
Abstract
Background
Loose bodies are one of the most frequently seen pathological processes observed in the knee joint. Just as loose bodies may settle within the knee joint cavity, they may also be localized within recesses and bursae.
Purpose
To determine in which anatomic localizations and at what frequencies loose bodies were located in recesses and bursae within the knee joint. It was also aimed to review the radiological anatomy of the common and unusual knee joint synovial recesses and bursae including arthroscopic blind spots on MRI.
Material and Methods
A total of 145 loose bodies in 104 knees evaluated by MRI were identified. The locations of loose bodies around the knee joint were divided into 11 groups and some of these groups were divided into specific subgroups on MRI. The anatomic localizations, the number, and dimensions of loose bodies were determined.
Results
There were 145 loose bodies and 45 patients had one, 19 patients had two, and 40 patients had three or more loose bodies in different locations. The average size of loose bodies was 9.3 mm (range = 9–23 mm). Posterior cruciate ligament recess was the most frequent location; the subpopliteal recess was the second and posterior femoral recess was the third most common location for the loose bodies.
Conclusion
The correct identification, the number, size, and anatomic localization of loose bodies on MRI is critical in the determination of the appropriate treatment and, thus, the development of osteoarthritis can be prevented. Loose bodies were mostly localized in the posterior, primarily in the posterior cruciate ligament recess, most were multiple and < 1 cm.
Introduction
Loose bodies (LBs) are one of the most frequently seen pathological processes observed in the knee joint (1). The knee is a large joint with a complex anatomic structure with synovial recesses and bursae. Just as LBs may settle within the knee joint cavity, they may also be localized within recesses and bursae (2).
The standard method for treatment of the knee LBs is surgical removal. Arthroscopy is the preferred technique to remove LBs (3). By becoming trapped between joint surfaces, mobile LBs may cause pain, limitations in movement, intermittent locking in the joint, and edema (1). When there is repeated internal derangement, the articular surface can be damaged, leading to early osteoarthritis (OA) (3). The determination of LBs during imaging of the knee and identification of the correct anatomic localization is extremely important for surgical planning in the early stage; thus, the development of OA can be prevented. Recent studies have been conducted on chronic OA cases of the effects of surgical removal of LBs. In one recent study, the cure rates of chronic OA patients were reported to be higher in those who had undergone arthroscopic LB excision (4).
Although intermittent clinical findings generally suggest LB, they are not specific. Therefore, there is a need for radiological imaging to confirm the diagnosis. LBs may be chondral, osseous, or osteochondral (5). Osseous and osteochondral LBs can be detected radiographically because of the osseous component and the initial diagnosis is usually made from plain radiographs. However, non-calcified chondral LBs cannot be seen on plain radiographs or on computed tomography (CT) without prior arthrography. Therefore, the imaging modality of choice for the assessment of intra-articular LBs is magnetic resonance imaging (MRI) (5). Nevertheless, LBs may be overlooked when evaluating MRI, especially those in unusual localizations.
To be able to plan the correct treatment, it is necessary to know the usual and uncommon anatomic localizations of LBs in the knee and to be able to differentiate LBs from other pathologies, which may occur in these areas. However, there are blind spots in the knee joint which are difficult to reach in a standard arthroscopic examination. Accessory portals may be required during arthroscopic removal of LBs in these areas. It is important to know these areas on MR images and to identify LBs located there to be able to determine the surgical approach (3).
The aim of this study was to determine in which anatomic localizations and at what frequencies LBs were located in recesses and bursae within the knee joint. It was also aimed to review the radiological anatomy of the common and unusual knee joint synovial recesses and bursae including arthroscopic blind spots for LBs on MRI.
Material and Methods
This retrospective study was approved by the Institutional Review Board of Izmir Katip Celebi University (IRB number 433). Since the study was retrospective, informed consent by patients and providers was not required.
The scans were obtained on a 1.5-T Signa MRI unit (General Electric Medical Systems, Milwaukee, WI, USA) in conjunction with the superficial knee coil. The patient was in a supine neutral position. Sagittal proton-density (PD) fat-suppressed turbo spin echo (TSE) (TR/TE = 1500/15, acquisition matrix = 256 × 384, field of view [FOV] = 18 cm), coronal PD fat-suppressed TSE (TR/TE = 1500/15, acquisition matrix = 256 × 320, FOV = 18 cm), coronal T1-weighted TSE (TR/TE = 500/18, acquisition matrix = 256 × 320, FOV = 21 cm), axial T2-weighted (T2W) fat-suppressed TSE (TR/TE = 2000/60, acquisition matrix = 256 × 288, FOV = 16 cm), and axial T2W gradient echo (MERGE-Multiple Echo Recombined Gradient Echo) (TR/TE = 656/5, acquisition matrix = 256 × 288, FOV = 16 cm) sequences were included into the scan as the standard sequences. The slice thickness was 3 mm with a 1-mm interslice gap. MR images were also obtained digitally using a picture archiving communication system (PACS) and MRI evaluation was performed using the PACS software.
