
Abstract
Background
Several interventional procedures show a dependency on fluoroscopy times (FT) and level of training. Furthermore, FT and dose area products (DAP) vary depending on access site and target vessel for chest port implantations, but not for other thoracic interventions such as percutaneous coronary interventions.
Purpose
To evaluate the influence of the combination of venous access site and level of training on FTs and DAPs during peripherally inserted central catheters (PICC) implantations in a large cohort of patients.
Material and Methods
In this retrospective study, PICC implantations of 681 consecutive patients (385 women, 296 men; mean age = 55.0 ± 16.7 years) were analyzed. Two groups of junior (< 50 interventions) and senior (≥ 50 implantations) radiologists were investigated in respect to FT and DAP during PICC placement procedures. Statistical analysis included the Mann–Whitney U test and the Kruskal–Wallis test. P values < 0.05 were considered significant.
Results
Senior radiologists required significantly less FT (senior = 0.43 s, junior = 0.53 s, P = 0.041), but there was no significant difference in DAPs (senior = 56.3 µGy*m2, junior = 60.6 µGy*m2, P = 0.151). PICC implantations through the left side resulted in a significant reduction of the median FT by 60.9% (left = 0.45 s, right = 1.15 s, P = 0.010).
Conclusion
Due to considerable dose reduction, the left-sided puncture, especially via the basilic and brachial veins, performed by well-trained interventional radiologists seem to be the preferable approach for PICCs.
Keywords
Introduction
In the last two decades, peripherally inserted central catheters (PICC) have become widely available and were frequently used for chemotherapy, parenteral nutrition with hyperosmolar infusions, frequent blood tests, and high-pressure injections in both in- and outpatient settings (1–6).
Historically, Werner Forssmann described the first fluoroscopic guided placement of a 65-cm, 4F central venous catheter (CVC) in the right atrium in 1929 (7). In the following years, different kinds of central venous access devices like Midline, supra, and infraclavicular CVC, Broviac and Hickman catheters, as well as totally implantable central venous port devices have been established (8).
In comparison to non-tunneled CVCs, PICCs could be used for a longer period (2–3 months vs. 14 days) and were associated with lower infection rates than CVC (0.36/1000 catheter days vs. 0.57/1000 catheter days). Additionally, it has been shown that PICCs are more cost-effective than a peripheral intravenous (i.v.) catheter after four days of infusion therapy (9).
There are three different implantation techniques described in the literature. First, the landmark technique estimating the length of the catheter using cutaneous anatomical landmarks. A final radiograph approved the correct tip placement. Second, the ECG-guided approach observing morphological variations of the P wave, which could also be performed by nurses trained in specialized i.v. access teams (10). Finally, the ultrasound-guided puncture and fluoroscopic-guided approach, which was the preferred implantation technique in our institution due to its high success rate (11).
Nevertheless, fluoroscopic guidance requires radiation exposure to the patient, the operator, and assistant staff (12). Several interventional procedures show a dependency on fluoroscopy times (FT) and level of training in small study populations (13,14). Furthermore, FTs and dose area products (DAP) seemed to vary depending on the access site and target vessel for chest port implantations (15), whereas radiation doses required for other thoracic interventions such as percutaneous coronary interventions seemed not to differ significantly based on the site of vascular access (16).
The purpose of this study was to evaluate the influence of the combination of venous access site and level of training on FTs and DAPs during PICC implantations in a large collective.
Material and Methods
Study design
A total of 681 consecutive patients (385 women, 296 men; mean age = 55.0 ± 16.7 years), referred to our department for PICC implantation between April 2010 and April 2015, were included in this retrospective study. Institutional ethics committee approval and written informed consent were obtained. All interventions were performed using the MultiDiagnost Eleva FD2.1 (Philips Healthcare, Best, The Netherlands) fluoroscopy unit equipped with a flat panel detector. All inserted PICCs were PowerPICCs (Bard Access Systems, Salt Lake City, UT, USA). The actual catheter size and number of lumen varied according to the clinical requirement. A group of 20 radiologists were divided into a junior subgroup (n = 11) and a senior subgroup (n = 14). The same radiologist could be a participant in both groups as soon as the 50th PICC implantation was reached. Both subgroups were evaluated with regard to FT and DAP.
