
Abstract
Background
Diffusion-weighted imaging (DWI) and susceptibility-weighted imaging (SWI) are reliable imaging modalities for brain tumors. However, the role of DWI and SWI in the diagnosis of common lateral ventricular tumors has not been systematically evaluated.
Purpose
To evaluate the diagnostic performance of DWI and SWI in common lateral ventricular tumors.
Material and Methods
Fifty-two patients with histopathologically confirmed lateral ventricular tumors were included in this study (18 with central neurocytomas, nine with ependymomas, seven with high-grade gliomas, and 18 with meningiomas). The relative minimum apparent diffusion coefficient (rADCmin) and relative average apparent diffusion coefficient (rADCave) measured by DWI and the intratumoral susceptibility signal intensity (ITSS) of hemorrhage acquired by SWI were calculated. These quantitative parameters were evaluated using the Mann–Whitney U test, receiver operating characteristic curve, and logistic regression analyses.
Results
The rADCmin and rADCave ratios of central neurocytomas were significantly lower than those of the other neoplasms. The rADCmin and rADCave ratios of ependymomas and the rADCave ratio of high-grade gliomas were significantly higher than those of meningiomas. The ITSS score of meningiomas was significantly lower than those of the other tumors, while the score of central neurocytomas was obviously lower than those of ependymomas and high-grade gliomas. The combination of the rADC ratio with the ITSS showed no significant difference, except in discriminating between meningiomas and high-grade glioma-ependymomas.
Conclusion
The rADC ratios and ITSS may be useful for differentiating common lateral ventricular tumors. The diagnostic performance may be improved with the use of the rADC ratios and ITSS scores.
Keywords
Introduction
Lateral ventricular tumors refer to heterogeneous neoplasms that arise and expand within the lateral ventricle or originate from the walls of the ventricle and extend in their growth mainly within the ventricular cavity (1). Any parenchymal tumor can grow into the lateral ventricle, especially high-grade gliomas. Because of the complex origins and various histopathologic types and grades of lateral ventricular tumors, an accurate differential diagnosis is challenging for clinical neuroradiologists. Due to differences in the biological and histological nature of lateral ventricular tumors, treatment strategies and prognosis for these entities vary substantially. Benign neoplasms such as meningiomas and central neurocytomas are usually associated with a favorable prognosis after complete resection of the tumors (2), whereas ependymomas with cerebrospinal fluid dissemination and high-grade gliomas still possess poor prognosis after radiation therapy or chemotherapy in addition to surgery (3,4). Clinically, meningiomas and central neurocytomas are the two commonest tumors in the lateral ventricle, but ependymomas and high-grade gliomas need to be further discriminated with the formers. Therefore, a reliable preoperative differentiation of the four tumors plays a crucial role in the patient’s prognosis.
In many cases, these lesions are relatively easy to differentiate by conventional magnetic resonance imaging (MRI), along with the clinical conditions. However, obtaining an accurate differential diagnosis by conventional MRI alone can be very difficult because the imaging features of these tumors exhibit considerable overlap. Advanced MRI techniques, including diffusion-weighted MRI (DWI) and susceptibility-weighted MRI (SWI), may supplement physiological information and allow further specification in the differential diagnosis of brain tumors (5). As a quantitative imaging marker, DWI can non-invasively reflect tumor cellularity together with the extracellular space by the measurement of the apparent diffusion coefficient (ADC) value (6). As previously reported, DWI has been widely utilized to describe the diffusional properties of meningiomas, central neurocytomas and high-grade gliomas within the brain parenchyma, indicating that the ADC value and ADC ratio may be useful in the differential diagnosis of these entities (7–9). However, few systematic reports have clarified the ADC value or ADC ratio measurements for the differential diagnosis of common lateral ventricular tumors. SWI is a relatively emerging MRI technique, which is much more sensitive to T2* signaling caused by local susceptibility effects (10). This novel technique has been proven to be a valuable tool in assessing intracranial tumors because it can provide more information about hemorrhage, venous blood vessels and calcification (11,12). Recently, intratumoral susceptibility signals (ITSS) derived from SWI have been used as quantitative or semi-quantitative parameters for the discrimination of primary central nervous system lymphoma from high-grade gliomas (13,14). Nevertheless, little is known about whether ITSS can add value when differentiating among common lateral ventricular masses.
