
Abstract
Background
The diagnosis of a tumor depends on accurate identification of the target area for biopsy. However, tumor heterogeneity and the inability of conventional structural data for identifying the most malignant areas can reduce this accuracy.
Purpose
To evaluate the feasibility and practicality of magnetic resonance spectroscopy (MRS)- and arterial spin labeling (ASL)-guided MRI navigation for needle biopsy of intracranial tumors.
Material and Methods
Thirty patients with intracranial tumors who underwent intraoperative stereotactic biopsy were retrospectively analyzed. Contrast-enhanced 3D-BRAVO or 3D-T2FLAIR structural data, combined with MRS and ASL data, were used to identify the target area for biopsy. High-choline or high-perfusion sites were chosen preferentially, and then the puncture trajectory was optimized to obtain specimens for histopathologic examination.
Results
Twenty-two specimens were collected from 20 glioma patients (two specimens each were collected from two patients) and ten specimens were collected from ten lymphoma patients. The diagnosis rate after the biopsy was 93.3% (28/30). Two gliomas were initially diagnosed as gliosis and subsequently diagnosed correctly after the collection of a second biopsy specimen. Combined MRS and ASL helped target selection in 23 cases (76.7%), including three cases each of low-enhancing and non-enhancing gliomas. In two cases, the target selection decision was changed because the areas initially chosen on the basis of positron emission tomography data did not match the high-perfusion areas identified with ASL.
Conclusion
Compared with conventional MRI, combined MRS and ASL improved the accuracy of target selection for the stereotactic biopsy of intracranial tumors.
Introduction
The management of intracranial tumors depends on their histopathological subtype, which can be quickly and safely established via needle biopsy (1). However, tumors are heterogeneous masses consisting of a complex mixture of normal, inflammatory, and tumor tissues (2), and a single tumor may contain areas of different histopathological grades. Stereotactic biopsy can be used to target specific tumor areas, but biopsies mostly depend on contrast enhancement, which can result in the “under-grading” of as many as 30% of intracranial tumors (3). The diagnostic accuracy could be improved by multiple tissue samplings, but this method would also increase the risk of complications such as cerebral hemorrhage and neuronal damage (4,5). Various imaging modalities have been used to identify the target tumor area for biopsy, but all of these have certain disadvantages. Conventional magnetic resonance imaging (MRI) techniques, such as gadolinium-enhanced T1-weighted (Gd-T1W) imaging, are commonly used for navigation guidance, but low-grade gliomas (LGGs) usually show little or no enhancement, and even high-grade gliomas (HGGs) occasionally demonstrate no enhancement (6). The T2-weighted fluid-attenuated inversion recovery (T2 FLAIR) sequence may be used to guide biopsy in non-enhancing tumors, but it is not a tumor-specific sequence because peritumoral edema may obscure the precise tumor location. Furthermore, those sequences only reflect the degree of blood–brain barrier disruption and demonstrates the tumor location; they do not provide metabolic information or indicate the degree of malignancy (7). Positron emission tomography (PET)–MRI, which displays molecular metabolism, is very useful for target selection, but high cost and exposure to ionizing radiation are major limitations. New techniques that use multimodal functional imaging that can reflect specific tumor characteristics are now available. Magnetic resonance spectroscopy (MRS) can reflect the tumor metabolism and biological tumor characteristics without the use of tracers or contrast agents (8), and in combination with conventional imaging, it can effectively identify the tumor type and predict the glioma grade (9). However, the baseline of MRS scan is influenced by factors such as cerebrospinal fluid, the skull, and motion artifacts. Moreover, multi-voxel MRS cannot be applied in patients with multiple lesions due to time limitation, as it is difficult to visualize all lesions in the same plane. Dysfunctional vascularity is an indicator of high malignancy (10). Arterial spin labeling (ASL) is a non-invasive technique that uses free water protons in the arterial blood as an endogenous tracer to quantify blood flow within the lesion, and it has been used to assess the microvascular density of glial tumors and quantify tumor regions with abnormally elevated perfusion (11,12). However, ASL usually shows an area of high perfusion whose volume is obviously larger than that of the biopsy needle tip; this reduces the accuracy of biopsy. Multi-voxel 1H-MRS can locate a single lesion with multiple voxels and is therefore a perfect complement to ASL.
We hypothesized that combining the two modalities—MRS and ASL—could reduce the sampling error during the biopsy of intracranial tumors. The aim of this study was to determine the efficacy of combined MRS and ASL guidance for stereotactic biopsy of intracranial tumors.
