fast kilovoltage (kV)-switching between 80-kV and 140-kV in 20 patients with metallic dental prostheses. CT data were reconstructed with and without MARS, and with synthesized monochromatic energy in the range of 40–140-kiloelectron volt (keV). For quantitative analysis, the artifact index of the tongue, buccal, and parotid areas was calculated for each scan. For qualitative analysis, two radiologists evaluated 70-keV and 100-keV images with and without MARS for tongue, buccal, parotid areas, and metallic denture. The locations and characteristics of the MARS-related artifacts, if any, were also recorded.
Results
DECT with MARS markedly reduced metallic dental artifacts and improved image quality in the buccal area (P < 0.001) and the tongue (P < 0.001), but not in the parotid area. The margin and internal architecture of the metallic dentures were more clearly delineated with MARS (P < 0.001) and in the higher-energy images than in the lower-energy images (P = 0.042). MARS-related artifacts most commonly occurred in the deep center of the neck.
Conclusion
DECT with MARS can reduce metallic dental artifacts and improve delineation of the metallic prosthesis and periprosthetic region.
Keywords
Introduction
Computed tomography (CT) plays an important role in visualizing the head and neck region to evaluate various diseases, including tumors and inflammation (1). However, many patients have metallic dental prostheses such as dental fillings or implants (e.g. amalgam, cobalt-chromium, nickel-chromium, gold alloy), which may degrade image quality by causing artifacts, such as beam hardening and photon starvation artifacts. These artifacts frequently degrade the image quality of the oral cavity and buccal area, making it difficult to delineate important anatomical structures or pathologic conditions (1–3).
To overcome metallic dental artifacts, removal of metallic dental prostheses is ideal, but is not practical in most cases. The second method involves the use of dual-energy CT (DECT). Virtual monochromatic imaging produced by dual-energy acquisition can reduce beam hardening artifacts (4). Beam-hardening artifacts result from the X-ray polychromaticity. Because low-energy X-rays are preferentially absorbed when passing through a metallic prosthesis, the average energy of the X-ray beam increases (beam hardening), which causes CT number shifts, resulting in dark bands or streaks near a dense object (3). In contrast, monochromatic X-ray does not show an increased mean energy after passing through a metallic prosthesis, thereby reducing perceived artifacts (5).
The third method employs the use of metal artifact reduction software (MARS) (6). With MARS, metal prostheses can be segmented from the conventionally reconstructed images based on a CT number threshold. Using forward projection, the metal artifact-corrected images are overlaid on the original images. MARS can also replace photon-starved regions with information derived from accurate projection measurements using material decomposition on the corrected projections and monochromatic images (4,7).
In a previous study using a human cadaver, MARS reconstruction in CT images of the oral cavity was reported to decrease the artifact area related to dental hardware (1). However, there is little information available on the use of DECT with MARS in the head and neck regions to reduce metallic dental artifacts.
The purpose of this study was to assess the usefulness of DECT with virtual monochromatic imaging and MARS for reducing metallic dental artifacts.
Material and Methods
Study population
This retrospective study was approved by the institutional review board of our hospital, and the requirement for informed consent was waived. In February 2013, 20 patients with metallic dental prostheses were enrolled in this study (12 men, 8 women; mean age, 54.7 years; age range, 23–78 years). The CT examinations of the neck were performed for cancer work-up (n = 17), neck pain (n = 1), dry mouth (n = 1), or sialolithiasis (n = 1).
CT protocol
CT was performed on a 64-channel DECT (GE Discovery CT 750 HD, GE Healthcare, Waukesha, WI, USA) using fast kV-switching Gemstone spectral imaging (GSI) between 80-kVp and 140-kVp. CT scans were acquired with 40 mm beam collimation, 2.5 mm reconstructed slice thickness, 0.7 s rotation speed, 275 mA, and 0.969:1 pitch. All CT scans were obtained parallel to the orbitomeatal line. The contrast agent (300 mg of iodine/mL [Omnipaque 300; GE Healthcare, Princeton, NJ, USA]) was injected at a flow rate of 3 mL/s (volume, 90 mL). A scan delay of 60 s was used. The CT dose index (CTDIvol) and dose length product (DLP) were 26.9 mGy and 866.8 mGy-cm, respectively. The images were reconstructed both with and without MARS. Synthesized monochromatic images in the range of 40–140-keV were generated using dedicated GSI viewer software (GSI viewer 2.00 and GE Volume Share 4 AW 4.4, GE Healthcare).