Most importantly, the combination of DWI and SWI in the differential diagnosis of four common lateral ventricular tumors has never been examined in previous studies. Thus, the purpose of our study was to investigate whether DWI and SWI could non-invasively differentiate these entities, including meningiomas, central neurocytomas, ependymomas, and high-grade gliomas.
Material and Methods
Patients
The institutional review board of our hospital approved this retrospective study and the requirement for patients’ informed consent was waived due to its retrospective nature. Potentially eligible patients with lateral ventricular tumors who had undergone surgical resection in our hospital were selected. The inclusion criteria were as follows: (i) definite histopathological diagnosis of central neurocytoma, meningioma, high-grade glioma, or ependymoma in the lateral ventricle according to the World Health Organization (WHO) 2016 classification criteria (15); (ii) DWI and SWI in addition to conventional MRI were performed before treatment; and (iii) all data available were obtained by 3.0-T MR. Finally, a total of 52 patients were enrolled in the study.
Imaging protocol
All MR images were acquired in the routine clinical work-up using a 3.0-T MRI system (Magnetom Verio TIM; Siemens Healthcare, Erlangen, Germany) with an eight-channel head coil. The conventional MRI protocols consisted of the following sequences: axial T1-weighted (T1W) gradient-echo imaging (TR/TE = 250/2.48 ms), axial T2-weighted (T2W) turbo spin-echo imaging (TR/TE = 4000/96 ms), axial T2W fluid-attenuated inversion recovery (FLAIR; TR/TE = 9000/94 ms, TI = 2500 ms), and three orthogonal planes of contrast-enhanced gradient-echo T1W imaging (CE-T1W imaging; TR/TE = 250/2.48 ms).
DWI was performed by a multi-slice, single shot echo planar imaging (EPI) sequence in the axial plane. The imaging protocols adopted were as follows: TR/TE = 8200/102 ms, slice thickness = 5 mm, gap = 1 mm, matrix = 128 × 128, field of view (FOV) = 22 × 22 cm, average = 1, scanning time = 1 min 32 s. Two b-values of 0 and 1000 s/mm2 were used in the read, phase, and slice directions.
SWI was performed on a cross-section with a three-dimensional (3D) fully flow-compensated gradient-echo sequence with the following parameters: TR/TE = 27/20 ms, flip angle = 15°, FOV = 230, matrix = 256 × 243 mm, number of excitation = 1, section thickness = 1.5 mm, intersection gap = 0.3 mm. Subsequently, the SWI sequences were reconstructed with the minimum intensity projection (MinIP) technique to obtain images with a section number, thickness, and position similar to other sequences.
Data processing
All imaging assessments were performed on an off-line Siemens workstation with standard software (Magnetom Verio TIM; Siemens Healthcare). For the assessment of DWI data, ADC values were measured by manually placing the region of interest (ROI) inside the tumor regions on the ADC maps. First, SWI images were used as a reference to avoid hemorrhage, small veins, cysts, necrosis, and calcifications. Second, the ROIs were placed on the enhancing solid portion of the tumors corresponding to CE-T1W imaging. Third, at least five uniform small round ROIs with sizes of approximately 30–40 mm2 were selected to place inside the tumors on the ADC maps. The ROI with the lowest ADC value was chosen as the minimum ADC (ADCmin) and an average value from multiple ROIs was chosen as the average ADC (ADCave). In addition, the same ROIs were placed on the contralateral normal-appearing white matter (NAWM; defined on T2W imaging and CE-T1W imaging) at the same layer on ADC maps. The relative ADCmin and ADCave (rADCmin and rADCave) ratios of the tumors were calculated as the ratios of the ADCmin and ADCave of the tumors divided by the mean ADC of the contralateral NAWM.
For semi-quantitative analysis of SWI data, the number of intralesional hemorrhages was calculated and graded for each tumor. Hemorrhagic lesions could be different from calcification based on the combination of phase images. The grading standard in the ITSS scoring system was set as follows: Grade 0 = no hemorrhage; Grade 1 = 1–10 dot-like hemorrhages; Grade 2 = 11–20 dot-like hemorrhages; Grade 3 = more than 20 dot-like hemorrhages (13). The relative ADC values derived from DWI and the ITSS generated from SWI were measured by two independent neuroradiologists (with eight and seven years of experience) who were blinded to the histopathological findings. If a disagreement occurred, a consensus was reached by discussing the images with another neuroradiologist (with 30 years of experience).
