
Abstract
Background
Positron emission tomography (PET) imaging using the radiotracers 18F-fluorodeoxyglucose (FDG) or 18F-fluorothymidine (FLT) has been proposed as imaging biomarkers of cell proliferation.
Purpose
To explore the correlations of FDG and FLT uptake with the Ki-67 labeling index in patients with lung cancer.
Material and Methods
Major databases were systematically searched for all relevant literature published in English. The correlation coefficient (rho) and its 95% confidence interval (CI) of individual studies were meta-analyzed using a random-effects model. The sources of heterogeneity were explored by subgroup analyses.
Results
Twenty-seven articles involving 1213 patients were included in this meta-analysis, comprising 22 studies for FDG uptake/Ki-67 expression correlation and eight for FLT uptake/Ki-67 expression correlation. The pooled rho values for 18F-FDG/Ki-67 correlation and 18F-FLT/Ki-67 correlation were 0.45 (95% CI, 0.41–0.50) and 0.65 (95% CI, 0.56–0.73), respectively, which indicated a moderate correlation for the former and a significant one for the latter. Although the subgroup analyses based on study design, scanner, sample method, and Ki-67 labeling method did not significantly explain the heterogeneity, these factors were potential sources of heterogeneity. In lung cancer, the pooled SUVmax of FDG uptake was significantly higher than that of FLT uptake (7.59 versus 3.86, P < 0.05). In addition, compared to FDG, FLT showed higher specificity yet lower sensitivity for the diagnosis of pulmonary lesions.
Conclusion
Both 18F-FDG and 18F-FLT correlate significantly with the Ki-67 labeling index in pulmonary lesions, and the latter, with a stronger correlation, may be more reliable for assessing tumor cell proliferation in lung cancer.
Introduction
Lung cancer continues to be the most common cause of cancer death, accounting for more than one-quarter of all cancer deaths worldwide (1). To improve the outcome of patients with lung cancer, it is crucial to choose the appropriate therapy, mainly according to the accurate classification and staging. Based on the metabolic differences of glucose between benign and malignant tumors, positron emission tomography (PET) with 2-deoxy-2-18F-fluoro-D-glucose (FDG) is a well-established functional imaging technique not only for diagnosing, staging, restaging, and determining the response to the treatment of lung cancer (2–5), but also for predicting prognosis (6,7). However, 18F-FDG is not a tumor-specific tracer and false-positive findings can occur in inflammatory lesions (8).
In contrast to FDG uptake values, the Ki-67 immunohistochemistry, a method for evaluating tumor cell proliferation, is considered to be a specific sign of malignant tumors (9). High Ki-67 expression has been reported to be associated with increased aggressiveness and invasiveness of pulmonary tumors, and tumors with better differentiation have lower Ki-67 expression (10). Many studies have been published that focused on whether FDG uptake in PET can reflect tumor cell proliferation in pulmonary lesions; however, the correlation of FDG uptake with Ki-67 expression is still controversial (11–14).
Currently, 3’-deoxy-3’-18F-fluorothymidine (FLT), a thymidine analogue, is under consideration as a stable imaging agent of tumor cell proliferation (15). The accumulation of FLT serves as an indirect measurement of cell proliferation by reflecting thymidine kinase-1 expression (TK1), which is closely associated with cellular proliferation (16). In clinical studies, 18F-FLT uptake showed a significant correlation with the cell proliferation indicated by the Ki-67 index in pulmonary nodules (17–20), although this is not always the case (21,22). In addition, the sample sizes of these studies were small.
Therefore, we performed this meta-analysis to explore and compare the correlation of 18F-FDG and 18F-FLT uptake with Ki-67 expression and to provide evidence-based references for clinical application.
