
Abstract
Background
Elastography has been introduced as an additional diagnostic tool to ultrasonography (US) which helps clinicians decide whether or not to perform biopsy on US-detected lesions.
Purpose
To evaluate the role of strain elastography in downgrading Breast Imaging Reporting and Data System (BI-RADS) category 4a breast lesions according to personal risk factors for breast cancer in asymptomatic women.
Material and Methods
Strain elastography features of a total of 255 asymptomatic category 4a lesions were classified as soft and not soft (intermediate and hard). Malignancy was confirmed by surgery or biopsy, and benignity was confirmed by surgery or biopsy with no change on US for at least six months. Malignancy rates of lesions with soft and not soft elastography were calculated according to the presence of risk factors.
Results
Of 255 lesions, 25 (9.8%) were malignant and 230 (90.2%) were benign. Of 195 lesions in average-risk women, the malignancy rate of lesions with soft elastography was 1.5% (1/68), which was significantly lower than the 14.2% (18/127) of lesions with not soft elastography (P = 0.004). Of 60 lesions in increased-risk women, the malignancy rate of lesions with soft elastography was 15.0% (3/20), which was not significantly different from the 7.5% (3/40) of lesions with not soft elastography (P = 0.390).
Conclusion
In average-risk women, category 4a lesions with soft elastography could be followed up with US because of a low malignancy rate of 1.5%.
Introduction
Screening ultrasonography (US) is widely performed for dense breasts and this common practice has resulted in an increasing number of false-positive cases as more American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS) category 3 lesions are followed up for a short period of time and as more category 4 lesions undergo biopsies (1,2). Category 4 lesions are further classified by BI-RADS into the 4a, 4b, and 4c subcategories (3,4). The recommended malignancy rate of BI-RADS category 4a lesions is 2–10%, thus, most biopsy results are benign (5). To reduce the number of false-positive cases, elastography has been introduced as an additional diagnostic tool to B-mode US which helps clinicians decide whether or not to perform biopsy on US-detected lesions (6–13). Several studies have evaluated the additional value of elastography in downgrading BI-RADS category 4a lesions detected on US and its effect on reducing the number of unnecessary biopsies being performed (11–16). In one small series study, none of the BI-RADS category 4a lesions detected on US with soft elastography features was malignant; therefore, they could be managed with follow-up instead of biopsy (11). Other studies also showed that elastography increased specificity when downgrading BI-RADS category 4a lesions and that its addition allowed patients to avoid unnecessary benign biopsies (12–16). However, biopsy is currently performed for all BI-RADS category 4a breast lesions in daily clinical practice.
To our knowledge, there has been no study on the malignancy rate of BI-RADS category 4a lesions according to the existence of concurrent breast cancer. However, the malignancy rate of BI-RADS category 3 lesions has been shown to differ according to the presence of concurrent breast cancer and its location (17). In a previous study, the malignancy rate of category 3 lesions with concurrent breast cancer was overall 11.4%, with 16.4% in the ipsilateral breast and 4.2% in the contralateral breast, and these values were > 2% (17). Variations occurred because every woman undergoing screening US has different risk factors for breast cancer. To our knowledge, no study has yet evaluated the role of elastography in the assessment of BI-RADS category 4a lesions in asymptomatic women according to risk factors for breast cancer.
In this study, we evaluated the role of strain elastography in downgrading BI-RADS category 4a breast lesions according to personal risk factors for breast cancer in asymptomatic women.
Material and Methods
The Institutional Review Board approved this retrospective study and required neither patient approval nor informed consent for our review of patient images and medical records.
Study population
From June 2014 to October 2015, 719 breast lesions assessed as BI-RADS category 4a in 630 women underwent elastography before core needle biopsy (CNB) or vacuum-assisted biopsy (VAB) in our institution. Of these, 344 symptomatic lesions, 113 lesions with benign pathology without surgery or at least six months of follow-up US after biopsy, and seven lesions in patients who had undergone ipsilateral breast surgery and radiation therapy were excluded. Finally, 255 asymptomatic lesions assessed as BI-RADS category 4a in 223 women who underwent surgery or at least six months of follow-up US after biopsy were included in this study (Fig. 1). Among them, 19 women had two lesions, five had three lesions, and one had four lesions. Mean patient age was 46.1 ± 9.7 years (age range = 20–79 years). Mean lesion size was 10.0 ± 5.5 mm (age range = 3–44 mm).
