
Abstract
Background
Wilson’s disease (WD) is a copper metabolism disorder that causes hepatolenticular degeneration. It is important to diagnose WD before central nervous system involvement.
Purpose
To demonstrate the early susceptibility changes associated with the copper accumulation in the brain of neurologically asymptomatic pediatric patients with WD using quantitative susceptibility mapping (QSM).
Material and Methods
Twelve patients with neurologically asymptomatic WD (mean age = 13.7 ± 3.3 years) and 14 age-matched controls were prospectively examined using a 1.5-T clinical scanner. Routine magnetic resonance (MR) sequences and a three-dimensional multi-echo spoiled gradient echo (GRE) sequence were used and QSM maps were reproduced. The quantitative susceptibility of corpus striatum, thalamus, substantia nigra, and pons were analyzed with the region of interest analysis on QSM maps. The susceptibility values of two groups were statistically compared using a two-sample t-test.
Results
Conventional MR images of the patients and control group were similar. However increased magnetic susceptibility in the thalamus, pons and left posterior putamen were observed in the patients compared to the control group (p < 0.05).
Conclusion
We observed statistically increased susceptibility values in the brains of neurologically asymptomatic patients with WD although the conventional MR images were normal. This might be compatible with early brain impairment, before neurological symptoms occur.
Keywords
Introduction
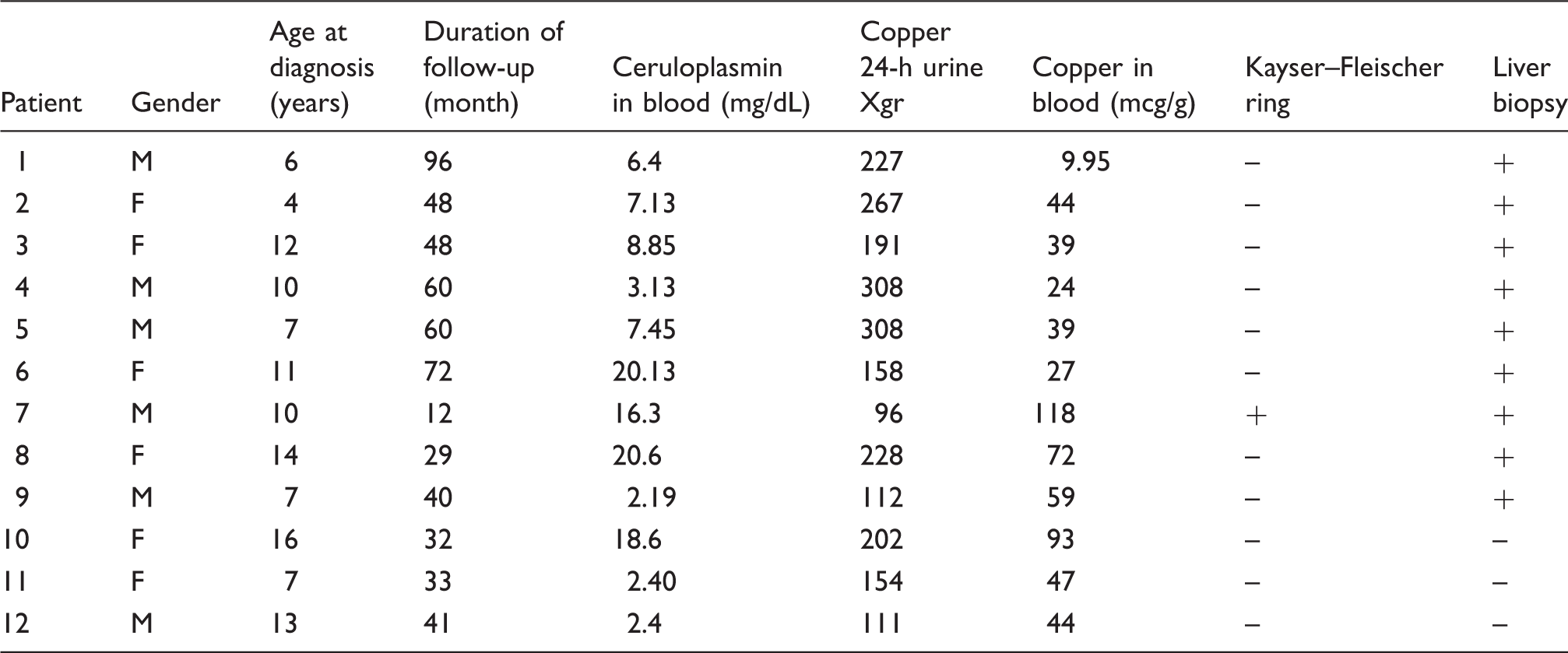
Wilson’s disease (WD) is a monogenic, autosomal recessive disorder of copper metabolism which leads to degenerations in liver and brain. WD is caused by a mutation in the ATP7B gene acting in the transportation of the copper (1–3). Owing to defective transportation, copper cannot be excreted into the bile from the liver (1,3). Copper accumulates primarily in the liver and later in the brain (4,5). This is supposed to be responsible for the pathogenesis of the disease (6–8). The peak age of presentation is 8–16 years (9). WD may onset in early infancy, as a nine-month-old case is reported in literature (10). Clinical phenotypes include hepatic, neurological, or neuropsychiatric disease. Main neurological and psychiatric symptoms in WD include dysarthria, dystonia, tremors, dizziness, lack of strength, excessive salivation, slurred speech, ataxia, bradykinesia, personality changes, anxiety, increased irritability or disinhibition, and headache. Tremor and dysarthria together strongly suggest the diagnosis of WD. WD can present as acute liver failure or chronic liver disease. Increased urinary copper in 24-h urine, the presence of Kayser–Fleischer ring, decreased serum ceruloplasmin, and copper deposition found in the liver biopsy are assessed in clinically suspected cases (11).