A total of 145 LBs in 104 knees evaluated by MRI during 2008–2012 were identified via a radiology information system (RIS) keyword search. Patients were excluded if they were aged < 18 years, had a mass lesion in the knee, or had a history of open or arthroscopic knee surgery.
The knee MR images were reviewed by an attending musculoskeletal radiologist with 15 years of experience. The locations of LBs around the knee joint were divided into 11 groups and some of these groups were divided into specific subgroups on MRI as follows:
Posterior femoral recess (Subgastrocnemius recess, Retrocondylar joint recess): Localized between the deep surfaces of the lateral and medial heads of the gastrocnemius and the posterior of the femoral condyles.a. Medial femoral condyle posteriorb. Lateral femoral condyle posterior Knee joint spacea. Lateral tibiofemoral compartmentb. Medial tibiofemoral compartmentc. Midline of tibiofemoral jointd. Central synovial recess Proximal tibiofibular joint: Between the head of fibula and the tibia. Suprapatellar pouch: Over the patella, extending between the quadriceps tendon and the anterior surface of the femur.a. Lateralb. Medial Subpopliteal recess: Located between the posterior aspect of the lateral meniscus and the tendon of the popliteus muscle. Posterior cruciate ligament (PCL) recess (posterior capsular recess): Located between the PCL and the posterior joint capsule. Gastrocnemius-semimembranosus bursa (interior of Baker’s cyst): Located between the medial head of the gastrocnemius muscle and the semimembranosus tendon. Semimembranosus-tibial collateral ligament bursa (Semimembranous bursa): The superficial part of the bursa is located between the superficial section of the semimembranosus tendon and the medial collateral ligament. The deep part is located between the deep section of the semimembranosus tendon and the medial tibial condyle. Pes anserinus bursa: Located between the tibial attachment site of the medial collateral ligament and adherent distal tendons of the sartorius, gracilis, and semitendinosus muscles (pes anserinus). Suprahoffatic recess: Observed in the form of a vertical cleft close to the inferior edge of the patella at the level of the infrapatellar fat pad. Infrahoffatic recess: Observed in the form of a horizontal cleft extending to the anterior of the inferior section of the infrapatellar plica.
The anatomic localizations of LBs were identified. The number and dimensions of LBs were also determined.
Results
The study group consisted of 104 patients (51 women [61.3%], 53 men [38.7%]; average age = 54.8 years; age range = 20–87 years).
There were 145 LBs: 45 patients had one; 19 patients had two; and 40 patients had three or more LBs in different locations. The average size of LBs was 9.3 mm (range = 9–23 mm).
Knee MR images identified 55 LBs in the PCL recess (Fig. 1), 24 LBs in the subpopliteal recess (Fig. 2), 17 LBs in the posterior femoral recess (Fig. 3), 15 in the knee joint space, 14 in the suprapatellar pouch, 13 in the gastrocnemius-semimembranosus bursa (Fig. 4), three in the pes anserine bursa (Fig. 5), two in the suprahoffatic recess (Fig. 6), and one each in the infrahoffatic recess (Fig. 6) and semimembranosus-tibial collateral ligament bursa (Fig. 7).