Statistical analysis included the Shapiro–Wilk test, Spearman’s correlation, Mann–Whitney U test, and the Kruskal–Wallis test using SPSS Statistics (IBM Version 23, Armonk, NY, USA). P values < 0.05 were considered significant.
Procedure
In our institution, the preferred access vessel was the superficial basilic vein. Further targets could be the deep brachial or the superficial cephalic vein. After the assessment of target vessel’s patency using a 7.5-MHz linear array probe, skin disinfection and sterile dressing were accomplished. Then, an ultrasound-guided puncture of the target vessel was performed using a 21G micropuncture needle in local anesthesia with prilocaine and epinephrine (Xylonest 1%; AstraZeneca, Wedel, Germany). A tourniquet was usually used to facilitate the puncture. Entering the target vessel, a 0.0018-inch guide wire was advanced, preferably into the inferior vena cava under fluoroscopic guidance to assure venous access. Length of the PICC was adjusted according to the length of the inserted guide wire, measuring 65 cm in total. The favored tip position was the cavoatrial junction. Removing the puncture needle, a peel-away sheath was advanced over the wire in the Seldinger technique. After retrieving the guide wire, the shortened PICC was inserted with the guide wire under fluoroscopic guidance. As soon as the PICC reached the final position, the guide wire and the peel-away sheath was removed. Following the PICC fixation and dressing, a final single shot radiograph was obtained to assure correct placement (11).
Results
All 681 reported PICC implantations were performed successfully without any major complications according to the Society of Interventional Radiology (SIR) guidelines (17).
Number of implanted PICCs.
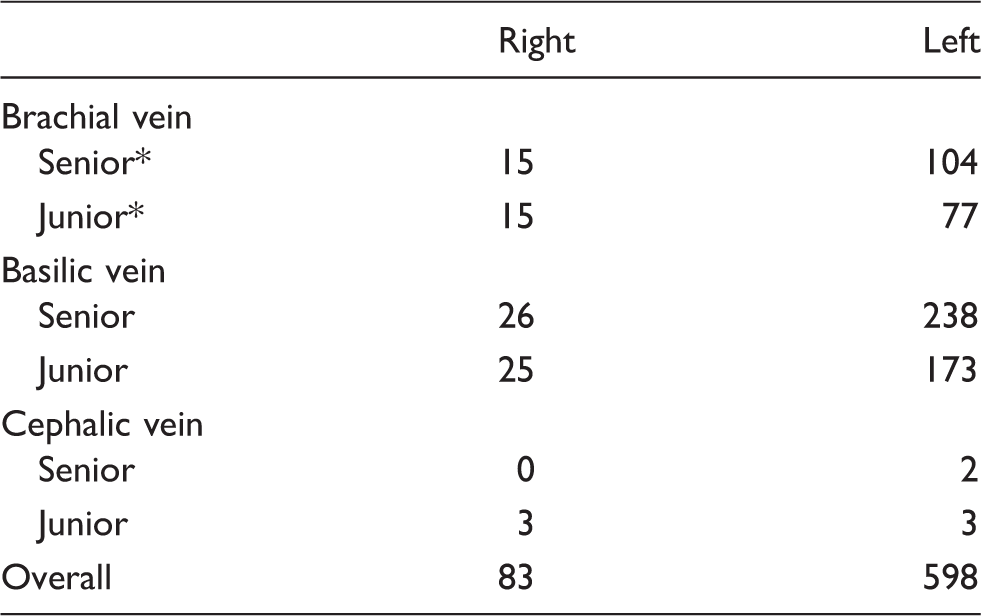
Senior > 50 implantations; junior < 50 interventions.
PICC, peripherally inserted central catheters.
Radiation dose – junior vs. senior radiologists.

Mean and median values of the dose area product (DAP) and the fluoroscopy time (FT) vs. junior and senior radiologists.

