
Abstract
Background
Supplemental breast ultrasonography (US) has been used as a surveillance imaging method in women with personal history of breast cancer (PHBC). However, there have been limited data regarding diagnostic performances.
Purpose
To evaluate diagnostic performances of supplemental breast US screening for women with PHBC and to compare with those for women without PHBC.
Material and Methods
Between 2011 and 2012, 12,230 supplemental US exams were performed in 12,230 women with negative mammograms: 6584 women with PHBC and 5646 women without PHBC. Cancer detection rate, interval cancer rate, abnormal interpretation rate, positive predictive values (PPVs), sensitivity, and specificity were calculated and compared.
Results
Overall cancer detection rate and first-year interval cancer rate were 1.80/1000 exams and 0.91/1000 negative exams, both of which were higher in women with PHBC than in women without PHBC (2.88 vs. 0.53 per 1000, P = 0.003; 1.50 vs. 0.20 per 1000, P = 0.027). Abnormal interpretation rate was lower in the women with PHBC than in women without PHBC (9.1% vs. 12.1%, P < 0.001). Sensitivity was not different (67.9% vs. 75.0%, P = 1.000), whereas specificity and PPV3 were higher in women with PHBC than in women without PHBC (91.2% vs. 88.0%, P < 0.001; 22.6% vs. 3.1%, P < 0.001). The majority of detected cancers in women with PHBC (78.9%, 15/19) were stage 0 or 1.
Conclusion
Supplemental breast US screening increases early stage second breast cancers with high specificity and PPV3 in women with PHBC, however, high interval cancer rate in younger women with PHBC should be noted.
Introduction
Women with personal history of breast cancer (PHBC) have increased risk for development of second breast cancers at an incidence of 0.5–1% per year (1–3). As earlier detection of a second breast cancer after treatment might improve survival benefit (4), annual mammography and clinical surveillance after treatment are recommended for women with PHBC by the American Society of Clinical Oncology and National Comprehensive Cancer Network (5,6). However, as mammography surveillance has shown relatively lower sensitivity and higher interval cancer rate in women after breast cancer treatment (7), supplemental magnetic resonance imaging (MRI) screening (8–10) or breast ultrasonography (US) screening (11,12) has been increasingly used despite limited data regarding its accuracy.
Supplemental breast US screening is now recommended for high-risk women ineligible for MRI screening or for whom MRI is inaccessible, and is also considered for women with dense breasts regardless of the risk as it can increase node-negative invasive cancer detection rates (13–15). However, concerns remain over the higher abnormal interpretation rate (20% versus 10%) and lower positive predictive value of findings biopsied (PPV3) (6–8% versus 25–35%) compared with those at mammography (16). In addition, for women with PHBC, there have been few studies regarding standard outcome measures including cancer detection rate, interval cancer rate, sensitivity, and specificity, which are necessary to establish clinical practice guideline.
At our institution, supplemental breast US screening has been used as part of imaging surveillance modality for women with PHBC or women with mammographically non-fatty breasts in the last decade. As a result, we were able to retrospectively collect data and evaluate performance outcomes of supplemental breast US screening in women with PHBC according to the patient age or mammographic density.
Therefore, the purpose of our study was to evaluate diagnostic performances of supplemental breast ultrasonography (US) screening for women with PHBC and to compare those for women without PHBC.
Material and Methods
Study population
Characteristics of women with PHBC and women without PHBC.