Material and Methods
Literature search
The MEDLINE, EMBASE, and Cochrane Library databases were searched for eligible research articles. The search was performed with language restrictions (English) and the publication date was limited to between January 1999 and October 2015. The search strategy was based on the combination of these key words: “positron emission tomography OR PET OR positron emission tomography/computed tomography OR PET/CT OR PET-CT OR positron emission tomography-computed tomography” AND “18F-FDG OR fluorodeoxyglucose OR FDG OR 18FDG OR thymidine OR fluorothymidine OR FLT OR fluorodeoxythymidine OR deoxy-thymidine OR deoxy-l-thymidine OR 18F-FLT” AND “ki67 OR ki-67 OR Ki 67 OR mitotic index OR proliferation index OR MIB1 OR MIB-1 OR mitosis index” AND “lung cancer OR lung carcinoma.” The reference lists of included articles were manually cross-checked to identify additional eligible studies.
Selection of articles
Two reviewers independently screened the retrieved articles according to the selection criteria. The inclusion criteria were as follows: (i) investigation of the relationship between the uptake of 18F-FDG or 18F-FLT and the expression of Ki-67 in pulmonary lesions; (ii) studies focusing on patients with malignant pulmonary tumors, or studies in which the vast majority of included tumors were malignant; (iii) identification and characterization of benign or malignant lesions by cytopathology or histopathology; and (iv) if data were presented in more than one article, the article with more detail or the most recent article was chosen. Exclusion criteria included: (i) an irrelevant topic (not about FDG, FLT, Ki-67, or lung cancer); (ii) reviews, case reports, letters, meeting abstracts, and animal experiments; (iii) a sample size smaller than ten; or (iv) articles without sufficient data to obtain or calculate the correlation coefficient. In addition, articles that involved post-treatment patients were excluded because Ki-67 expression is affected by previous treatments, particularly radiotherapy (23).
Data extraction and quality assessment
The information extracted from each article included the following items: (i) overall study characteristics (first author, publication year, sample size, study design, tumor type, and identification method); (ii) technical characteristics of the PET scan and Ki-67 measurement (imaging equipment, agent dose, uptake time, uptake index, and labeling index); and (iii) correlation coefficient between 18F-FDG or 18F-FLT uptake and Ki-67 expression. To ensure that an unbiased estimate was obtained, we only analyzed and pooled the Spearman correlation coefficient (rho), which could be directly extracted in some studies. In cases where rho values were not reported, this estimate was calculated based on the raw data or scatter plot. In addition, the Pearson correlation coefficient was converted to the Spearman correlation coefficient (24). The 95% confidence intervals (CIs) were calculated by applying Fisher’s z transformation and inverse Fisher transformation.
The methodological quality of the included studies was assessed using the Quality Assessment of Diagnostic Studies 2 (QUADAS-2) tool (25), which consists of “risk of bias” and “applicability concerns.” The former includes four domains: patient selection, index test, reference standard, and flow and timing, and the first three domains are also assessed for concerns regarding applicability. Each domain was scored as “high,” “low,” or “unclear.” To ensure the application of QUADAS-2 in our analysis, the PET scan was designated as the “index test” and the Ki-67 immunohistochemistry as the “reference test.” Discrepancies on the assessments were resolved by consensus.
Data analysis
Based on the correlation coefficients obtained for the individual studies, the overall estimates were pooled. Higher values indicated stronger correlation (rho < 0.21: poor correlation; 0.21 ≤ rho < 0.41: average correlation; 0.41 ≤ rho < 0.61: moderate correlation; 0.61 ≤ rho < 0.81: significant correlation; rho ≥ 0.81: strong correlation) (26,27). The heterogeneity of the rho values between studies was determined by the I2 index (28). I2 > 50% indicated a distinct heterogeneity, which meant a random effects model was used; otherwise, a fixed effects model was used. In our analysis, we used the random effects model to pool and analyze the estimates. Sources of heterogeneity were explored by subgroup analysis according to factors such as: study design (prospective versus retrospective); Ki-67 labeling index (Ki-67max or Ki-67mean); pathology collection methods (surgery, biopsy or both); and imaging equipment (PET or PET/CT). In addition, the publication bias was evaluated by Begg’s test.
Statistical manipulation was performed with STATA software, version 12.0 (Stata Corporation, College Station, TX, USA). The level of statistical significance was set to a two-sided P value of 0.05.