Diagram of the malignancy rates of the 255 BI-RADS category 4a lesions according to risk factors and elastography.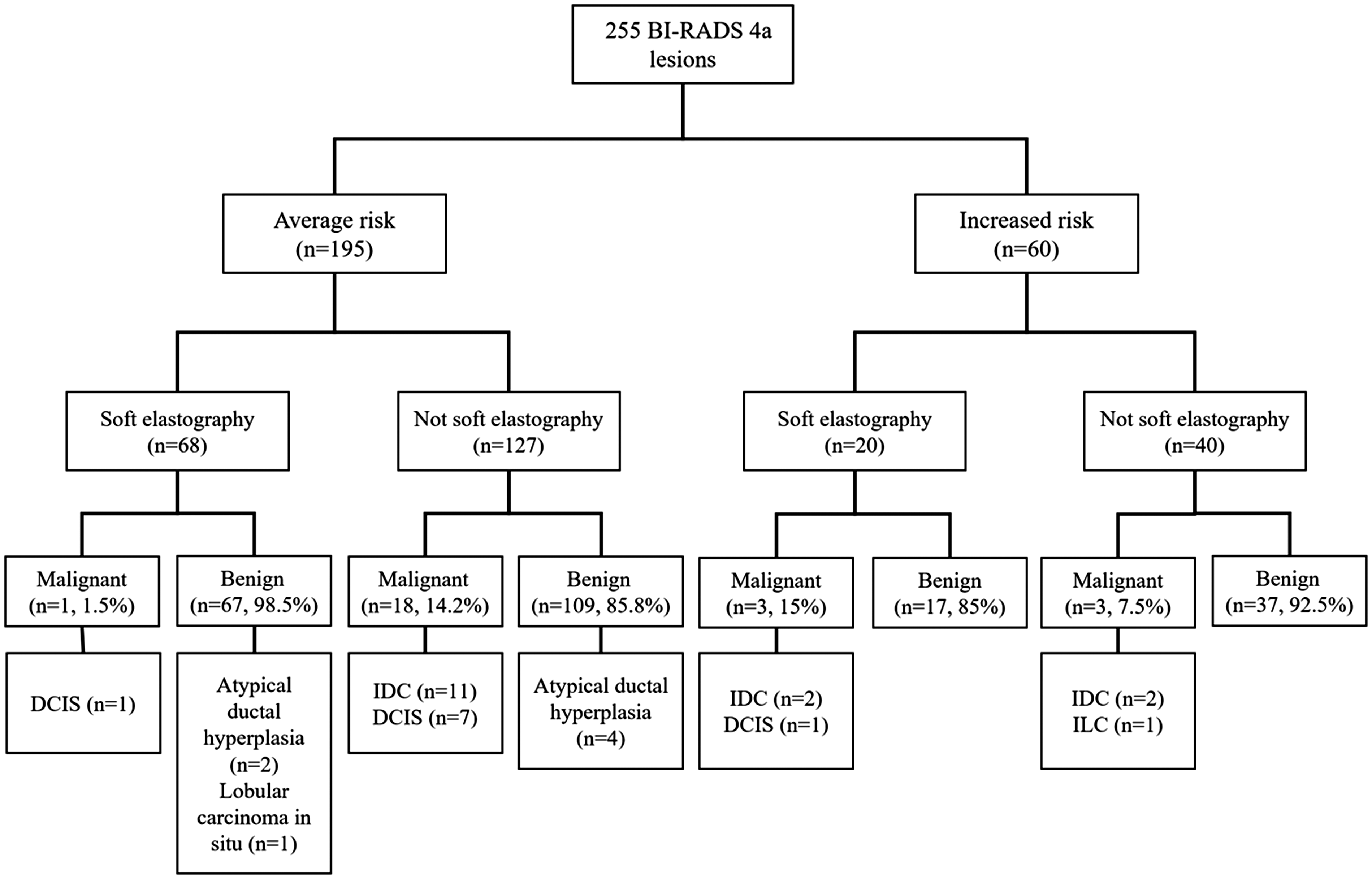
After reviewing the medical records, risk factors for breast cancer, including a personal history of breast cancer, first-degree relatives with breast cancer history, a personal history of atypical ductal hyperplasia or lobular neoplasm, and presence of the BRCA1 or BRCA2 mutation were recorded. When any of the risk factors were present, women were regarded to be at increased risk for developing breast cancer. Women without risk factors were regarded to be at average risk. Forty-seven women with 60 lesions (23.5% of 255) were considered to be at increased risk and were classified into the increased risk group. Eight women with ten lesions had a past history of contralateral breast cancer, 26 women with 35 lesions had concurrent contralateral or ipsilateral breast cancer, nine women with 11 lesions had a first-degree relative with breast cancer history, two women with two lesions had a history of atypical ductal hyperplasia, and one had a history of lobular carcinoma in situ. One woman with a personal history of breast cancer also had the BRCA2 mutation. The remaining 176 women with 195 lesions (76.5% of 255) were considered to be at average risk and were classified into the average-risk group.