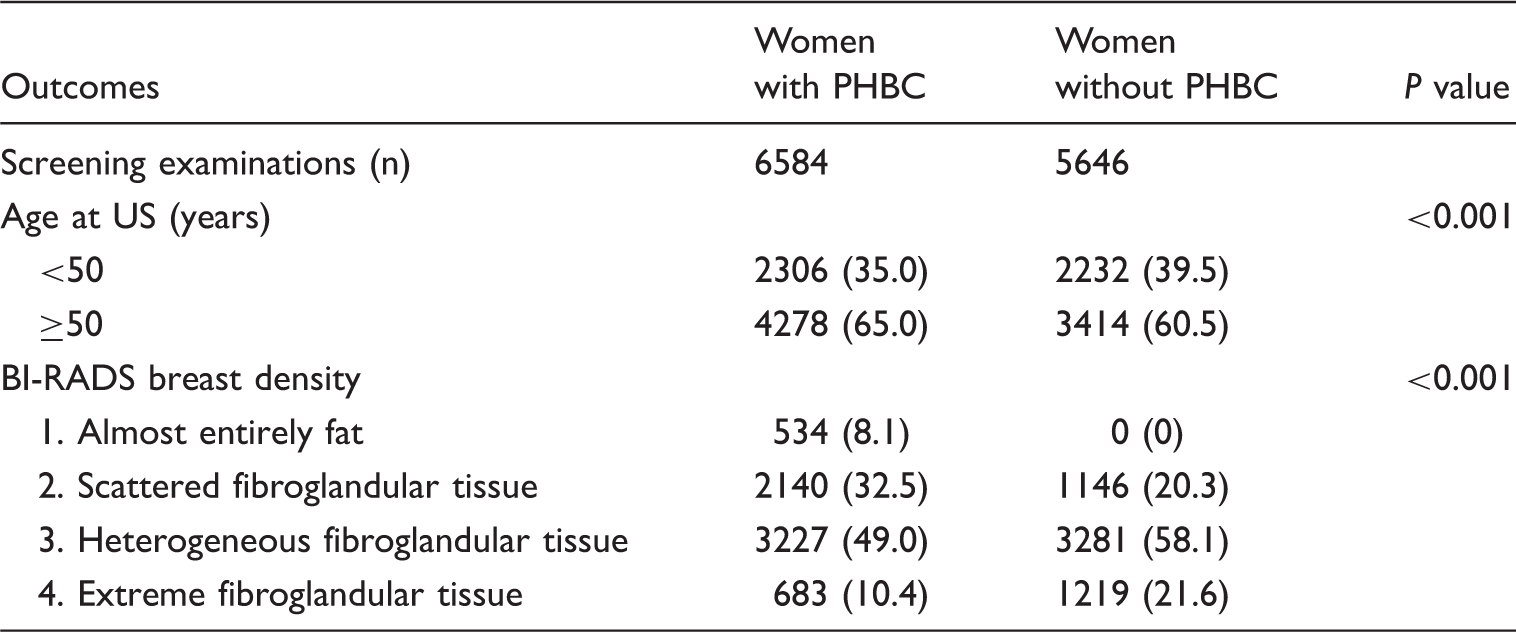
PHBC, personal history of breast cancer.
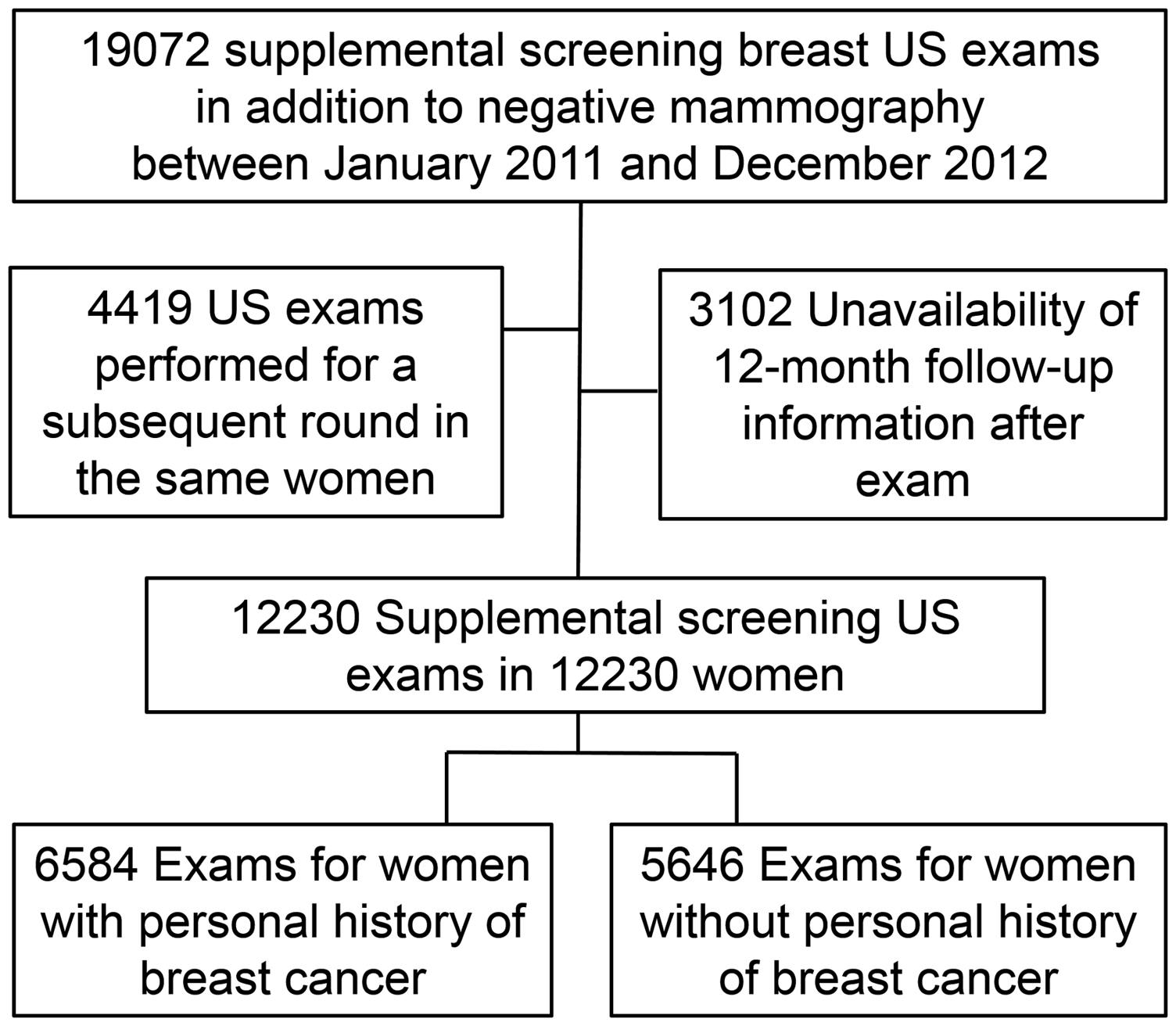
Inclusion criteria of the study population.
Supplemental breast US screening
Supplemental breast US screening examinations have been performed since 2003 for women with PHBC or women with non-fatty breasts on mammography. Mammography was performed using one of two dedicated digital mammography units (LORAD Selenia [Hologic, Bedford, MA, USA] or Senographe 2000D [GE Healthcare, Milwaukee, WI, USA]). Each US examination room was equipped with a 5-Mp (2560 × 2048 pixels) liquid crystal display system (ME511 L; Totoku Electric, Tokyo, Japan) and a picture archiving and communication system (PACS) workstation. Immediately after mammographic image acquisition and just prior to each US examination, one of ten breast radiologists (2–20 years of experience in breast imaging interpretation) reviewed their present and previous mammograms as well as previous US images using a PACS and then performed bilateral whole breast US examinations. Mammographic density was prospectively recorded based on the BI-RADS 4th edition in this period (17): grade 1 (<25% glandular); grade 2 (25–50% glandular); grade 3 (51–75% glandular); and grade 4 (> 75% glandular). The radiologist then performed bilateral whole breast US examinations using one of high-resolution US machines including EUB-8500 (Hitachi Medical Systems America, Twinsburg, OH, USA) with a 40-mm L14-6 MHz transducer, iU22 (Philips Medical Systems, Bothell, WA, USA) with a 50-mm L12-5 MHz transducer, or Aixplorer (SuperSonic Imagine, Aix en Provence, France) with a 50-mm SL15-4 MHz transducer. Final assessment categories were assigned for US examinations based on the most suspicious finding according to the BI-RADS Atlas: category 1 = negative findings; category 2 = benign findings; category 3 = probably benign findings; category 4 = findings suspicious for malignancy; and category 5 = findings highly suggestive of malignancy (18). A category 2 assessment was assigned for the presence of one or more simple cysts, intramammary lymph nodes, and nodules with uniform hyperechogenicity (18,19), and routine 12-month follow-up was recommended (18). Category 3 assessment was assigned for solid masses showing an oval shape, a circumscribed margin, and parallel orientation without any suspicious features (20), and six-, 12-, and 24-month follow-up was recommended (18). Category 4 or 5 assessment was assigned for masses with any suspicious features such as an indistinct margin, irregular shape, or a non-parallel orientation, and biopsy was recommended.
