
Abstract
Background
In clinical practice, we have often observed contrast material spreading into the epidural space during lumbar facet joint injection. However, the exact incidence of epidural spread and contrast pattern have not been reported.
Purpose
To evaluate the incidence and pattern of epidural spread in lumbar facet joint injection.
Material and Methods
One hundred consecutive patients (38 men, 62 women; mean age 68 years; age range 20–88 years) who underwent lumbar facet joint injection at two sites between April 2014 and June 2014 were investigated in this prospective study. Initial oblique, final anteroposterior, and lateral fluoroscopic images were obtained and evaluated for the presence of epidural spread and its contrast pattern (based on direction and extent) with the consensus of three radiologists. The relationship between epidural spread and its potential predictors was analyzed using the chi-squared test, Fisher’s exact test, and the t-test.
Results
The incidence of epidural spread during lumbar facet joint injection was 64.6% (n=64) in 99 patients and 49.5% (n=95) in 192 procedures; ventral spread occurred in 29.2% and foraminal spread in 18.8%. When epidural spread occurred, the most commonly identified distributions were unilateral (73.7%), dorsal (92.6%), and cephalad (92.6%). Epidural spread increased significantly in the caudocephalic direction (P < 0.0001), in men (relative risk [RR]=1.478), in the adjacency of posterior fusion level (RR=1.545), in patients with spondylolisthesis (RR=1.454), and when there was no other leakage (RR=0.334).
Conclusion
Epidural spread occurred at about half the number of lumbar facet joint injections and showed a contrast pattern similar to that seen with the interlaminar approach.
Introduction
Lumbar facet joint injections (LFJI) are the second most common interventional procedures for chronic pain related to facet joints (1,2) and is considered to be a relatively simple and minimally invasive procedure (3). However, multiple studies have shown that intra-articular FJIs have little long-term utility (2,4–8) and medial branch blocks, which, if effective in short-term pain relief and followed by radiofrequency ablation (RFA), are the treatment of choice for lumbar and cervical facet pain (9,10). Nevertheless, because of its safety, the clinical applications of LFJIs are steadily increasing in a broad range of spinal diseases, yet their usefulness is controversial.
In clinical practice, we have often observed contrast material spreading into the epidural space on fluoroscopic images during LFJI. Our hypothesis was that epidural spread (ES) in LFJI occurs often and has relevant contrast patterns; hence, LFJI could be an effective alternative to lumbar epidural steroid injection (LESI) for treatment of lumbar radiculopathy. Recently, Hwang et al. (11) reported that LFJI could be an indirect method for approaching the epidural space and mentioned the efficiency of LFJI as an alternative to LESI.
The possibilities and therapeutic implications of ES in LFJI were first mentioned in the literature by Dory and Moran et al. in the 1980s (12,13); however, these were either descriptive statements and not substantiated by quantitative data (12) or a limited study of a few cases of one cadaver (13). Several retrospective studies have reported the incidence of ES during LFJI to be 50–81% in patients undergoing intervention for rupture of a lumbar facet joint ventral synovial cyst (14,15) and in those with central canal stenosis and a high risk of bleeding (11). However, to our knowledge, the exact incidence of ES in the general patient population during the LFJI has not been reported. Further, there has been no published study investigating the contrast patterns of and predisposing factors for ES in LFJI. If the ES during the LFJI procedure occurs to a considerable extent, intra-articular LFJI may be an alternate way to access the epidural space where direct epidural injection is not feasible.
Therefore, the purpose of this study was to determine the incidence of ES and its spread patterns during fluoroscopically guided intra-articular LFJI.
Material and Methods
This prospective study was approved by the institutional review board and all patients provided signed informed consent.
Patients
We prospectively recruited 99 patients (38 men, 61 women; mean age = 68 years; age range = 20–88 years) who underwent LFJI in our department between April 2014 and June 2014. Patients were included in the study if they had undergone LFJI at two sites (one-level bilateral or two-level ipsilateral). The exclusion criteria were a single site of LFJI, LFJI combined with LESI, and previous involvement in the study.
Injection technique
Each LFJI procedure was performed by one of three musculoskeletal radiologists who had three months, two years, and 10 years of experience in administering spinal injections. The LFJIs were performed in an angiography suite equipped with uniplanar fluoroscopy (Integris Allura Xper FD 20; Philips, Amsterdam, The Netherlands). Following sterile preparation and draping, a 12-cm 22-gauge spinal needle was inserted into either the inferior recess or the inferior aspect of the posterolateral capsule of the facet joint under intermittent fluoroscopic guidance.