Experience vs. FT in seconds (a - log scale) and vs. DAP in µGy*m2 (b - linear scale).
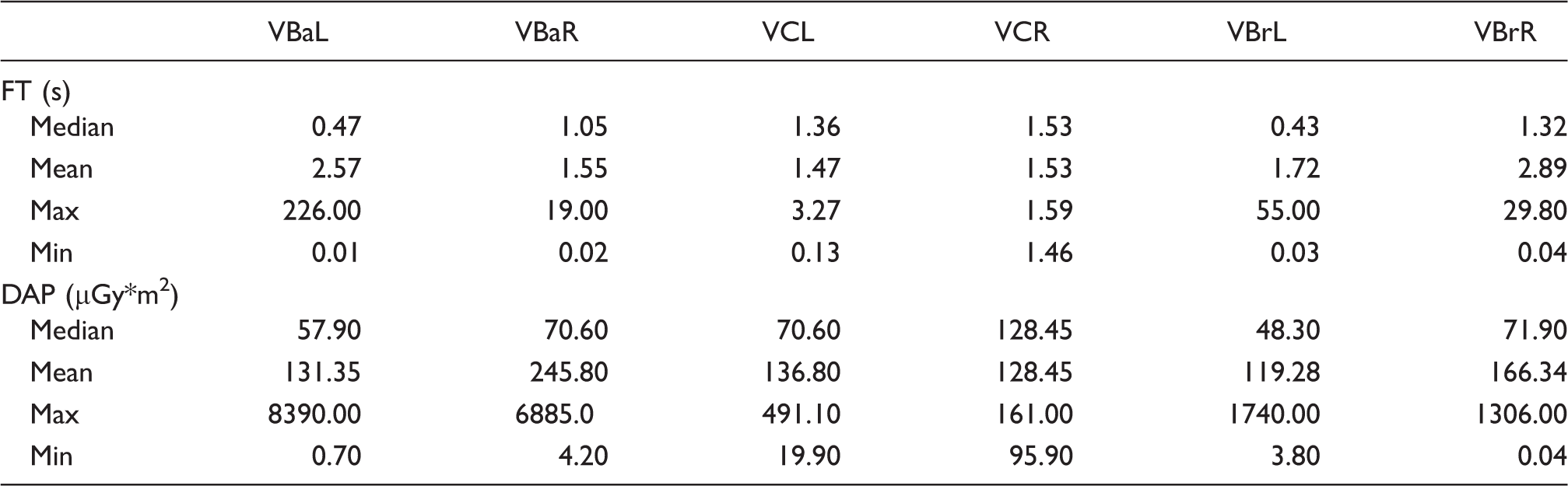
Moreover, there were no significant differences between each analyzed target vessel in FT (P = 0.061) and DAP (P = 0.375). Although access through the left-sided vessels required less FT than each right-sided equivalent (brachial vein: left = 0.43 s, right = 1.32 s; basilic vein: left = 0.47 s, right = 1.05 s) (Fig. 2, Table 3), there was no statistical significance between the FTs.
