
Abstract
Background
Computed tomography (CT) is used routinely for the preoperative detection of colorectal cancer (CRC) metastases. When small indeterminate focal liver lesions are detected that are too small to characterize (TSTC) on CT, additional imaging is usually needed, resulting in a potential delay in obtaining a complete diagnostic work-up.
Purpose
To determine the diagnostic accuracy of ultrasound (US) of the liver performed in direct conjunction to CT in the preoperative investigation among patients with newly diagnosed CRC when indeterminate liver lesions were found on CT.
Material and Methods
Preoperative investigations with CT and consecutive US where CT had shown at least one focal liver lesion in 74 patients diagnosed with CRC between June 2009 and February 2012 were retrospectively reviewed. Either histopathological findings or a combination of imaging and clinical follow-up one to three years after surgery was used as the reference.
Results
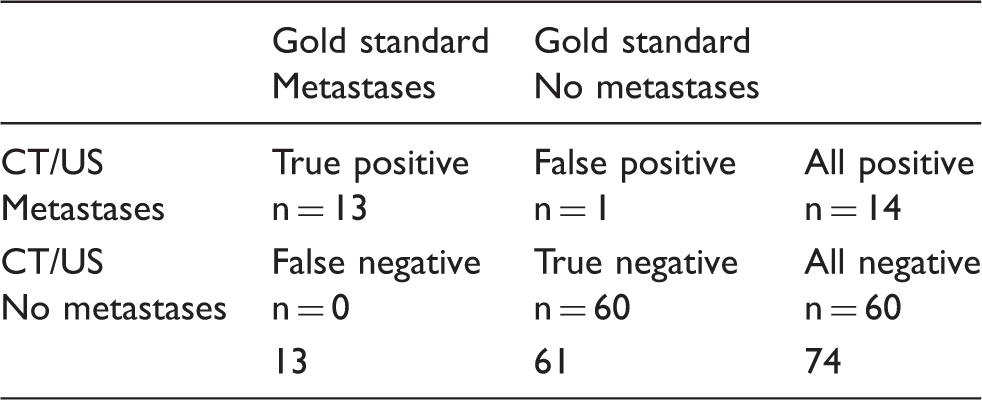
Liver metastases were diagnosed with CT/US in 13 out of 74 patients (17.6%). In one patient, a liver cyst was preoperatively regarded as liver metastasis by a combined CT/US. The sensitivity and specificity for the CT with consecutive US procedure was 100% (13/13) and 98.4% (60/61).
Conclusion
US performed in conjunction with CT in patients with indeterminate focal liver lesions on CT is an accurate work-up for detection of liver metastases in patients with newly diagnosed CRC. Although our results are promising, they cannot be considered safely generalizable to all hospitals.
Introduction
Colorectal cancer (CRC) is the third most common form of cancer in Sweden and the world (1). CRC tend to metastasize to the liver, about 15–25% of the liver metastases are synchronous, i.e. already diagnosed when the primary colorectal cancer is diagnosed (2–4). Curative treatment for these metastases can be offered in 10–30% of all colorectal cancer patients with metastatic disease (3). In general, 25% of patients become free of the metastases after surgery and five-year survival is around 40% in these cases (5). Early diagnosis increases the possibility for curative surgery and consequently long-term survival (6–9).
The most commonly used imaging modality to detect liver metastases preoperatively is computed tomography (CT). A challenge with imaging is that liver lesions smaller than 10 mm are frequently difficult to characterize, such as differentiating a small hypoattenuating cyst from a hypovascular metastasis (4). For characterization of these lesions, either ultrasound (US), contrast-enhanced ultrasound (CEUS), or magnetic resonance imaging (MRI) of the liver are commonly performed. With increasing complexity and demand on healthcare, this approach may both delay the time to treat as well as resulting in additional costs. For this reason, alternative approaches for diagnostic work-up should be explored.
The aim of this study was to investigate the value of the use of US, with or without contrast performed in conjunction with CT in the preoperative investigation of patients with newly diagnosed CRC in cases of indeterminate liver lesions on CT.
Material and Methods
Patients
Data from all patients who underwent surgical resection for colorectal cancer from June 2009 to February 2012 from one University Hospital were analyzed. Patients were retrieved from the Swedish Colorectal Cancer Registry, where data of all cancers are reported from both clinicians and pathologists. During this period, patients at this hospital were routinely scheduled both for CT and US at the same occasion to be able to directly perform US in all patients if indeterminate liver lesions were found on CT, or if in doubt whether a focal liver lesion was present or not. With this work-up there was also an opportunity to cancel US if CT was normal. All patients with indeterminate lesions found on preoperative CT and had a consecutive US performed were included in the study.