B-mode US and elastography
B-mode US and elastography were performed with either a 5–12-MHz linear transducer (iU22; Philips Medical Systems, Bothell, WA, USA) or a 6–15-MHz transducer (LOGIQ E9; GE Healthcare, Milwaukee, WI, USA) by one of 14 board-certified radiologists dedicated to breast imaging with 1–21 years of experience. Both B-mode US and elastography findings were prospectively recorded. On B-mode US, breast lesions were analyzed according to the BI-RADS criteria and a BI-RADS category was finally assigned (4). Category 4a was assigned when there were one or more minor suspicious findings, such as round shape, uncircumscribed margin, non-parallel orientation, ductal extension, complex echogenicity, and posterior shadowing (18). Strain elastography was performed before any biopsies by the same radiologist who performed CNB or VAB with the same US unit. A square region of interest was drawn at the target lesion including the subcutaneous fat layer to the pectoralis major muscle, and the probe was positioned perpendicular to the skin. Light contact without manual compression was applied with the Philips machine and minimal repetitive compression was applied with the GE machine above the targeted breast lesion during elastography (19). For optimal elastography acquisition, we continued imaging acquisition until the color of the entire target was completely stable, and the compression bar in the Philips machine or the quality graph and quality bar in the GE machine were monitored (19,20). With the split-screen mode, gray-scale US images were displayed on the left and corresponding elastography images were displayed on the right. Elastography images were displayed with 256 colors for each pixel ranging from a color spectrum of red to blue; the softest component was displayed in red and the stiffest component in blue. Elasticity scores were recorded according to the BI-RADS lexicon as soft, intermediate, and hard (4,21). A BI-RADS category 4a lesion was dichotomized as “soft” and “not soft,” with a soft lesion having a soft elasticity score, and a not soft lesion having an intermediate or hard elasticity score.
Core-needle biopsy, vacuum-assisted biopsy, surgery, and follow-up
Of the 255 BI-RADS category 4a lesions, surgery was performed on 61 (23.9%) lesions because of malignant biopsy results (n = 20), because they were increased risk or borderline risk lesions (n = 35) or benign lesions in concurrent breast cancer (n = 4), and at patient request (n = 2). VAB was performed in 45 (17.6%) lesions after CNB to remove small intraductal papilloma, sclerosing adenosis, or radial scars (n = 30) or to remove benign lesions at the request of the patient or physician (n = 15). One lesion assessed as atypical ductal hyperplasia on VAB underwent surgery. One hundred and forty-nine lesions (58.4%) were followed up with US after CNB. US-guided CNB was performed with at least five passes using a 14-gauge dual-action semi-automatic needle with a 22-mm throw (Stericut with coaxial; TSK Laboratory, Tochigi, Japan). US-guided VAB was performed to remove the entire visible lesion with an 11-gauge or 8-gauge needle (Mammotome; Ethicon Endo Surgery, Cincinnati, OH, USA) or with a 12-gauge or 9-gauge needle (Atec; Hologic, Indianapolis, IN, USA).
