
Abstract
Background
Deep, high-grade bursal-sided supraspinatus tendon tears are sometimes preoperatively misinterpreted as full-thickness tears on shoulder magnetic resonance imaging (MRI).
Purpose
To determine the usefulness of disproportionate fluid sign for differentiating high-grade bursal-sided partial-thickness tears from full-thickness tears on conventional MRI.
Material and Methods
Preoperative MRIs of 198 patients with arthroscopically confirmed high-grade bursal-sided partial-thickness tears and full-thickness tears were independently reviewed by two readers on two occasions. The presence of high-grade bursal-sided partial-thickness tears with a confidence level using a five-point grading scale was assessed based on tear depth alone and also in combination with disproportionate fluid sign, defined as a prominent subdeltoid or subacromial-subdeltoid bursal fluid distension with a relative paucity of effusion in the glenohumeral joint. The sensitivity, specificity, accuracy, and area under the receiver operating characteristic curve (AUC) were calculated, as well as inter-observer reliability.
Results
The disproportionate fluid sign was identified in 60/74 (81.2%) bursal-sided partial-thickness tears and 9/124 (7.5%) full-thickness tears. The sensitivity and accuracy of the diagnosis of bursal-sided tear were higher when disproportionate fluid sign was used in conjunction with the tear depth, compared with tear depth alone (P < 0.001). There was excellent inter-observer agreement for disproportionate fluid sign and deep bursal-sided tear. The AUCs were significantly higher in combination with disproportionate fluid sign.
Conclusion
The disproportionate fluid sign indicates the presence of a deep, high-grade bursal-sided partial-thickness tear, which can be misinterpreted as a full-thickness tear. Thus, it can provide greater diagnostic assistance to less-experienced radiologists and clinicians.
Introduction
Ultrasonography (US), magnetic resonance imaging (MRI), and magnetic resonance arthrography (MRA) are commonly used for imaging evaluation of the rotator cuff tendons of the shoulder. Although MRA is slightly more sensitive and more specific than either US or MRI in diagnosing full-thickness tears, all the above methods provide good diagnostic accuracy, and any of them could be used to detect full-thickness tears in patients with shoulder pain who are being considered for surgery (1–7). However, both US and MRI may offer less diagnostic accuracy in detecting partial-thickness tears compared with MRA (2,3,5,8–10). Therefore, further research is warranted to determine whether advances in criteria, reader training, or MRI techniques could improve the diagnostic performance in partial-thickness tears, including bursal-sided or articular-sided tears.
MRI is increasingly being used in daily practice to evaluate painful shoulders. Thus, the authors have experienced numerous cases in which preoperative diagnoses using MRI initially suggested the presence of full-thickness tears, but subsequent arthroscopy confirmed deep, high-grade bursal-sided partial-thickness tears. In such cases, we anecdotally perceived a characteristic MRI feature: a prominent subdeltoid or subacromial-subdeltoid bursal fluid distension with a relative paucity of effusion in the glenohumeral joint in the setting of a visible rotator cuff tear on preoperative conventional MRI (Fig. 1). We defined this feature as the “disproportionate fluid sign.” There has been little information regarding the disproportionate fluid sign in deep, high-grade bursal-sided partial-thickness tears mimicking full-thickness tears. Therefore, the purpose of this study was to retrospectively determine the usefulness of the disproportionate fluid sign in differentiating high-grade bursal-sided partial-thickness tears from full-thickness tears on conventional MRI.
A 63-year-old man with a deep bursal-sided tear of the supraspinatus tendon of the right shoulder. Oblique coronal fast spin-echo T2W MR image with fat suppression (a) shows near full-thickness defect of the tendon at the footprint (arrowhead). On oblique sagittal fat-suppressed fast spin-echo T2W MR image (b), the prominent subdeltoid bursal effusion (arrow) is noted. In contrast, marked collapse of the axillary pouch (blank arrowhead) and paucity of the effusion in the glenohumeral joint is seen. This is consistent with the disproportionate fluid sign. He was preoperatively diagnosed with a full-thickness tear. Arthroscopic rotator cuff repair was performed two weeks after the MRI. A glenohumeral arthroscopic view (c) enabled us to confirm the minimally fibrillated articular surface of the supraspinatus tendon without a defect. H, humeral head; BT, biceps tendon; A, rotator crescent; B, rotator cable; asterisk, air bubble. Subacromial bursoscopic view (d) shows a focal bursal-sided tendon defect (black arrows) and exposed pinkish insertional bone marrow of the footprint of the greater tuberosity (asterisk).