Due to practical reasons, not all patients had both CT and US on the same day. Although the median time between CT and US was < 1 day (range, 0–30 days) the mean time was three days.
MRI of the liver was performed preoperatively after CT and US in 14 patients and this investigation agreed with the results of the CT and US (seven patients with liver metastases and seven with benign lesions).
Regarding follow-up to provide a reference to preoperative CT/US findings, liver metastases were verified with either postoperative pathology or biopsy. In patients with palliative treatment where liver surgery was not performed, clinical and/or radiological follow-up was used as a reference. Benign liver lesions such as hemangioma or cysts were verified either by radiological (CT, US, or MRI) or clinical follow-up and carcinoembryonic antigen assay (CEA) (ref < 5 µg/L) (Fig. 1). In cases where it was questionable whether lesions detected at follow-up were new or present at the preoperative investigations, the radiological examinations were reviewed.
Study flow diagram.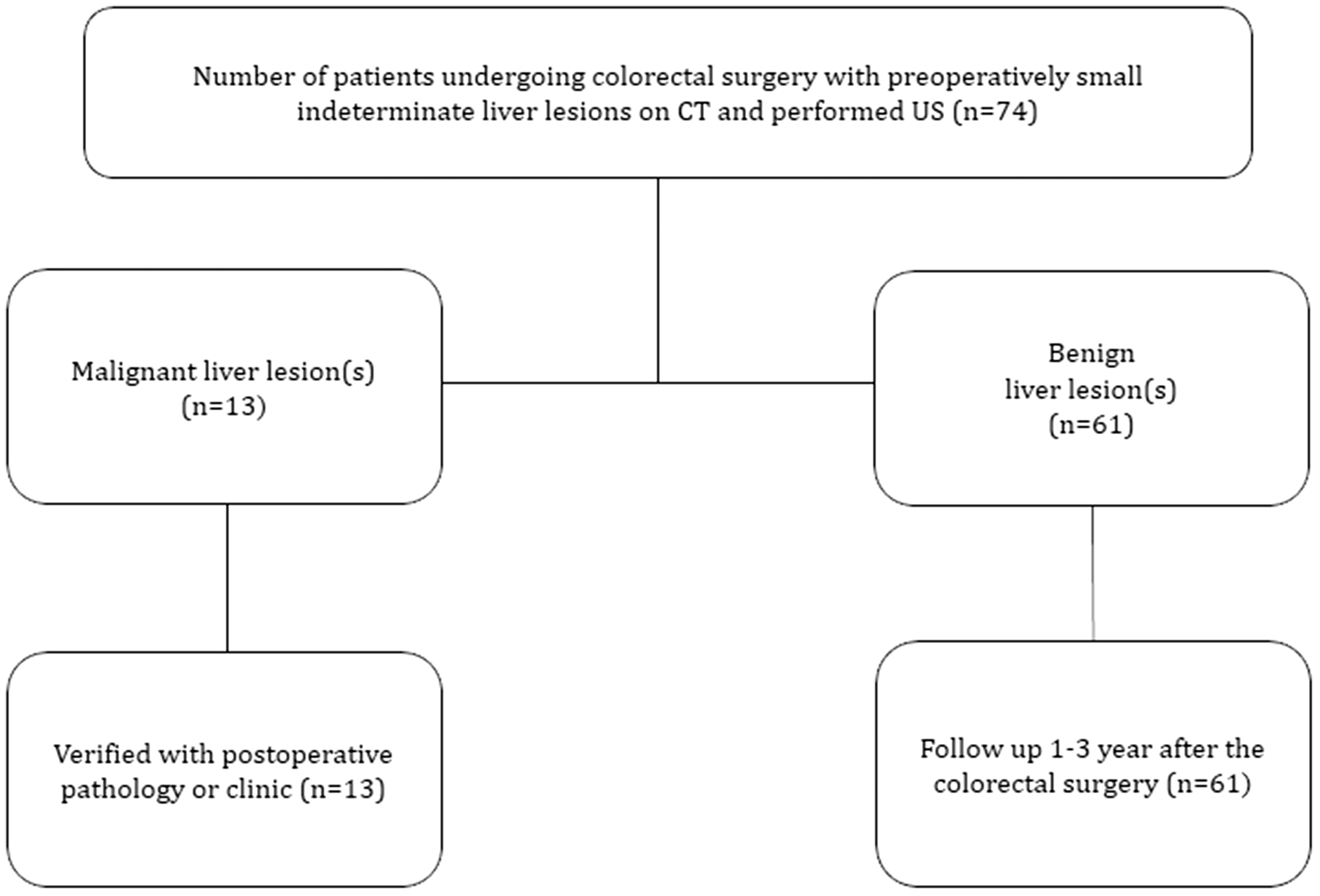
Baseline characteristics of patients with small, indeterminate liver lesions (n = 74).