Image analysis
Both quantitative and qualitative analyses were performed. For quantitative analysis, manually drawn elliptical regions of interest (ROIs) were placed on the five representative soft tissue areas, including the oral tongue, bilateral buccal, and parotid areas in one representative slice, by one author (JC) (Fig. 1). ROIs were drawn to include reference tissue as much as possible (e.g. gland tissue for parotid area, fat tissue for buccal area, tongue tissue for oral tongue area). Hounsfield units (HUs) within the same ROIs on the monochromatic images in the range of 40–140-keV with and without MARS were extracted using Matlab software (MathWorks, Inc., Natick, MA, USA) to perform further analysis. To quantify the severity of metal artifacts, the artifact index (AI) was introduced, which was defined as AI = SDa / SDb, where SDa is the noise in the ROI measured on the image of particular energy and SDb, the noise in the ROI on the corresponding 70-keV reference image without MARS. We compared the AIs in the five soft tissue areas, which were calculated on the monochromatic images in the range of 40–140-keV with and without MARS.
Example image shows the ROIs placement on the tongue, bilateral buccal, and parotid areas for quantitative analysis. Elliptical ROIs were drawn on the one representative axial slice.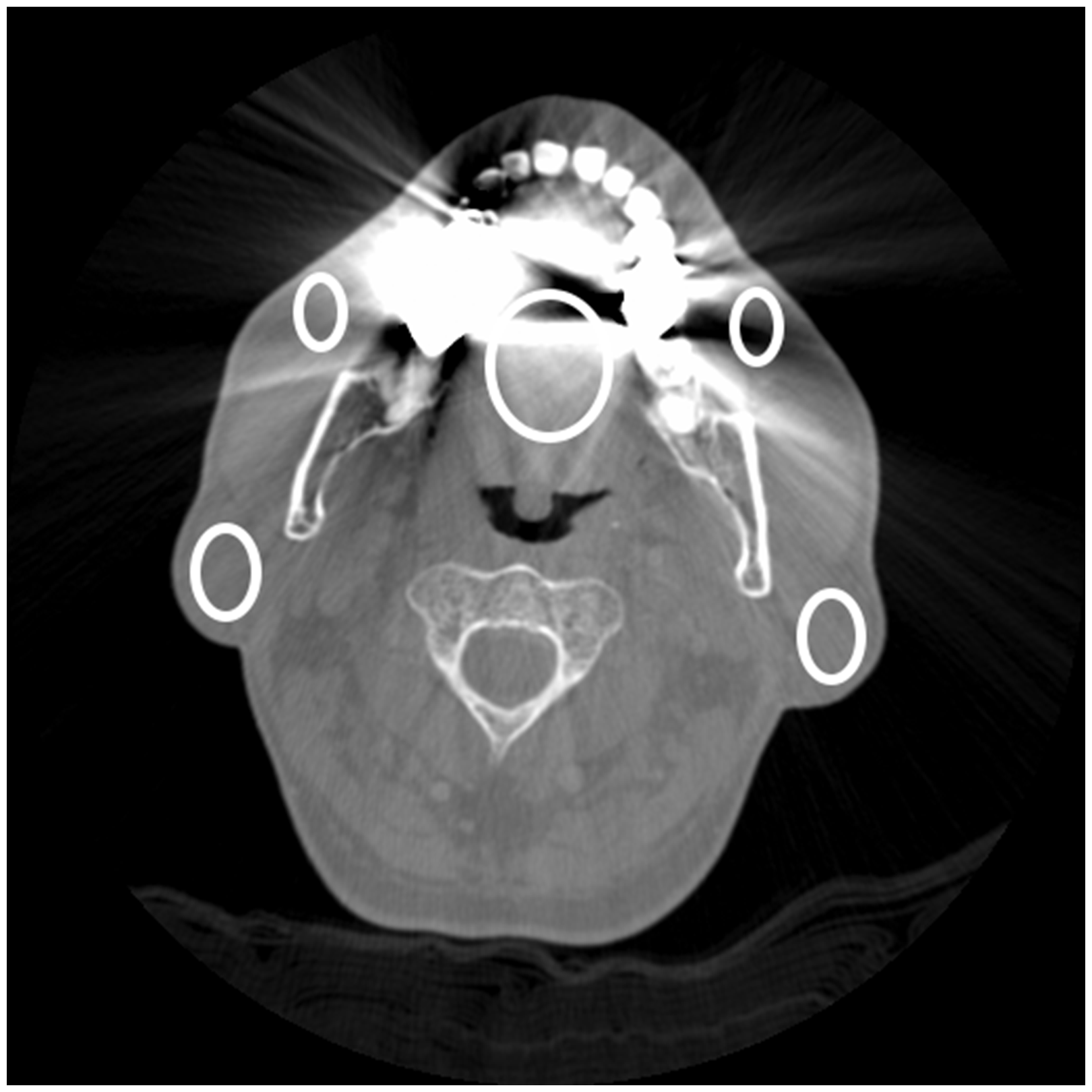