Material and Methods
Patient selection
This was a retrospective study approved by the institutional review board at our institution. The requirement for informed consent was waived, in view of the nature of the study. We reviewed a surgical database consisting of 800 arthroscopic rotator cuff repair surgeries performed by one experienced orthopedic surgeon (SHK) at our institution between October 2007 and October 2013. Only shoulders with a full-thickness tear with mild retraction (<2.5 cm) or high-grade bursal-sided partial-thickness tear of the supraspinatus were included, providing a pool of 293 shoulders. A number of patients were excluded from this pool for the following reasons: (i) one patient who underwent rotator cuff surgery without preceding MRI; (ii) one patient who had a history of fractures around the shoulder; (iii) one patient who had a past medical history of infectious or inflammatory arthritis in the affected shoulder; (iv) 51 patients who underwent preoperative direct or indirect MRA or computed tomography (CT) arthrography instead of conventional shoulder MRI; (v) eight patients who underwent MRI of suboptimal image quality or protocol composition at other hospitals; and (vi) 33 patients who experienced a time interval of >100 days between preoperative MRI and arthroscopic surgery. A total of 198 patients were finally enrolled into the study (109 men, 89 women; mean age = 58.6 ± 8.3 [SD] years) and included 124 patients (60 men, 64 women; mean age = 61.1 ± 7.2 years) with full-thickness tears and 74 patients (49 men, 25 women; mean age = 54.6 ± 8.6 years) with high-grade bursal-sided partial-thickness tears. The mean time between preoperative MRI and shoulder arthroscopy was 36.9 ± 25.4 days.
MRI acquisition
MR parameters focusing on the fluid-sensitive sequences.

FSE, fast spin-echo; SE, spin-echo.
Image analysis
To assess the added value of the disproportionate fluid sign in the differentiation of very high-grade bursal-sided partial-thickness tears from full-thickness tears, the diagnostic performance of conventional MRI alone and also in combination with the disproportionate fluid sign were compared. One senior resident (SJ) and one musculoskeletal radiologist (J-YC, with 11 years of post-residency experience in shoulder MRI) independently and retrospectively analyzed the MR images. Image interpretations were performed twice by each reader, with a four-week interval between readings. All MR images were presented randomly, and the readers were blinded to both the other radiologist’s interpretations and to the arthroscopic findings. Before the study, the resident received training by a board-certificated musculoskeletal radiologist regarding the definitions of abnormalities. If a fluid-equivalent hyperintense defect extending along the entire depth of the tendon was visible on T2W imaging, it was considered to be a full-thickness tear (11). If a fluid-equivalent focal hyperintense region that contacted the bursal surface of the rotator cuff was visible on T2W imaging, it was considered to be a bursal-sided partial-thickness tear (11). The partial-thickness tear is considered high-grade when it involves >50% of the tendon thickness. The training images were not included in the study cases. In the first session, each case was categorized (by forced choice) as either a high-grade bursal-sided partial-thickness tear or full-thickness tear, based on the tear depth alone, as in daily practice. Each reader was asked to assign a confidence level to the diagnosis using a five-point grading scale (1 = definite full-thickness tear, 2 = probable full-thickness tear, 3 = possible high-grade bursal-sided partial-thickness tear, 4 = probable high-grade bursal-sided partial-thickness tear, and 5 = definite high-grade bursal-sided partial-thickness tear). The cut-off score of the diagnosis of the high-grade bursal-sided partial-thickness tear was defined as 3. In the second reading session, all MR images were evaluated for the presence of the disproportionate fluid sign. The disproportionate fluid sign was defined as a prominent subdeltoid or subacromial-subdeltoid bursal fluid distension with a relative paucity of effusion in the glenohumeral joint, which means that there is little or no effusion in the posterior recess on axial intermediate-weighted images and collapse of the axillary pouch on oblique coronal T2W images, in the setting of a visible rotator cuff tear. If the disproportionate fluid sign was present, it was considered to be a very high-grade bursal-sided partial-thickness tear, even if the tear appeared to affect the entire tendon in depth. The level of confidence for the presence of a high-grade bursal-sided partial-thickness tear was rated in the same way as during the first session. Disagreements over the presence of the disproportionate fluid sign were adjudicated by a third observer (YSK, with two years of experience in shoulder MRI) who was blinded to the other observers’ interpretations and the arthroscopic diagnosis.