Results
Literature search and study description
Fig. 1 described the study identification process in detail. Ultimately, 27 articles (Supp. refs. 1–27) were included in this meta-analysis; of these, 22 were about the relationship between FDG uptake and Ki-67 expression and eight focused on the relationship between FLT uptake and Ki-67 expression.
Flow chart of study selection (identification, screening, exclusion and inclusion).
All the included studies involved a total of 1213 patients. The majority of the included studies were prospectively designed, but eight enrolled patients respectively. For the scanning modality, 14 studies used the PET scanner alone while 11 other studies used an integrated PET/CT; one study used both. With regard to the measurement of Ki-67 expression, the majority of studies measured the highest proliferation rate (Ki-67max) in the samples, which were usually obtained by surgical resection. The detailed characteristics of the individual studies are summarized in Suppl. Tables 1 and 2.
Quality assessment by QUADAS-2
Regarding patient selection, the risk of bias was low in 25 studies, whereas only two studies had a high risk of bias, which was mainly caused by the lack of availability of patient inclusion and exclusion criteria. Twelve studies in the aspect of index test and nine in the aspect of reference standard displayed an unclear or a high risk of bias, with the common weakness concentrated in the interpretation of the index test (PET scan) results and reference standard (Ki-67 Immunohistochemistry) results not being blinded to one another. Due to a lack of information about the appropriate interval between the index test and the reference standard, the risk of bias in terms of flow and timing was high or unclear in two studies. In addition, most studies dealt with pulmonary lesions with acceptable methods (PET scan and Ki-67 immunohistochemistry), leading to a low concern for applicability with the index test and reference standard. Five studies were assigned unclear or high applicability concerns regarding patient selection because these studies included a small quantity of benign pulmonary lesions, although the majority of included patients had malignant lesions.
The results of the meta-analysis
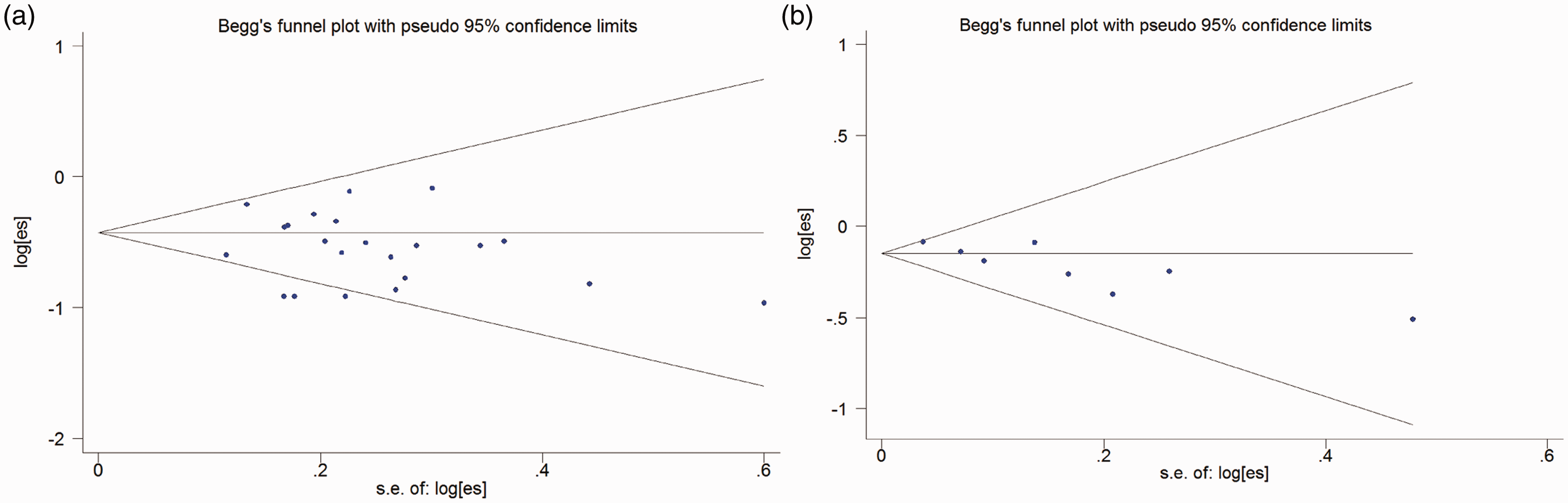
18F-FDG/Ki-67 correlation: The pooled rho for all 22 studies was 0.45 (95% CI, 0.41–0.50), which indicated a moderate correlation between FDG uptake and Ki-67 expression with notable heterogeneity (I2 = 66.2%, P < 0.001) (Fig. 2a). In addition, the results of Begg’s test (P = 0.384) indicated an absence of publication bias among the included studies (Fig. 3a).