Data and statistical analysis
Breast lesions with malignant results at surgery, CNB, or VAB were considered malignant. Breast lesions with benign or increased risk results at surgery were considered benign. If a benign lesion at CNB or VAB showed no change on US after at least six months of follow-up US, it was considered benign. Malignancy rates were calculated and compared according to elastography features and according to the presence of risk factors. Categorical variables were analyzed by the Chi-square test and Fisher’s exact test. Statistical analysis was performed using SPSS® statistical software, ver. 20.0 (SPSS Inc., Chicago, IL, USA). A two-sided P value < 0.05 was considered statistically significant.
Results
Clinicopathologic and elastography results of the 255 BI-RADS category 4a lesions.
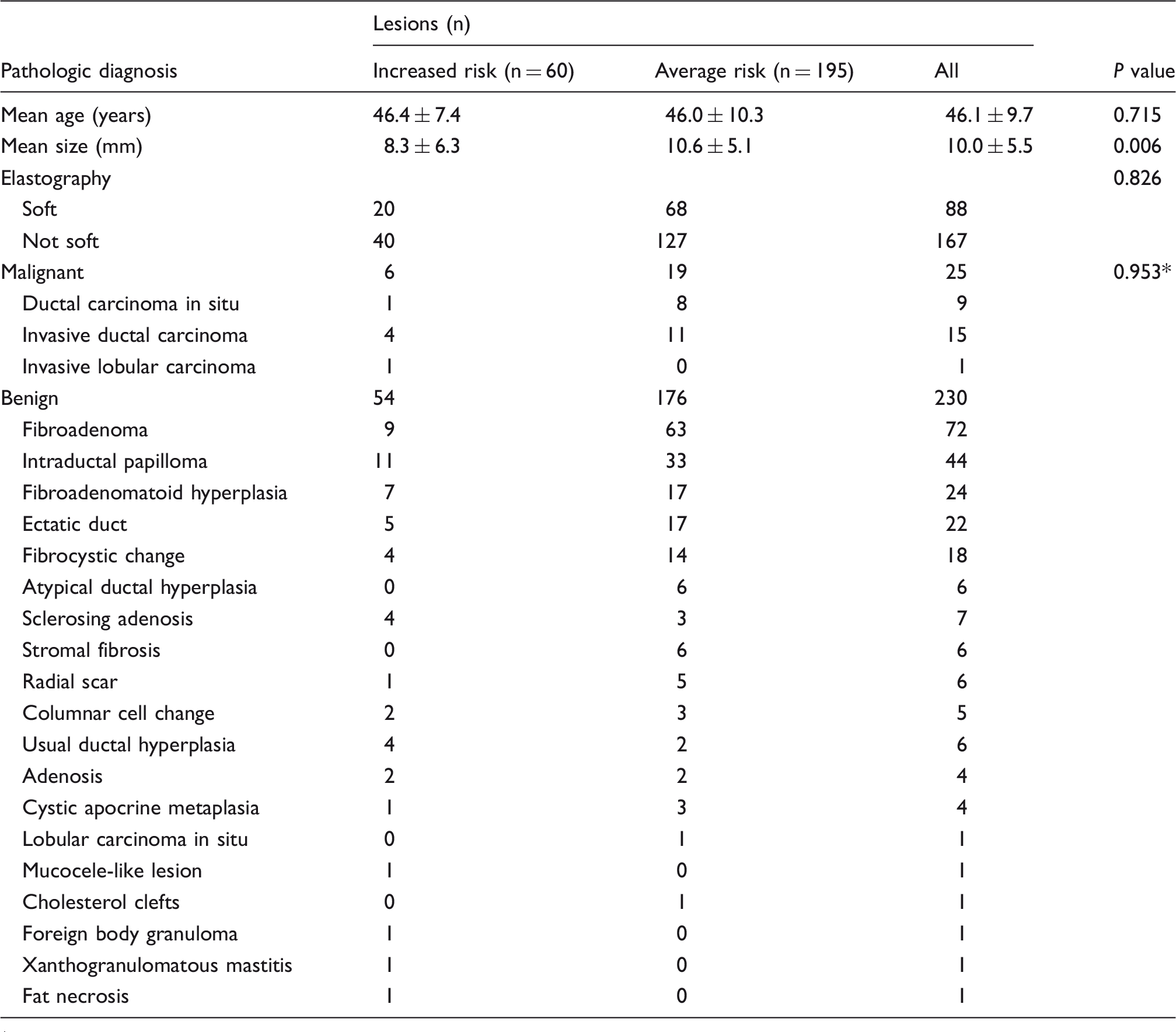
P value was calculated by comparing benign and malignant lesions in the increased-risk and average-risk group.