Statistical analysis
All quantitative parameters are presented as the means ± standard deviation (SD). Next, the Welch test and Mann–Whitney U test were used to compare the differences in the rADCmin and rADCave ratios among these tumors. In addition, the Kruskal–Wallis H test and Mann–Whitney U test were applied to compare the differences in the ITSS among different lateral ventricular tumors. In this study, when conducting receiver operating characteristic (ROC) curve analysis, high-grade gliomas and ependymomas were grouped together as HGG-EP for comparisons with central neurocytomas or meningiomas. The ROC curve was analyzed to define the optimal cutoff value to maximize the sum of the sensitivity and specificity. Binary logistic regression analysis was performed to evaluate the significant difference between each signal parameter and the added imaging parameter. The ability of the logistic regression model to allow for discrimination among four common lateral ventricular tumors was analyzed by the area under the curve (AUC). All P values <0.05 were considered to represent statistical significance. Statistical analysis was performed using SPSS software (Version 20.0 for Windows, SPSS Inc., Chicago, IL, USA) and MedCalc (Version 12.1.0, MedCalc Inc., Mariakierke, Belgium).
Results
The primary clinical manifestation of the four common types of lateral ventricular tumors.
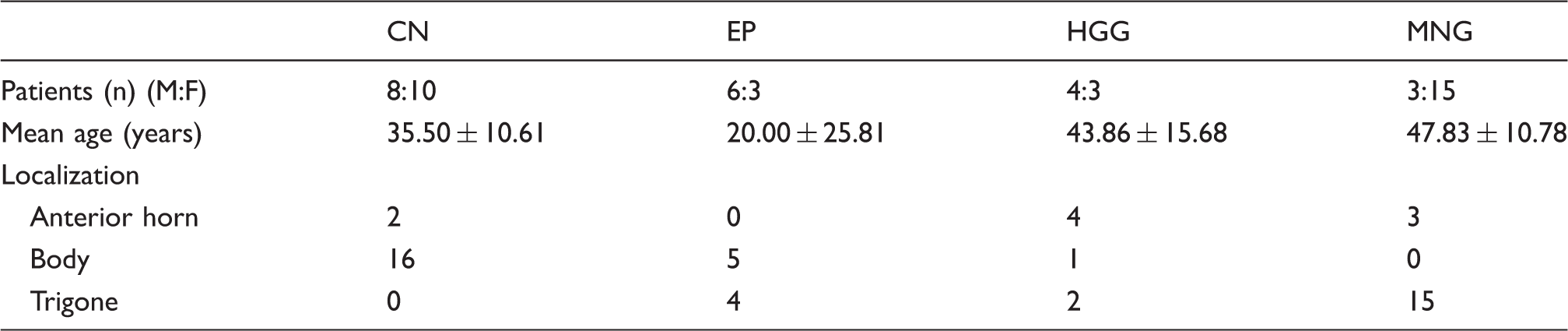
CN, central neurocytomas; EP, ependymomas; HGG, high-grade gliomas; MNG, meningiomas.
The rADCmin, rADCave ratios, and ITSS of the four common different lateral ventricular tumors (mean ± SD).

CN, central neurocytomas; EP, ependymomas; HGG, high-grade gliomas; MNG, meningiomas. rADCmin, the relative minimum apparent diffusion coefficient; rADCave, the relative average apparent diffusion coefficient; ITSS, intratumoral susceptibility signal intensity.