For qualitative analysis, two authors (JC and H-J K, neuroradiologists with 5 and 25 years of experience, respectively) evaluated the 70-keV and 100-keV images both with and without MARS. Discrepancies were resolved by consensus. We chose the 70-keV image, because it best resembles the 120-kVp polychromatic image which is standard for soft tissue evaluation (8). We also chose the 100-keV image, because the preliminary quantitative analysis revealed almost plateau pattern of the AIs on the images above 100-keV and soft tissue contrast is expected to be reduced on the images using an extremely high energy above 100-keV. The quality of these 70-keV and 100-keV images was evaluated at the five soft tissue areas (oral tongue, bilateral buccal, and parotid areas) using soft tissue window (window width, 300 HU; window level, 30 HU) with a four-point scale as follows: 1 (unacceptable), when the anatomy was nearly unrecognizable; 2 (poor), when the artifacts covered more than 50% of the area; 3 (fair), when the artifacts covered less than 50% of the area; 4, (good), when there were no or only minor streak artifacts. Metallic dental prostheses were also evaluated using bone window (window width, 3077 HU; window level, 570 HU) with a three-point scale as follows: 1 (poor), when the margin and internal architecture were unrecognizable; 2 (fair), when the margin and internal architecture could be identified but blurred; 3 (good), when the margin and internal architecture were clearly seen. Finally, we recorded any potential artifact generated by application of the MARS algorithm (MARS-related artifact, Fig. 2).