BI-RADS, Breast Imaging Reporting and Data System.
Of 195 lesions in average-risk women, 68 (34.8%) showed soft elastography and 127 (65.1%) showed not soft elastography (Fig. 1). The malignancy rate of lesions with soft elastography in average-risk women was 1.5% (1/68) and the single case was ductal carcinoma in situ (DCIS), significantly lower than the 14.2% (18/127) of lesions with not soft elastography (P = 0.004) (Fig. 2). Of 67 benign lesions with soft elastography, two were atypical ductal hyperplasia (ADH) and one was lobular carcinoma in situ. Of 109 benign lesions with not soft elastography, four were atypical ductal hyperplasia (P > 0.999). One ADH with not soft elastography found at VAB was < 1 mm in size and was followed up, while the other high-risk lesions were excised.
A 39-year-old woman without risk factors had a 5-mm-sized category 4a nodule in her right breast in the 10 o’clock direction (arrow). The lesion showed soft elastography. Core needle biopsy was performed and the result was a radial scar. The lesion was subsequently removed by vacuum-assisted excision and fibroadenomatoid hyperplasia was confirmed. She was followed up for 18 months without residual lesions.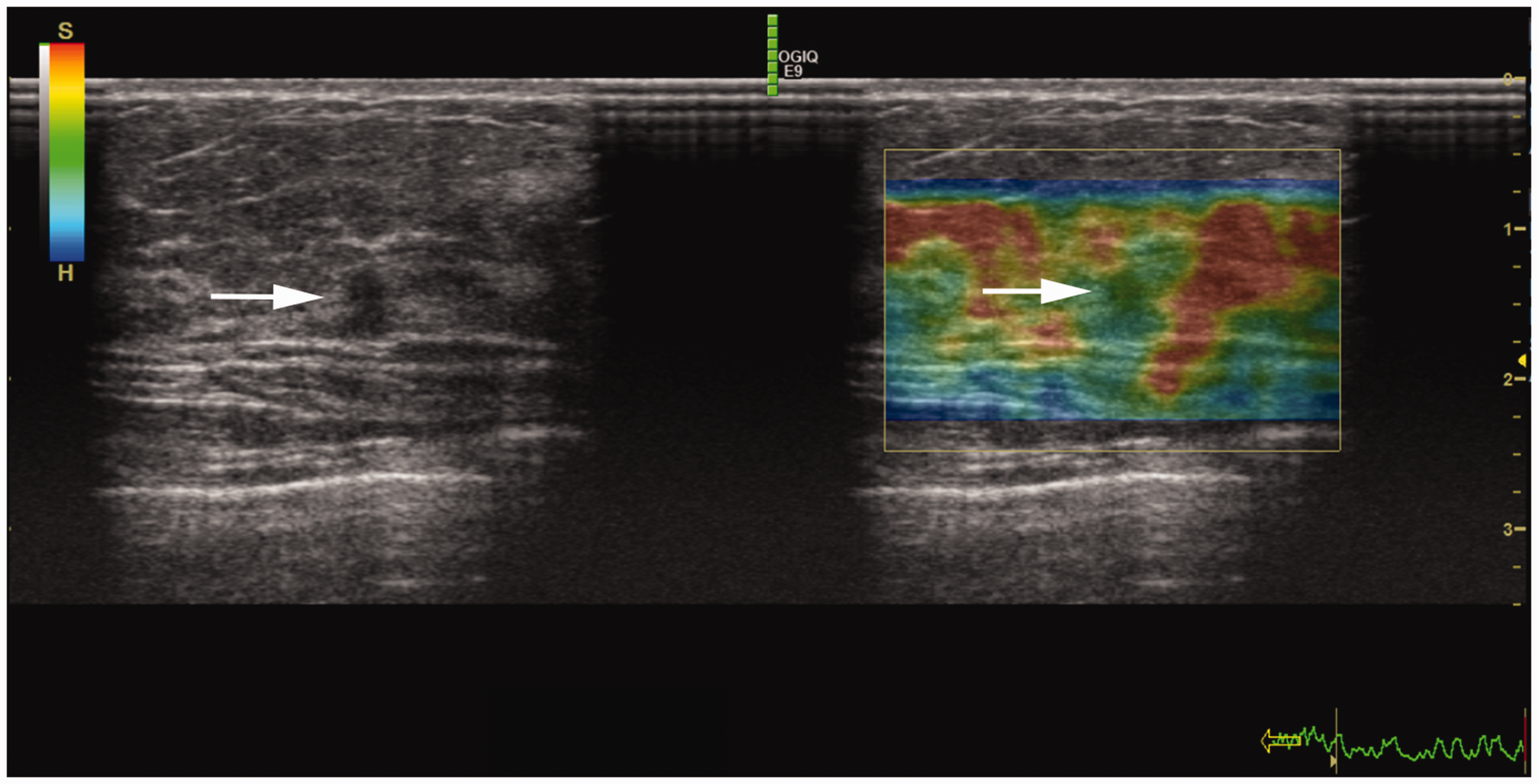
Of 60 lesions in increased risk women, 20 (33.3%) showed soft elastography and 40 (66.7%) showed not soft elastography. All six malignancies in increased women were found in patients with concurrent breast cancer at the time of diagnosis. The malignancy rate of lesions with soft elastography in increased risk women was 15.0% (3/20), which was not significantly different from the 7.5% (3/40) of lesions with not soft elastography (P = 0.390) (Fig. 3). Eleven lesions in nine patients with family history or gene carriers were all benign: six lesions were soft on elastography and five were not soft. In increased risk women, there were no high-risk lesions among any of the lesions with soft and not soft elastography.
A 60-year-old woman with a past history of breast cancer in her left breast. B-mode US showed a 6-mm-sized category 4a lesion which showed soft elastography (arrow). Core needle biopsy was performed and the result was atypical ductal hyperplasia. The final pathology result from excision was ductal carcinoma in situ.
Discussion