In patients with neurological form, conventional T2-weighted (T2W) images may show hyperintensity of globus pallidus, corpus striatum, and brain stem that correlates with the neurologic symptoms (12–15). The hyperintensity of bilateral lentiform nuclei on T1-weighted (T1W) images may be detected before neurologic impairment and is imputed to hepatic dysfunction (14,15). The magnetic resonance imaging (MRI) findings can completely regress after treatment (16).
Quantitative susceptibility mapping (QSM) is a MR post-processing technique to display tissue susceptibility. It was shown to be useful in the detection of intracranial calcification and hemorrhage (17–23) and measuring iron levels in the brain (24). Recently QSM was reported to be effective in two studies in evaluation of copper accumulation in the brains of patients with WD. Fritzsch et al. found increased susceptibility values associated with copper accumulation in patients with WD (25). Similarly, Doganay et al. showed increased tissue susceptibility in the brains of pediatric patients with neurologic WD (26).
In this study, we hypothesized that pediatric patients with neurologically asymptomatic WD might also display susceptibility changes induced by copper accumulation. These patients appear normal on conventional brain MRI. Confirming copper accumulation before neurological symptoms emerge could impact clinical treatment of WD. We aimed to quantitatively study the susceptibility values of putamen, globus pallidus, caudate nucleus, thalamus, substantia nigra, and pons of these patients, using QSM technique in comparison to the healthy controls.
Material and Methods
Patient selection
This study was approved by the institutional ethics committee. We evaluated 24 pediatric patients with WD who were followed up in the pediatric gastroenterology and neurology clinics of our institution. The diagnosis of WD was based on combinations of presence of Kayser–Fleischer ring, increased urinary copper, low serum ceruloplasmin concentration, and quantification of copper with liver biopsy (11,27,28). Two pediatric neurologists assessed that the patients were neurologically asymptomatic. Sixteen patients that had no neuropsychiatric findings (hepatic form) were included and the others were excluded due to their neuropsychiatric findings. Two pediatric radiologists evaluated their conventional brain MR images. We had to exclude four patients because of mildly hydrocephaly, slightly hyperintense basal ganglia, and unidentified small white matter hyperintensities on their brain MR images. Twelve patients with conventional MRI evaluated as normal were included in the study. The mean age of the patient group was 13.7 ± 3.3 years.
The age of the control group was selected in a similar manner to the patient group, due to age-related physiological changes. The control group included 14 children with headache complaints who applied to the pediatric neurology clinic and whose clinical evaluations were normal. The control group was age-matched to the patient group. There was no increased serum ceruloplasmin or urinary copper excretion in the control group in terms of WD. Written informed consent was obtained.
Two pediatric neurologists evaluated the patients and control group with consensus.
MRI and QSM analysis
The patients and control group were examined at 1.5-T clinical scanner (Magnetom Aera, Siemens, Erlangen, Germany) using a 20-channel neuro coil. The following were used for imaging: (i) coronal and axial T2W turbo spin echo; (ii) three-dimensional (3D) T1-weighted (T1W) magnetization prepared rapid acquisition gradient echo (MPRAGE); and (iii) axial 3D multi-echo spoiled gradient echo (GRE) sequence (T2*). The protocol parameters for the multi-echo spoiled GRE sequence were as follows: flip angle = 25°; repetition time (TR) = 80 ms; number of echoes = 5; echo times (TE) = 8.3, 16.8, 24.7, 32.7, 40.7 ms; number of slices = 64; slice thickness (ST) = 2.5 mm; field of view (FOV) = 220 × 206 mm; matrix = 192 × 154; bandwidth (BW) = 130 Hz/pixel; GRAPPA acceleration factor of 2; and acquisition time (Tacq) = 4 min 17s.
