
Abstract
Background
Diffusion-weighted imaging (DWI) provides useful information for the identification of benign and malignant uterine lesions. However, the use of the apparent diffusion coefficient (ADC) for histopathological grading of endometrial cancer is controversial.
Purpose
To explore the use of ADC values in differentiating the preoperative tumor grading of endometrioid adenocarcinomas and investigate the relationship between the ADC values of endometrial cancer and the histological tumor subtype.
Material and Methods
We retrospectively evaluated 98 patients with endometrial cancers, including both endometrioid adenocarcinomas (n = 80) and non-endometrioid adenocarcinomas (n = 18). All patients underwent DWI procedures and ADC values were calculated. The Kruskal–Wallis test and the independent samples Mann–Whitney U test were used to compare differences in the ADC values between different tumor grades and different histological subtypes.
Results
The mean ADC values (ADCmean) for high-grade endometrioid adenocarcinomas were significantly lower than the values for low-grade tumors (0.800 versus 0.962 × 10–3 mm2/s) (P = 0.002). However, no significant differences in ADCmean and minimum ADC values (ADCmin) were found between tumor grades (G1, G2, and G3) of endometrial cancer. Compared with endometrioid adenocarcinomas, the adenocarcinoma with squamous differentiation showed lower ADC values (mean/minimum = 0.863/0.636 versus 0.962/0.689 × 10–3 mm2/s), but the differences were not significant (Pmean = 0.074, Pmin = 0.441). Moreover, ADCmean for carcinosarcomas was significantly higher than the value for G3 non-carcinosarcoma endometrial cancers (1.047 versus 0.823 × 10–3 mm2/s) (P = 0.001).
Conclusion
The ADCmean was useful for identifying high-grade and low-grade endometrioid adenocarcinomas. Additionally, squamous differentiation may decrease ADCmean and ADCmin of endometrioid adenocarcinoma, and carcinosarcomas showed relatively high ADCmean.
Keywords
Introduction
Endometrial cancer is the most common gynecological malignancy in industrialized countries (1). The prognosis depends on several factors, including the clinical stage, depth of myometrial invasion, histological grade, cell type, lymphovascular invasion, nodal status, and patient age (1). The histological grade of the tumor is one of the most important prognostic factors because it is closely associated with lymph node metastasis and overall patient survival (2). In addition, histological grade contributes to the choice of surgical treatment plan (including whether to perform lymph node dissection) (3).
Magnetic resonance imaging (MRI) is the main method for preoperative staging of endometrial cancer because it allows accurate assessment of the depth of myometrial invasion (1). Diffusion-weighted imaging (DWI) is a technique that detects water molecule diffusion in tissues in vivo, improving the detection rate of malignant tumors and differentiating benign from malignant lesions in endometrial cancer. Different reports have shown significantly lower apparent diffusion coefficient (ADC) values for endometrial cancer (0.86–0.98 × 10–3 mm2/s) than for normal endometrium (1.53–1.65 × 10–3 mm2/s) and benign endometrial lesions (e.g. hyperplasia and polyps, 1.27–1.63 × 10–3 mm2/s) (4–8). However, the use of ADC values for histopathological grading of endometrial cancer remains controversial (3,6,8–13).
Many endometrial cancers exhibit different types of differentiation and several types of metaplasias are observed. According to the literature (14), the histological subtypes of endometrial cancer include endometrioid adenocarcinoma (including variants with squamous differentiation), mucinous carcinoma, serous carcinoma, clear cell carcinoma, mixed carcinoma, squamous cell carcinoma, and undifferentiated carcinoma. Among these categories, endometrioid adenocarcinoma is the most common (approximately 80%) (15). Different histological subtypes present various organizational structures and differences in ADC values may occur. Our hypothesis was that because previous studies have treated the different histological subtypes of endometrial cancer as a single group and the numbers of cases were different, differences between different histological grades could not be distinguished, which may be the main reason for the current controversy. The aim of this study was therefore to assess the correlation between ADC values and tumor histological subtypes in patients with endometrial cancer.
Material and Methods
Patient selection
This retrospective study was performed at a single institution from September 2012 to January 2016 and included 98 consecutively enrolled patients with histologically proven endometrial cancer. All patients received MR examinations before surgery and underwent total hysterectomy within two weeks. The patients’ mean age was 52 years (range = 24–74 years). The exclusion criteria were: (i) no total hysterectomy performed within two weeks after the MRI examination; (ii) preoperative treatment with chemoradiation; (iii) tumors that were too small to be visible on the MRI; (iv) images with obvious motion artifacts; and (v) contraindications for MRI examination. The study was approved by the local institutional ethics committee on human research of the Shaanxi Provincial Tumor Hospital; IRB number 2012-018.