Example of MARS-related artifact. Note the difference between the 70-keV image without MARS (a) and with MARS (b). The MARS-related artifacts are demonstrated as thick bands or streaks and most commonly occurs in the deep center area including retropharynx, perivertebral space, and spinal cord (arrows).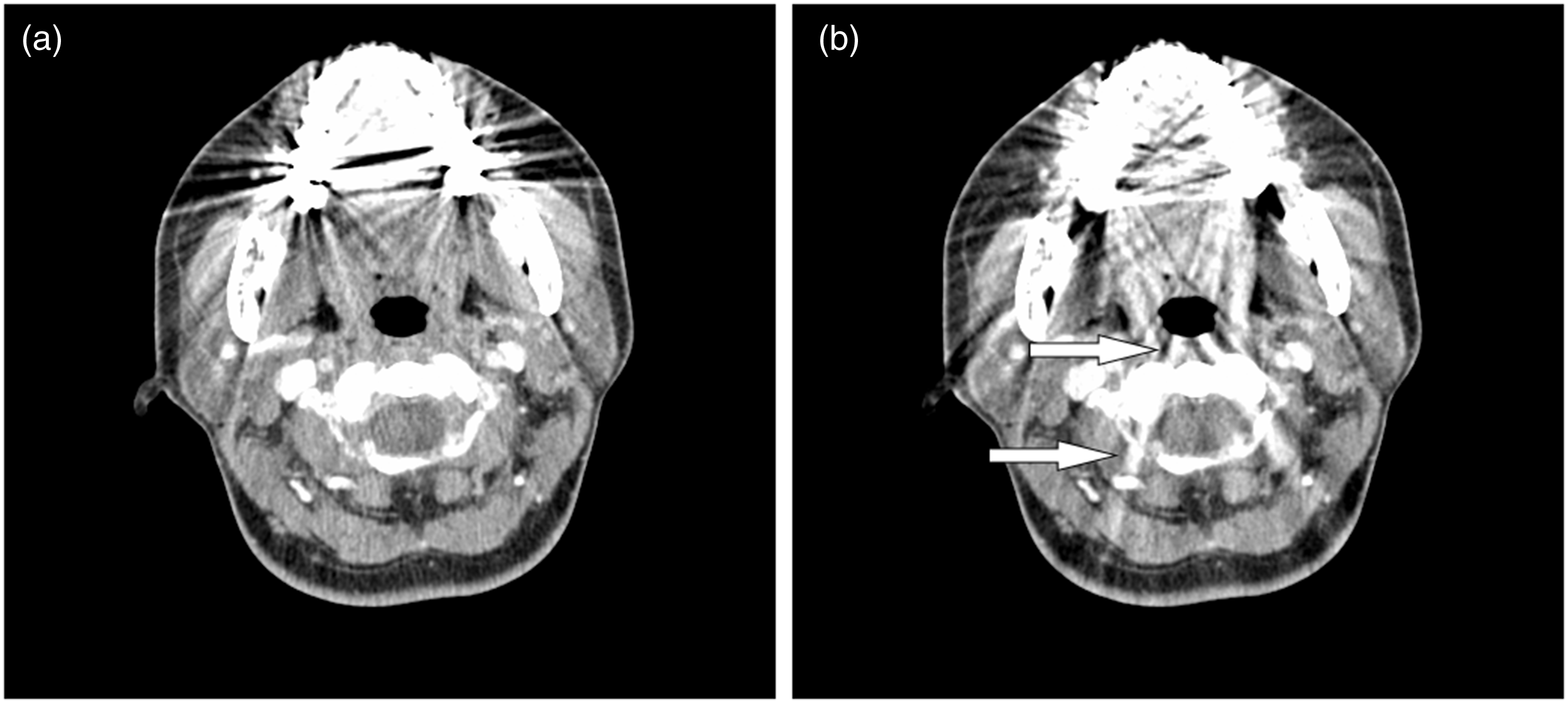
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics 21 (IBM Corp., Armonk, NY, USA) and R statistical software version 3.1.3 (R foundation for Statistical Computing, Vienna, Austria). We used the Mann–Whitney test to compare the scores determined from the five soft tissue areas and metallic dental prostheses on the 70-keV and 100-keV images obtained with and without MARS. For all statistical values, P values < 0.05 were considered to indicate a statistically significant difference.
Results
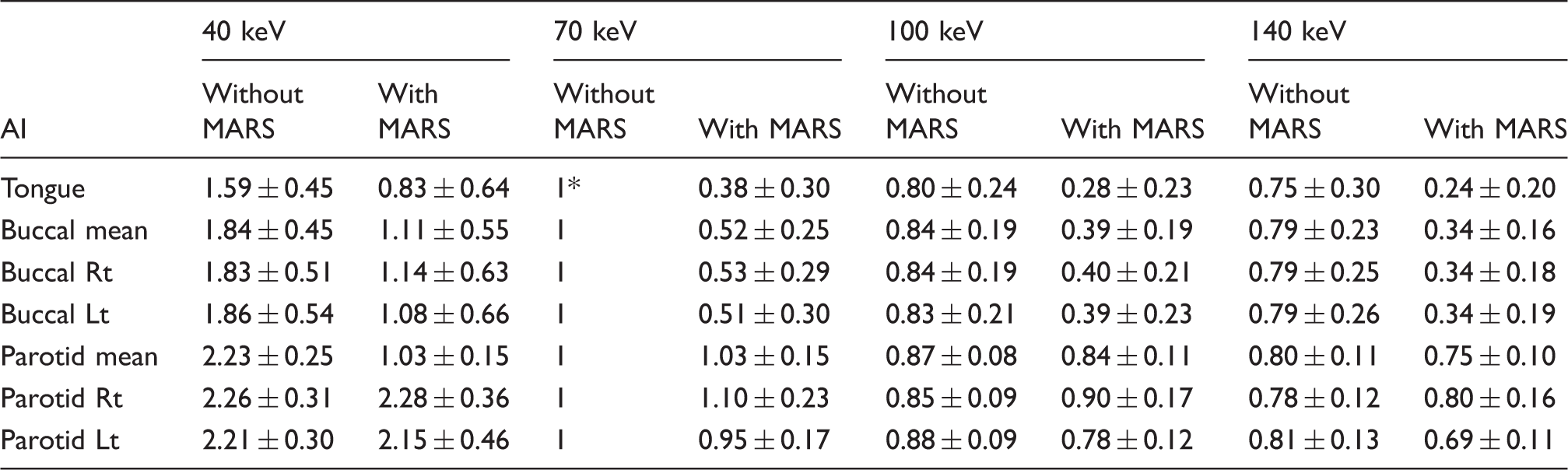
In the quantitative analysis, at all energy levels, the AIs in the tongue and buccal areas were markedly less with MARS than without it (0.38 and 0.52, respectively, for 70 keV). However, those in the parotid areas were near the same both with and without MARS (1.03 for 70 keV). Irrespective of the use of MARS, the AIs gradually decreased as keV increased. However, this effect was more prominent on the monochromatic images with lower keV (<100 keV). On the images with an energy greater than 100 keV, the AIs showed a plateau. Fig. 3 shows the AIs of each area without MARS and with MARS on quantitative analysis. Examples of AIs in several selected energies (40, 70, 100, and 140 keV) in each area (tongue, buccal, parotid area) are shown in Table 1.