QSM images were reconstructed from multi-echo GRE images. The reconstruction procedure involved phase unwrapping, background phase removal using projection onto dipole fields (PDF) approach (27) and morphology-enabled dipole inversion (MEDI) (29,30) to reconstruct the susceptibility maps.
The images of T1 and T2 sequences of both the patient and the control group were interpreted qualitatively normal by two pediatric radiologists in consensus.
Region of interest (ROI) analysis was performed on the basal ganglia, thalamus, and brain stem; anterior and posterior of globus pallidus; anterior and posterior of putamen; caput of caudate nucleus; thalamus; substantia nigra; and the pons adjacent to the cerebral aquaduct of each side on QSM images. ROIs were drawn manually on a single slice where the ROI is best visible, using Image J software (31) by a pediatric radiologist together with an observer radiologist in consensus. Each ROI was delineated according to anatomical boundary of the interested region. An additional reference measurement was obtained in a ROI containing only cerebrospinal fluid (CSF) using an elliptical ROI inside the frontal horn of lateral ventricle. CSF measurement value was subtracted from the other measured values for referencing. The statistical analysis was done using two-sample t-test. The susceptibility measurements were compared between the patients and control group <0.05 was considered statistically significant.
Results
The mean age for the patients and the control group was 13.6 ± 3.3 years (6 boys, 6 girls; age range = 8–19 years) and 13.2 ± 2.4 years (6 boys, 8 girls; age range = 8–16 years), respectively.
Clinical features of the patients with Wilson’s disease.