Surgical procedures were performed by two surgeons with >20 years of experience in the field and the clinical pathological assessment was completed by a pathologist with more than ten years of experience. The tumor grade (G1 = well differentiated; G2 = moderately differentiated; and G3 = poorly differentiated) was established in the endometrial cancer group and a similar histological classification method was used in the endometrioid adenocarcinoma group. Then, the endometrioid adenocarcinomas were divided into two groups: high grade (G3) and low grade (G1 and G2). In addition, endometrial cancers were divided into two histological subtypes: endometrioid adenocarcinoma and non-endometrioid adenocarcinoma. Squamous differentiation is a variant of endometrioid adenocarcinoma, which may have an impact on the ADC values of endometrioid adenocarcinoma. Therefore, endometrioid adenocarcinomas were divided into two groups according to the occurrence of squamous differentiation. Finally, G3 endometrial cancers were divided into two groups: carcinosarcomas and non-carcinosarcomas.
MR protocol
All of the MRI examinations were performed using a 1.5-T system (EXCELART Vantage™ powered by Atlas, Toshiba Medical Systems Corporation, Tochigi, Japan) with an eight-channel phased-array coil. Routine pelvic MR images were acquired using the following sequences: axial T1-weighted (T1W) imaging; axial and coronal T2-weighted (T2W) imaging; oblique sagittal T2W imaging; and oblique axial fat suppression T2W imaging.
Axial echo-planar DWI was obtained using the following parameters: repetition time (TR)/echo time (TE)/inversion time (TI) = 6900/80/150 ms; b factors = 0 and 650 s/mm2; matrix = 128 × 128; field of view (FOV) 40 × 40 cm; section thickness/intersection gap = 5/1.5 mm; speeder flag = 2; number of excitations (NEX) = 4. ADC maps were automatically reconstructed on a post-processing workstation.
Image analysis
Each patient was independently evaluated by two radiologists with more than six years of experience in diagnosing images of gynecological tumors. In addition to the postoperative histopathological findings of endometrial cancer, other data were treated with the corresponding information and methods blinded, including the location, pathological stage and histological grade of the tumor, and lymph node metastasis.
In DWI, endometrial cancer exhibits significantly higher signal intensity than the surrounding background. For each patient, a region of interest (ROI) was manually selected in the slice containing the largest tumor cross-section. The ROI was as large as possible to include the tumor and avoid contamination with normal tissue. Necrotic areas were excluded from the ROIs based on the T1W imaging, T2W imaging, and fat suppression T2W imaging.
Statistical analysis
Statistical analyses were performed with SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). The ADC values of endometrial cancer were indicated as
Results
Histopathological findings
ADC values of endometrial cancer in 98 consecutive patients.
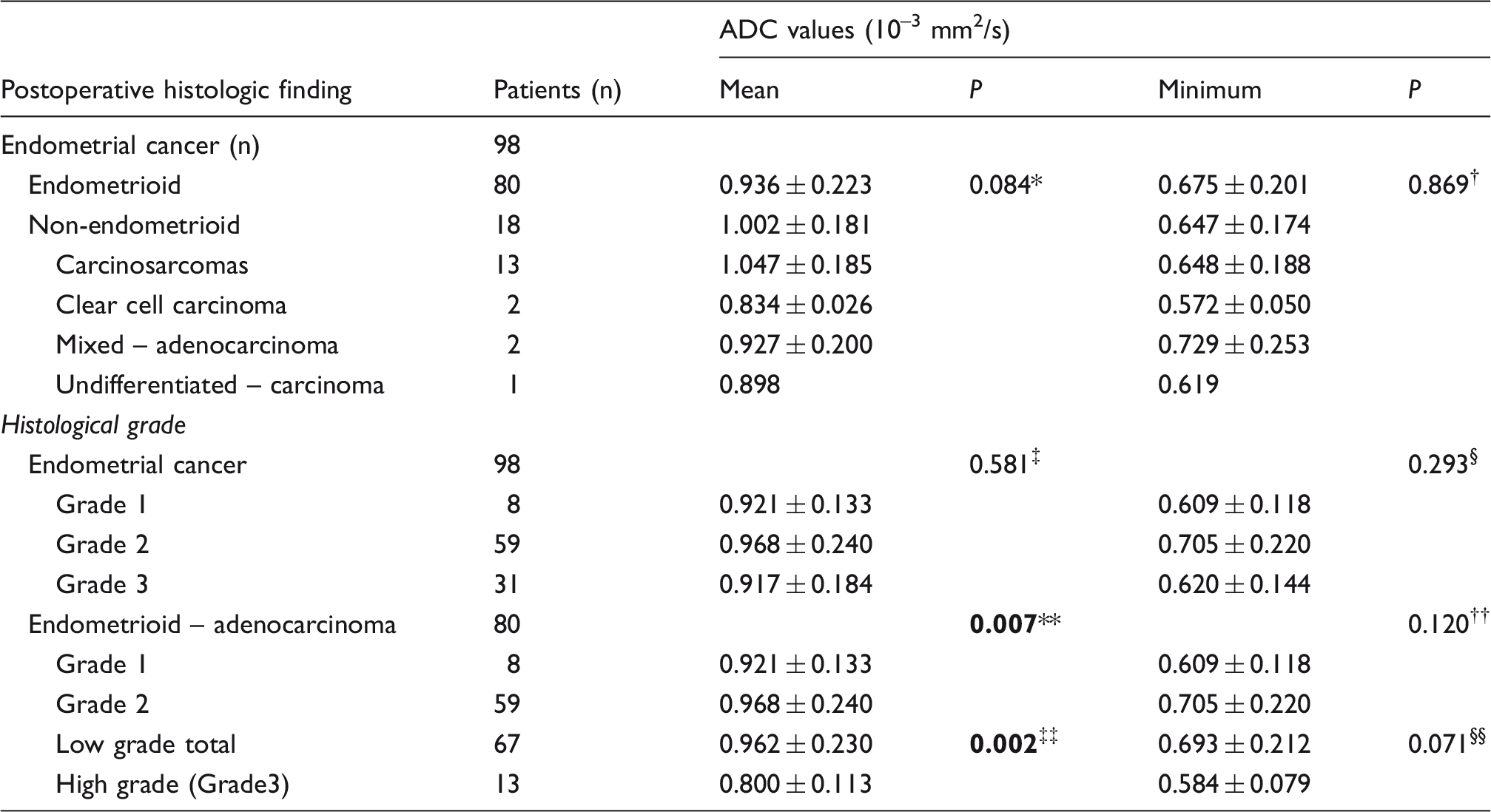
,†P values of the Mann–Whitney U test between endometrioid and non-endometrioid adenocarcinomas.