Statistical analysis
Statistical analyses were performed with the MedCalc for Windows software (version 13.3.3; MedCalc Software, Mariakierke, Belgium). The sensitivity, specificity, and accuracy of the diagnosis of a high-grade bursal-sided partial-thickness tear using the tear depth alone, as well as in combination with the disproportionate fluid sign, were determined by utilizing arthroscopy as the standard of reference. The McNemar test was used to compare the values, and the simple unweighted Cohen κ coefficient with a 95% confidence interval (CI) was used to assess the interobserver reliability of the type of tear and the presence of the disproportionate fluid sign. The kappa values can be interpreted as 0 representing less than chance agreement, 0.01–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement, and 0.80–0.99 almost perfect agreement (12). Receiver operating characteristic (ROC) analysis was performed for the diagnosis of a high-grade bursal-sided partial-thickness tear, and differences between the mean areas under the ROC curves (AUCs) for the two reading sessions were calculated.
Results
The disproportionate fluid sign was identified in 69/198 (34.8%) shoulders, including 60/74 (81.2%) bursal-sided partial-thickness tears (Fig. 1) and 9/124 (7.5%) full-thickness tears (Figs. 2 and 3). Preoperative MR reports, readers’ diagnosis, and arthroscopic results are summarized in Table 2. The sensitivity, specificity, and accuracy of the diagnosis of a deep bursal-sided partial-thickness tear in each reading session are shown in Table 3. For both readers, the sensitivity and accuracy of the diagnoses in combination with the disproportionate fluid sign were superior compared with conventional MR criteria alone, whereas the specificity was slightly worse in comparison. The diagnosis of high-grade bursal-sided partial-thickness tear made by each reader was significantly different when the disproportionate fluid sign was used in conjunction with the tear depth, compared with tear depth alone according to McNemar’s test (P < 0.001, respectively) (Table 3). The inter-observer agreement for the presence of the disproportionate fluid sign was excellent (κ = 0.858, 95% CI = 0.783–0.932). The inter-observer agreement for the diagnosis of a deep bursal-sided partial-thickness tear was also improved by using the depth of tear in combination with the disproportionate fluid sign (κ = 0.835, 95% CI = 0.758–0.912), compared with using tear depth alone (κ = 0.666, 95% CI = 0.548–0.783).