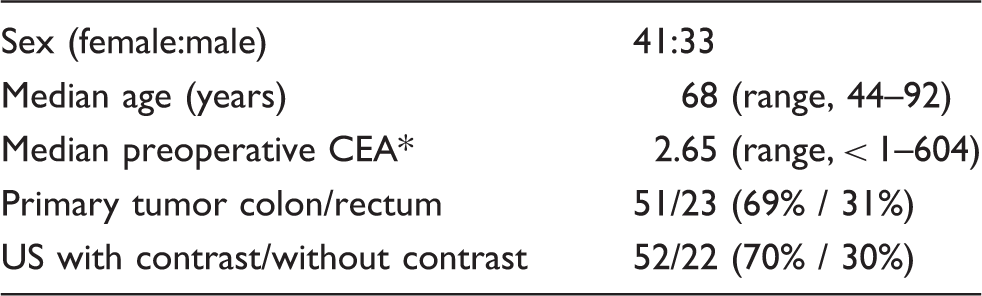
Three patients did not have CEA assessment.
CEA, carcinoembryonic antigen.
CT and US examinations
CT was performed with GE Healthcare Lightspeed (GE Healthcare, Milwaukee, WI, USA) scanners. A total of 500 mL of water was given as oral contrast 30 min before scanning with the last cup ingested 5 min before scan time. Imaging of the liver was performed with a slice thickness of 1.5-mm collimation, pitch 1.35, and was subsequently reconstructed to axial, coronal, and sagittal images with 5 mm thickness and 1 mm overlap. Omnipaque, 300 mg I/mL (GE Healthcare Inc, Princeton, NJ, USA) was injected at a rate of 3 mL/s (120 mL or 150 mL total for patients weighing < 60 kg or > 60 kg, respectively). Power injector was not used. The breath-hold acquisition was started 70 s following initiation of contrast injection. Scanning was performed from the lung bases to the anus.
US studies were performed using Sequoia 512 (Acuson, Mountain View, CA, USA). Baseline hepatic US was performed with a multifrequency 4C1 convex array probe. If the baseline study was inconclusive, CEUS was performed using the contrast pulse sequencing (CPS, Siemens, Erlangen, Germany) imaging, with the 4C1 convex array probe. A low mechanical index (0.1–0.2) was selected. CEUS investigations were performed following administration of 2.4 mL SonoVue (Bracco, Milan, Italy). The bolus was repeated if necessary for clarification. Enhancement patterns were studied up to 3.5 min, including the arterial, portal, and late phase.
CT and US examinations were assessed by experienced abdominal radiologists that had not been involved in the inclusion of patients in the study.
The study was approved by the local ethical committee of the Karolinska Institutet (KI 2014/80-31).
Results
Patient with liver lesions (n = 74).
Liver metastases
Liver metastases were diagnosed with CT and US in 13/74 (17.6%) patients.
The number of liver metastases per patient in the study group was described in 11 of 13 patients, median 2 (range, 1–5) and mean 2.7 ± 1.4 lesions per patient. In three patients, a single metastasis was reported; in eight patients, multiple lesions were found; and in two patients, the number of lesions was not reported on CT/US.
The location of the lesions was mainly in the right liver lobe (eight patients). In five patients, there were metastases in both the right and left liver lobe.
The size of liver metastases was specified in 16 lesions on CT/US. The median and mean of the size was 15 mm (range, 5–40 mm) and 16.9 mm ± 11.1, respectively. In three lesions, the size was not mentioned or specified in the reports.
The diagnosis was confirmed with postoperative histopathology of the liver specimen after liver resection in four patients. In another four, radiofrequency ablation (RFA) with repeated intraoperative US of the lesion were performed. In five patients, multiple, non-resectable lesions were diagnosed, these patients received palliative treatment with chemotherapy and confirmation was made by clinical follow-up visits and repeated CT scans.
Benign liver lesions
All 60/74 (82.4%) patients with liver lesions that were considered benign on preoperative CT/US were confirmed to be benign with either CT/US or clinical assessment at one-year follow-up.
Among 49 of 60 patients, the preoperative CT/US assessed the benign lesions as cysts. In five of 60 patients, the lesions were described as hypoattenuating/hypoechoic benign lesions confirmed by follow-up as benign lesions and in the remaining six patients the lesions were characterized as hemangioma both by preoperative CT/US and follow-up.
The number of benign lesions found on CT/US were reported in 49 patients; the median was 1 (range, 1–4) and mean was 1.5 ± 0.7 lesions per patient. In the remaining 11 patients, the number of lesions was not specified. In 30 patients, a single benign lesion was reported; in 19 patients, multiple benign lesions were described; and in 11 patients, the number of lesions was not specified.