P values of the Kruskal–Wallis test in endometrial cancer.
P values of the Kruskal–Wallis test in endometrioid adenocarcinoma.
P value of the Mann–Whitney U test between high-grade and low-grade endometrioid adenocarcinoma.
G1, well differentiated; G2, moderately differentiated; G3, poorly differentiated; low grade, G1 and G2; high grade, G3.
Reader agreement
Inter-observer variability in measurements of ADC values by two observers.

CI, confidence interval; ICC, intra-class correlation.
MRI findings
There were no disagreements between the two radiologists in the evaluation of the MRI findings, including the DW images. The results are shown in Table 1 and Fig. 1. No disagreements were revealed in the ADC measurements (Table 2).
A 60-year-old woman with histopathologically proven Grade 2 (G2) endometrioid adenocarcinoma with squamous differentiation (deep-myometrial invasion). The tumor is hyperintense relative to the surrounding normal myometrium in T2W and fat suppression T2W images (a, c) and isointense relative to the myometrium in the T1W image (b). On DWI (d), the tumor is brightly hyperintense compared to the myometrium, and the tumor is hypointense on the ADC map (e). The mean and minimum tumor ADC values were 0.869 × 10−3 mm2/s and 0.492 × 10−3 mm2/s, respectively. The histological slice (f) reveals moderately differentiated endometrioid adenocarcinoma with squamous differentiation (hematoxylin-eosin (H&E) stain; original magnification = × 40).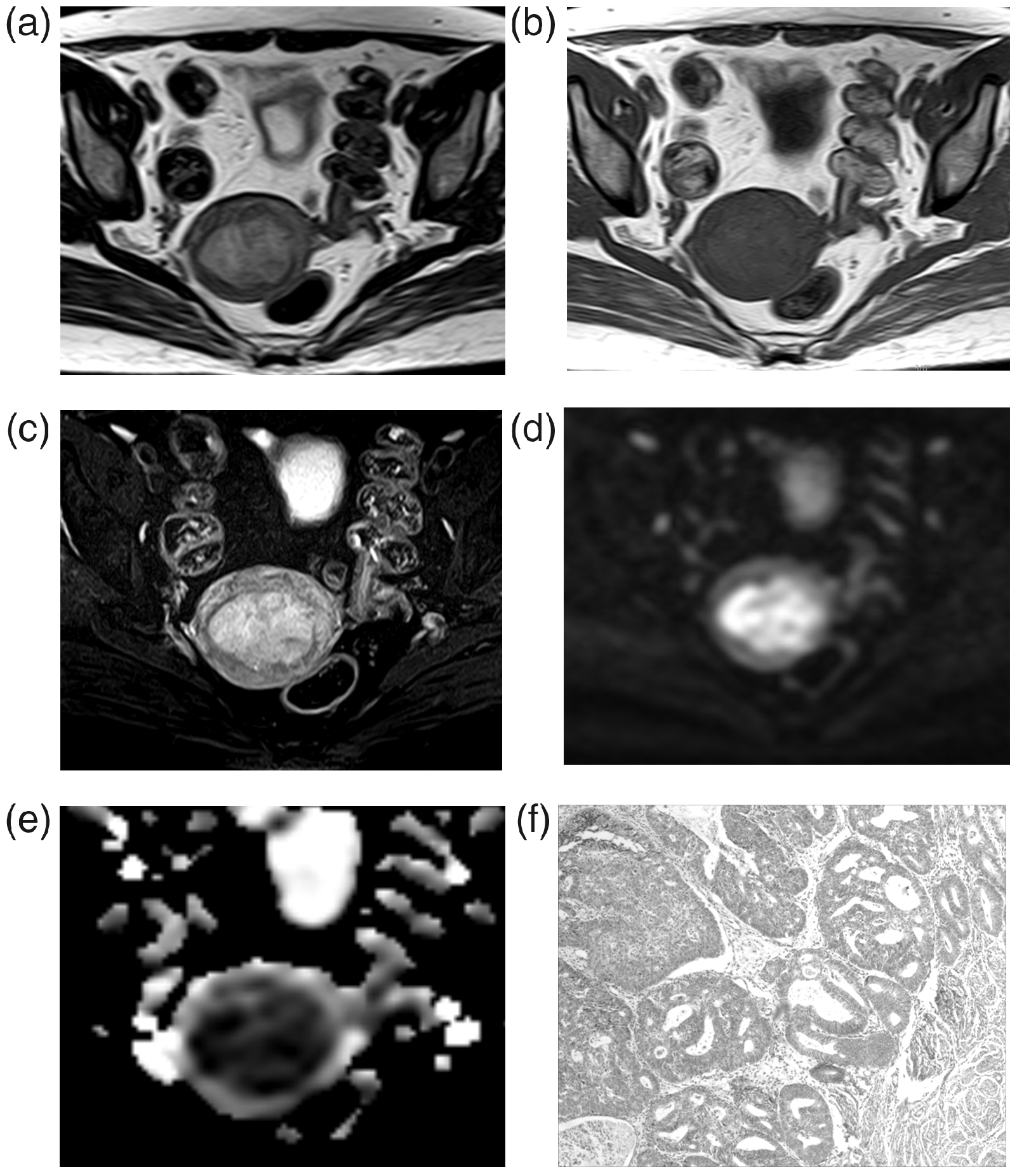
The ADCmean and ADCmin for different histological grades are presented in Table 1. For the endometrial cancer group, no significant differences in ADC values were observed among different tumor grades (Pmean = 0.581, Pmin = 0.293, Fig. 2a and 2b).
The mean (a, c) and minimum (b, d) ADC values for different histological grades of endometrial cancer and endometrioid adenocarcinoma according to the Mann–Whitney U test. ▴, ▴▴, and ▴▴▴ indicate P values for the comparisons of the ADC values of Grade 1 (G1) and Grade 2 (G2), G2 and Grade 3 (G3), and G1 and G3 tumors, respectively.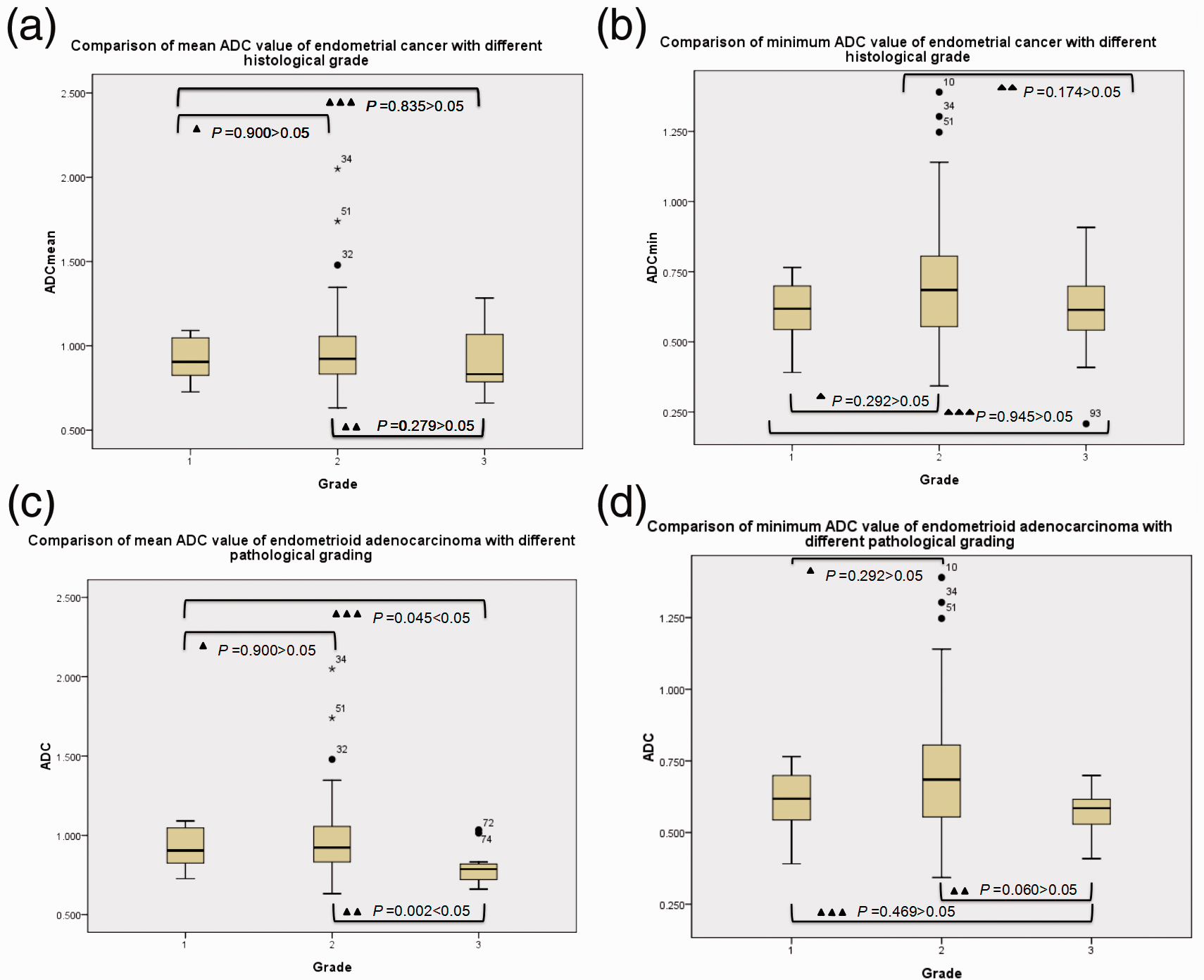
In the endometrioid adenocarcinoma group, significant differences in ADCmean were observed between the different grades of tumors (P = 0.007), whereas no significant difference was observed in ADCmin (P = 0.120). The difference between low-grade and high-grade tumors was significant (P = 0.002) for ADCmean but not significant (P = 0.071) for ADCmin (Table 1 and Fig. 2c and 2d).