Barplots show mean and 95% confidence interval of AI according to keV (40–140 keV) with and without MARS in tongue (a), buccal (b), and parotid (c) area in quantitative analysis. Without MARS, AI gradually decreases with increasing keV; however, more than 100 keV shows almost plateau. With MARS, AI markedly decreases at all energy range compared to without MARS except parotid area. The representative AI with MARS and without MARS in each area in quantitative analysis. Numbers represent mean ± standard deviation. 70 keV without MARS as reference.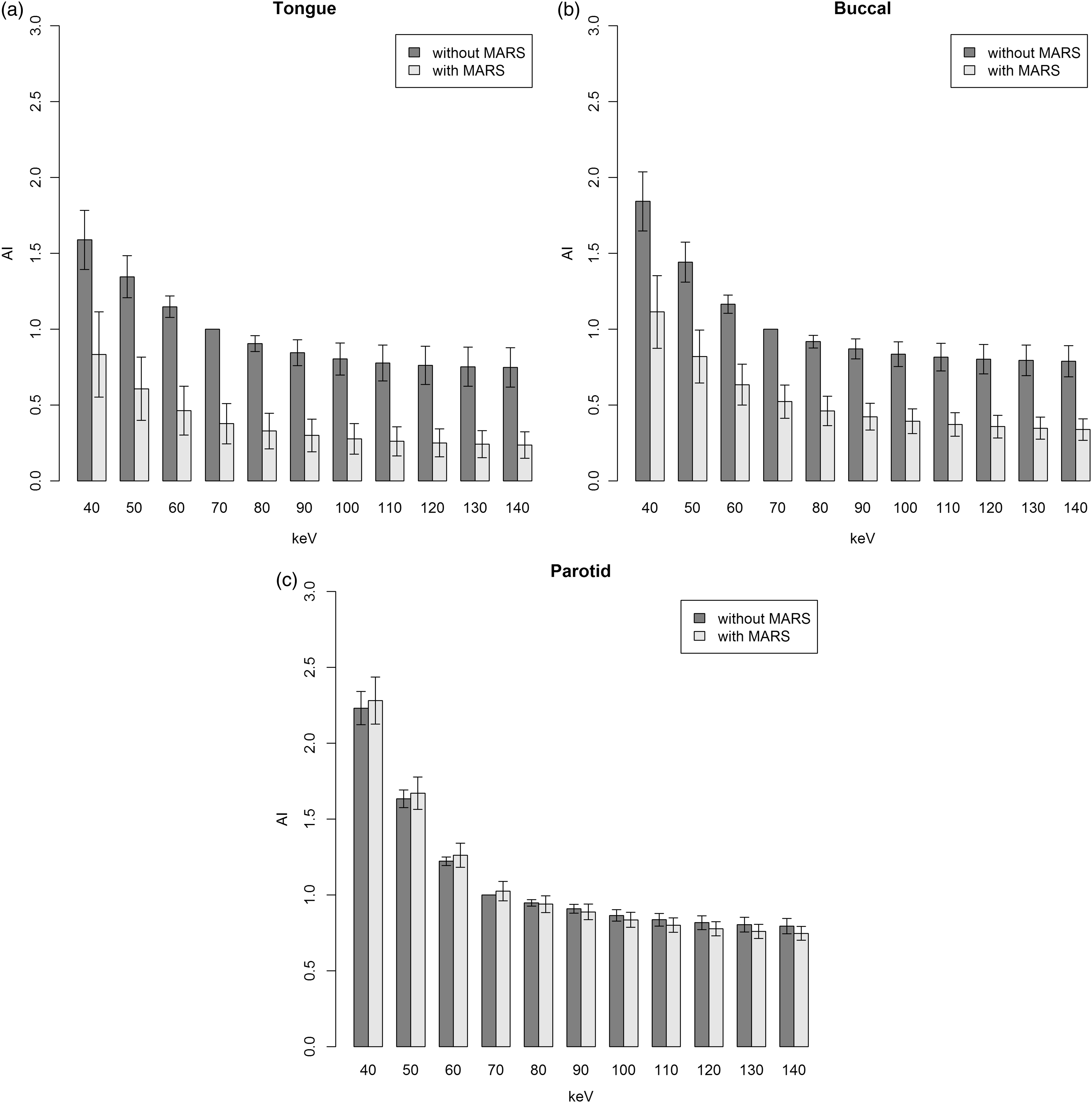
The image quality score in each area in qualitative analysis.