Forest plots of the pooled correlation coefficient (rho) with corresponding 95% CIs for the correlation between 18F-FDG uptake and tumor cell proliferation (a) and for the correlation between 18F-FLT uptake and Ki-67 expression (b). The funnel plots of publication bias for FDG/Ki-67 correlation (a) and FLT/Ki-67 correlation (b). The nonsignificant slope indicates the absence of publication bias (P = 0.384 for FDG/Ki-67 correlation, P = 0.293 for FLT/Ki-67 correlation).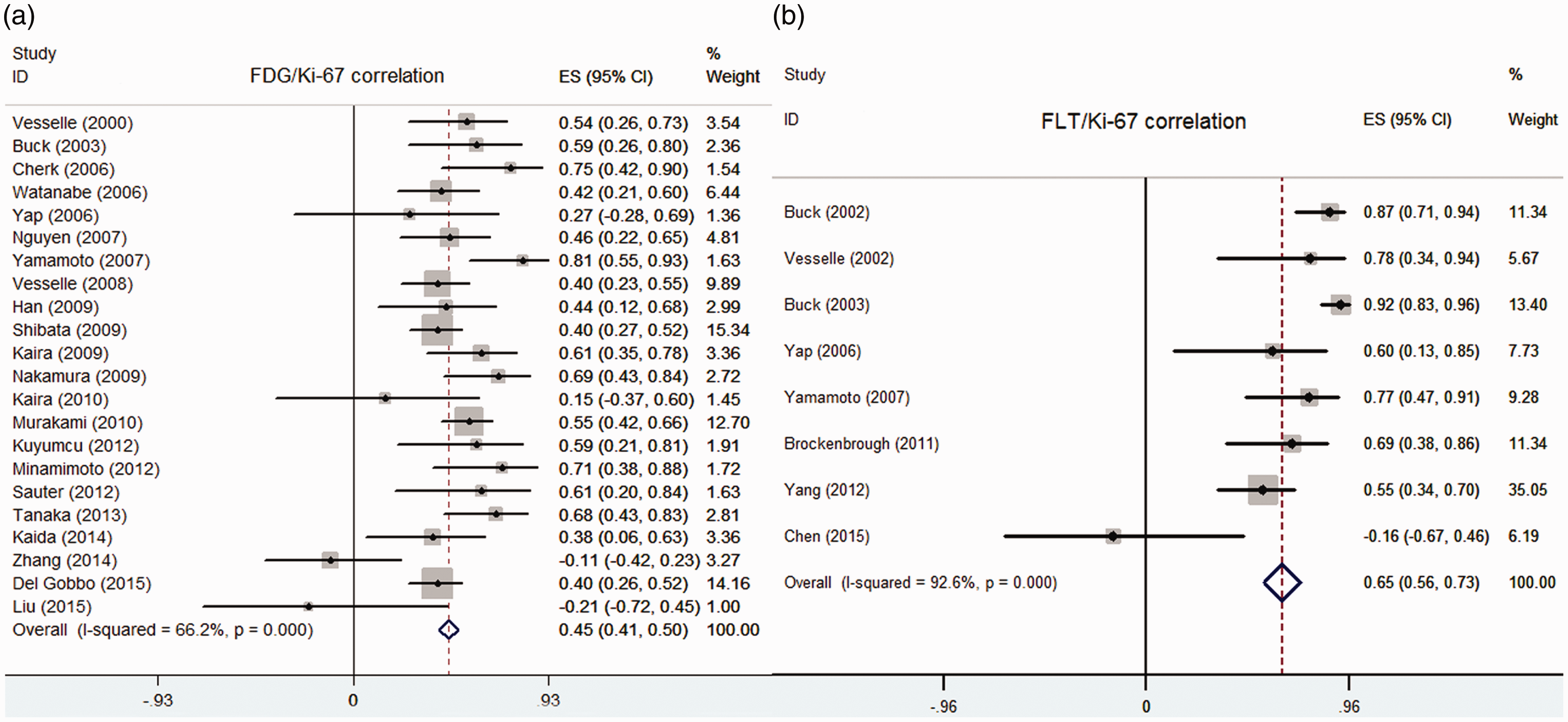
The results of the subgroup analysis are shown in Fig. 4a and Suppl. Table 3. The combined rho values based on the study design were 0.45 (95% CI, 0.39–0.51; I2 = 72.2%; P < 0.01) for prospective studies and 0.45 (95% CI, 0.38–0.53; I2 = 54.9%; P = 0.03) for retrospective studies, which still indicated heterogeneity among subgroups. The heterogeneity of some subgroups (surgery, surgery + biopsy, PET/CT, and Ki-67mean) was still relatively high, while that of other subgroups (Ki-67max and PET/CT) decreased.
Forest plots of subgroup analysis based on study design, sample method, labeling method, and scanner for FDG/Ki-67 correlation (a) and FLT/Ki-67 correlation (b).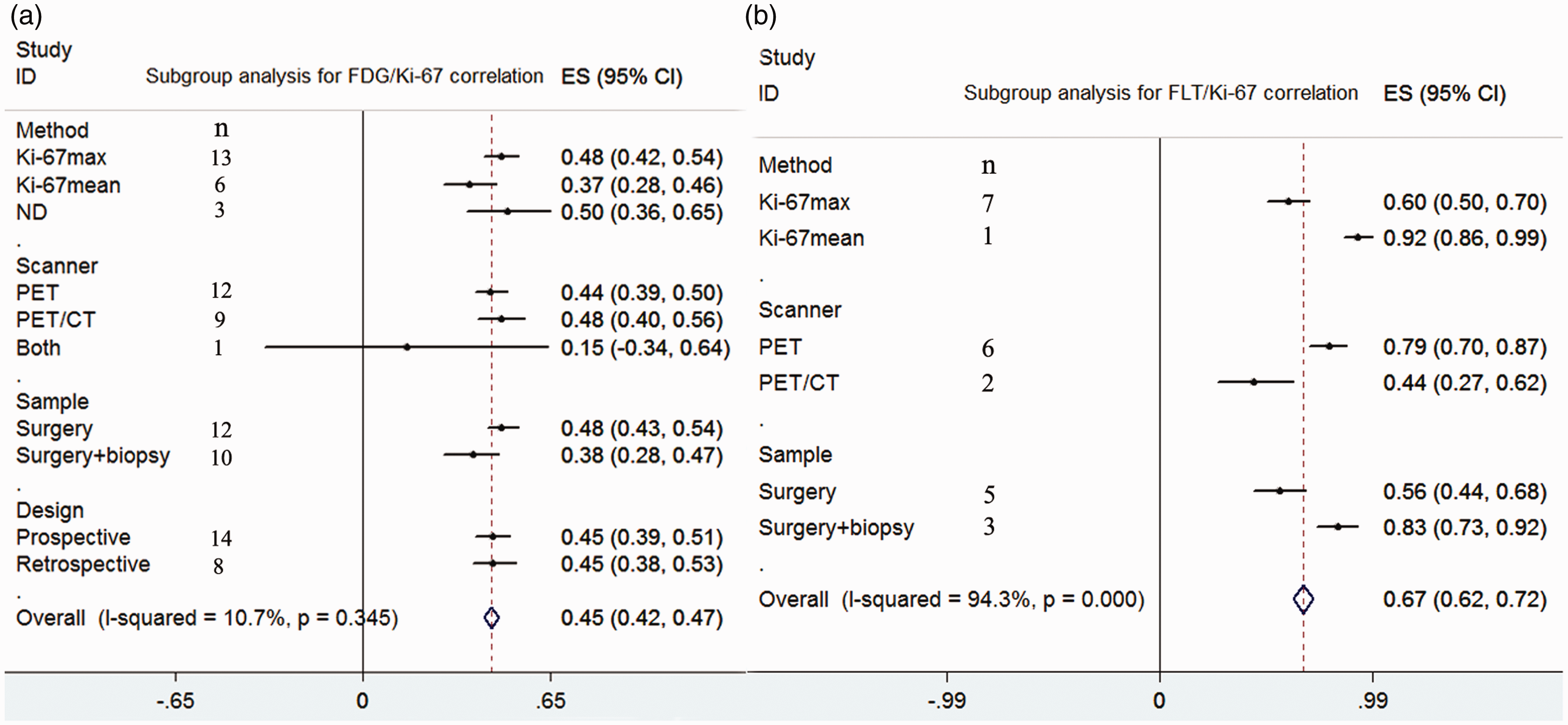
