
Abstract
Background
Increased pulmonary blood flow (PBF) and shear stress may provoke irreversible vascular remodeling, yet invasive visualization of the microvasculature complicates monitoring. A non-invasive imaging methodology would therefore safely provide mechanistic insights into the progression of high PBF-induced vascular remodeling.
Purpose
To establish a novel microvasculature visualization method using synchrotron radiation pulmonary microangiography (SRPA) that can also calculate PBF velocity in vivo.
Material and Methods
A high PBF rat model was established by making a fistula between the abdominal aorta and inferior vena cava. After eight weeks, SRPA was performed and the dynamic density changes in the right lower pulmonary artery (PA) were calculated by software. SRPA was performed with a HARP (High-Gain Avalanche Rushing amorphous Photoconductor) receiver. PBF velocity was calculated by contrast medium transit time within the PA. All data were presented as mean ± standard error (SE). Student's t-test was used for comparison between the two groups.
Results
High dynamic spatial and contrast resolution from SRPA in the PA allowed for clear pulmonary microangiography and accurate detection of higher PBF in the rat model (82.3 ± 8.5 mm/s high-PBF group vs. 46.1 ± 4.3 mm/s control group, P < 0.01).
Conclusions
These novel results demonstrate that SRPA was useful in both visualizing the dynamic flow distribution within the microvasculature and calculating PBF velocity. This newly developed, non-invasive technology may become a powerful tool in clarifying the mechanism of vascular remodeling associated with high PBF-induced shear stress.
Keywords
Introduction
Congenital heart disease with high pulmonary blood flow (PBF) is frequently complicated by the development of irreversible pulmonary hypertension (PH). The mechanical shear stress from the increased pressure triggers endothelial cell dysfunction and maladaptive vascular remodeling. Although this mechanism remains unelucidated, it has been reported that high pressure leads to increased vascular resistance and lesions (1–3). Therefore, a non-invasive yet accurate method is needed to evaluate the health of the vascular system in congenital heart disease presenting with high PBF.
Precise visualization of the microvasculature bed and the measurement of PBF velocity could provide critical insight into endothelial reactivity caused by the shear stress derived from high PBF. Furthermore, it may provide critical morphological details that could serve as biomarkers of the underlying molecular mechanism of vascular remodeling.
Imaging of pulmonary microvasculature can be performed using synchrotron radiation, which consists of electromagnetic waves produced when high-energy electrons that go straight at near the speed of light are bent with a strong magnetic field (Fig. 1) (4). The chief characteristic of synchrotron radiation-derived X-rays is increased photon density (up to 10,000 times higher than conventional X-rays) providing a high resolution of 12 µm per pixel with our protocol (5). Additionally, the straightness of synchrotron waves provides clear edge contrast in the target structure. These two characteristics make it possible to achieve extremely high spatial microangiographic resolution that clearly visualizes structural remodeling in the microvasculature (6). We established the usefulness of this technique in several previous reports on synchrotron radiation microangiography for coronary micro-angiography in both excised and in vivo rat hearts (5,7,8). Additionally, this technique has been used to visualize other cardiac disease pathologies, such as the acceleration of coronary microcirculatory dysfunction due to chronic intermittent hypoxia in insulin-resistant rats (9). We also reported on the extension of this modality into pulmonary microvascular imaging to investigate pulmonary emphysema and lung cancer (4,10). However, as far as we know, there are no reports of using synchrotron radiation microangiography for observation of dynamic PBF distribution of pulmonary microvasculature in a high-PBF rat model in vivo.
Synchrotron radiation.
The aim of this study is to therefore establish an in vivo method for calculating PBF velocity by using synchrotron radiation pulmonary microangiography (SRPA) in a high-PBF rat model.
Material and Methods
Animals
A high-PBF rat model system was created by making an arteriovenal fistula between the abdominal aorta and the inferior vena cava in male Wistar rats (Charles River Japan, Yokohama, Japan; n = 7). Sham-operated rats were used as a control (n = 5) (3,11). After eight weeks, SRPA was performed by transvenous infusion of 32% iodine contrast medium (2 mL/s) via the right jugular vein under general anesthesia (5,7). All animal experiments were conducted with the approval of the Institutional Animal Care and Use Committee of the University of Tsukuba. The rats used were cared for according to the Guiding Principles for the Care and Use of Animals based on the Helsinki Declaration of 1964.