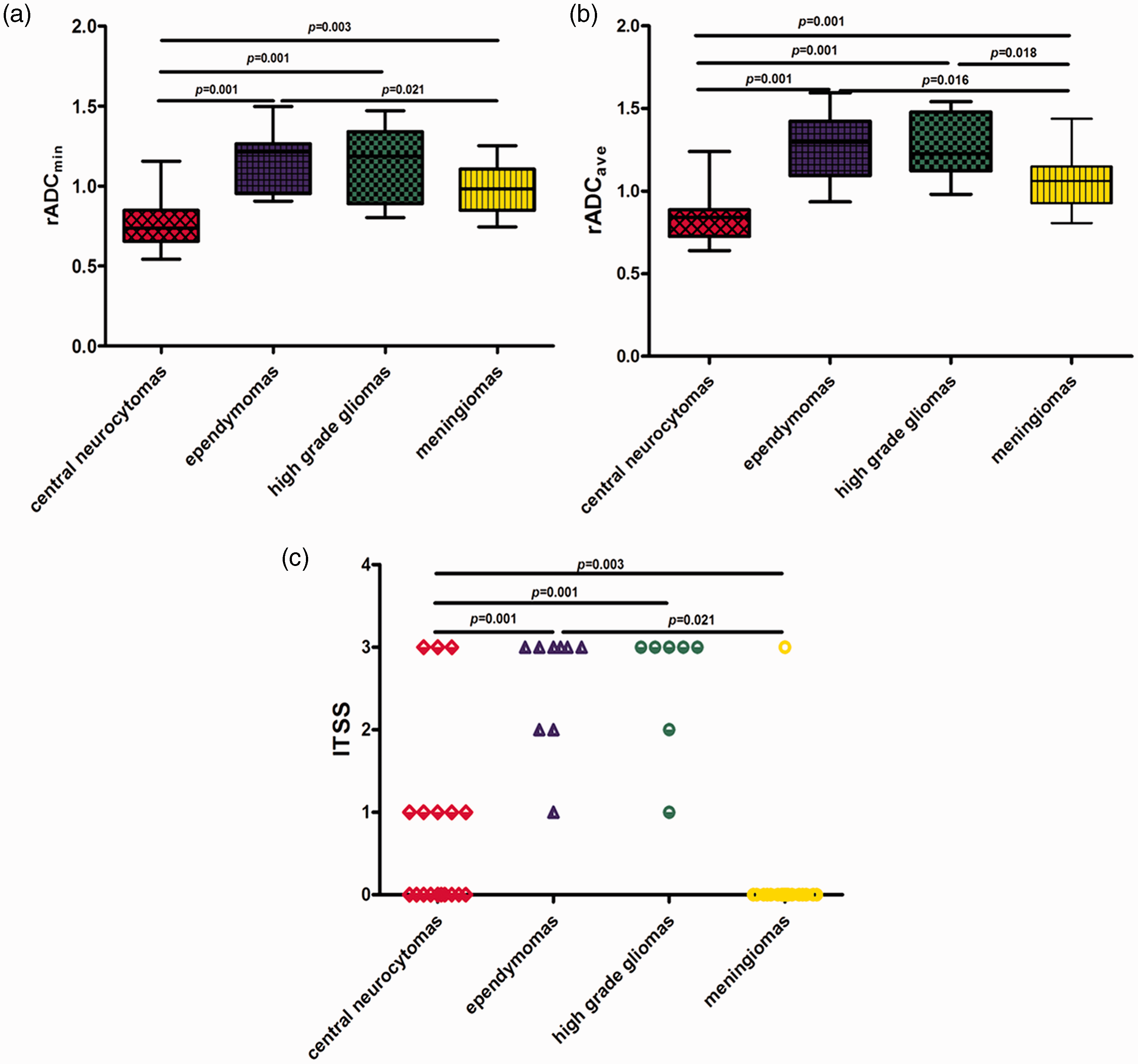
Comparison of (a) the relative minimum apparent diffusion coefficient (rADCmin), (b) the relative average apparent diffusion coefficient (rADCave), and (c) the intratumoral susceptibility signal intensity of hemorrhage (ITSS) among four common lateral ventricular tumors using the Mann–Whitney U test.