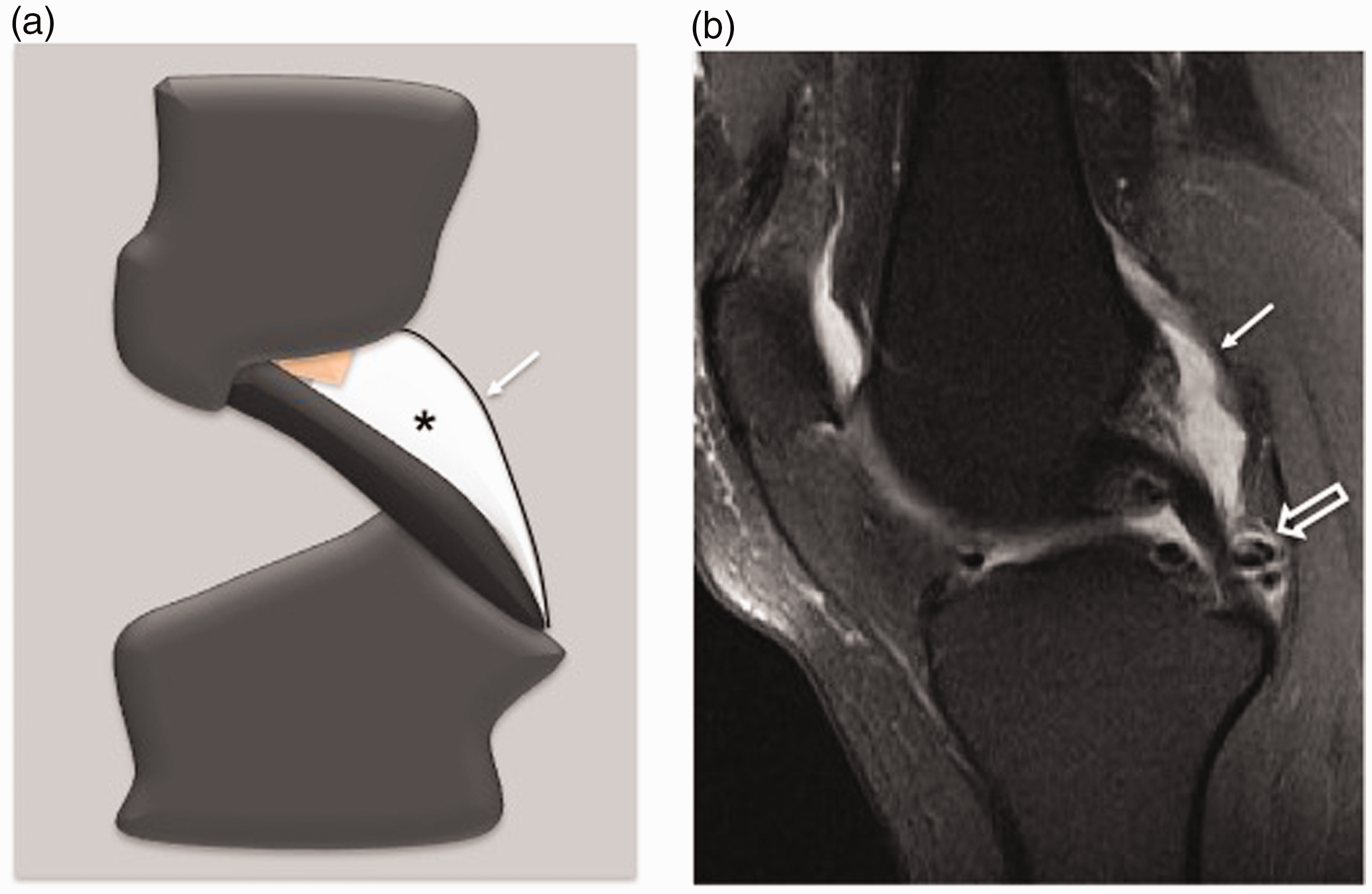
(a) Sagittal plan schematic drawing shows posterior cruciate ligament (PCL) recess (asterisk indicates PCL recess, arrow indicates posterior joint capsule). The pink colored area represents the fat tissue. (b) Proton-density (PD) fat-suppressed turbo spin echo (TSE) image shows multiple LBs (open arrow) in the PCL recess.

(a) Sagittal plan schematic drawing shows subpopliteal recess (asterisk). Arrow indicates popliteal hiatus. (b) Sagittal proton-density (PD) fat-suppressed turbo spin echo (TSE) image shows two LBs (open arrows) in the subpopliteal recess. Arrowhead indicates popliteal hiatus located superior to the subpopliteal recess.
(a) Sagittal plan schematic drawing shows posterior femoral recess (asterisk). Arrow indicates the posterior joint capsule. (b) Sagittal proton density (PD) fat-suppressed and (c) coronal PD fat-suppressed turbo spin echo (TSE) images show two LBs (open arrows) in the posterior femoral recess located posterior superior to the medial femoral condyle.