Localization of the intra-articular needle was confirmed by injecting 0.5 mL of contrast material (Omnipaque 300; Amersham Health, Princeton, NJ, USA) (denoted by a “test contrast”) and an initial oblique capture image was obtained. If no visualization of the facet arthrogram persisted until all of test contrast was injected, the periarticular injection was carried out. Once the intra-articular positioning was confirmed, 1 mL of medication (mixture of triamcinolone acetonide (Tamceton [40 mg/mL]; Hanall Pharmaceutical, Seoul, Republic of Korea) and ropivacaine hydrochloride (Ropiva [7.5 mg/mL]; Hanlim Pharmaceutical, Seoul, Republic of Korea) at a 1:1 ratio) was injected. Next, we injected additional contrast material to deliver the injectate into the epidural space (denoted as “push contrast”). To compare the incidence of ES according to injection volume, we divided patients into two groups to receive either 0.5 mL or 1.5 mL of push contrast. In order to match patient demographic characteristics, we used three different types of injection protocol (A, B, and C) as explained in Table 1. The final anteroposterior (AP) and lateral capture images were stored immediately after delivery of the prescribed injectate volumes.
Injection volume protocol.
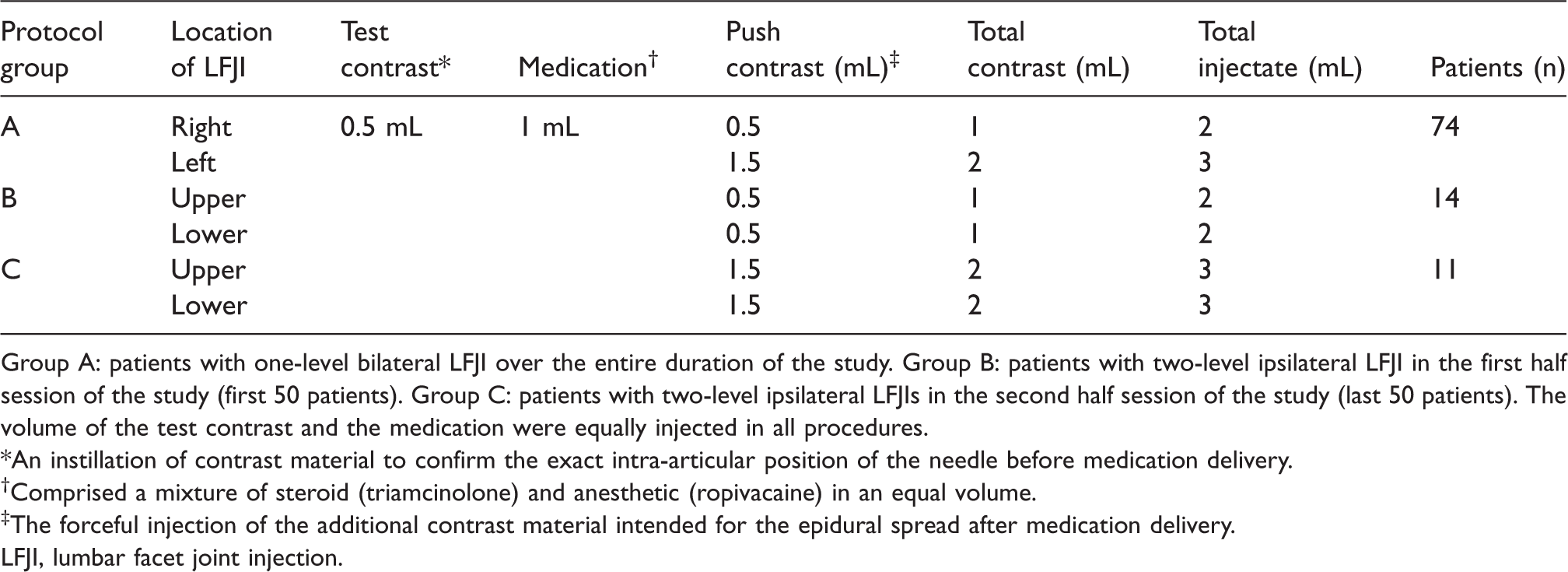
Group A: patients with one-level bilateral LFJI over the entire duration of the study. Group B: patients with two-level ipsilateral LFJI in the first half session of the study (first 50 patients). Group C: patients with two-level ipsilateral LFJIs in the second half session of the study (last 50 patients). The volume of the test contrast and the medication were equally injected in all procedures.
*An instillation of contrast material to confirm the exact intra-articular position of the needle before medication delivery.
†Comprised a mixture of steroid (triamcinolone) and anesthetic (ropivacaine) in an equal volume.
‡The forceful injection of the additional contrast material intended for the epidural spread after medication delivery.
LFJI, lumbar facet joint injection.