BI-RADS category 4a lesions with soft elastography in average-risk women can be followed up with US due to a low malignancy rate of 1.5%. However, with a malignancy rate of 14.2%, BI-RADS category 4a lesions with not soft elastography in average-risk women should undergo biopsy. In increased risk women, we would cautiously recommend follow-up for BI-RADS category 4a lesions because those with soft elastography and not soft elastography have malignancy rates of 15% and 7.5%, respectively. Mean lesion size in the average-risk group was significantly larger than the increased-risk group and also in malignant lesions. This difference in size might have influenced the elastography findings, but as the mean size of the malignant lesions in both groups was < 10 mm, the effect of differing size is thought to be minimal.
Screening US has been extensively performed since numerous breast-density laws were passed in the United States (22–24). One of the main issues with screening US being commonly performed is false-positive results and the consequent increase in health costs and patient anxiety (25,26). The main source of false-positive results is category 3 or 4a assessments. Because of a high incidence of 8.5–27.5% but a malignancy rate of < 1% for category 3 lesions (27–29), 12 months of follow-up has been suggested instead of six months in the screening setting (30). Also, category 4a assessment in asymptomatic women comprises 7.8–9.4% of cases (28,31). The malignancy rate of BI-RADS category 4a lesions in asymptomatic women has been reported to be in the range of 4.8–6.5% (31,32). Assessing a lesion as BI-RADS category 4a leads to the most unnecessary benign biopsies being performed and false-positive results. In our study, the malignancy rate of BI-RADS category 4a lesions was 9.4%. In other words, approximately 90 benign biopsies were performed to find ten cancers. In average risk women, BI-RADS category 4a lesions with soft elastography had a low malignancy rate of 1.5% and BI-RADS category 4a lesions with not soft elastography had a malignancy rate of 14.2%. The pathology of malignancy in average-risk women with soft elastography was DCIS. Thus, in average-risk women, elastography could differentiate which BI-RADS category 4a lesions should undergo biopsy and which lesions should be followed up with US. In increased-risk women, the malignancy rate of BI-RADS category 4a lesions was 10%, which was comparable with the 9.7% in average-risk women. However, the malignancy rate of BI-RADS category 4a lesions with soft elastography and BI-RADS category 4a lesions with not soft elastography was 15% and 7.5%, respectively. Our results meant that elastography had no role in differentiating BI-RADS category 4a lesions in increased-risk women and that BI-RADS category 4a lesions in these women should undergo biopsy regardless of elastography features.