A 53-year-old man with a full-thickness tear of the supraspinatus tendon of the right shoulder. On an oblique coronal fat-suppressed fast spin-echo T2W MR image (a), a high-grade bursal-sided tendon defect (arrowhead) is demonstrated with a fluffy articular surface. There is a positive disproportionate fluid sign with fluid-distended subacromial-subdeltoid bursitis (arrow) and scanty glenohumeral effusion (blank arrowhead). He was preoperatively diagnosed with a high-grade deep bursal-sided tear. Arthroscopic rotator cuff repair was performed two weeks after the MRI. A glenohumeral arthroscopic view (b) shows an articular-sided defect (black arrows) at the footprint and the rotator crescent with a marked irregular surface. H, humeral head; BT, biceps tendon. A full-thickness tear was arthroscopically confirmed two weeks after the MRI scan. A 53-year-old man with a full-thickness tear of the supraspinatus tendon of the right shoulder. On an oblique coronal fat-suppressed fast spin-echo T2W MR image (a), a near full-thickness tendon defect (arrowhead) is demonstrated near the footprint. There is a fluid-distended subacromial-subdeltoid bursitis (arrow). Axial fat-suppressed fast spin-echo T2W MR image (b) demonstrates a small amount of effusion in the axillary pouch and posterior recess of the glenohumeral joint (blank arrowheads). Distal subdeltoid bursal effusion is also noted (arrow). Given these findings, the disproportionate fluid sign is negative. Arthroscopic rotator cuff repair was performed five weeks after the MRI. A glenohumeral arthroscopic view (c) reveals a focal full-thickness defect (black arrows) near the