Material and Methods
Patients
This study was approved by the ethics committee of our hospital. Informed consent was obtained from all patients. Patients were eligible for inclusion if they: had an intracranial tumor; and were aged 12–80 years.
From October 2016 to December 2017, 30 patients (16 men, 14 women; age range = 12–75 years; mean age = 47.2 years) with intracranial tumors were retrospectively analyzed. For further clinical management, stereotactic biopsy was performed for all patients for the following reasons: (i) in 16 patients, the clinical features and imaging data were atypical, and the tumor type (glioma vs. lymphoma) and tumor grade (mainly in the case of gliomas) needed to be confirmed; (ii) in 17 patients, the lesions were located in important functional areas (e.g. the precentral gyrus and brainstem), and complete tumor resection would have led to functional impairment or serious complications; and (iii) in 15 patients with multiple lesions, complete surgical resection was not feasible.
MRI
A 3.0-T MR system (Discovery MR750, GE Medical Systems, Milwaukee, WI, USA) with an eight-channel phased array coil was used for imaging. Every patient underwent preoperative conventional MRI and functional MRI (including multiple-voxel 1H-spectroscopy and ASL sequence). Three-dimensional (3D) contrast-enhanced T1W imaging (3D-brain volume imaging) or contrast-enhanced T2 FLAIR was performed after contrast injection. The contrast agent was gadolinium-diethylenetriamine penta-acetic acid (Gd-DTPA; 1 mmol/L; Omniscan; GE Healthcare, Co. Cork, Ireland). Gd-DTPA (0.1 mmol/kg) was injected via an intravenous catheter at a flow rate of 3 mL/s using a power injector and was followed by a 20-mL saline flush at the same flow rate. ASL sequence (using a pseudocontinuous pulse sequence) was performed with the following parameters: slice thickness = 4 mm; slice gap = 0 mm; number of slices = 28; field of view (FOV) = 24 × 24 cm; TR/TE = 4527/10.5 ms; point = 512; arms = 8; number of excitations (NEX) = 3; post-label delay = 1525 ms; and overall scan time = 263 s. For multi-voxel 1H-spectroscopy, the parameters were: TR/TE = 1500/144 ms; flip angle = 90; voxel size = 10 × 10 × 10 mm; and total acquisition time = 330 s.
The data were transferred to an AW4.6 workstation (GE Healthcare, Milwaukee, WI, USA), and the MRS data and ASL relative cerebral blood flow (rCBF) maps were integrated with contrast-enhanced 3D-BRAVO or contrast-enhanced T2 FLAIR sequences. Ratios of choline (Cho)-containing compounds to N-acetyl-aspartate were calculated for each 1H-MRS voxel. The cerebral blood flow (CBF) should be expressed relative to an internal reference such as the contralateral white matter. Two experienced neuroradiologists (TJ and YR, each with > 5 years of experience in neuroradiology) processed the MRS and ASL data after discussion with neurosurgeons. Regions with high choline/N-acetyl-aspartate (Cho/NAA) index on MRS and high perfusion on ASL were identified to optimize target selection.
Target selection
We defined high-perfusion areas (high rCBF value) as those showing the highlighted region from the ASL color map, and the high Cho/NAA index (CNI) value must be accompanied with an elevated Cho peak. The target region was selected as follows: (i) if the lesion was single and enhanced, we chose the area with high perfusion and the maximum CNI value in the contrast-enhanced 3D T1W images; (ii) if the lesion was diffuse, we chose a high-perfusion lesion that was situated relatively superficially in the brain parenchyma and then selected the region with the highest CNI; and (iii) if tumor enhancement was very poor or absent, we chose the region with the highest CNI (in case of single lesions) or the area with highest perfusion (in case of multiple lesions) in the contrast-enhanced T2 FLAIR images.
Stereotactic biopsy guided by MRI data
The contrast-enhanced 3D BRAVO or contrast-enhanced T2 FLAIR (anatomical images) sequences were sent to a MEI De medical workstation (Sinorao; Shenzhen, PR China). To generate visible biopsy targets, image markers (white squares) were created based on the MRS data, and these could be viewed from different angles and in different image planes. The selected puncture target was framed (voxel = 10 × 10 × 10 mm) on volumetric images and the data were sent to the neuronavigation system (Stealth Station TREON; Medtronic, Minneapolis, MN, USA). All patients underwent frameless stereotactic biopsy using the navigation system in the operating theater. The puncture needle (Medtronic) used for sampling was a 2.2 × 9-mm side-cut needle, and the volume sampled was > 30 mm3. Screenshots of the puncture trajectory were saved during the biopsy. The accuracy of biopsy was evaluated on intraoperative MR images after surgery. If the intraoperative frozen biopsy tissue did not display the tumor’s histological type the first time, the tissue sampling was repeated along the original path to obtain more tissue. After the tissue sample was obtained, the needle was retained in the puncture site for a few minutes to achieve hemostasis via local pressure. The targeting was considered successful when intraoperative MRI showed the needle tip to be located at the correct location.