The AUC of ADCmean was 0.777 (Fig. 3), indicating that ADCmean was an effective tool for distinguishing high-grade and low-grade endometrioid adenocarcinomas. According to the ROC curve analysis, 0.835 × 10–3 mm2/s was the optimal cutoff value. The corresponding sensitivity, specificity, and accuracy were 84.6%, 74.6%, and 76.3%, respectively.
ROC curves for the ADC to distinguish high-grade and low-grade endometrioid adenocarcinomas. The area under the curve (AUC) was 0.777 (95% confidence interval = 0.639–0.914; P = 0.002).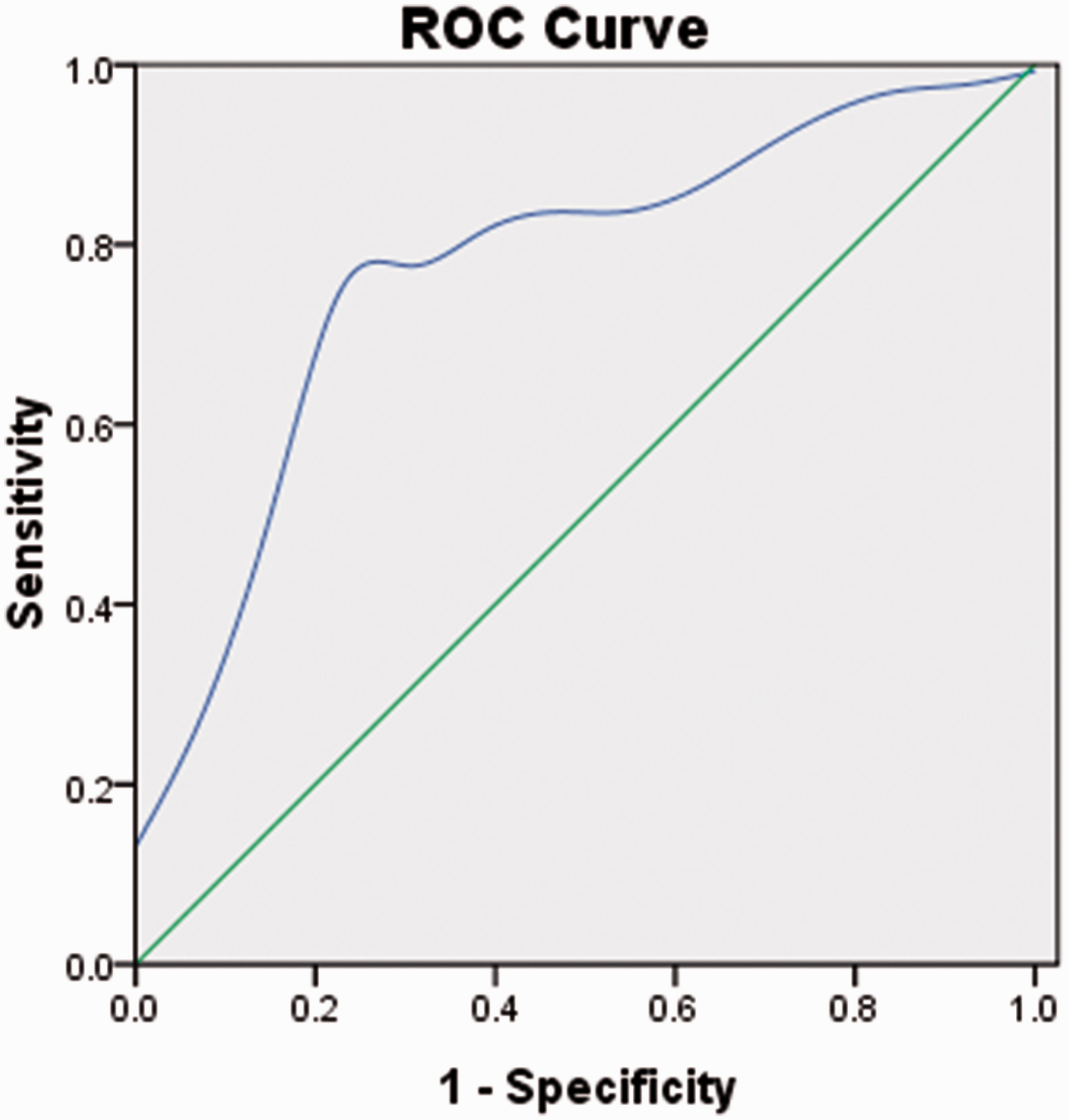
Significant differences in ADCmean and ADCmin were not observed between endometrioid adenocarcinoma ([0.962 ± 0.242] and [0.689 ± 0.216] × 10−3 mm2/s, n = 59) and endometrioid squamous differentiation ([0.863 ± 0.136] and [0.636 ± 0.148] × 10−3 mm2/s, n = 21) (Pmean = 0.074, Pmin = 0.441). However, ADCmean and ADCmin for endometrioid adenocarcinoma were higher than the values for endometrioid squamous differentiation. Furthermore, the proportion of squamous differentiation in the high-grade group (5/13, 38%) was higher than the proportion in the low-grade endometrioid adenocarcinoma group (16/67, 24%), but no significant difference was observed between the two groups (P = 0.310).
Compared with G3 non-carcinosarcoma endometrial carcinomas, the carcinosarcomas (Fig. 4) exhibited a higher ADCmean (1.047 versus 0.823 × 10–3 mm2/s, P = 0.001). However, no significant difference in ADCmin was observed (P = 0.155). Additionally, compared with endometrioid adenocarcinoma, non-endometrioid adenocarcinomas displayed higher ADCmean and ADCmin (Table 1), but significant differences were not observed (Pmean = 0.084, Pmin = 0.869).
A 66-year-old woman with histopathologically proven carcinosarcoma (Grade 3; deep-myometrial invasion). Sagittal and axial T2W images (a, b) reveal a large endometrial mass of heterogeneous high intensity expanding in the endometrial cavity. The mass (c, d) shows heterogeneous high signal intensity on DWI, and intra-tumoral heterogeneity of the mass is observed on the ADC map. In this patient, the mean and minimum tumor ADC values were 1.135 × 10−3 mm2/s and 0.702 × 10−3 mm2/s, respectively. Adenocarcinoma of the uterine endometrium in carcinosarcoma (e); the cells are arranged in an adenoid with necrosis (H&E stain; original magnification = × 100). High-grade sarcoma in carcinosarcoma (f); the spindle cells are arranged in a diffuse pattern with significant cell atypia, mitotic figures are easily found, and the epithelial and mesenchymal elements do not merge (H&E stain; original magnification = × 100).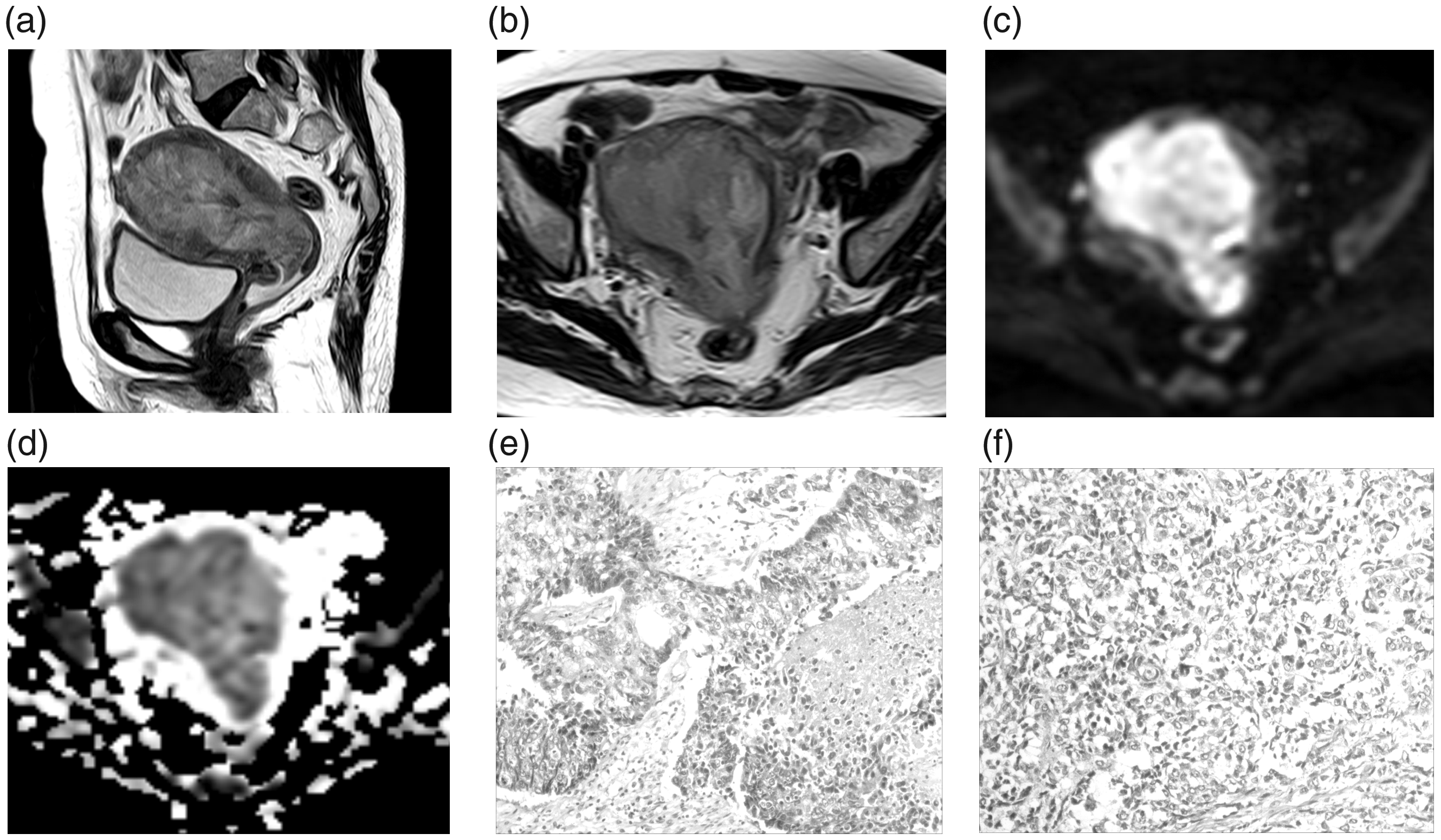