No signal changes were found on conventional MRI in the patients with WD and the controls.
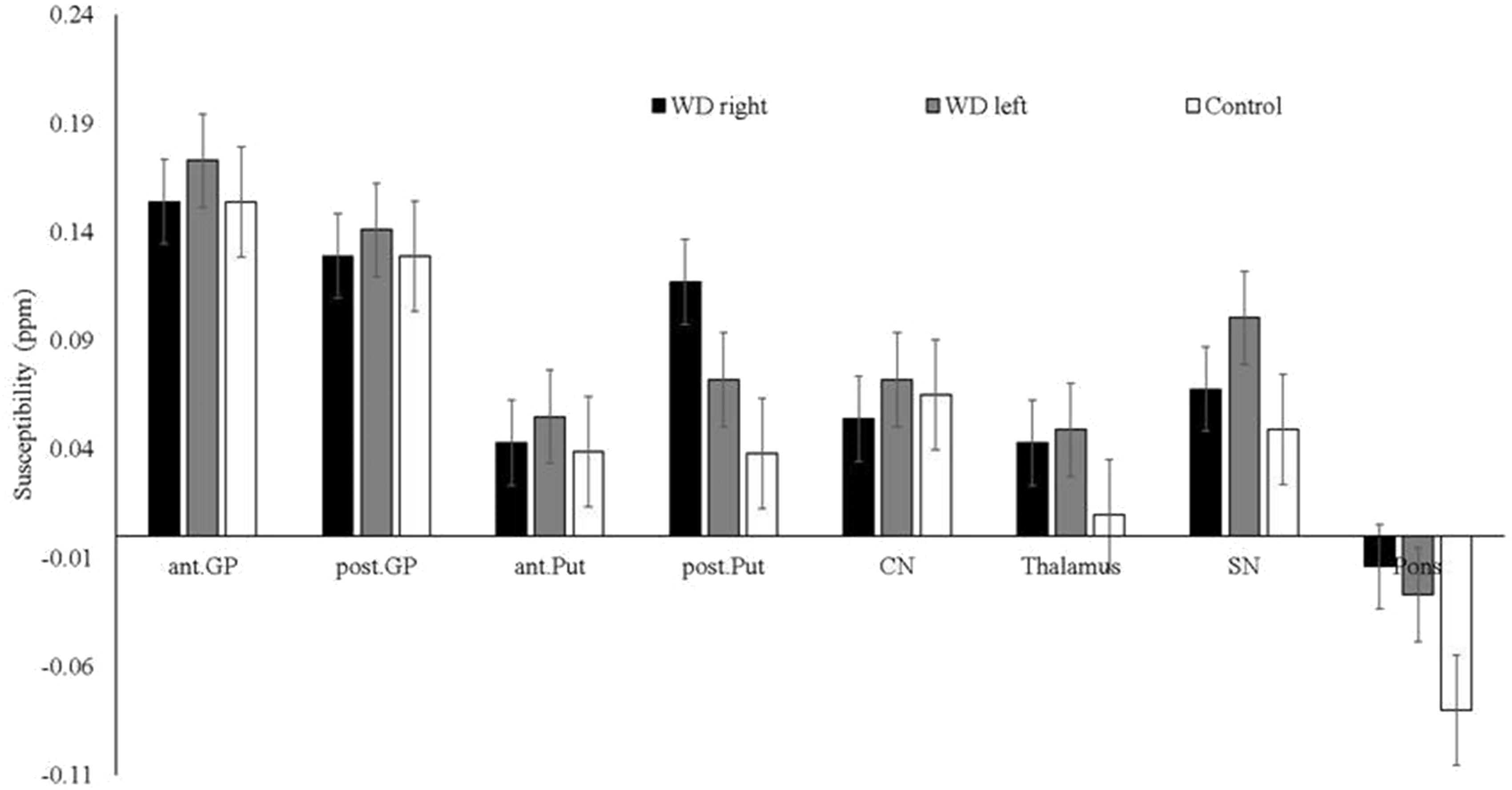
Although the patient group with WD were neurologically asymptomatic, we detected increased magnetic susceptibility in thalamus, pons, and left posterior putamen when compared with the control group (P < 0.05) (Fig. 1). No significant differences in susceptibility for the bilateral caudate nuclei, globus pallidus, and substantia nigra were found when compared to the control group (P > 0.05). The measured values of QSM maps were presented in Fig. 2.
The MR images of a 17-year-old girl with WD. (a) T2W axial image and (b) T1W axial image show normal signal intensity on bilateral caudate nuclei, putamen, and thalami. (c) QSM image shows increased susceptibility changes of bilateral, globus pallidus, putamen, and caput of caudate nuclei. But only the increased signal intensity of the thalami was statistically significant. The black arrow shows an artifact on the posterolateral of the left putamen. Susceptibility values in various regions in the right and left brains of the patients and the controls. GP, globus pallidus; Put, putamen; CN, caudate nucleus; Tha, thalamus; SN, substantia nigra.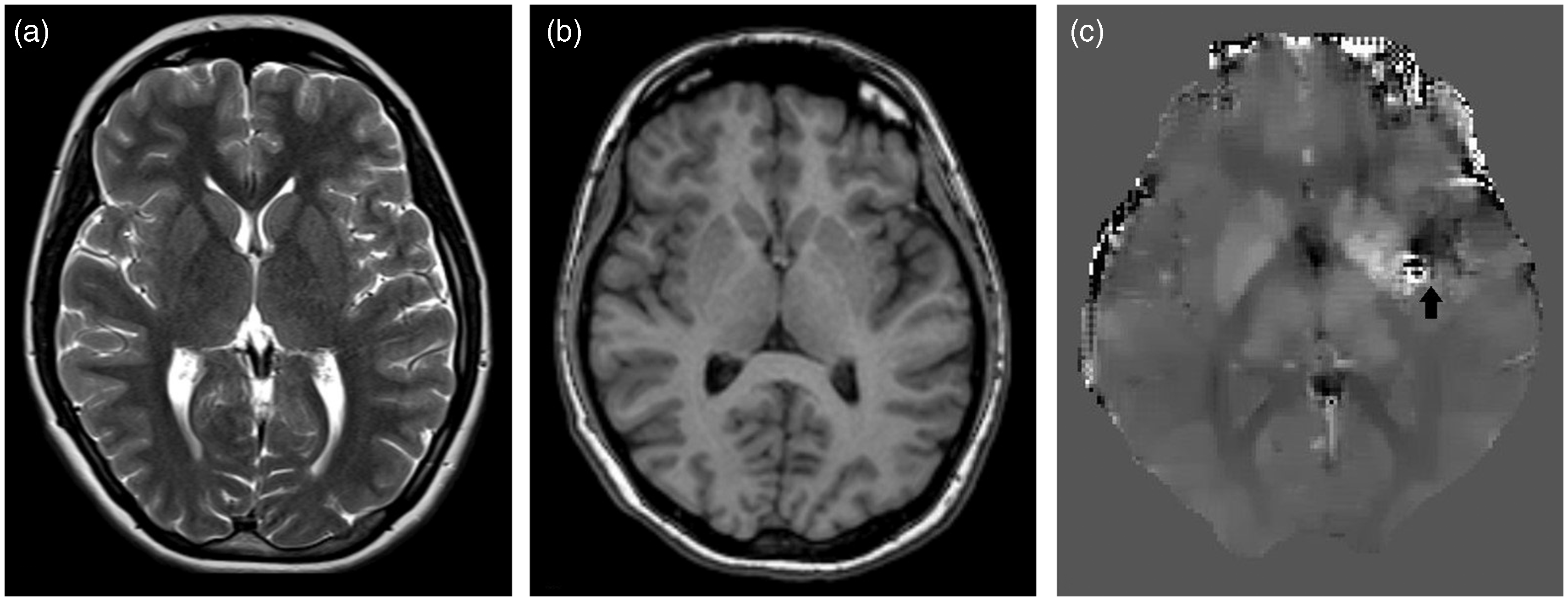
Discussion
We quantitatively evaluated the tissue susceptibility in the basal ganglia, thalamus, and brain stem of pediatric WD patients who were neurologically asymptomatic. Our study results showed that there was a statistically significant increase in the susceptibility of the pons, left posterior putamen, and thalamus in the patient group in comparison to the control group. This change was observed while there were no alterations evident on T1W and T2W MR images.