Pathologic evaluation
Each biopsy sample was fixed in 10% formalin and delivered to the pathology department. Pathologic evaluation included two parts: intraoperative frozen section examination and detailed examination in the pathology department. For final diagnosis, the samples were paraffin-embedded, sectioned, and stained with hematoxylin and eosin. Histopathological analysis was performed by two senior pathologists who were blinded to patient data. All tumors were classified according to the 2016 World Health Organization (WHO) classification of central nervous system tumors.
Statistical analysis
The Student’s t-test was performed using SPSS version 21 (SPSS Inc., Chicago, IL, USA). Two-sided P < 0.05 was considered statistically significant.
Results
Intraoperative stereotactic biopsy
Demographic information of the patients.
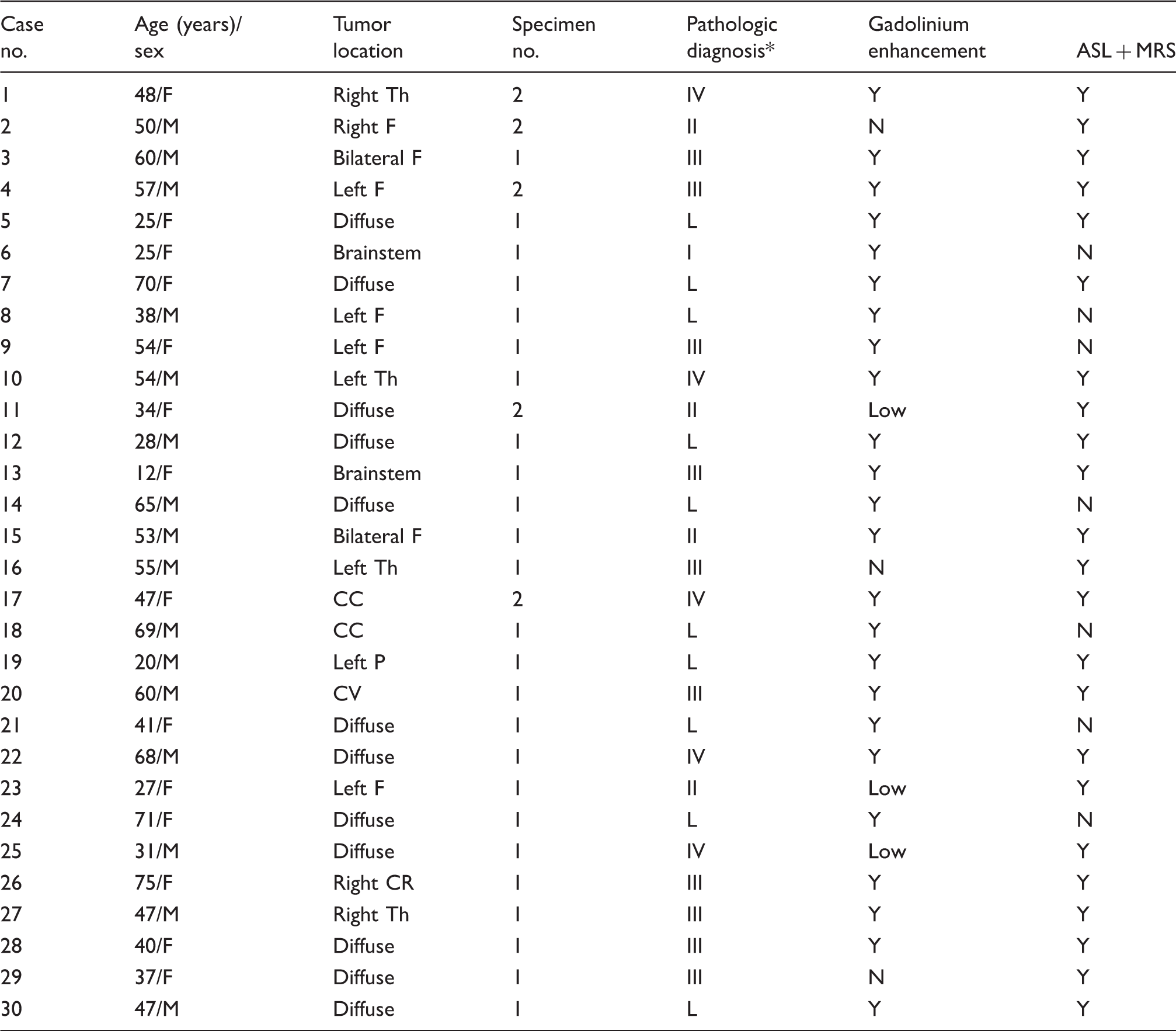
Pathologic diagnosis: I = grade I (astrocytoma); II = grade II (astrocytoma); III = grade III (anaplastic astrocytoma); IV = grade IV (glioblastoma).