Discussion
In this study, we aimed to explore the use of ADC values in differentiating preoperative tumor grading of endometrioid adenocarcinoma and distinguishing the histological subtype of endometrial cancer. We found that the ADCmean plays an important role in differentiating high-grade from low-grade endometrioid adenocarcinoma, as well as the histological subtype of endometrial cancer (e.g. carcinosarcomas and adenocarcinoma with squamous differentiation, which may influence the ADC value).
ADCmean provided useful and reliable information for predicting the histological grade of tumors. The values of high-grade endometrioid adenocarcinoma were significantly lower than those for low-grade tumors. In our series, the sensitivity, specificity, and accuracy were 84.6%, 74.6%, and 76.3%, respectively, for a cutoff value of 0.835 × 10–3 mm2/s. Some possible explanations for these findings are discussed. First, the ADC value may reflect microstructural features of the tissue, including the nuclear-to-cytoplasmic ratio and cellular density (12), which may affect internal water molecule diffusion. Specifically, cellular density is one of the most important factors determining tumor grade (12). Additionally, differences in the proportion of the glandular cavity are observed between different histological grades of endometrial cancer, which may lead to differences in the ADC values. According to the International Federation of Gynecology and Obstetrics (FIGO) grading system, when endometrial cancer cells are transformed into solid sheets of cells from a glandular or papillary pattern, the tumor is considered to be poorly differentiated (15). Therefore, lower-grade tumors exhibit smaller solid areas and larger glandular or papillary areas, leading to higher ADC values; in contrast, high-grade tumors present lower ADC values. Liu et al. (16) investigated 98 cases with different histopathological grades of uterine cervical cancer using DWI and observed significant inverse correlations between the ADC values (mean and minimum) and the histopathological grades of the tumors, i.e. the higher the tumor grade, the lower the ADC value.