Synchrotron radiation pulmonary microangiography (SRPA)
SRPA was performed at the Photon Factory of the High Energy Accelerator Research Organization (Tsukuba, Japan). Synchrotron radiation was obtained from a 6.5-GeV electron beam converted to monochromatic X-rays by a 13 ° reflection off of silicon crystal (8,12). High-contrast resolution was obtained from a high-sensitivity HARP (High-Gain Avalanche Rushing amorphous Photoconductor) detector camera (Science and Technical Research Laboratories of the Japan Broadcasting Corporation, Tokyo, Japan). HARP photoconductive film within the image pickup tube is made with amorphous selenium that converts light into an electrical signal by exploiting the avalanche multiplication phenomenon (13). The HARP camera has a resolution of 1920 × 1080 (full HD standard) on a 23 × 13 mm image sensor. This system detects even slight changes of contrast medium density making it possible to measure dynamic contrast medium changes in the distal PA within the high PBF rats.
Images were acquired using a two-dimensional recording system with 30 ms of exposure time with 3 ms between each exposure (i.e. every 33 ms) (Fig. 2). A preliminary resolution study (data not shown) indicated the smallest pulmonary arteriole that could be identified was 100 µm in diameter.
System of synchrotron radiation pulmonary microangiography with rat model. The HARP receiver is a very high sensitivity image pickup tube.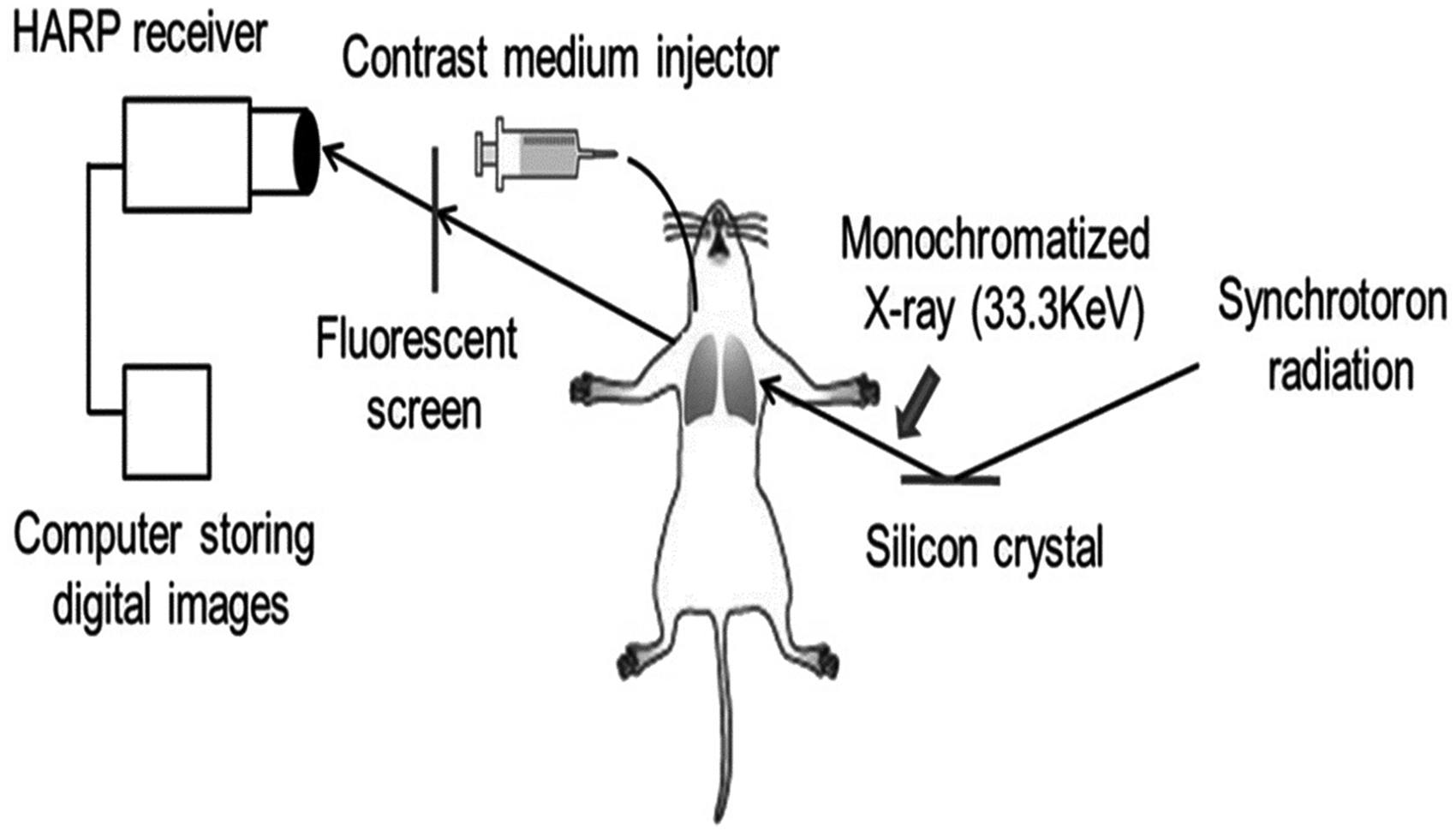
Pulmonary blood flow measurement
After eight weeks, SRPA was performed and dynamic density changes within the right lower pulmonary artery (PA) were measured by specialized software (Gray-val®, Library Co., Ltd., Tokyo, Japan). Measurements were based on transit time of the contrast medium during its first pass between two arbitrary points in the right lower PA. The distance between these two points was also measured using Gray-val®. PBF velocity was calculated by the approximation of:
Flow velocity ∝ distance (μm) / transit time (s) (Fig. 3.).