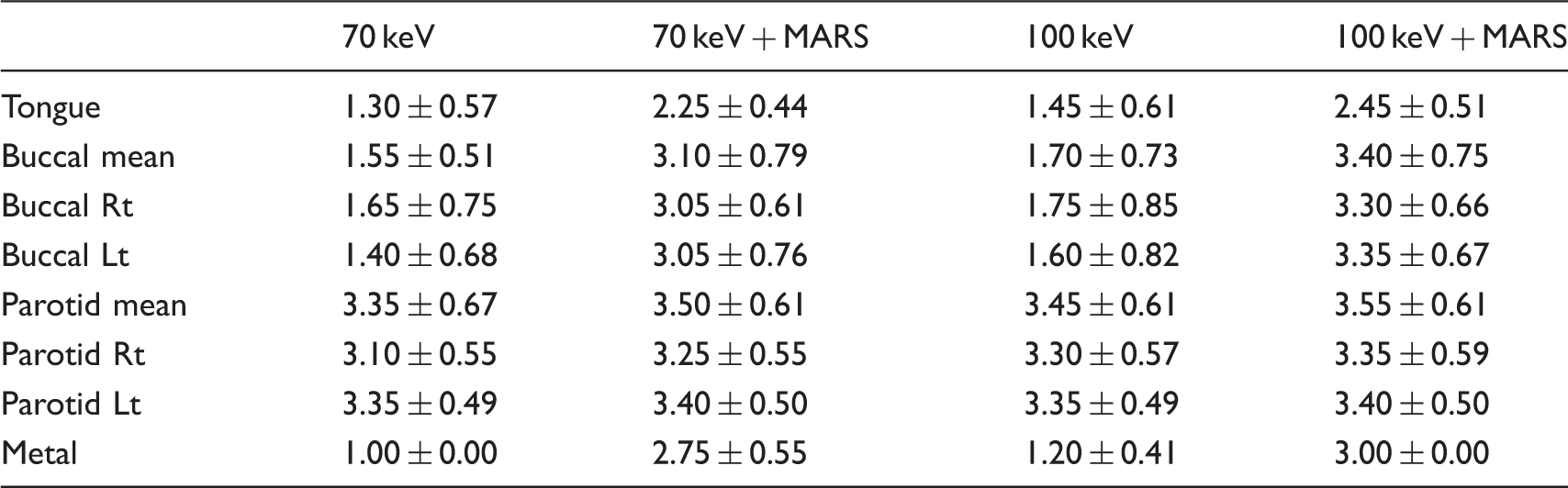
Numbers represent mean ± standard deviation.
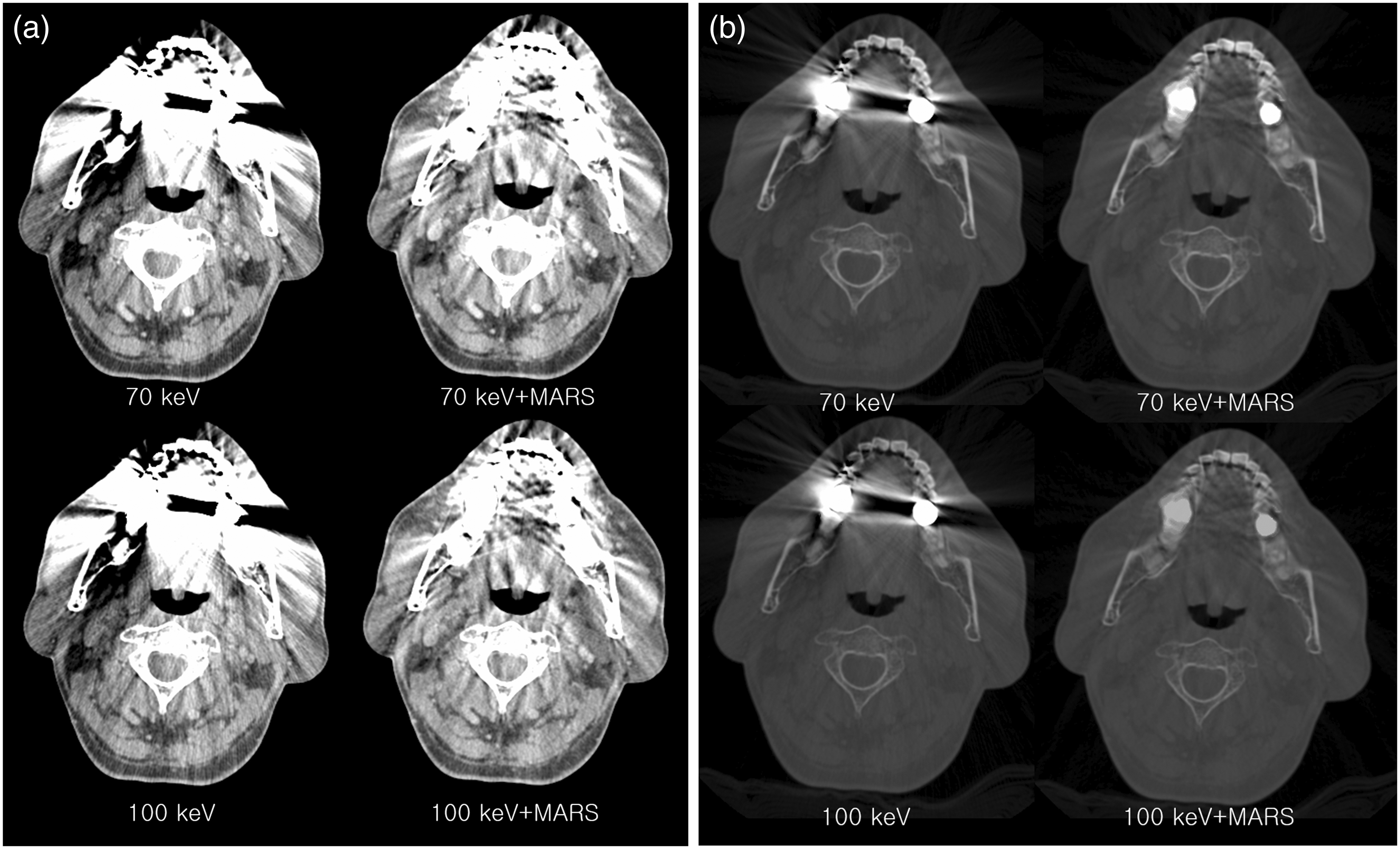
Representative case with soft tissue window (a) and bone window (b). With soft tissue window (a), metal artifact is decreased with MARS, especially in the tongue and buccal area. The artifact of parotid area is not decreased. The artifact is not significantly decreased on 100 keV compared to 70 keV. With bone window (b), the margin of metal is delineated better with MARS, and the difference of 70 keV and 100 keV is not definite.
The MARS-related artifacts appeared as a thick band or streak, most commonly occurring in the deep central areas, including the retropharynx, perivertebral spaces, and spinal cord (n = 16). Less commonly, they occurred in the lateral neck (n = 4) and tongue (n = 1) (Fig. 2).
Discussion
In this study, we evaluated the performance of the metal artifact reduction in head and neck region using virtual monochromatic images derived from DECT, with and without MARS. Increased keV in the range of 70–100 keV was not sufficient to suppress metal artifacts related to dental metallic prosthesis. In contrast, MARS suppressed metal artifacts sufficiently even with low keV reconstruction. MARS with moderate keV (70–100 keV) reconstruction showed the best result. MARS improved the delineation of the metallic prosthesis itself as well as periprosthetic region. MARS was most effective in tongue and buccal space; however, there was no benefit of MARS in parotid area. Moreover, artifacts possibly related to the MARS algorithm occurred in the deep center of the neck such as retropharynx, perivertebral space, and spinal cord.