Currently, the use of ADC values to identify endometrial cancer grade is controversial. In the initial report by Tamai et al. (6), the ADC values were employed to differentiate between endometrial cancer and normal endometrium and were helpful in differentiating between high-grade and low-grade endometrial cancer. Similar reports have been published. According to Nakamura et al. (9), ADCmin for G1 tumors is higher than that for G3 endometrioid adenocarcinoma (P < 0.05). In a study by Seo et al. (10), ADCmean for G1 tumors was higher than those for G2 and G3 endometrial cancer (P < 0.001). In a recent study by Nougaret et al., in which ROIs were selected based on whole-tumor volumes (11), the minimum, 10th, 25th, 50th, 75th, and 90th percentile ADC values were significantly lower for G3 tumors than for G1 and G2 tumors. However, the controversy persists. According to Kishimoto et al. (12) and Bharwani et al. (8), ADCmean and ADCmin are not useful in differentiating histological grades. In our study, ADCmean was only correlated with the histological tumor grade in endometrioid adenocarcinoma. If the tumors were not stratified by different subtypes, we expect that the opposite results would be obtained. The ADCmean and ADCmin were not useful in differentiating the histological tumor grade of endometrial cancer. A possible reason for this finding is that the ADC values differ between different histological subtypes of endometrial cancer. According to the histopathological grading, some special histological types (such as serous carcinoma, clear cell carcinoma, undifferentiated carcinoma, and carcinosarcoma) are classified as G3 tumors (15). Thirty-one histological G3 tumor cases were included in the present study, and non-endometrioid adenocarcinomas accounted for 58% (18/31) of these cases, among which carcinosarcomas predominated (13/18). Compared with G3 non-carcinosarcoma endometrial cancers, carcinosarcomas exhibited a higher ADCmean (P = 0.001). According to Takeuchi et al. (17), ADCmean of carcinosarcomas is higher than ADCmean of high-grade (G2 and G3) endometrioid adenocarcinomas. The highly malignant nature of carcinosarcomas is due to intra-tumoral heterogeneity, with necrosis and epithelial cystic components. Thus, if these characteristics are not distinguished, ADCmean of G3 endometrial cancer will be increased. We suggest that differences in the microstructures of different subtypes might be responsible for the contradictory conclusions regarding the ADC values of endometrial cancer.