Th, thalamus; F, frontal lobe; P, parietal lobe; CV, cerebellar vermis; CC, corpus callosum; BG, basal ganglia; CR, corona radiata; L, lymphoma; diffuse, indicates multiple lesions.
Gliomas
Twenty-two specimens were collected from 20 glioma patients (two specimens each were obtained from two patients). Combined ASL and MRS was useful for target determination in 18 of the 20 patients (Fig. 1). Although the puncture needle tip was inserted into predetermined target areas under intraoperative MRI guidance, the first specimen obtained from two gliomas was diagnosed as gliosis. In these patients, the histopathological diagnosis was confirmed using a second specimen. The mean rCBF and CNI values of the biopsy targets were 2.05 ± 0.83 and 2.91 ± 0.75, respectively, in the case of LGGs. For HGGs, the corresponding values were 3.04 ± 1.51 and 5.44 ± 1.82. CNI was significantly higher in HGGs than in LGGs (P = 0.027).
A 75-year-old woman with a WHO grade III glioma. (a) Axial enhanced 3D brain volume imaging shows a ring-enhancing lesion (arrow) and a solid-enhancing lesion (arrowhead) involving the right corona radiata. (b) MRS shows an elevated Cho peak in two areas: voxel 5 and voxel 8 with CNI values of 3.619 and 3.689, respectively (arrow). (c) However, only the ring-enhancing