Dental metallic prostheses can result in artifacts that seriously reduce image quality of CT scans of the neck (1,9). Although great endeavors have been exerted to reduce dental artifacts, such as use of thinner slice reconstruction, higher kVp and mAs, and improved reconstruction algorithms (1,3,10), they still remain problematic. With DECT, we can synthesize monochromatic or monoenergetic imaging (11). In this study, we used simultaneous DECT acquisition with fast kV switching between 80 and 140 kVp (12,13). The fast switching between the two energy spectrums can eliminate motion misregistration and yield more consistent energy information (14–16). After dual energy CT data acquisition, we can produce virtual monochromatic imaging in the range of 40–140 keV using dedicated reconstruction software. Previous reports showed that monochromatic images with high energy (greater than 100 keV) displayed a superior image quality, with reduced metal artifacts, compared to conventional polychromatic images or monochromatic images with lower energy (4,11,14,17,18). Increasing the tube voltage increases the effective X-ray energy, which can improve beam penetration, resulting in decreased metal artifact (1). However, soft tissue contrast is also reduced with high energy, and thus delineation of soft tissues or contrast-enhancing lesions is more difficult on the high-energy images. A previous study showed that lesion enhancement peaked in the 40-keV series and CNR was highest in the 60-keV reconstructions (19). Therefore, in this study, we considered 100 keV as a reasonably high energy to evaluate metal as well as soft tissues. Our quantitative analysis also showed an almost plateau pattern of the artifacts on the high-energy images above 100 keV. Although the scores of image quality with 100 keV were slightly increased compared to those with 70 keV, the difference was not statistically significant. It means that an increased energy level from 70 keV to 100 keV is not enough to suppress metal artifacts related to dental prostheses. Higher energy such as 140 keV can be tried; however, image quality may be impaired on 140 keV due to decreased tissue contrast (20).