Schema of pulmonary blood flow measurement.
Statistical analysis was performed using SPSS 19.0 for Windows (SPSS Inc. Chicago, IL, USA). All data are presented as mean ± standard error (SE). Student's t-test was used for comparison between the two groups. A value of P < 0.05 was considered to be statistically significant.
Results
SRPA provided high in vivo spatial resolution in the rat model and the HARP receiver achieved enough contrast resolution to clearly detect the right lower PA and visualize the distal micro-vasculature. The smallest pulmonary arteriole thusly identified was 100 µm in diameter (Fig. 4.).
Synchrotron radiation pulmonary microangiography. The minimum identified vascular diameter was 100 μm. Bar scale indicated 1 mm. The pulmonary flow velocity of the right lower pulmonary artery measured by synchrotron radiation pulmonary micro-angiography in high pulmonary flow rat model was significantly increased compared with control.
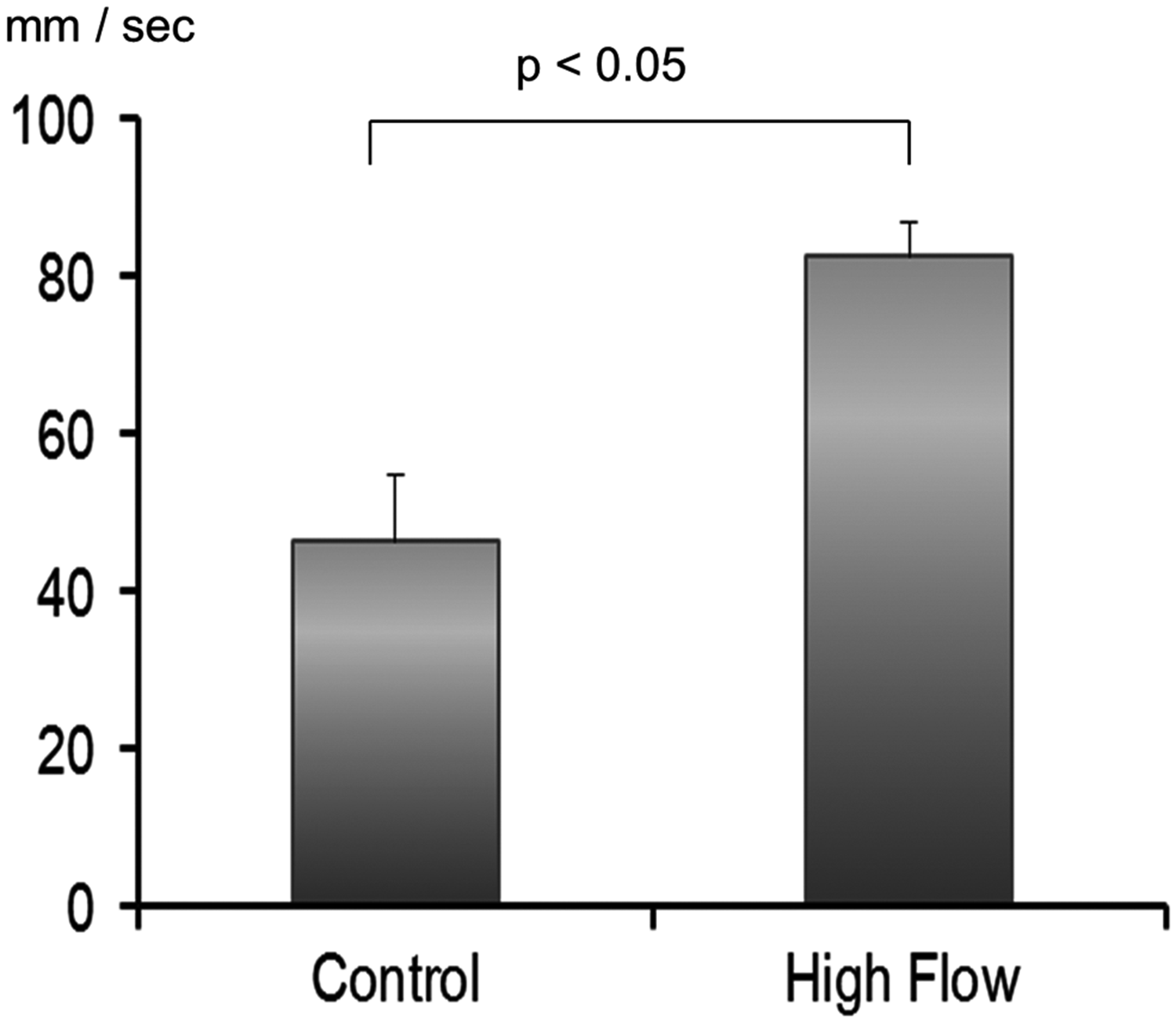
The first pass of the contrast medium through the right lower PA was measured by software and the estimated velocity of the PBF in the high-PBF rats was significantly increased compared to controls (82.3 ± 8.5 mm/s vs. 46.1 ± 4.3 mm/s, P < 0.05) (Fig. 5).
Discussion
The key findings of this study were that SRPA allowed both visualization of dynamic PBF distribution within the pulmonary microvasculature and detection of increased PBF at the distal pulmonary circulation in the high-PBF rat model. This result may also suggest increased microvascular shear stress in the high-PBF rats and is, to the best of our knowledge, the first report of its kind to demonstrate this finding.
Conventional pulmonary angiography is not sensitive enough to visualize low-contrast structures whereas the HARP receiver, by virtue of avalanche multiplication, detected diluted, low-contrast medium in the distal microvasculature (13). With the combined use of synchrotron radiation and the HARP receiver, the PBF velocity could be calculated using the estimated transit time of contrast medium during its first pass and the distance between two points in the right lower PA in the rat model.
However, one disadvantage to SRPA is radiation exposure. The measured surface dose for HARP angiography was 9.36mGy/s (5) and single-shot SRPA needs at least 2–3 s to capture 60–90 frames. Thus, estimated radiation exposure is 18.72–28.02mGy. With respect to the tolerable radiation limit, if the acceptable absorbed dose in one angiography session is assumed to be 1 Gy, the SRPA single-shot radiation exposure falls within that range.