lesion demonstrates high perfusion (rCBF value = 2.97) (arrow). Therefore, it was chosen as the biopsy target. (d) Intraoperative screenshots from the neuronavigation system demonstrates the biopsy pathway navigated by enhanced 3D BRAVO. The puncture needle is located in voxel 8 finally (arrow). The puncture depth and its distance from the target is shown on the top left of the screen. (e) After the biopsy, intraoperative T1W contrast-enhanced images confirms biopsy accuracy (arrow) and excludes cerebral hemorrhage.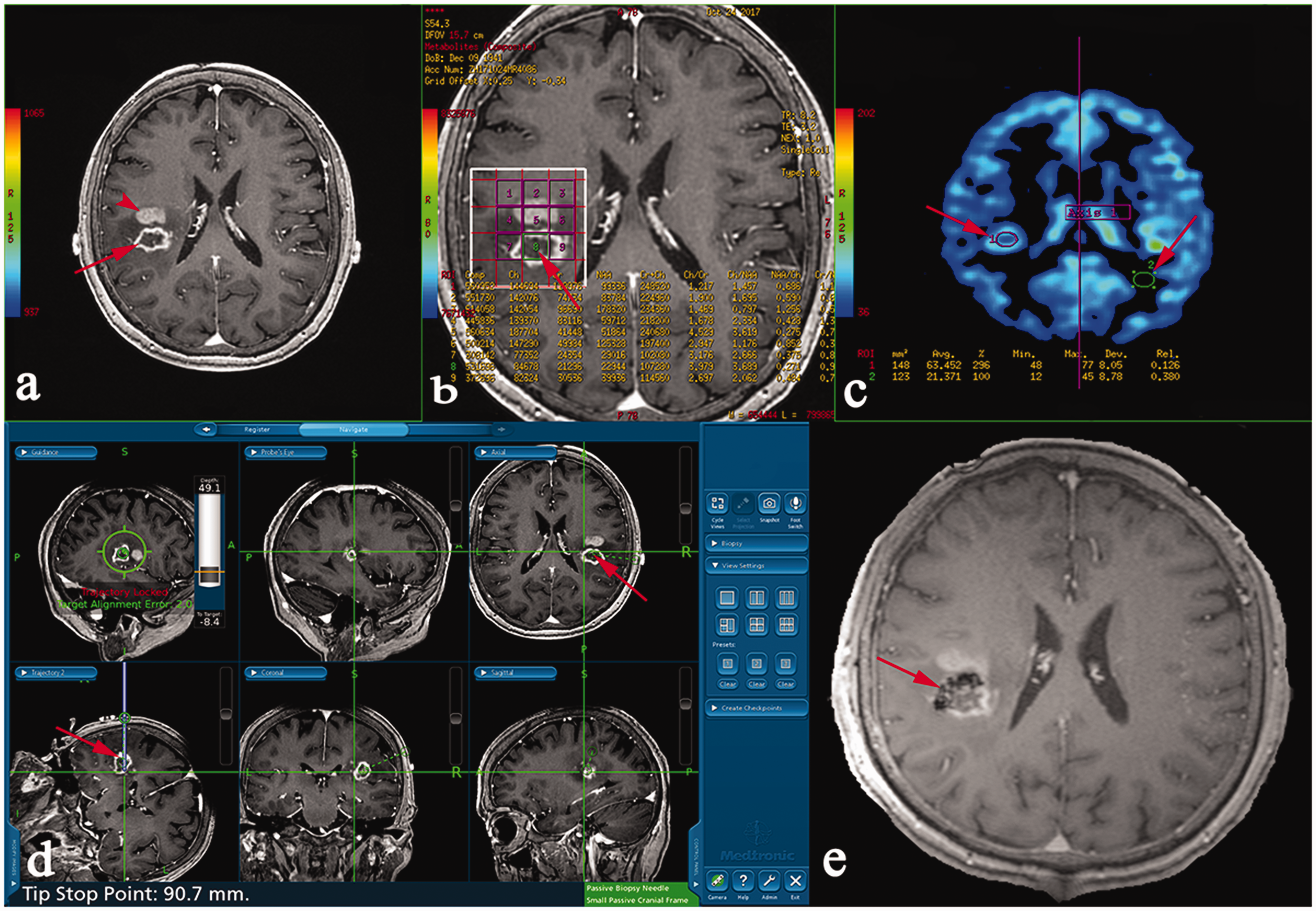
In two patients with multiple cerebral gliomas (cases 4 and 28), the neurosurgeon decided to change the biopsy target intraoperatively, because the initial target (an area with high mitotic activity on PET but without high perfusion) was discarded in favor of another area that showed high CBF and elevated choline on MRS. In one patient (case 13), the glioma was located in the brainstem, with one part that enhanced well situated deep in the brainstem and another part that did not enhance situated more superficially. The latter part also showed high perfusion and a high CNI, and for safety reasons, it was chosen as the target. The biopsy was successful, and there were no complications. In six gliomas (three LGGs and three