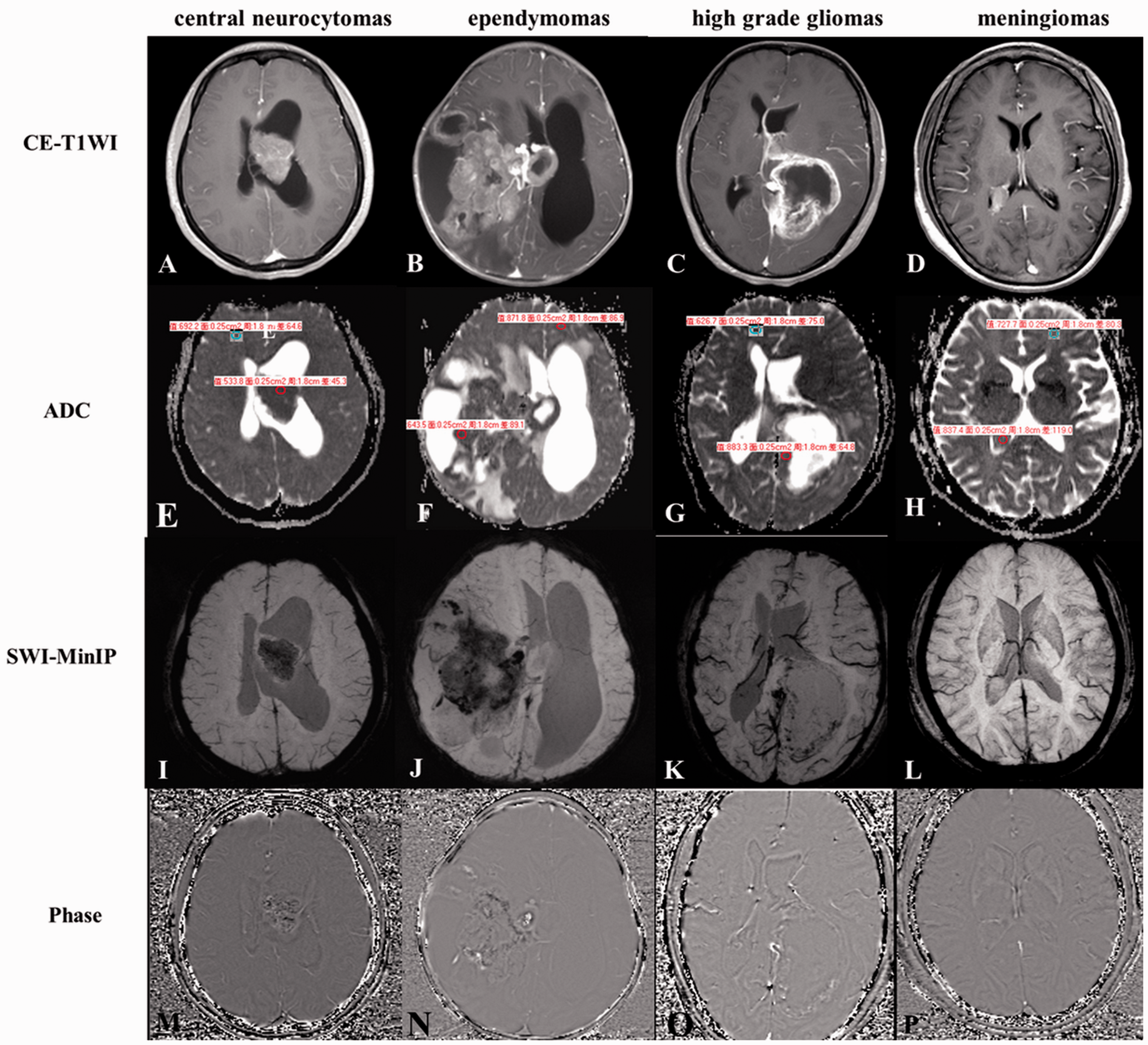
Representative images of four common lateral ventricular neoplasms. All four tumors of the lateral ventricle demonstrated obvious enhancement on CE-T1W images, especially in (a–d). On the corresponding ADC maps, relatively decreased ADC values were shown in (e) central neurocytomas (rADC = 0.77) and (f) ependymomas (rADC = 0.74), whereas increased ADC values were shown in (g) high-grade gliomas (rADC = 1.33) and (h) meningiomas (rADC = 1.18). On SWI-MinIP and corresponding phase images, multiple spotted hemorrhagic signals were found in ependymomas (j, n) and high-grade gliomas (k, o), and calcific signals were found in central neurocytomas (i, m), whereas no microhemorrhages were found in meningiomas (l, p).