18F-FLT/Ki-67 correlation: As showed in Fig. 2b, the pooled rho for the correlation of 18F-FLT uptake with Ki-67 expression was 0.65 (95% CI, 0.56–0.73), indicating a significant level despite high heterogeneity (I2 = 92.6%, P < 0.001). In addition, the funnel plot in Fig. 3b showed no notable publication bias (P = 0.293). The results of the subgroup analysis for 18F-FLT/Ki-67 correlation are presented in Fig. 4b and Suppl. Table 3. Scanning modality and sample method might be possible causes for the heterogeneity between studies; however, the sample size of included studies was too small.
Diagnosis with FDG/FLT PET/CT: For the FDG uptake, fourteen studies yielded the pooled SUVmax of 7.59 (95% CI, 7.20–7.98), and for the FLT uptake, seven studies yielded the pooled SUVmax of 3.86 (95% CI, 3.46–4.26). FLT showed significantly lower uptake in pulmonary lesions that FDG (P < 0.05) (Fig. 5). As shown in Suppl. Table 4, the FLT PET/CT demonstrated lower sensitivity (0.79 versus 0.91) yet higher specificity (0.93 versus 0.53) for the diagnosis of pulmonary lesions, compared with FDG PET/CT.
The funnel plots of SUVmax of FDG uptake (a) and FLT uptake (b) in pulmonary lesions.
Discussion
Our results showed that there was a moderate correlation between FDG uptake and Ki-67 expression (rho = 0.45) and a significant correlation between FLT uptake and Ki-67 expression (rho = 0.64). Although both were significantly correlated with proliferative activity, the latter had greater potential as a biomarker for cell proliferation, which was in good agreement with the previous study (29).
The Ki-67 labeling index, as a marker of proliferation in malignant tumors, is currently under discussion for its prognostic and predictive value in lung cancer (30–32). However, the proliferation rate has commonly been measured in only a small, representative sample and not in the entire tumor, resulting in some drawbacks, such as sampling error and no repeat procedures (33). By contrast, PET imaging, as a non-invasive method to assess proliferation of entire tumor that can be repeated at any point during treatment, has become a focus of research (10,13,33). In clinical studies, FDG uptake has been reported to correlate with Ki-67 expression in pulmonary lesions; however, the results did not reach consensus, with rho value ranging from −0.21 to 0.87. Based on our analysis, FDG uptake only partially reflected proliferation with a low rho value of 0.45. The proliferative cells might increase tumor-specific FDG uptake for energy production, but this correlation was unspecific and indirect. In addition, FDG uptake also originates from additional mechanisms, such as the expression of glucose transporters and hexokinase (34,35).