The location of the lesions was mainly in the right liver lobe (29 lesions) and eight lesions were in the left lobe of the liver. In seven patients, the lesions were in both the right and the left liver lobe, and in six patients, the location of the lesions was not specified in the report.
The size of lesions was described in 50 lesions, the median size was 10 mm (range, 2–70 mm) and mean 13.2 mm ± 13.8, and in 16 patients the size was not specified or given.
False positive liver metastases
In one patient, a small hypoattenuating lesion located in the right liver lobe was described at the preoperative CT but was too small to be characterized. US with contrast agent was performed the same day and showed a 7-mm lesion in segment 6 of the liver, judged as a metastasis. Surgery of the colon cancer was performed and further investigation/follow-up was carried out with CT and US after three and four months. It showed that the lesion had not increased in size during these months, therefore it was not defined as a metastasis. A further follow-up with CT after three, six, and 12 months showed that the lesion was unchanged and was finally regarded as a benign cyst.
Discussion
The results of this study show that US performed in addition to CT in case of indeterminate liver lesion is an accurate combined procedure for preoperative detection of liver metastases among patients with newly diagnosed colorectal cancer. In our study, 82.4% of the patients with indeterminate liver lesions where benign both according to preoperative CT/US and the follow-up. This proportion is in line with previous studies with ranges of 80.0–92.5% (4,7,10–12).
The definition of indeterminate liver lesion varies, making comparison with other trials difficult. The size is defined in the range of 10–20 mm or smaller and some reports did not include colorectal metastases exclusively (10,13,14).
Although none of the patients in the present study with benign lesions showed progression of the liver lesion over time, there is described a progression of small liver lesions consistent with metastases in 10.9% (4). The difficulty to characterize these lesions may lead to delay of the final stage of the disease and optimal treatment of patient.
The choice of surveillance imaging of these lesions differs in various institutes and countries. With conventional CT, hepatic lesions smaller than 10 mm can be difficult to characterize with CT alone (7). The advantage of CT is its non-invasive nature and its wide availability (15). In contrast, MRI has been shown to be superior to CT imaging in characterizing these lesions with a sensitivity to detect colorectal metastases of up to 95% compared with CT with up to 79% (16–20). There are some disadvantages with MRI as it requires more time and is more expensive. Other surveillance modalities include intraoperative ultrasound (IOUS) with a high sensitivity over 90% and it also allows perioperative identification of focal liver lesions (12,21,22). IOUS has an influence on surgical decisions in 32–51% of the patients planned for hepatic surgery (16,23,24). Beyond the advantage of detection of extrahepatic metastases, 18F-flourodeoxyglucose positron emission tomography has a reported sensitivity and specificity for colorectal liver metastases of 88% and 96%, respectively (25). However, the drawbacks of the method are lack of anatomic localization, inability to detect small indeterminate lesion, and thus it is mainly used to detect extrahepatic disease in patients with suspected liver metastases. Although all patients were not examined with contrast agents, the sensitivity and specificity was high. In the current study, in 70% (n = 52) of the patients, CEUS was used, the radiologist first examined the liver without contrast agents, and if there was an obvious lesion that could be determined, contrast agents were not used. However, CEUS/US still has limitations: it is user-dependent, and in obese patients the accuracy in some parts of the liver is limited because of reduced penetration. In the follow-up period where examinations have to be compared, long recorded video sequences from CEUS/US are more difficult to review than CT examinations (26).
There is obviously a need to identify the most effective multimodality imaging approach to manage characterization of indeterminate liver lesions in patients with colorectal cancer. In the present study, CT and US was complemented with MRI of the liver in 14 patients but showed the same result as the CT and US. MRI examination could be performed if liver metastases are suspected, to ensure that the patients are not eligible for curative treatment.
In the current study, CT and US performed in conjunction during the preoperative investigation of small liver lesions were effective in this content with a high sensitivity and specificity for these lesions of 100% (13/13) and 98.4% (60/61), respectively.
A combined limitation and also strength of the present study is that it was a retrospective single-center study, where a limited number of radiologists performed and reviewed the radiological investigations.
Another limitation of the study was that histopathological confirmation could not be obtained in all patients. A selection bias may have occurred as all elderly and patients with widespread metastases in the liver and other organs were not subjected to an additional US of the liver. Finally, the sample size of the study was small, and our results should be confirmed and further explored in a larger study to determine its clinical relevance. Although our results are promising, they cannot be considered safely generalizable to all hospitals.
In conclusion, CT with dedicated consecutive US in patients with indeterminate focal liver lesions on CT is an accurate work-up for detection of liver metastases in patients with newly diagnosed CRC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided through Knut Karlssons and Birgitta Björnsson Karlssons and Bengt Ihre Foundation.