Puncture site vs. FT in seconds (a) and vs. DAP in µGy*m2 (b). VBaL, left basilic vein; VBaR, right basilic vein; VCL, left cephalic vein; VCR, right cephalic vein; VBrL, left brachial vein; VBrR, right brachial vein. Radiation dose in dependency to puncture site. Puncture site vs. fluoroscopy time (FT) in seconds and vs. dose area product (DAP) in µGy*m2. VBaL, left basilic vein; VBaR, right basilic vein; VCL, left cephalic vein; VCR, right cephalic vein; VBrL, left brachial vein; VBrR, right brachial vein.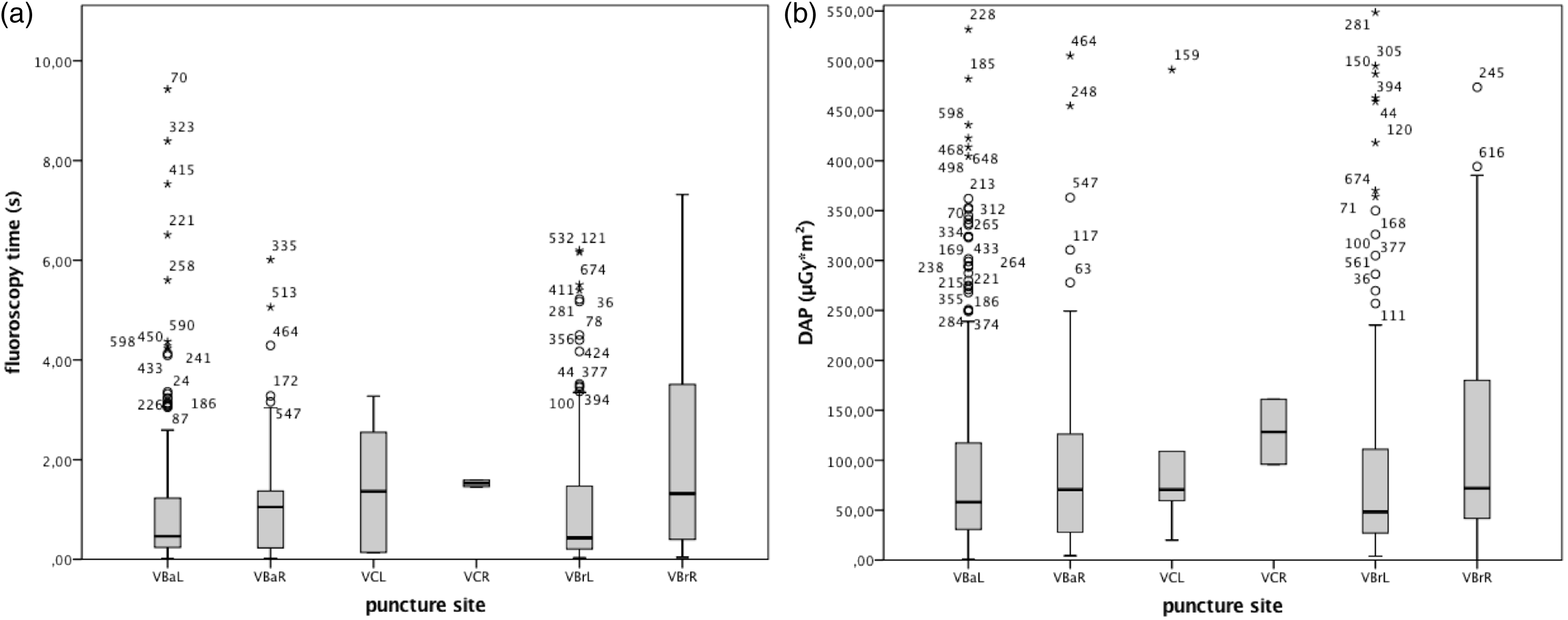
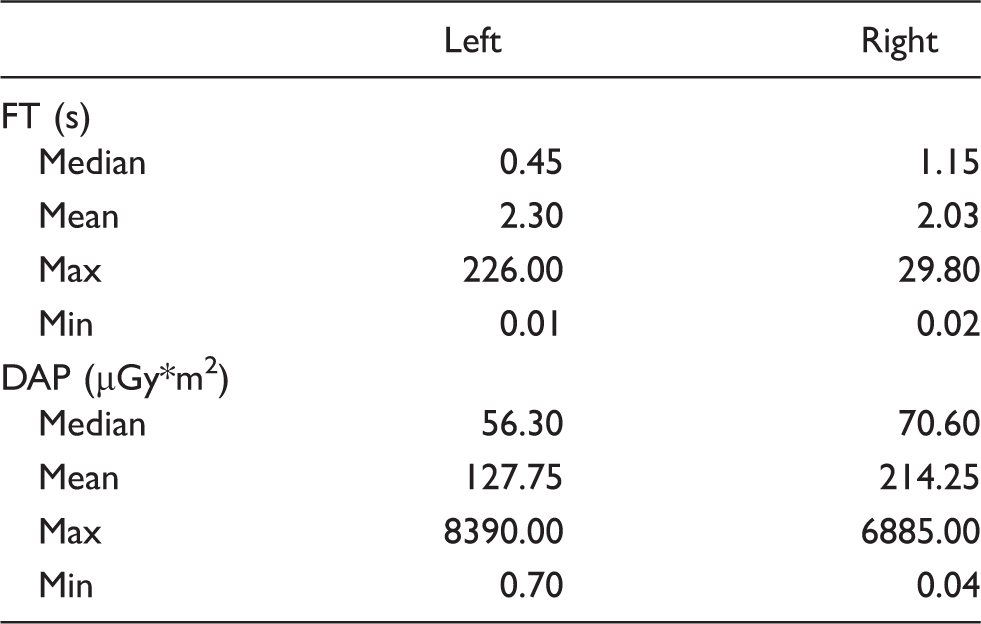
All PICC implantations from the left side together showed significant savings of about 60.9% in FT (median: left = 0.45 s, right = 1.15 s, P = 0.010; Fig. 3, Table 4). Although DAPs from the left were in median approximately 20.25% lower and no significance could be attested in this study (median: left = 56.30 µGy*m2, right = 70.60 µGy*m2, P = 0.130). The number of implantations from the right and left side did not show significant variations between both observed subgroups (P = 0.311).
Access side vs. FT in seconds (a) and vs. DAP in µGy*m2 (b). Radiation dose in dependency to access side. Mean and median values of the dose area product (DAP) and the fluoroscopy time (FT) vs. access side.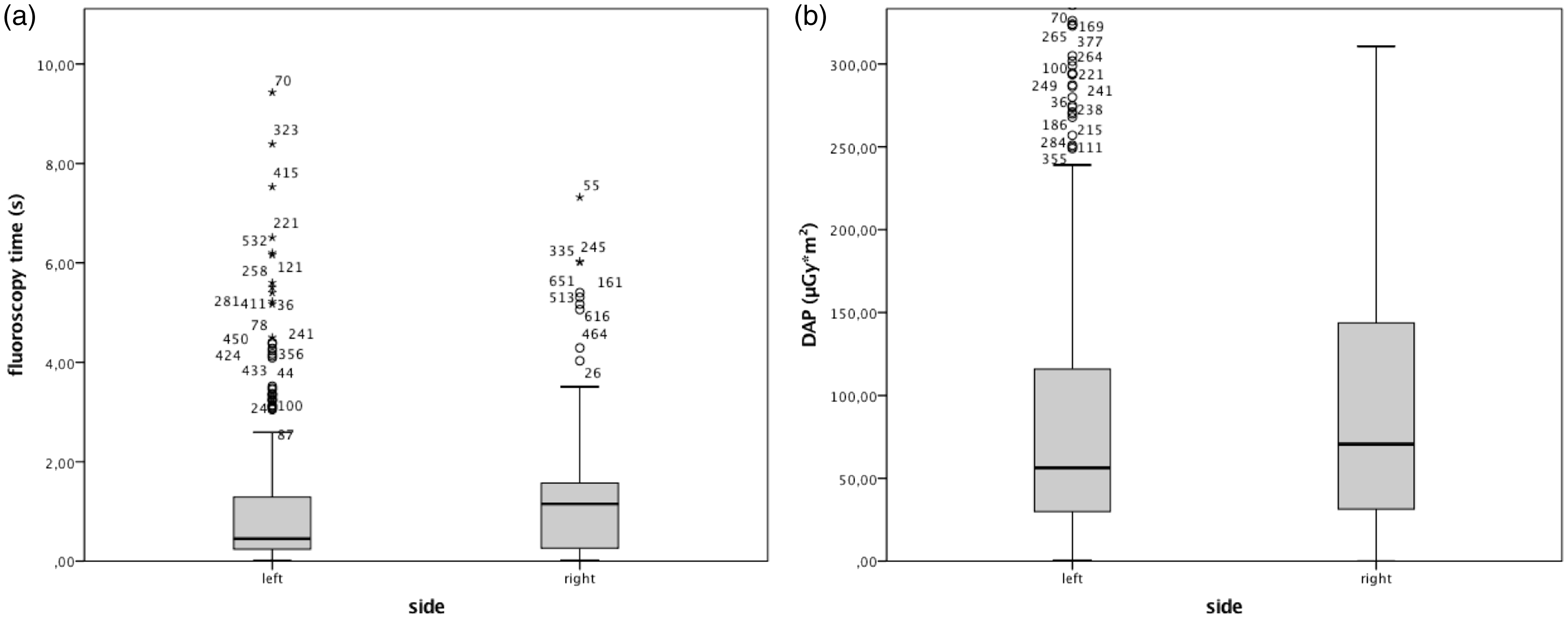
Discussion
The present study demonstrated that a left-sided puncture was associated with a significant reduction in FT throughout both subgroups of patients (P = 0.010). In particular, the left basilic and left brachial vein showed a decrease of FT by 50% in comparison to all other investigated target vessels (P = 0.061). The right cephalic vein showed the largest FTs and DAPs in this study, which was probably due to the curvy anatomical course. However, statistical analyses did not reveal any significance in DAP values depending on the puncture side or the