HGGs), little or no enhancement was found. We first used ASL to locate the high-perfusion region of the tumor, and then performed MRS in this area to obtain the highest CNI value for more accurate targeting (Fig. 2). The biopsy was successful in these six cases, and no complications occurred during the next three months of follow-up.
Images of a 31-year-old man with multiple cerebral gliomas (MCG). (a) Enhanced 3D brain volume imaging shows weak enhancement in the left frontal lobe and right centrum semiovale (arrow), but only the left lesion shows hyperperfusion (b). MRS shows an elevated choline peak and decreased NAA peak; the CNI is 9.16 in voxel 10 (c, d). This strongly favors the presence of a high-malignancy element in the left frontal lobe. We selected this target for stereotactic biopsy (e). Histopathologic examination identified high-grade glioma (grade IV).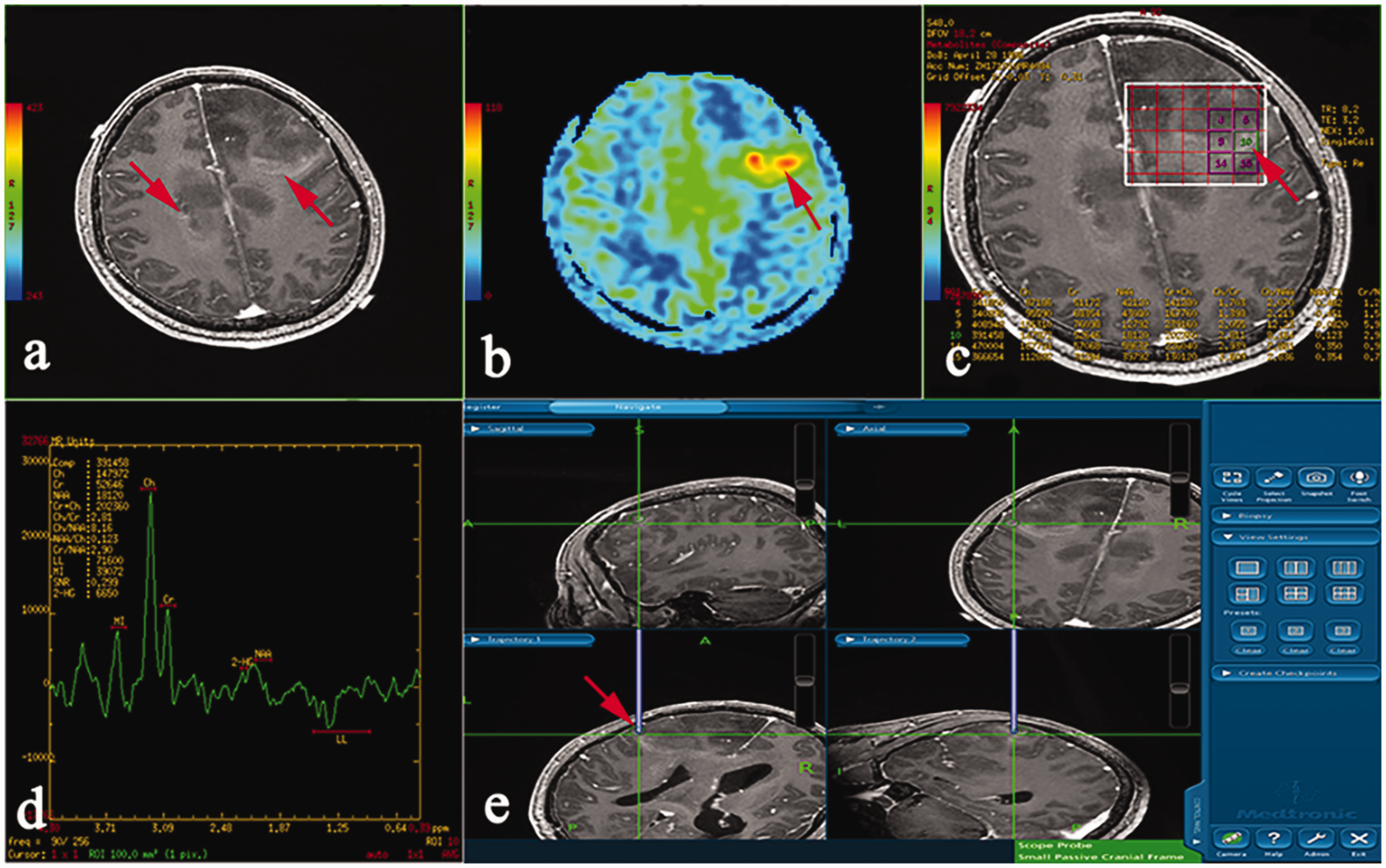
Lymphomas
Combined ASL and MRS was successful in target determination in five lymphoma patients (Fig. 3). The mean rCBF and CNI of the lymphomas were 2.40 ± 1.53 and 4.05 ± 1.73, respectively. In the other five lymphomas, ASL did not show areas of high perfusion. The biopsy sites in these cases were chosen based on MRS. All ten patients had improved after three months.