In the healthy human brain, there is a high copper level in the putamen, globus pallidus, and caudate nuclei when compared to the cerebral cortex (32). Brain copper content increases especially in the putamen and globus pallidus in WD (33). Basal ganglia and pons are the most commonly affected sites on conventional MR images. However, we found increased tissue susceptibility possibly due to copper accumulation in the thalami and pons of patients who had no neurological symptoms yet.
Susceptibility changes observed in basal ganglia and brain stem in patients with WD may be due to paramagnetic iron and copper (II) accumulation. The paramagnetic minerals change the phase of local MR signal. Tissue containing copper (II) compounds and iron are paramagnetic whereas copper and copper (I) compounds are diamagnetic (34). QSM technique made it possible to map magnetic susceptibility of brain tissue in vivo. It is a post-processing technique that inverts the phase data to magnetic susceptibility maps (27,29,30). QSM enables quantitative measurement of tissue susceptibility. The susceptibility value measured is relative to a reference region that was CSF in our analysis. Increased susceptibility value relative to the reference region generally indicates paramagnetic minerals such as iron and copper (II) compounds in the tissues. Thus, the increased susceptibility values in thalamus, pons, and putamen indicate paramagnetic minerals. Literature reports that in WD, putamen is the most frequently affected region on T2W MR images followed by the other components of the corpus striatum and thalamus (6,11–15,17).
The normal occurrence of conventional brain MR examinations of the cases in our study group was considered to be associated with a short duration of the disease. But using QSM images, increased susceptibility values were detected in pons and thalami in the patients. In literature, Fritzsch et al. showed that patients with WD had significantly increased susceptibility in basal ganglia compared with healthy controls in patients with neurological WD and with isolated hepatic WD. In our study, there were no statistically significant susceptibility changes in the basal ganglia and substantia nigra. This could be due to magnetic field strength. We used a 1.5-T MR scanner while Fritzsch et al. used a 7-T MR scanner. High field strength results in better susceptibility contrast.
MRI of WD showed symmetric hyperintensity on T2W images of basal ganglia, brainstem, cerebellar peduncles, and supratentorial white matter (5,6,35). The MRI signal changes may reflect reversible myelinolisis, cytotoxic edema, spongiform degeneration, and necrosis due to copper toxicity (4,35). In the initial stages of WD, diffusion restriction was detected in basal ganglia. In our study, we showed that statistically significant increased susceptibility in the pons, thalami, and left posterior putamen while T2W and T1W images were normal. Fritzsch et al. found a clear trend to more copper accumulation in putamen in the patients with neurological WD. In contrast there was no significant difference between the controls and the patients with hepatic WD. Perhaps the patients become neurologically symptomatic after statistically increased copper accumulation in the putamen.
This study has some limitations. First, our study group was relatively small because we evaluated only neurologically asymptomatic pediatric patients with WD. There is a need for further evaluation with larger patient groups which will make our results more meaningful. The scope of the new studies may be early detection of the copper accumulation and prevention before neurological symptoms appear. Second, we observed a signal loss artifact on a few QSM maps that partially or completely prevented ROI measurement. Lastly, we made ROI measurements on a single slice. Future studies should use 3D ROIs. We also note that using higher magnetic field strength would allow better contrast in the susceptibility maps.
In conclusion, in WD patients with no neurological symptoms, the susceptibility changes can be quantitatively measured with QSM method, before detection at conventional MRI. The increased susceptibility changes may be the early marker of brain impairment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.