target vessel. This might be due to a larger acquired field of view for left-sided approaches. Storm et al. reported FTs of approximately 102 s and a mean DAP of 287 µGy*m2 in 493 PICC implantation procedures (18). These values were markedly higher than in our study and in both observed subgroups.
The radiation dose depends on multiple factors (12). One of these was the level of training as senior radiologist required in median 19% less FT than junior radiologists (P = 0.041). The FT mainly served as a surrogate parameter for intervention time, which will decrease concordantly to interventionalist’s experience. Nevertheless, Xu et al. reported, that years in residency alone showed no significant reduction in FTs (14). No significance could be found comparing senior and junior radiologists in terms of required DAP for this procedure as the discrepancy in FT of 0.1 s is probably not technically relevant, although statistically significant.
PICC had reasonably low complication rates. Moureau et al. reported an overall complication rate in 50,470 patients with different catheter types, whereas midline catheters had a complication rate of 4.5/1000 catheter days, PICCs of 2.0/1000, non-tunneled CVC of 1.1/1000, tunneled CVC 1.0/1000, and chest ports of 0.52/1000 (19). Further studies showed that catheter-associated bloodstream infection rates seem not to vary depending on the right or left implantation side (20). However, a study of 798 sequential PICC revealed that venous thrombosis was not significantly associated with the laterality of implantation (right = 1.23%, left = 1.30%) (21). Nevertheless, Liem et al. found out that most thrombosis occurred in the cephalic vein with 7.2%, in the basilic vein with 1.9%, and 0% in the brachial vein (22).