The ITSS score was lowest in meningiomas (0.17 ± 0.70) and highest in high-grade gliomas (2.67 ± 0.82). A significant difference was also found among the four neoplasms for the ITSS (H = 30.52, P < 0.001). The ITSS in meningiomas was significantly lower than the values in the other tumors (all P < 0.05). Furthermore, the ITSS scores in central neurocytomas were obviously lower than those in ependymomas and high-grade gliomas (both P < 0.05).
Measurements of the sensitivity, specificity, PPV, NPV, CV, and AUC of rADCmin and rADCave ratios for differentiation among CN, MNG, and HGG-EP.
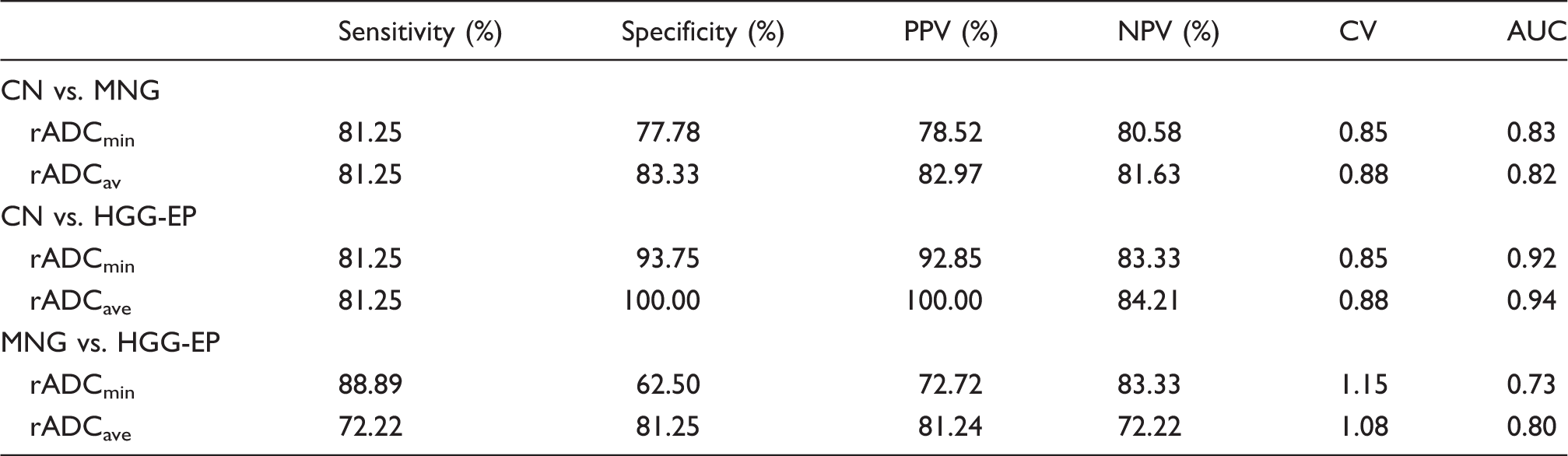
rADCmin, the relative minimum apparent diffusion coefficient; rADCave, the relative average apparent diffusion coefficient; CN, central neurocytomas; MNG, meningiomas; HGG-EP, high-grade gliomas and ependymomas; PPV, positive predictive value; NPV, negative predictive value; CV, cutoff value; AUC, area under the curve.
Measurements of the sensitivity, specificity, PPV, NPV, CV, and AUC of ITSS for differentiation among CN, MNG, and HGG-EP.

ITSS, intratumoral susceptibility signal intensity. CN, central neurocytomas; MNG, meningiomas; HGG-EP, high-grade gliomas and ependymomas; PPV, positive predictive value; NPV, negative predictive value; CV, cutoff value; AUC, area under the curve.
Comparison of univariate and bivariate models for differentiation among CN, MNG, and HGG-EP.