Lymphoma in a 20-year-old man. (a) An irregular mass can be seen in the occipital lobe, with obvious enhancement on 3D-T1W images (arrow). (b) There is restricted diffusion on diffusion-weighted imaging (DWI; b value = 2000 s/mm2). (c) ASL shows relatively high perfusion (arrow) in the lesion, but the difference in rCBF value was not significant in this case. We therefore analyzed the MRS features (d, e) and finally selected a superficially located area with a relatively high CNI (3.615, voxel 17) as our target. (f) Six voxels are marked on the neuronavigation system; the biopsy needle is accurately located in voxel 17.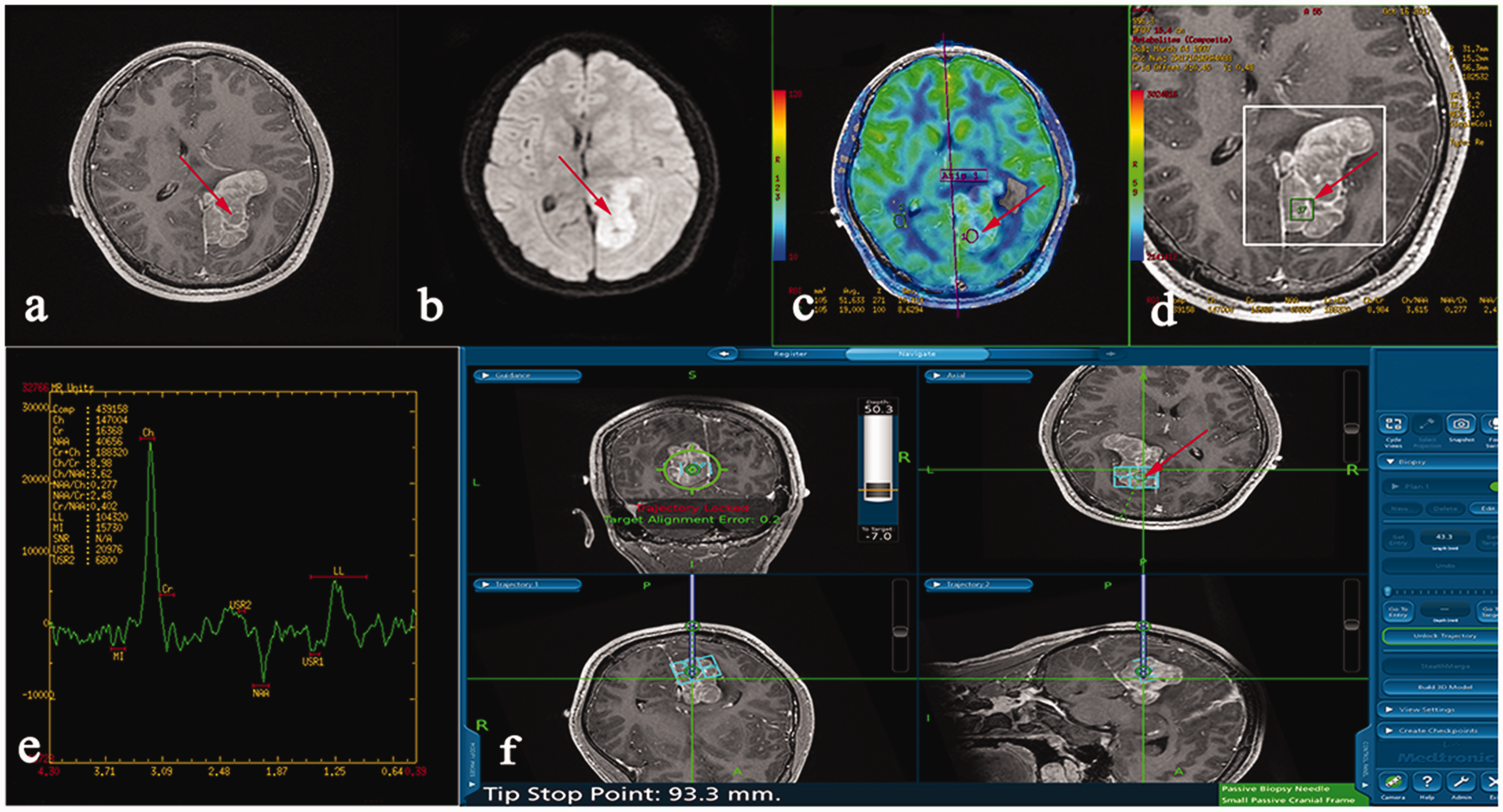
Discussion
This study aimed to evaluate the usefulness of combined MRS and ASL for the stereotactic biopsy of intracranial tumors. Our findings show that this combination is a convenient and non-invasive method that can improve the accuracy of biopsy.
MRS can demonstrate metabolic changes caused by cellular density or the mitotic index and can predict patient prognosis, survival, and tumor grades (13). Choline is an indicator of myelination and cell metabolism, and elevated choline is closely correlated with the Ki-67 cellular proliferation index (14). Abdelaziz et al. (13) reported that preoperative diagnosis using MRS-guided stereotactic biopsy was strongly correlated with the Cho/NAA ratio and histopathological diagnosis. Our results partially support these findings. We chose target areas with high CNI values and achieved excellent precision (point-to-point registration), demonstrating the reliability of the relationship between CNI and pathological characteristics.