There were further implantation approaches without fluoroscopy guidance such as the landmark-based and the ECG-guided technique for tip-positioning. However, a post-implantation radiograph will mostly confirm correct tip placement after the implantation procedure. For ECG guidance, it has been reported that 10% of patients showed no p-wave changes, especially in left-sided approaches, which was the preferred insertion side with 87.8% of all implantations in this study. Moreover, it has been shown, that ECG guidance is more reliable for shorter and stiff catheters due to more stable lead connections (23). Another disadvantage of the ECG method and the landmark approach was their inability to differentiate between intra- and extravascular catheter position (24). However, real-time fluoroscopy guidance facilitated catheter placements in cases with anatomical variants, venous thrombosis, and strictures (8).
This study has limitations due to its retrospective design. Moreover, data concerning infection rates and complications associated to the level of training would have been desirable. However, long-term follow-up of the entire population could not be ensured. Although, radiation doses from CVCs were comparably low compared to other interventional procedures, no reference values were existing so far. Larger multicenter studies should be performed with a standardized protocol to define an optimal dose range as already done for many other procedures (25).
In conclusion, due to considerable dose reduction, the left-sided puncture, especially via the basilic and brachial veins performed by well-trained interventional radiologists, seem to be the preferable approach for PICCs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Martin Jonczyk and Federico Collettini are participants in the BIH-Charité Clinical Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Martin Jonczyk and Federico Collettini are participants in the BIH-Charité Clinical Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health.