In addition to monochromatic reconstruction, the application of MARS has the potential to further decrease metal artifacts. In monochromatic images, photon starvation still exists and impairs the quality of the image (5). Indeed, MARS technology can be applied to various other metallic devices, such as hip prostheses, total knee arthroplasty prostheses, vertebral interbody fusion devices, and intracranial aneurysm coils. A previous report indicated that MARS reconstruction was better than standard reconstruction in nearly 60% of patients (21).
Like the previous studies, our study also revealed that MARS could suppress metal artifacts effectively even with low-energy reconstructions. In general, the performance for metal artifact reduction was even better on the images using standard energy with MARS than on those using higher energy without it. For example, while the AIs in the tongue were 0.38 and 0.28 on the 70-keV and 100-keV images with MARS, respectively, it was 0.75 on the 140-keV image without MARS. MARS improved the delineation of the metallic prosthesis itself as well as the periprosthetic region. The image delineation of the prosthesis and periprosthetic region depends on the change in energy (6). According to Brook et al. (21), spectral CT with the use of MARS improved tumor visibility in the vicinity of metal. In the present study, we focused on the periprosthetic regions. While the performance of MARS was almost equally good on the images using either 70 keV or 100 keV, extremely low- and high-energy reconstructions showed increased heterogeneity, probably due to increased noise.
Contrary to the literature supporting the value of MARS (6,17,21), there have also been several reports against MARS. In the study evaluating the effect of combined use of monochromatic images and MARS in patients with scoliosis having pedicle screws, Wang et al. (4) reported that although the artifacts around the screws were reduced on MARS-reconstructed images, screw visibility was also significantly reduced on those images. De Crop et al. (1) reported in their recent study with phantom and one human cadaver that MARS reconstruction was insufficient to reduce dental metal artifacts on CT images of the oral cavity and might even contribute adversely to image quality. Although they judged overall image quality by summing up the ratings at eight different regions of the neck, they did not present the ratings of image quality at the individual region. In terms of specific regions of the neck, our study revealed that MARS was effective in the tongue and buccal areas, whereas no benefit was found in the parotid areas and even induced MARS-related artifact in some area. In a previous study, Brook et al. (21) showed that MARS reconstruction eliminated the near-field artifacts but increased mildly the far-field artifacts in the study using gold fiducial markers. De Crop et al. (1) also found newly induced artifacts after MARS application in their cadaver study of head and neck region; however, the exact character and location of them were not described. The MARS-related artifacts can be explained by the fact that although MARS can effectively eliminate blooming of the metal, it can also introduce far-field artifacts of a “dark star” type on axial images, probably representing photon starvation (21,22). In the present study, we noted MARS-related artifacts appearing as a thick band or streak in the deep neck such as the retropharynx, perivertebral spaces, and spinal cord, distant from the metal prostheses, similar to previous studies (Fig. 2). We recommend that radiologists should use MARS with knowledge regarding its weak points and related artifacts to better interpret CT images of the neck.
Our study has several limitations. First, the exact composition of the dental prostheses was unknown. Because of the retrospective study in nature, identification of dental prostheses was difficult prior to scanning in this study. The composition of the prosthesis can influence image quality as MARS has been reported to be effective for the visualization of stainless steel, but not for titanium (6,23). Second, we only evaluated the effect of MARS in the subjects without pathology in the oral cavity. Further study on the ability of MARS to evaluate pathologic conditions is warranted. Third, other CT techniques that might be useful for reducing metal artifacts, such as iterative reconstruction, were not tested. Previous study showed iterative metal artifact reduction improves visualization of critical soft-tissue structures in patients with spinal hardware (10). In addition, the performance of various metal artifact reduction algorithms from different vendors may differ. Comparison studies analyzing these various MARS algorithms might be needed.
In conclusion, DECT with virtual monochromatic imaging and MARS can reduce dental metallic prosthesis-related artifacts and improve delineation of prostheses and the periprosthetic region. In contrast to the tongue and buccal areas, however, the effects of metal artifact reduction are limited in the parotid areas. In addition, MARS-related artifacts should be kept in mind for better image interpretation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.