footprint and bursal space (asterisk) is seen through the defect. Summary of preoperative MR reports, readers’ diagnosis, and arthroscopic results. Number within the parentheses: confidence level using a five-point grading scale, mean ± SD. DFS, disproportionate fluid sign. Sensitivity, specificity, and accuracy of diagnosing a deep bursal-sided partial-ness tear of the supraspinatus tendon by using the tear depth alone and in combination with the disproportionate fluid sign (DFS). P value by McNemar’s test. CI, confidence interval.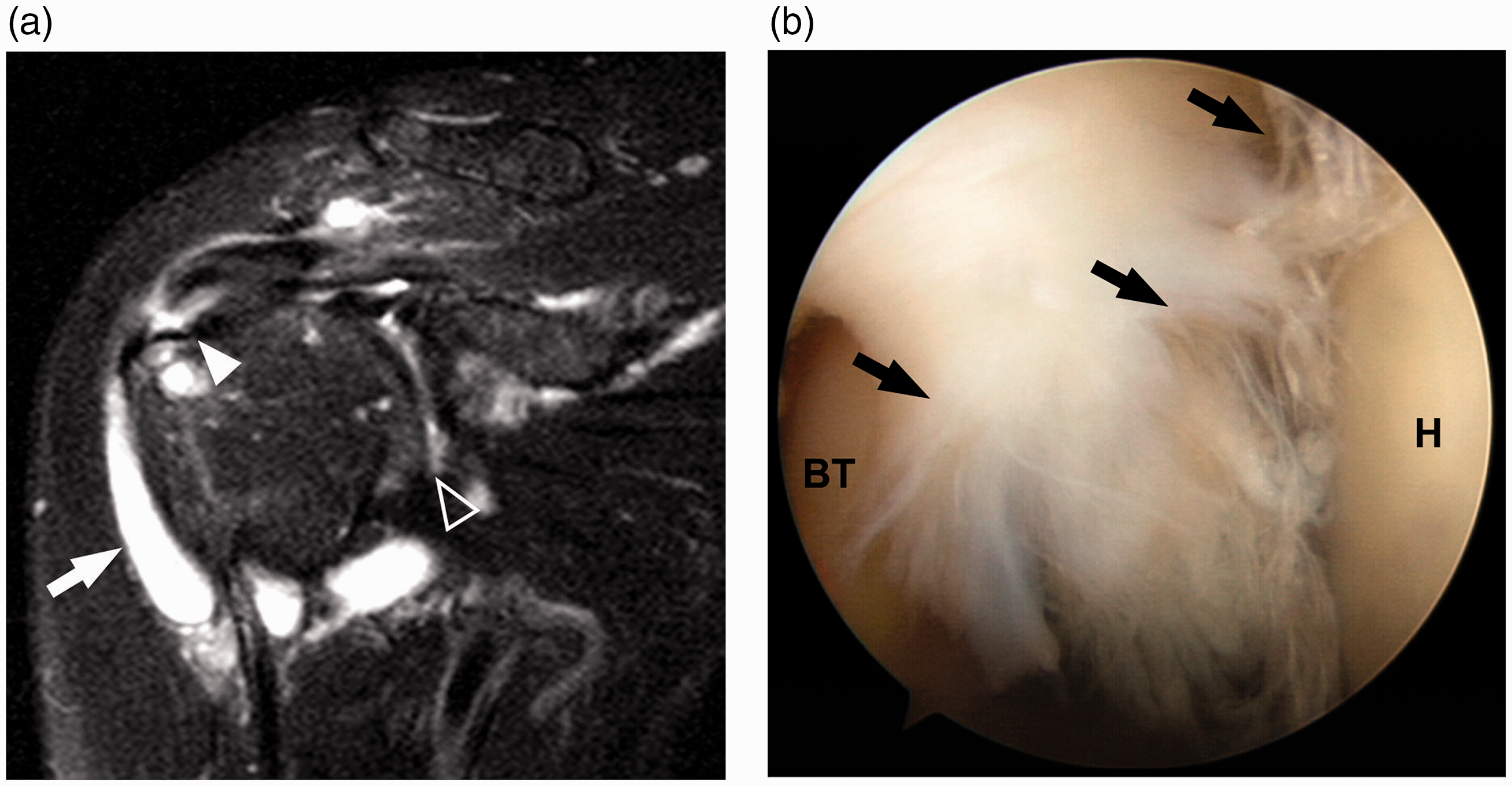
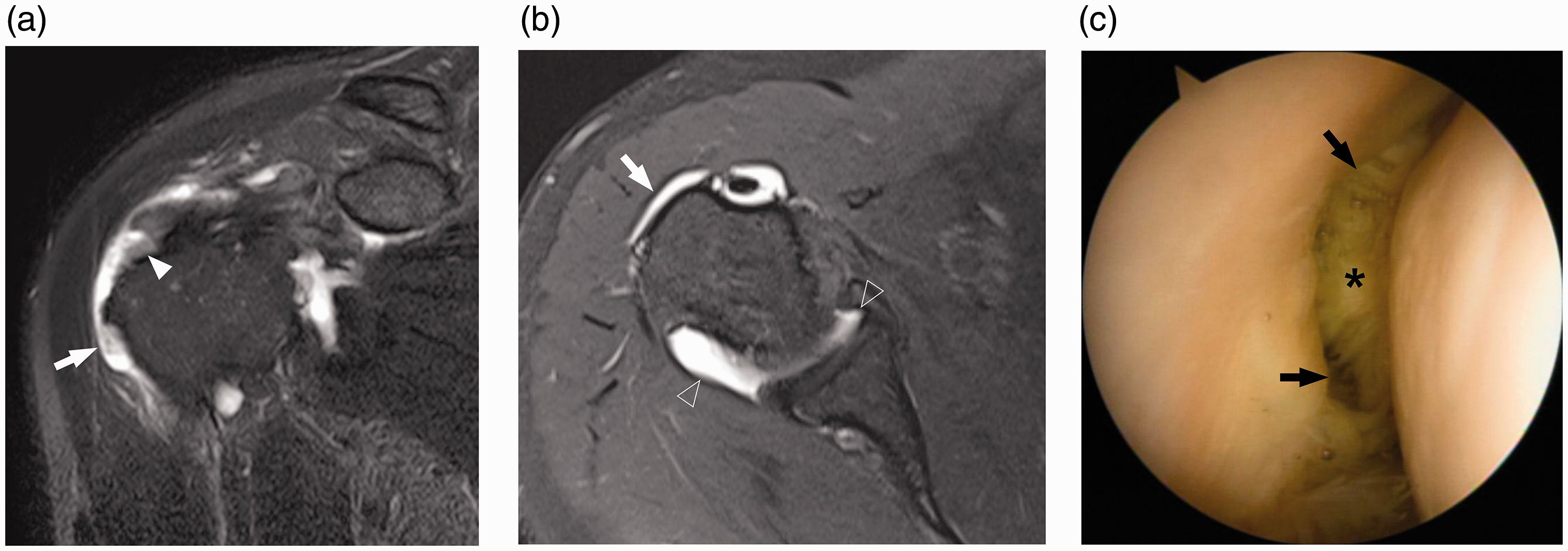

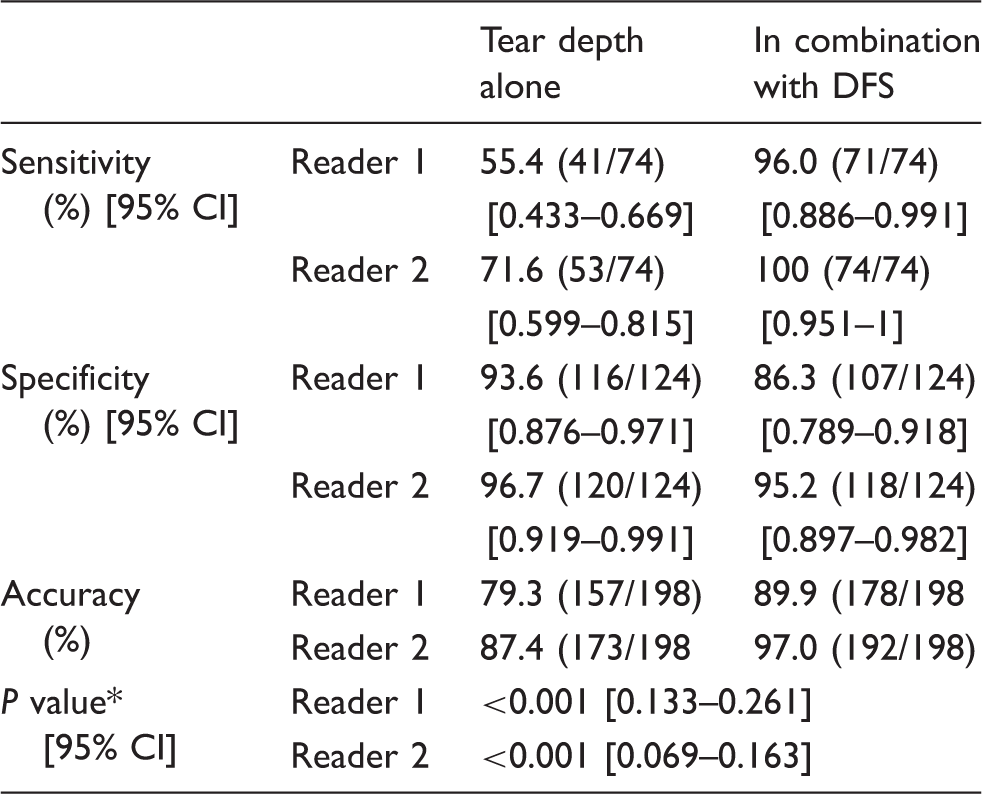
Fig. 4 presents the overall diagnostic performance of both readers with ROC curves and AUCs for each reading performed using tear depth alone and in combination with the disproportionate fluid sign. The AUC of both readers increased in diagnoses made using the disproportionate fluid sign, compared with those made without it (from 0.850 to 0.938, P = 0.002, 95% CI = 0.0313–0.145 for reader 1, and from 0.943 to 0.982, P = 0.013, 95% CI = 0.008–0.071 for reader 2).
The ROC curves and AUC values of the two radiologists for the detection of a deep bursal-sided partial-thickness tear of the supraspinatus tendon by using the tear depth alone and in combination with the disproportionate fluid sign: (a) reader 1 and (b) reader 2.
Discussion