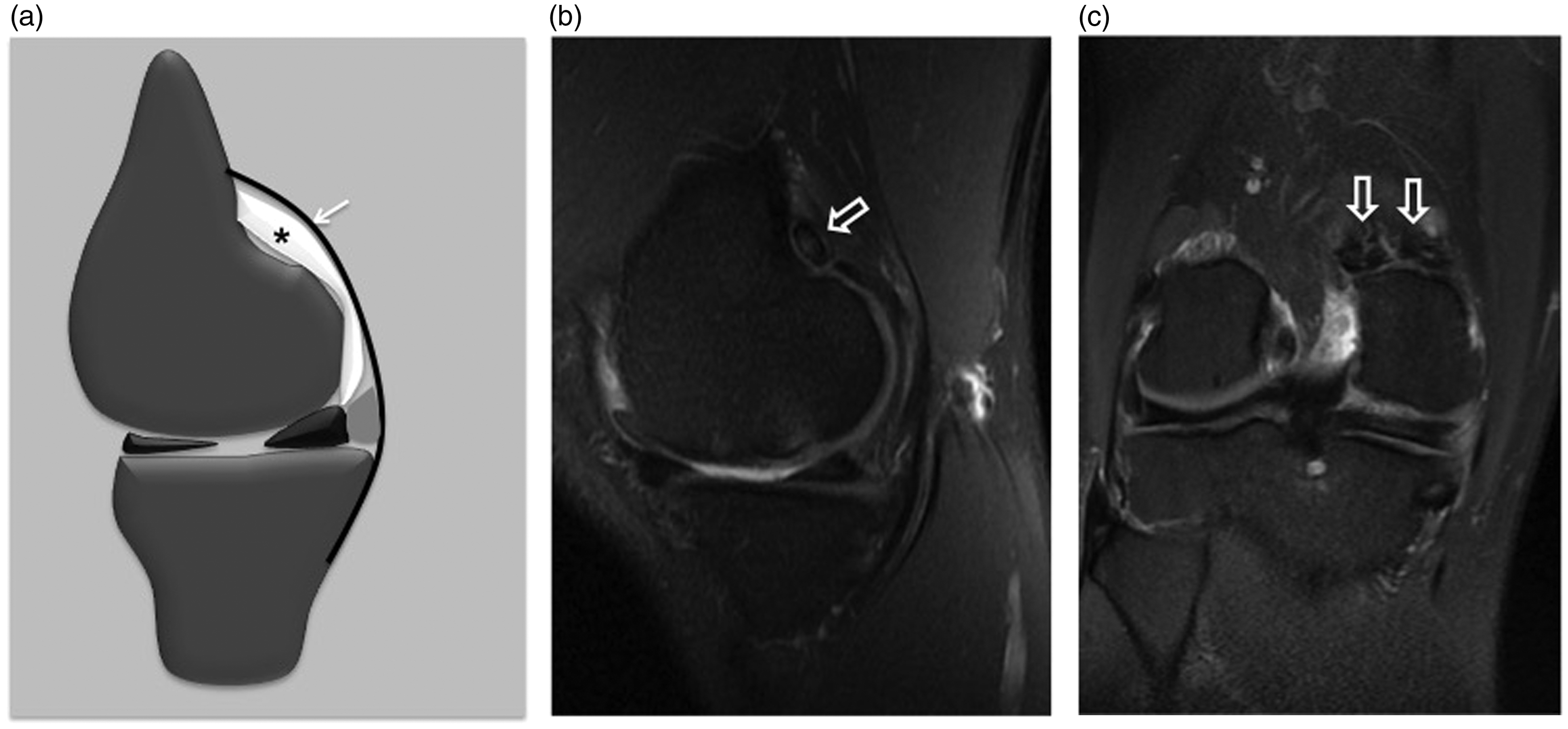
(a) Axial plan schematic drawing shows gastrocnemius-semimembranosus bursa (Baker’s cyst, asterisk). (b) Axial T2W gradient echo (MERGE) and (c) coronal PD fat-suppressed images show LBs (open arrows) in Baker’s cyst. (arrow: medial head of the gastrocnemius muscle, curved arrow: LB containing co-signaled area with yellow bone marrow)

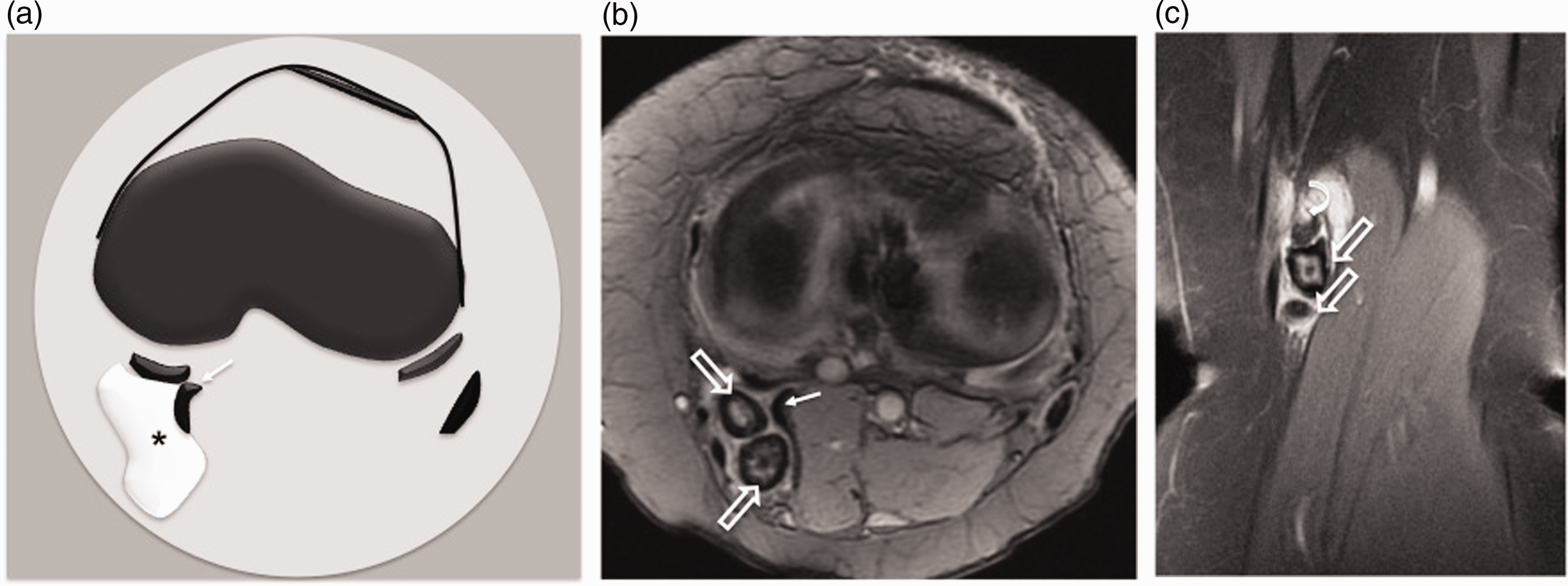
(a) Coronal plan schematic drawing shows pes anserine bursa (asterisk). Arrows indicate medial collateral ligament. (b) Coronal proton-density (PD) fat-suppressed turbo spin echo (TSE) and (c) axial T2W fat-suppressed TSE images show a LB (open arrow) in the pes anserine bursa. PA, pes anserine tendons.

(a) Sagittal plan schematic drawing shows suprahoffatic (asterisk) and infrahoffatic (arrow) recesses (arrowhead indicates anterior transvers intermeniscal ligament). (b) Proton-density (PD) fat-suppressed turbo spin echo (TSE) image shows a LB (open arrow) in the suprahoffatic recess. (c) Sagittal PD fat-suppressed TSE image shows a LB (curved arrow) in the infrahoffatic recess.
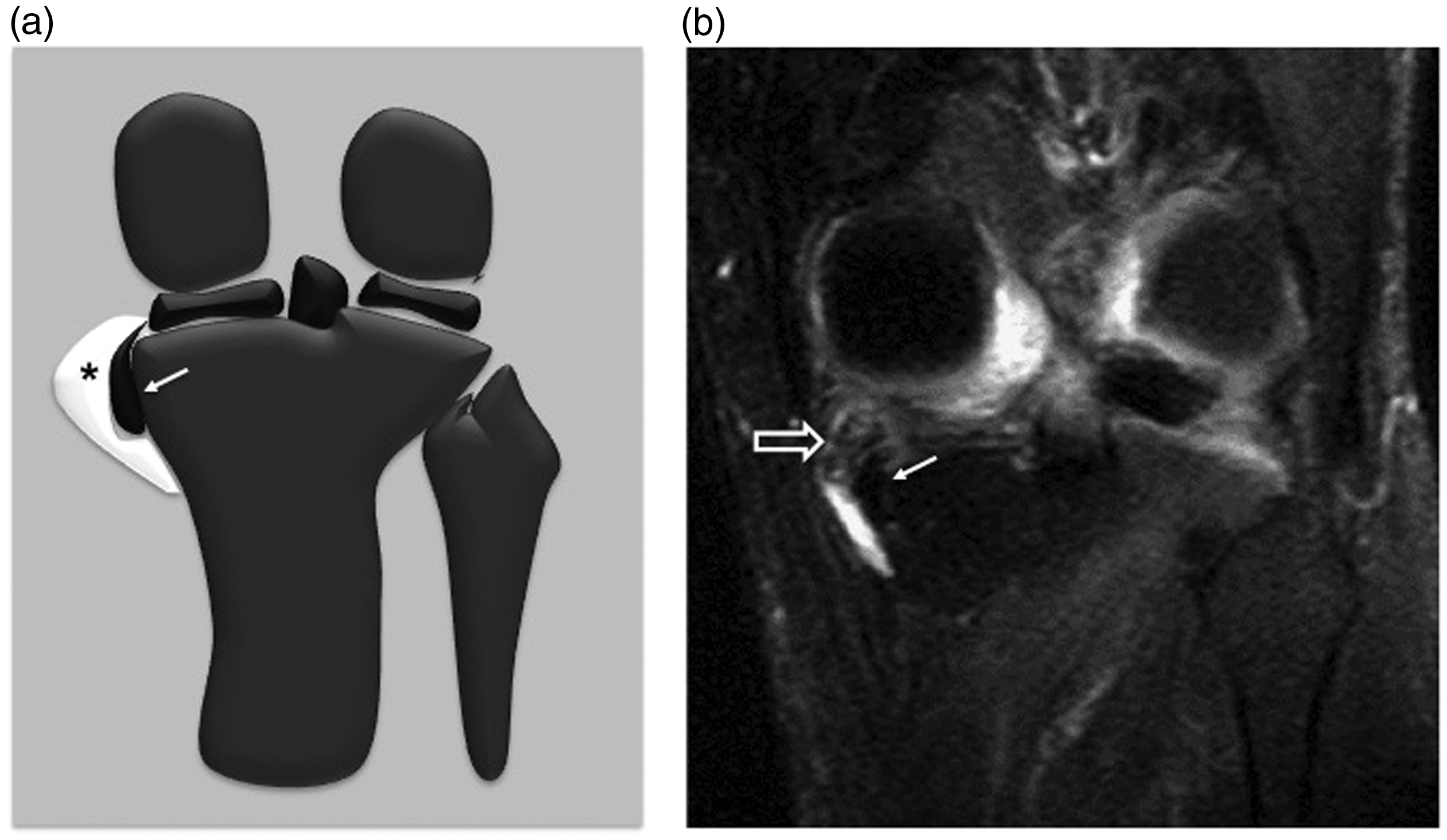