Outcome measurements
The cancer detection rate, interval cancer rate, abnormal interpretation rate, positive predictive values (PPV1, PPV2, or PPV3), sensitivity, specificity, and characteristics of the detected cancers, percentage of node-negative cancers, percentage of minimal cancers, percentage of stage 0 or 1 cancers were calculated based on BI-RADS Atlas (21). The cancer detection rate was defined as the number of detected cancers per 1000 screening examinations. Negative examinations were defined as examinations with final assessment category of 1 or 2. Positive examinations were defined as examinations with final assessment category of 3, 4, or 5. Interval cancer was defined as a breast cancer diagnosed after the last negative screening examination but before the next scheduled screening examination (less than 12 months) due to clinical symptoms or abnormalities on other images. The interval cancer rate was calculated as the number of interval cancers per 1000 negative examinations (22). The abnormal interpretation rate was defined as the percentage of positive examinations of final assessment categories 3, 4, or 5 (21). PPV1 was calculated as the number of detected cancers per positive examinations, PPV2 as the number of detected cancers per examinations with recommendation for tissue diagnosis (BI-RADS category 4 or 5), and PPV3 as the number of detected cancers per examinations with biopsy performed (21). Sensitivity was calculated as the number of positive examinations for which there was a tissue diagnosis of cancer within one year of examination, divided by all cancers present in the population examined in the same period (21). Specificity was calculated as the number of negative examinations for which there was no tissue diagnosis of cancer within one year of examination, divided by all examinations for which there was no tissue diagnosis of cancer within the same period (21). Minimal cancer was defined as invasive cancers ≤ 1 cm or ductal carcinoma in situ of any size (21).
Statistical analysis
For women with PHBC, age was dichotomized into the women aged < 50 years versus women aged ≥ 50 years. Mammographic density was dichotomized into dense (mammographic density grades of 3–4) and fatty (mammographic density grades of 1–2) breasts. To compare the diagnostic performance parameters and median size of invasive cancers of screening examinations according to the presence of PHBC and age groups, Fisher’s exact test or Mann–Whitney U test were used. Clinicopathologic features of screening detected cancers and interval cancers were compared using Fisher’s exact test. Statistical Package for the Social Sciences (SPSS, version 20; IBM, Armonk, NY, USA) software was used for all statistical analyses, and two-tailed P values of < 0.05 were considered indicative of a statistically significant difference.
Results
Outcomes according to the presence of PHBC
Outcomes of supplemental breast US screening according to the presence of PHBC.