Compared with endometrioid adenocarcinoma, the variant of adenocarcinoma with squamous differentiation displayed lower ADCmean and ADCmin, but no significant differences were observed. The ADC values for squamous cell carcinoma are significantly lower than those for adenocarcinomas in patients with lung cancer and uterine cervical cancer, according to series studies (18,19). This finding may be due to increased glandular content in adenocarcinomas compared with squamous cell carcinomas (19). However, the utility of ADC values in differentiating between endometrioid adenocarcinoma and the variant has not been well demonstrated in the literature. Histologically, endometrioid adenocarcinoma is relatively similar to endometrial hyperplasia and poorly differentiated lesions display fewer formed glands, exhibiting cribriform and solid areas (14). Additionally, approximately 25–50% of endometrioid adenocarcinoma exhibits squamous differentiation (14). In our results, 25%, 23%, and 38% of the endometrioid adenocarcinomas exhibiting squamous differentiation were categorized as G1, G2, and G3, respectively, and the percentage of high-grade endometrioid adenocarcinomas exhibiting squamous differentiation was increased compared with the low-grade group. However, no significant difference was observed. We speculate that squamous differentiation would increase the solid component of endometrioid adenocarcinomas, which may lead to a decrease in the extracellular space and in ADC values. However, the FIGO histological grading of endometrial cancer suggests that the squamous epithelium should not be considered solid glandular epithelium when grading the tumor (14). Thus, squamous differentiation may have an effect on the ADC value of endometrioid adenocarcinoma, but it is not associated with tumor grade.
Significant differences in ADCmean and ADCmin were not observed between endometrioid (0.943/0.675 × 10−3 mm2/s) and non-endometrioid (1.002/0.647 × 10−3 mm2/s) adenocarcinomas. Husby et al. (20) compared ADCmean in 100 cases of endometrioid (0.80 × 10−3 mm2/s) and non-endometrioid adenocarcinomas (0.83 × 10−3 mm2/s) and did not detect a significant difference (P = 0.467). Our results agreed with these findings. Our samples were similar to the samples in the previous study (endometrioid adenocarcinoma, n = 31 in Husby et al. and n = 80 in our study; non-endometrioid adenocarcinoma, n = 18 in both studies). Our ADC values for endometrioid and non-endometrioid adenocarcinomas were slightly higher than the values reported by Husby et al. (20), possibly due to the higher b value (650 versus 1000 s/mm2).
The ADCmin did not contribute to the grading of endometrioid adenocarcinomas or the identification of endometrial cancer histological subtypes. In theory, ADCmin is closely related to the cellular density of the tumor and the value decreases with an increase in tumor grading (3). However, ADCmin is affected by many other factors in addition to cellular density, such as tumor perfusion, the extracellular space compared to the normal tissue, the state of the stroma, and contamination by noise in DWI (12).
This study has several limitations. First, the study population was relatively small. Specifically, the number of histological subtypes of endometrial cancer, except endometrioid adenocarcinoma, was small. However, these histological subtypes of endometrial cancer show a low incidence. Thus, our conclusions were limited regarding the use of ADCmean to differentiate tumor grades in every subtype group, with the exception of endometrioid adenocarcinoma; more cases are needed to increase the statistical power Second, in this study, we did not establish a control group, such as a healthy population or patients with benign endometrial lesions. However, the purpose of our study was not to differentiate endometrial carcinoma from benign endometrial lesions using ADC values, which has been reported in previous studies.
In conclusion, ADCmean was useful for differentiating high-grade from low-grade endometrioid adenocarcinomas. Moreover, compared with G3 non-carcinosarcoma endometrial cancer, carcinosarcomas displayed higher ADCmean. Hence, we recommend that the distinction between different histological subtypes be considered when using the ADC value to predict the histological grade of endometrial cancer.
Footnotes
Author Contributions
Bin Yan (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Research Funds for the Central Universities of China (1191320118).