The current study showed that the sensitivity and accuracy of the diagnosis of high-grade bursal-sided partial-thickness tear made by each reader were higher when the disproportionate fluid sign was used in conjunction with the tear depth, compared with tear depth alone. To date, signs considered to be diagnostic of a bursal-sided partial-thickness tear on MRI have included a defect on the bursal side of the rotator cuff and a fluid intensity signal within the tendons that are in contact with the bursal side of the rotator cuff (8,9,11). In the literature, the sensitivity of conventional MRI and MRA is in the range of 62–84% for bursal-sided partial-thickness tears (4,8,13). It has previously been reported that US and conventional MRI were less accurate for diagnosing partial-thickness tears, and that a deep bursal-sided partial-thickness tear could simulate a full-thickness tear appearing as a focal defect (10). Such low values for the diagnostic accuracy of detecting bursal-sided partial-thickness tears can be explained by the underestimation of low-grade small bursal-sided partial-thickness tears and the overestimation of deep bursal-sided partial-thickness tears, which have an extremely thin residual articular surface and appear similar to focal full thickness defects (8,10,13). However, the use of the disproportionate fluid sign improves the discrimination between high-grade bursal-sided partial-thickness tears and full-thickness tears. Moreover, although it has been reported that the inter- and intra-observer agreement for bursal-sided partial-thickness tears were lower than those for the detection of articular-sided tears, and that readers were less confident in diagnosing bursal-sided partial-thickness tears (13), the inter-observer agreement and confidence level in the current study were both improved with the use of the disproportionate fluid sign.