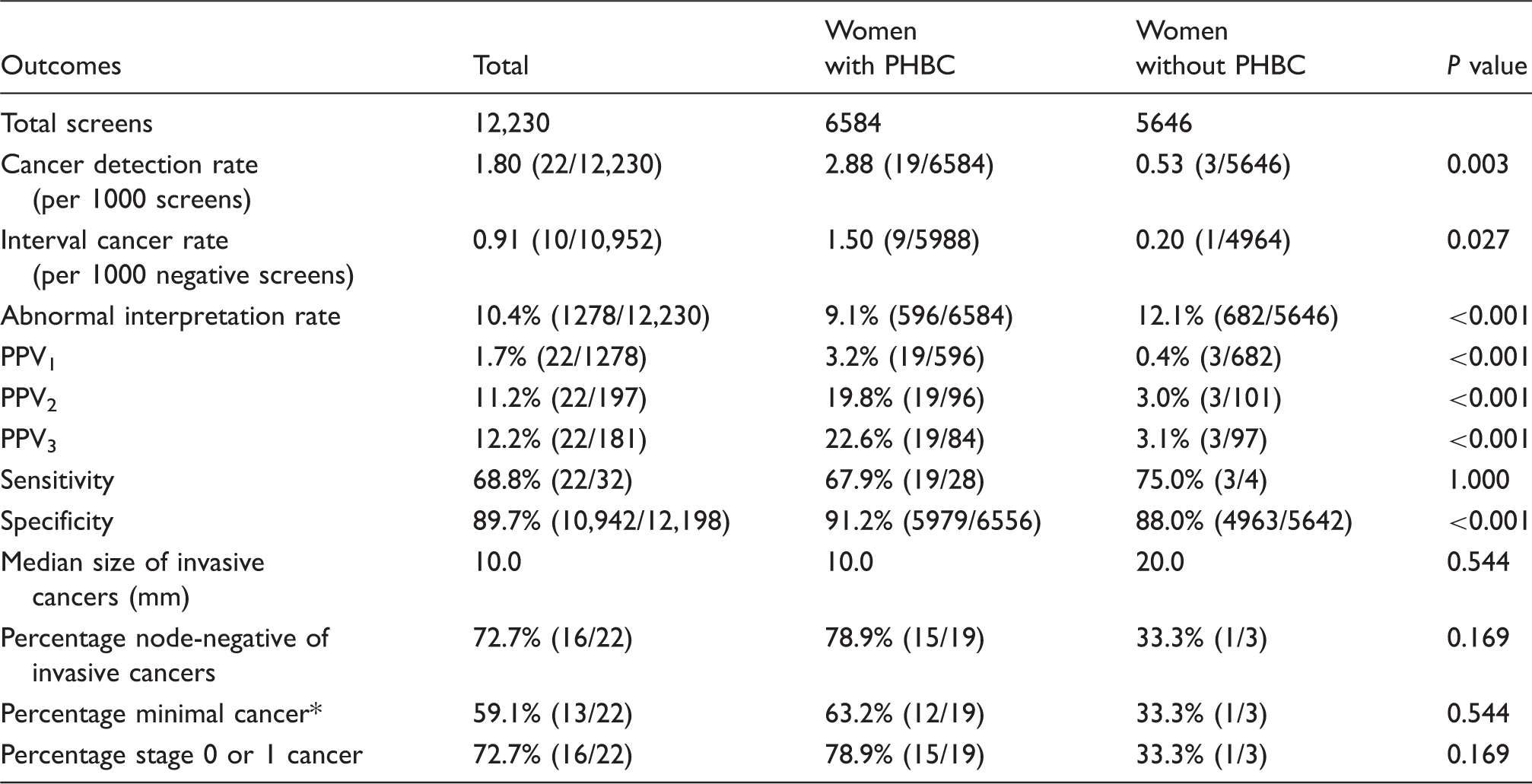
Minimal cancer: invasive cancers ≤ 1 cm or ductal carcinoma in situ of any size.
PPV1, number of detected cancers per positive examinations; PPV2, number of detected cancers per examinations with recommendation for tissue diagnosis (BI-RADS category 4 or 5); PPV3, number of detected cancers per examinations with biopsy performed; PHBC, personal history of breast cancer.