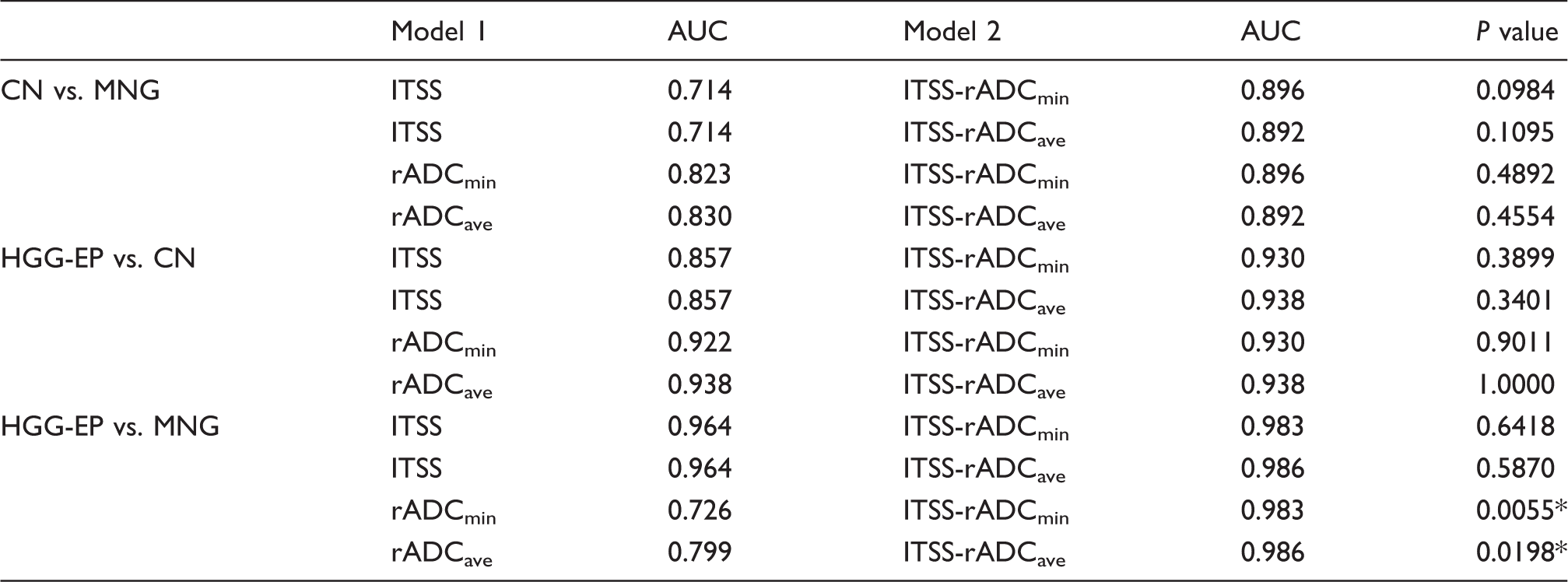
P < 0.05.
CN, central neurocytomas; MNG, meningiomas; HGG-EP, high-grade gliomas and ependymomas; rADCmin, the relative minimum apparent diffusion coefficient; rADCave, the relative average apparent diffusion coefficient; ITSS, intratumoral susceptibility signal intensity.
Discussion
It has been widely acknowledged that MRI is the ideal modality of choice to establish a reliable differential diagnosis of lateral ventricular tumors and define the therapeutic approaches (16,17). Unfortunately, although the role of conventional MRI in the characterization of common lateral ventricular tumors has been well established, in some cases, the imaging features of these tumors may be non-specific (18). In recent years, advanced MR techniques, including DWI and SWI, have been shown to be helpful for this crucial differential diagnosis. In our study, we evaluated SWI and DWI to improve the preoperative diagnostic accuracy of common lateral ventricular neoplasms, including central neurocytomas, meningiomas, high-grade gliomas, and ependymomas.