(a) Coronal plan schematic drawing shows semimembranosus-tibial collateral ligament bursa (asterisk). Arrow indicates semimembranosus tendon. (b) Coronal proton density (PD) fat-suppressed image shows a LB (open arrow) in the semimembranosus-tibial collateral ligament bursa.
PCL recess was the most frequent location in each of the 11 groups studied herein. The subpopliteal recess was the second most common location for the LBs. The quantitative distribution of LBs according to groups was shown in Fig. 8.
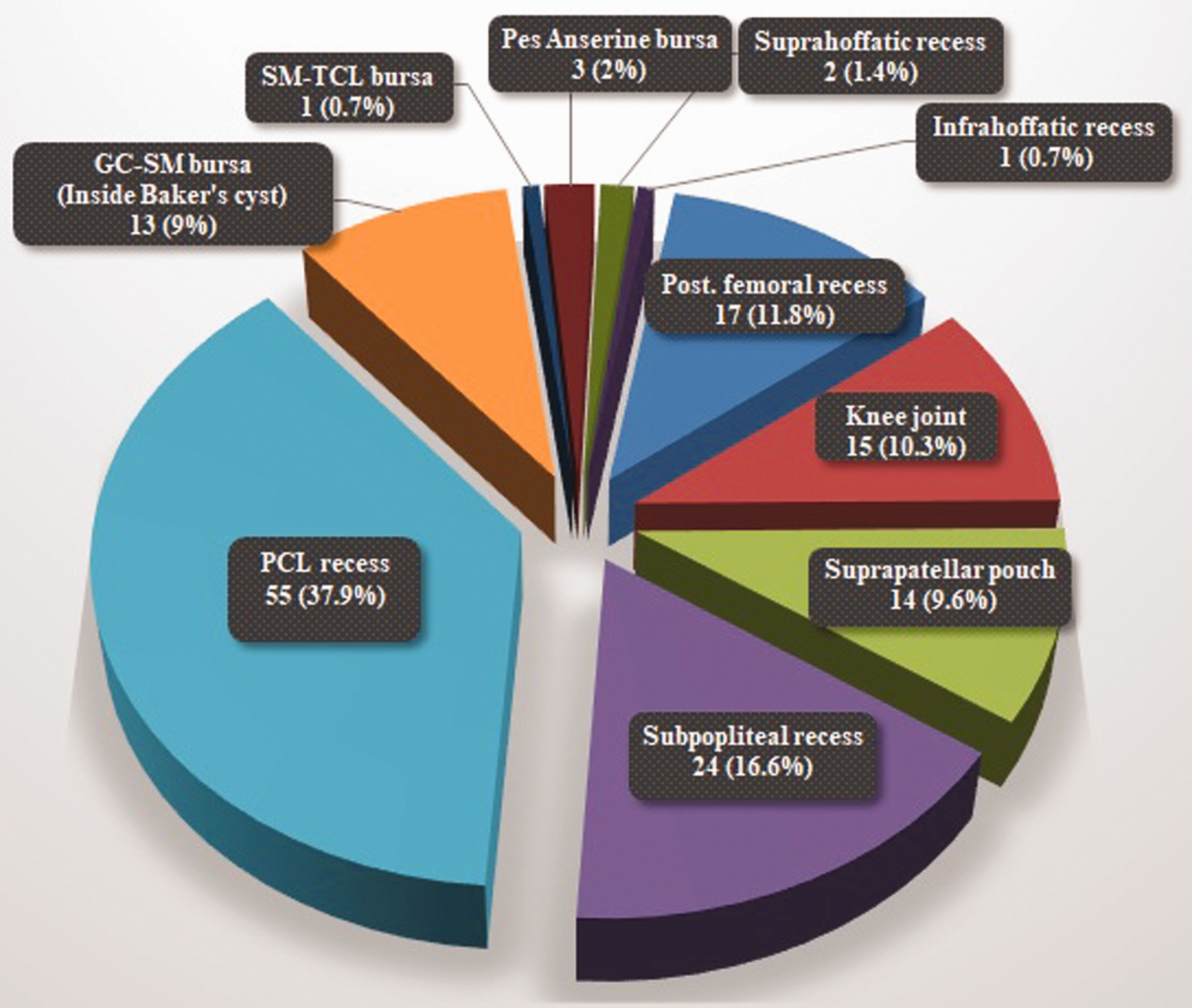
The quantitative distribution of LBs according to groups.
Discussion
LBs are cartilage or bone fragments that can develop as a result of injury or wear and tear over time. Just as LBs may be able to move easily within the knee joint, they may also be settled within synovial recesses or bursae. MR images of LBs vary depending on the degree of calcification or ossification. Chondral LBs are observed with high signal intensity on fat-suppressed PD and T2W sequences (6). Osseous LBs usually include a high T1 signal of the central fatty bone marrow signal. The peripheries are generally surrounded