When we compared the outcomes of supplemental US in women with PHBC and women without PHBC, both the cancer detection rate and the interval cancer rate were higher in the women with PHBC than in those without PHBC (2.88 vs. 0.53 per 1000, P = 0.003; 1.50 vs. 0.20 per 1000, P = 0.027), respectively (Table 2). Abnormal interpretation rate was lower in women with PHBC than in those without PHBC (9.1% [596/6584] versus 12.1% [682/5646], P < 0.001). PPV1, PPV2, and PPV3 were higher in women with PHBC than in those without PHBC (3.2% [19/596] versus 0.4% [3/682], 19.8% [19/96] versus 3.0% [3/101], 22.6% [19/84] versus 3.1% [3/97], all P < 0.001), respectively. Sensitivity was not different in women with PHBC and in those without PHBC (67.9% [19/28] versus 75.0% [3/4], P = 1.000). Specificity was higher in women with PHBC than in those without PHBC (91.2% [5979/6556] versus 88.0% [4963/5642], P < 0.001) (Table 2).
Outcomes in women with PHBC according to the age and mammographic density
Of the 6584 women with PHBC, 2306 (35.0%) were women aged < 50 years and 4278 (65.0%) were those aged ≥ 50 years (Suppl. Table 1). Cancer detection rate was not different between women aged < 50 years and those aged ≥ 50 years (3.90 versus 2.33 per 1000, P = 0.259) and between women with dense breasts and those with fatty breasts (3.58 versus 1.86 per 1000, P = 0.204). However, interval cancer rate was higher in women < 50 years than in those ≥ 50 years (3.86 [8/2071] versus 0.25 [1/3917], P = 0.001) and higher in women with dense breasts than in those with fatty breasts (2.58 [9/3481] versus 0 [0/2507], P = 0.013). Abnormal interpretation rate was higher in women aged < 50 years than in those aged ≥ 50 years (10.2% [235/2306] versus 8.4% [361/4278]), P = 0.018). Both the sensitivity and specificity were lower in women aged < 50 years than in those aged ≥ 50 years (52.9% [9/17] versus 90.9% [10/11], P = 0.049; 90.1% [2063/2289] versus 91.8% [3916/4267], P = 0.025).
Clinicopathologic features of interval cancers and screening detected cancers in women with PHBC
Clinicopathologic features of interval cancers and screening detected cancers in women with PHBC.

ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; PHBC, personal history of breast cancer.
Discussion
In this study, we found that supplemental breast US screening in women with PHBC detected additional cancers at an early stage in addition to mammography but also showed higher interval cancer rate than in women without PHBC, although majority of interval cancers showed stage 0 or 1.
Our overall cancer detection rate of 1.80 per 1000 is within ranges of other study results regarding supplementary US screening (cancer detection rate of 1.1–4.6 per 1000 exams) (13–15,22–28). For women with PHBC, our cancer detection rate of 2.88 per 1000 is at the lower part of the range of 3.7–4.2 per 1000 cancer detection rate reported in the American College of Radiology Imaging Network (ACRIN) 6666 study (14,15), but it is close enough to conclude that the additional cancer detection rate by supplemental breast US in women with PHBC is higher than those of women without PHBC.
Interval cancers tend to be aggressive and show advanced stage, thus, a low interval cancer rate is used as a measure indicating effectiveness of a screening examination (29). Our interval cancer rate of 1.50 per 1000 negative exams in women with PHBC is higher than 1.2 per 1000 (nine clinically detected cancers per 7473 exams) from the ACRIN 6666 study (15). Our interval cancer rate of 0.53 per 1000 negative exams in women without a PHBC is similar to 0.43 per 1000 women with average risk reported from the Japan Strategic Anti-cancer Randomized Trial (13). Corsetti et al. (22) reported that the interval cancer rate in women with dense breasts receiving mammography and US (1.1 cancers per 1000 negative exams) was similar to that in women with fatty breast receiving mammography alone (1.0 cancers per 1000 negative exams). Thus, they suggested that supplemental breast US screening might overcome decreased sensitivity in dense breasts. However, based on higher interval cancer rate in our women with PHBC relative to those without PHBC, supplemental breast US screening might not fully overcome decreased sensitivity of screening mammography in this population. In the ACRIN 6666 study in which 54% of the participants had PHBC, even immediately after three-year rounds of screening with mammography and US in women at elevated risk, 14.7 per 1000 cancers were additionally detected by supplemental MRI (15). Similar to a result of a recent study in which the most important risk factor for interval cancer in women with PHBC was younger age (29), interval cancers were more frequently found in women aged < 50 years than in those aged ≥ 50 years (3.86 [8/2071] versus 0.25 [1/3917], P = 0.001) and in women with dense breasts than in those with fatty breasts (2.58 [9/3481] versus 0 [0/2507], P = 0.013) in our PHBC group. Therefore, it should be noted that supplemental breast US screening is not sufficiently effective due to higher interval cancer rate for younger women aged < 50 years with PHBC.