Previous studies have suggested that extrinsic subacromial impingement could be the main cause of bursal-sided partial-thickness tears (8,14–16). Such tears are associated with histological inflammation of the subacromial-subdeltoid bursa from direct subacromial mechanical impingement and irritation (17,18). Fluid in the subacromial-subdeltoid bursa, especially when combined with joint effusion, has been used as an indirect sign of rotator cuff tear (18–21). In cases of full-thickness tears, the fluid is believed to easily spread into both the subacromial-subdeltoid bursa and glenohumeral joint, because they are linked to each other through the full-thickness tendon defect. However, in cases of bursal-sided partial-thickness tears, the fluid in the subacromial-subdeltoid bursa following the subacromial impingement tends to stagnate primarily in the bursa due to the absence of a pathway into the glenohumeral joint. The disproportionate fluid sign is visible as a result of this. Consistent with our results, it has anecdotally been suggested that the identification of a disorder affecting the subacromial-subdeltoid bursa without intra-articular fluid collection should cause the physician to look carefully for a lesion affecting the bursal surface of the tendon (22). Therefore, given the MR findings of a near full-thickness tendon defect at the footprint and prominent subacromial-subdeltoid bursal fluid despite a lack of effusion in the glenohumeral joint, the so-called positive “disproportionate fluid sign,” we believe that a deep bursal-sided partial-thickness tear can easily be differentiated from a full-thickness tear. Although high-grade bursal-sided partial thickness tears are treated similarly to full thickness tears by repairing all possible tendon back to bone, rehabilitation after repair of the high grade bursal-sided tears is faster than for full-thickness tears because there is little tension on the suture (23). So, the differentiation of high grade bursal-sided tear appearing a full-thickness tear from a true full-thickness tear could be helpful when explaining the disease and prognosis to the patients and planning surgery and rehabilitation.
There are a few limitations to our study. First, we included many MR examinations performed at outside institutions. In those cases, we tried to include the cases with proper MR image qualities to limit variability caused by different MRI quality and/or protocol. Second, some cases experienced a long time interval between preoperative MRI and surgery, potentially enabling a deep bursal-sided partial-thickness tear to progress to a full-thickness tear upon operation. Therefore, the sensitivity for bursal-sided partial-thickness tears may be underestimated. Third, because the cases that showed a positive disproportionate fluid sign tended to be diagnosed as deep bursal-sided partial-thickness tears in the second reading session, full-thickness tear with a positive disproportionate fluid sign, even though few in number, were then misdiagnosed as bursal-sided partial-thickness tears. Thus, the specificity for the detection of bursal-sided partial-thickness tears was slightly decreased. However, we assume that this does not matter in clinical practice because such cases can easily be identified as full-thickness tear upon glenohumeral arthroscopy. Fourth, we only performed a qualitative assessment of the presence of the disproportionate fluid sign, rather than a quantitative measurement. However, considering the definition of the sign, its clinical application in routine practice can be possible with visual assessment alone. Finally, the readers were aware that the patients had undergone arthroscopic surgery for rotator cuff repair even though they did not know the arthroscopic results, and this may decrease the generalizability of our results.
In conclusion, the disproportionate fluid sign was a common finding on shoulder MRI with very high-grade bursal-sided partial thickness supraspinatus tendon tears compared with full-thickness tears. The disproportionate fluid sign could, in the setting of a visible rotator cuff tear, help in the differential diagnosis of high-grade bursal-sided tear and full-thickness tears. This would be especially helpful for less-experienced radiologists and orthopedic surgeons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.