by a low signal ring, equivalent to the cortical bone signal (6,7). Osteochondral bodies usually have a heterogenous signal. In cases with effusion in the joint, LBs can be easily identified usually as ovoid or spherical-shaped structures with a lower signal in proportion to the fluid within the fluid with T2 high signal. However, when there is localization within more peripheral areas of the joint or within recesses or bursae, they may be missed. Therefore, knowing potential localizations where they can settle is important in the determination of osteochondral bodies.
Arthroscopic removal of LBs is a primary option for treatment (3). In a recent study, Zhao et al. investigated the efficacy of arthroscopic LB excision in patients with chronic OA (4). That study showed that surgical removal of LBs not only prevented the development of OA but was also an important treatment method in cases with chronic OA because of the ability to reduce the inflammatory reaction (4). However, there are blind spots that are difficult to reach during a conventional arthroscopic approach. The presence of LB in these areas can be determined with MRI before the intervention (3,8). If the presence of LBs is determined in these areas, they can be removed by reaching the area with accessory portals (9).
In the current study, the most frequently seen localization of LBs was the posterior capsular recess, which may be named in literature as the PCL recess. Of 145 LBs, 55 (37.9%) were determined in this localization. The PCL recess is located at the posterior of the PCL. The PCL recess can be easily seen on MR images when there is fluid in this area (10). Due to the effect of gravity, LBs has a tendency for localization in the posterior compartment. In a study of arthroscopic removal of LBs from the posterior compartment of the knee, Ahn et al. reported that the third most common localization was around the posterior septum (3). The area defined as around the posterior septum corresponds to the PCL recess in the current study, which was the most frequently determined area. Ahn et al. reported that the arthroscopic technique of identification and removal of LBs in the posterior section of the knee joint was difficult; they recommended MRI before arthroscopy for planning the procedure (3).