Currently, DWI is widely applied as a routine clinical examination for the diagnosis of brain tumors. Although ADC values and ratios generated from DWI have been used in brain tumors (7,8), no systematic studies have focused on the discrimination of lateral ventricular tumors based on rADCmin and rADCave ratios. Moreover, the rADC ratio is considered more reliable to demonstrate the changes of water diffusivity (19). In this study, we found that the rADCmin and rADCave ratios of central neurocytomas were lowest among the four tumors. Additionally, the rADCave ratio of high-grade gliomas and the rADCave and rADCmin ratios of ependymomas were significantly higher than those of meningiomas, which was consistent with the results of Haleena et al. (7). Similarly, Murat et al. (8) discovered that the rADC ratio of central neurocytomas was lower than those of astrocytomas and non-astrocytomas. De Belder et al. (9) suggested that ADC values were sufficient to distinguish between meningiomas and high-grade gliomas, which was consistent with our findings. As previously reported, ADC values can vary as a result of heterogeneous histopathology or tumor progression (20); therefore, the rADC ratios were very helpful in grading tumors as low-grade and high-grade. In respect of low-grade tumors, a high degree of malignancy is associated with decreased rADC values because of packed cells with little extracellular matrix (21). However, increased cellularity in central neurocytomas and meningiomas constitutes a relative barrier to water diffusion and results in a lower rADC ratio than in malignant tumors. Along with these results, our present study also indicated that both rADCmin and rADCave ratios were inadequate to distinguish between ependymomas and high-grade gliomas. Nevertheless, Charles et al. (22) found that differentiation was simple because brainstem gliomas always had a high ADC, whereas ependymomas had a low ADC, which is inconsistent with our research of supratentorial tumors, likely because anaplastic ependymoma, with microvascular proliferation and foci of necrosis (23), accounted for 66.7% (6/9) of the tumors in our study.
SWI has extraordinary sensitivity to the magnetic susceptibility differences of various tissues (10), making it superior for the detection of microhemorrhage (24–26). The ITSS grading system has been shown to strictly correlate with tumor grade and the differential diagnosis (13,26,27). However, for common lateral ventricular tumors, no study has reported the semi-quantitative analysis of ITSS in hemorrhage. In our present study, the lowest ITSS score was found in meningiomas, followed by central neurocytomas, whereas the highest score was in high-grade gliomas, which was consistent with previous studies (13,28). Meningiomas manifested obviously lower ITSS scores than the other tumors, indicating a lack of evidence of microhemorrhage within meningiomas in our study. Additionally, only one high-grade meningioma, a rhabdoid meningioma, was detected in this analysis, and the pathological features consisted of increased proliferation and hemorrhage (29). The score of central neurocytomas was significantly lower than that of ependymomas and high-grade gliomas, which may be explained by their well-differentiated nature with rare hemorrhage (30). Therefore, our results suggested that the ITSS of hemorrhage enhanced confidence in the differential diagnosis of the four tumors.
Another valuable finding of our study was that the optimal threshold value derived from the rADC ratios or ITSS could be considered a reference for the differential diagnosis of these tumors. In our present study, the combinational value of DWI and SWI was innovatively taken into consideration, and all AUCs in the combined parametric models were larger than those in the single model, indicating that to some degree, this combination could provide additional diagnostic value for the differentiation of these entities. Although a statistically significant difference was not found in most comparison groups, the combination of DWI and SWI may provide a better diagnostic performance with a higher AUC, and thus may be helpful for clinical work.
Our study has some limitations. First, the major limitation is the small number of patients. Therefore, a larger clinical trial is needed to establish for the combination of SWI and DWI in the diagnosis of lateral ventricular tumors. In addition, the physical contribution of the ITSS corresponds to hemorrhage, calcification, or neovascularity. However, in this study, we only evaluated the ITSS-intratumoral hemorrhage among these neoplasms. It is possible that calcification and intralesional vessels could also contribute to the differential diagnosis; therefore, ITSS-calcification and neovascularity should be further investigated. Third, we did not subcategorize the tumors into WHO grades due to the relatively small number of included tumors. Fourth, remarkable cystic and necrotic regions were obvious in some patients, which may lead to challenges and measurement error. Finally, histogram or texture analysis for DWI and SWI, which may provide more information than ROI measurement, were not performed in our present study and will be explored in our further study.
In conclusion, this study demonstrated that the rADCmin and rADCave ratios and ITSS-hemorrhage appear to be useful parameters to establish a differential diagnosis of common lateral ventricular tumors. In addition, the diagnostic performance may be improved using the combination of the rADC ratios and ITSS scores.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Leading Project of the Department of Science and Technology of Fujian Province (No. 2016Y0101), the Special Funds of Provincial Finance of Fujian Province (No. BPB-CDR2013), and the Research Foundation for Young Scholars of the Health Department of Fujian Province (No. 2013-1-34).