High-perfusion MRI sequences can guide biopsies since a tumor’s malignancy is closely correlated with its blood supply (15). Lefranc et al. (3) used dynamic susceptibility contrast-enhanced MRI (DSC-MRI) guidance for 21 stereotactic biopsies and found that it reduced sampling errors and optimized tumor targeting. However, DSC-MRI involves the use of contrast agents and may be contraindicated in patients with renal problems. ASL, which can non-invasively evaluate the tumor microcirculation and degree of tumor angiogenesis, is an attractive alternative (16,17). Multiple studies have shown that ASL is highly comparable to DSC-MRI in the evaluation of the tumor microcirculation (18). Weber et al. studied glioma biopsies (19) and confirmed the positive correlation of glioma grade with tumor proliferation-related (MRS) and vascularity-related parameters (ASL). They concluded that both techniques identified similar target tissues and suggested that patients need only undergo one of these techniques. However, this applies only to patients with single lesions. In patients with multiple tumor foci, especially multiple cerebral gliomas or lymphomas, ASL must be used to find high-perfusion areas and MRS must be performed on one of these areas to overcome scanning-time limitation and identify the exact biopsy target. Thus, each technique compensates for the other’s deficiencies, and hence, the combination is useful.
The value of our technique was best demonstrated in tumors with little or no enhancement. Although contrast enhancement is often used to evaluate glioma grade (20), one-third of non-enhancing gliomas are malignant and only 20% of LGGs show enhancement (21). Malignant cells often migrate beyond the regions of contrast enhancement and even into normal brain tissue, regardless of tumor grade. Due to the histological heterogeneity of gliomas, biopsies with conventional MRI techniques (3D T1W or T2 FLAIR) can miss the most malignant tumor tissue in up to 25% of cases (22). Based on the literature on MRS, an increase in the Cho peak strongly suggests tumor progression in LGGs (19,23), which is precisely the target that must be selected for biopsy. ASL has good application prospects in the non-invasive grading of tumors. HGGs can be distinguished from LGGs by the elevated perfusion parameters of the former (18). Treister et al. (20) proposed that ASL signal heterogeneity could help identify the desired biopsy target, leading to a more accurate histopathological grade. To the best of our knowledge, no study has yet reported on the use of ASL-guided stereotactic biopsy. In the present study, six gliomas (three LGGs and three HGGs) demonstrated very low or no enhancement. The contrast-enhanced T2 FLAIR sequence was not useful in these cases because peritumoral edema made target selection difficult. In these cases, we first performed ASL to identify high-perfusion areas and then performed multiple-voxel 1H-MRS in these areas to identify the voxel with the highest CNI. Biopsies from such areas were successful and led to definite pathological diagnoses. The treatment was effective in the six patients as demonstrated by three months of follow-up.
The success rate of combined ASL- and MRS-guided stereotactic biopsy was 90% for gliomas, which is higher than the success rate of conventional MRI (22). Only two gliomas were diagnosed as gliosis from the first biopsy specimen. It must be noted that pathological diagnosis may be uncertain even when intraoperative MRI confirms that sampling has been done from the target area. This is because the sample quantity is limited by the needle volume. In such cases, a second sampling must be performed along the same path. Our registration accuracy for biopsy was approximately 1 mm, and it was influenced by the quality of the 3D-BRAVO sequence. To obtain a good registration accuracy, it is important for patients to remain motionless during the MRI examination. With regard to lymphoma, Lefranc et al. (3) suggested that T1W contrast-enhanced imaging was the only method suitable for target tissue selection. Our results do not completely agree with this. In our study, biopsy with combined MRS and ASL was successful in five lymphoma patients. In the other five lymphoma patients, the tumors displayed relatively low perfusion, and ASL was of little value for stereotactic biopsy in these patients. We therefore used the 3D-BRAVO and MRS data for optimal target selection.
PET, another useful modality, can enable the targeting of areas with high cellularity (24). Combined MRS- and PET-guided stereotactic biopsy can improve the diagnostic accuracy of brain tumors (25). In two of our patients, the target areas were originally selected on the basis of high mitotic activity (but without high perfusion) displayed on PET. However, the ASL data suggested other areas as more likely targets, and because these areas were in a more superficial location, the surgeon successfully performed the biopsy on the high-perfusion regions for safety purposes. Given the cost and radiation hazards of PET, ASL may be a substitute for PET in the identification of areas of high malignancy.
This study has certain limitations. First, the number of cases, especially of LGGs (grades I and II) and lymphomas, was relatively small. Second, MRS was performed after the injection of a Gd-containing contrast agent, which may have decreased the Cho peak and interfered with the examination results (26).
In conclusion, CNI values and rCBF measurements provide diagnostic information not available from conventional images, and each of these measurements compensates for the other’s deficiencies. The combined use of MRS plus ASL for the guidance of stereotactic biopsy can therefore help identify the most malignant areas within heterogeneous tumors and improve the accuracy of the stereotactic biopsy of intracranial tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.