Mechanistically, expression levels of endothelial nitric oxide synthase (eNOS) and vascular endothelial growth factor (VEGF) have been reported to be significantly enhanced in high PBF-induced PH (1,3). This upregulation of eNOS and VEGF suggests ongoing tissue remodeling in PA exposed to high flow and shear stress (1,3) and subsequent pathological changes, including intimal hyperplasia, medial hypertrophy, and the formation of plexiform lesions in the microvasculature, are mediated by this process (14). However, the stepwise progression of vascular remodeling due to high PBF-induced PH is still unclear because invasive histological diagnosis is presently the only method for detecting the progression of the disease.
Here, we tested a newly developed technology, SRPA/HARP, that can less invasively visualize complex vascular remodeling at the temporal level to delineate the progression of disease. Therefore, this imaging technology could be a useful tool to study the correlation between vascular remodeling and high PBF-induced shear stress. As an intractable disease, PH mortality remains high in spite of various receptor-based therapies (15,16) and therefore pathological assessment by SRPA could become a powerful tool to evaluate both pharmacological efficacy and novel drug interventions against PH.
There was a limitation in our study. PBF velocity measured by SRPA is calculated by both distance and transit time and assumes that the blood vessel is parallel to the HARP detector. Therefore, there is the potential that we only measured the PBF velocity in a limited direction. However, we present our results as foundational evidence that highlights estimated PBF velocity differences in PH and supports the usefulness of SRPA as a new modality to investigate the dynamic PBF distribution within the pulmonary microvasculature.
In conclusion, the results obtained in this pilot study serve as an in vivo proof-of-concept for using SRPA/HARP to visualize PBF distribution and measure PBF velocity in the pulmonary microvasculature. This powerful and newly developed technology may therefore prove useful in mechanistic investigations into vascular remodeling associated with high PBF-induced shear stress and PH.
Footnotes
Acknowledgments
The authors thank Dr. Bryan J. Mathis of the Medical English Communication Center, University of Tsukuba, for the language review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by JSPS KAKENHI (Grant no. 23791560).