As a more tumor-specific proliferation tracer, FLT is a thymidine analogue, and its uptake was correlated with TK1, which is the specific enzyme in the S phase of the pyrimidine salvage pathway (16). Even though the detailed uptake mechanism is still unknown, tumor tissues tend to increase FLT uptake, and the correlation between FLT uptake and cell proliferation in pulmonary lesions has been confirmed to be significant in several studies (17,20,33). However, the findings of Chen et al. ran counter to previous studies by not showing a positive correlation (rho = −0.16). As the authors reported, several factors could account for the lack of correlation, including a small number of patients and only one slice available for Ki-67 staining, which may not represent the proliferation level of the whole tumor. In our meta-analysis, the rho value for FLT/Ki-67 in pulmonary lesions was 0.64, which was higher than that for FDG/Ki-67, suggesting that 18F-FLT uptake could be used as an indicator for assessing the proliferative activity of tumor cells. Preoperative FLT uptake determination could help select which patients should receive additional therapy because lung cancer patients with a high proliferation index are at high risk of recurrence after resection (33). In addition, FLT uptake has immense potential to be a more sensitive tracer to assess the therapeutic efficacy than does the FDG index (36,37). Moreover, because FLT uptake has been reported to be a prognostic factor in lung cancer, its value for predicting patient survival needs to be evaluated further (38,39).
Although there were no significant differences between the subgroups based on the study design, Ki-67 labeling method and sample method, these factors might be possible sources of heterogeneity because of the small sample size of the included studies. It has been reported that different methods of Ki-67 proliferative index assessment obtained different results, with a discrepancy of 67% in the examined cases (40). Moreover, the proliferative activity was overestimated using the Ki-67max measurement to some degree, and results greater than the cutoff value need to be interpreted with caution (40). However, the Ki-67mean, or the average of the immunohistochemistry measurements, were more reproducible, more stable, and less affected by bias (41). In our analysis, the rho value of the Ki-67mean subgroup was lower than that of the Ki-67max subgroup for FDG/Ki-67 correlation. In clinical practice, the Ki-67 index is usually obtained by evaluating sections that are only a few micrometers thick, while the SUVmax is identified by analyzing the whole volume of the lesion. In tumors with high intratumoral heterogeneity, the concordance between section and whole tumor might be low (42). In other words, the concordance of the Ki-67 index and SUVmax, which is the spatial co-localization between Ki-67 staining and FDG/FLT uptake in the same lesion, would be underestimated (21). In addition, a potential risk of bias exists that the Ki-67 results or other clinical data might have been known before assessing PET images in a retrospective study. Other sources of heterogeneity may be present, including the technical characteristics of the PET scanning and measurements in the included studies. Indeed, the scanning machines, as well as the protocols from different companies, varied significantly. It is clear that the reviewed studies did not reach consensus on the radiopharmaceutical dose and scanning time.
For the diagnosis of pulmonary lesions, FLT PET/CT showed a higher specificity but lower sensitivity than FDG PET/CT, indicating that FLT PET/CT might help solve the false positive problems using FDG. Our findings were similar to the previous study although the sample of included studies were too small (43). Although FLT cannot replace FDG in overall cancer diagnosis due to its lower sensitivity, it has more potential values for predicting prognosis and evaluating therapy response because it shows a closer relationship with cell proliferation.
The present meta-analysis has some potential limitations. First, although the total numbers of patients and articles included in this study were large, those for the FLT/Ki-67 correlation were small, resulting in inadequate analysis and reducing the strength of the conclusion. In particular, the subgroup analysis based on tumor subtype (adenocarcinoma versus squamous cell carcinoma) was not further performed although the biological behavior of these two subtypes was significantly different. Second, we included eligible studies involving only a few benign lesions, although the majority of enrolled patients had malignant pulmonary lesions, which might have led to a selection bias. Third, the exclusion of non-English studies and unpublished articles as well as a small size of identified databases might result in incomplete retrieval, generally associated with a bias of the true effect. In addition, due to various factors, the heterogeneity of this meta-analysis was significant.
In conclusion, this present meta-analysis suggested that in pulmonary lesions, 18F-FDG uptake had a moderate correlation with the Ki-67 labeling index while 18F-FLT uptake showed a significant correlation at a higher level. 18F-FLT, used as an indicator of cell proliferation, may therefore be the superior tracer for the assessment of therapy responses and outcome prediction. However, large-sample, prospective studies are needed for further confirmation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (Grant No. 81471692).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.