Elastography has been used to downgrade BI-RADS category 4a lesions in previous studies (11–13,15,16,33). Au et al. used shear-wave elastography (SWE) to downgrade 90% of 44 BI-RADS category 4a lesions to category 3 (13). Although individual risk factors or symptoms were not considered in their analysis, the study showed that elastography could play a role in differentiating BI-RADS category 4a lesions with follow-up (13). Lee et al. also performed SWE in asymptomatic women and found specificity to be significantly improved when downgrading BI-RADS category 4a lesions, but the exact percentage of increased-risk women was not available (15). Ko et al. applied SWE to 19 BI-RADS category 4a non-mass lesions and reported that 79% of unnecessary biopsies could be avoided with its addition to US, while more than half of the study population was symptomatic, individual risk factors were also not evaluated (16). Youk et al. compared SWE and strain elastography and 56% and 38% of category 4 lesions were downgraded to category 3 with both elastography techniques showing similar diagnostic performance (12). There was also no information on symptoms or risk factors in Youk’s study (12). Another study with strain elastography reported that none of the non-palpable BI-RADS category 4a lesions with soft elastography showed malignancy; thus, follow-up was suggested for these lesions (11) even though 4% of the lesions had nipple discharge and individual risk factors were not considered in analysis (11). None of the prior studies applied criteria which differed according to individual risk factors when downgrading BI-RADS category 4a lesions. Although the rate of downgrading BI-RADS category 4a lesions through addition of elastography varied from study to study, all studies showed that elastography could downgrade BI-RADS category 4a lesions into category 3 (11–13,15,16). However, BI-RADS categories can be assessed differently depending on which risk factors are present, a subject discussed in a prior study with BI-RADS 3 lesions with concurrent breast cancer which showed a malignancy rate > 2% (11). Through our study, we hoped to reduce the number of benign biopsies by applying individual risk factors through strain elastography to downgrade BI-RADS category 4a lesions. We found that BI-RADS category 4a lesions can be differently downgraded according to individual risk factors in asymptomatic women.
There were several limitations in our study. First, with its retrospective design, a selection bias might exist. Second, benign lesions without at least six months of follow-up US were excluded, and if we take into consideration that most of these women were probably followed up at the hospital where they were first referred from and that lesions in these women were most likely benign, this might have caused an overall overestimation of the malignancy rate. However, as the malignancy rate in average risk women with soft elastography would also have been lowered, the general conclusions of our study are thought to be the same. Third, there might have been false-negative results in the biopsied lesions and six months of follow-up might not be long enough to confirm their existence. Therefore, a study with long-term follow-up is needed to generalize our results to clinical practice. Fourth, elastography was performed by several radiologists with variable experience levels. Inter-observer variability was not evaluated and could impact our results. However, we tried to reduce inter-observer variability through discussions at our weekly conference. Fifth, we used a heterogeneous definition for the increased risk group in this study. There are several established risk factors for developing breast cancer and various models have been studied (34–36). Thus, differing definitions for these risk factors would influence the study results. We could not consider all possible risk factors in this study due to its retrospective nature, and simply used a personal history of breast cancer or familial breast cancer. Therefore, further studies need to be performed to confirm the role of elastography in various subsets of risk factors.
In conclusion, in average risk women, BI-RADS category 4a lesions with soft elastography could be followed up with US because of a low malignancy rate of 1.5%.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.