With regard to the abnormal interpretation rate and PPV, main barriers to implement supplemental US, our abnormal interpretation rate of 10.4% (1278/12230) and PPV1 of 1.7% (22/1278) are comparable to other US screening study results (5.5–28.3% abnormal interpretation rate; 1.9–3.5% PPV1) (13–15,21,25–28). However, when our results are compared to the 10.6% abnormal interpretation rate and 4.4% PPV1 of screening mammography derived from the Breast Cancer Surveillance Consortium (25), abnormal interpretation rates are similar but PPV1 are lower. The main reason for the lower PPV1 in our study is thought to be the 8.8% (1081/12,230) proportion of BI-RADS category 3 and its 0% (0/1081) cancer yield. To calculate the PPV1, the final assessment category 3 was counted as a positive result; thus, to improve the PPV1, present imaging criteria for BI-RADS category 3 on US in our practice should be downgraded to BI-RADS category 2. A previous study on US elastography has shown its potential to reduce abnormal interpretation rate and improve PPV1 in a diagnostic setting (30). Further validation is required to evaluate its efficacy in a screening setting for the future research.
On the other hand, our PPV3 of 22.6% in women with PHBC is higher than the range 2.3–16.2% of PPV3 from other study results and 11.4–16.2% from the ACRIN 6666 study (14,15). The relatively higher PPV3 in our study might be from that most of the examinations were incidence screening and placement of PACS workstations in each of our US examination rooms in order to review present and previous mammograms and previous US images just prior to the US examination, leading to more follow-ups rather than biopsies for stable solid masses.
Finally, the majority (78.9%, 15/19) of screening detected cancers for women with PHBC were stage 0 or 1 cancers and the median size of invasive cancers was 10.0 mm (range = 1–40 mm). Our results are comparable with those from the ACRIN 6666 study in which majority of detected cancers were stage 0 or node negative invasive cancers with a median size of invasive cancers of 16 mm (range = 3–40 mm) (15).
There are several limitations in our study. First, women aged < 50 years (39.5% versus 35.0%) or women with heterogeneously or extremely dense breast tissue (79.7% versus 59.4%) were more frequently found in women without PHBC than in those with PHBC, which might have resulted in higher abnormal interpretation rate, lower PPV1, and lower specificity in women without PHBC. However, this distribution difference might have not reversed the higher cancer detection rate and higher interval cancer rate in our PHBC group. Second, breast US examinations were performed by radiologists in a single academic institution. Thus, we cannot generalize our outcomes to those performed by technologists or automated breast US. Third, additional costs and physician time by supplemental breast US were not calculated in this study, which needs to be further investigated to implement supplemental breast US in clinical practice.
In conclusion, supplemental breast US screening detected additional 2.88 early stage second breast cancers per 1000 women who had PHBC with acceptable abnormal interpretation rate of 9.1% and relatively high PPV3 of 22.6%. However, relatively high interval cancer rate in younger women with dense breasts should be noted. Our study would be informative for women with PHBC to choose supplemental screening modality in addition to mammography.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2014R1A1A2055402).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.