The second most common localization (16.6%) of LBs in the current study was the subpopliteal recess. The subpopliteal recess is an inferior extension of the knee joint cavity and is covered by the popliteus tendon (11). In literature, the subpopliteal recess may be known as the subpopliteal bursa, popliteus bursa or the popliteus tendon recess (3,12). On sagittal and coronal MR images, the subpopliteal recess is seen just below the popliteal hiatus (13). The popliteal hiatus and subpopliteal recess are arthroscopic blind spots (3,8). Chen et al. reported that when LBs were located 2–3 cm below the tibial plateau, they could not be removed, even with accessory portals (8). As the surgical approach may be changed with correct identification of LBs in this area, which is difficult to reach arthroscopically, MRI is of great importance.
The third most common localization of LBs in the current study was the posterior femoral recess. In literature, this recess may have different names such as the subgastrocnemius recess or the retrocondylar joint recess (2,14). As the posterior femoral recess is connected to the intra-articular joint cavity, mobile LBs can easily move to this area from the joint space. Of the LBs, 89.7% were located in the bursae and recesses out of the central synovial recess. Entrapment in these recesses and bursae following movement of free bodies in the joint space to these areas could cause this situation. There is also the possibility of the formation of osteochondral bodies by chondrometaplasia in the recesses and bursae. As there is a high probability of overlooking LBs when there is a small amount of fluid, all the recesses and bursae must be carefully evaluated. However, it should be kept in mind that MRI may not always show LBs. There may be small fragments, which may not enter into the slice thickness. Some small LBs in recesses and bursae, which do not contain effusion, may not be differentiated from adjacent soft-tissue signal on MRI due to their signal characteristics. Negative MR examination does not exclude the diagnosis of LBs. Evaluation of the X-ray examination together with MRI can help in demonstrating the small LBs with osseous component, which may be overlooked. Arthroscopy allows surgeon to thoroughly examine the knee for LBs. Hence, it is the best diagnostic and therapeutic modality available. However, since diagnostic arthroscopy is an invasive method, MRI is the imaging method to be selected as the non-invasive and radiation-free modality to show the presence and distribution of LBs at the time of diagnosis.
In the current study, 13 (9%) LBs were within the popliteal cyst known as Baker’s cyst. Of the 13 LBs within Baker’s cyst in the current study, in 11 there was no accompanying LB in the tibiofemoral joint space and central synovial recess. In six cases, LB was determined only in Baker’s cyst.
The localizations where the lowest rates of LBs were determined were the pes anserinus bursa, the semimembranosus-tibial collateral ligament bursa, suprahoffatic recess, and infrahoffatic recess. Localization of three LBs was determined in the pes anserinus bursa and of one in the semimembranosus-tibial collateral ligament bursa. Two separate synovial recesses are defined at the level of the infrapatellar fat pad. The suprahoffatic recess is found in 71% of knees on routine MR images, while the infrahoffatic recess is observed in 45% of knees on routine MR images (15). To date, the presence of LB in these localizations has been reported in very few cases in literature (16). In the current study, LB was detected in the suprahoffatic recess in two cases and in the infrahoffatic recess in one case.
Of the 104 cases in the current study, two or more LBs were detected in 59 (56.7%). In literature, multiple LBs have been reported to be seen at the rate of 30%, so the rate in the current study was higher than these findings in literature (2). The mean size of LBs in the current study was < 1 cm. When there is no joint fluid, it can be particularly difficult to identify LBs on MRI. Fragment size is important as it can affect the selection of arthroscopic or open surgical treatment.
There were some limitations of this study, primarily that it was retrospective in design and the diagnosis of LBs was made based on the MR images. As arthroscopic removal of the LBs was not applied to all the patients, no comparison could be made with the gold standard method in diagnosis. However, this limitation can be considered to have been minimized as all the MR images were evaluated by a musculoskeletal radiologist with 15 years of experience; the LBs were well-identified with typical MRI characteristics. Another limitation of this study was that since our hospital serves as an adult hospital, we could not include pediatric patients in this study. Strong aspects of the study can be considered to be the large sample size and that the recesses and bursae of the knee joint were examined systematically and separately to be able to clearly identify the localization of the LBs.
In conclusion, when LBs are in an unusual anatomic localization they can often be overlooked, and repeated internal derangement can cause the development of early OA. It has been reported that surgical removal of LBs in cases with chronic OA has increased the cure rates. Therefore, the correct identification of the presence of LBs, the number, and the anatomic localization, is critical in the determination of the appropriate treatment and the success of that treatment. The results of this study showed that localization was mostly in the posterior, primarily in the PCL recess and the subpopliteal recess and most were multiple.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.