In short, the three-step injection with a total injectate volume of 2 mL or 3 mL and a three-image acquisition with oblique, AP, and lateral fluoroscopic capture images were performed for the respective facet joint.
Imaging analysis
The fluoroscopic imaging was reviewed by consensus of three radiologists who had participated in the procedures. Success of intra-articular LFJI, presence of ES, and patterns of the contrast distribution on ES were evaluated per procedure. The first author, one of the three radiologists mentioned above, recorded the basic data of the LFJI approach, including the injection method, the level, the laterality, the operator, and the total injectate volume, on the basis of medial record. Intra-articular LFJI was confirmed to be correct when sigmoid or ovoid filling of contrast material projecting over the corresponding facet joint was seen on the initial oblique projection (Fig. 1a). If not, the case was recorded as “targeting failure” and excluded from further analysis.
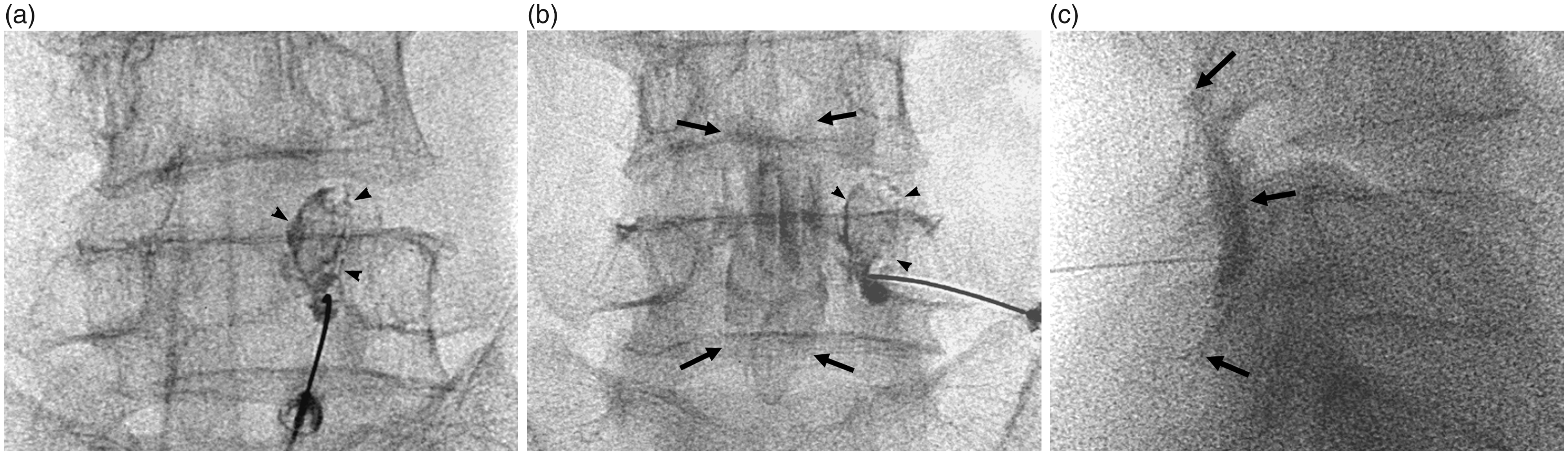
One-level bilateral facet joint injection at L4/5 in a 59-year-old woman. On the initial oblique projection (a), the needle tip is in the inferior portion of the right L4/5 facet joint, and the ring and ovoid filling of contrast material projecting over the corresponding joint is seen, confirming correct intra-articular LFJI. On the final anteroposterior (b) and lateral (c) projections, central spread is observed as the dispersed contrast material medial to the right pedicle projection (arrows, b) and anterior to the spinolaminar line (arrows, c). Foraminal spread is not seen. The distribution of the central spread is recorded as bilateral (crossing the spinous process on the AP projection), dorsal (confined to the posterior epidural space with a curvilinear filling and just anterior to the spinolaminar line), cephalad, and caudad (longitudinal contrast filling above and below the boundary of the facet arthrogram) spreads. The type of epidural spread pattern is bilateral central only. LFJI, lumbar facet joint injection; AP, anteroposterior.
ES was determined when central and/or foraminal spread was observed on the final two projections. Central spread was defined as: (i) medially dispersed contrast separated from the medial margin of the pedicle on the AP projection (Fig. 1b); and (ii) a curvilinear or tubular contrast spreading pattern delineating the epidural space, distinguished from the facet arthrogram (confined to the posterior element), on the lateral projection (Fig. 1c). Foraminal spread was defined as: (i) filling of the nerve root with contrast material along the inferomedial margin of the pedicle with or without (ii) an irregular and tubular-shaped extraforaminal extension along the spinal nerve sheath in an inferolateral direction on the anteroposterior projection (Fig. 2a).
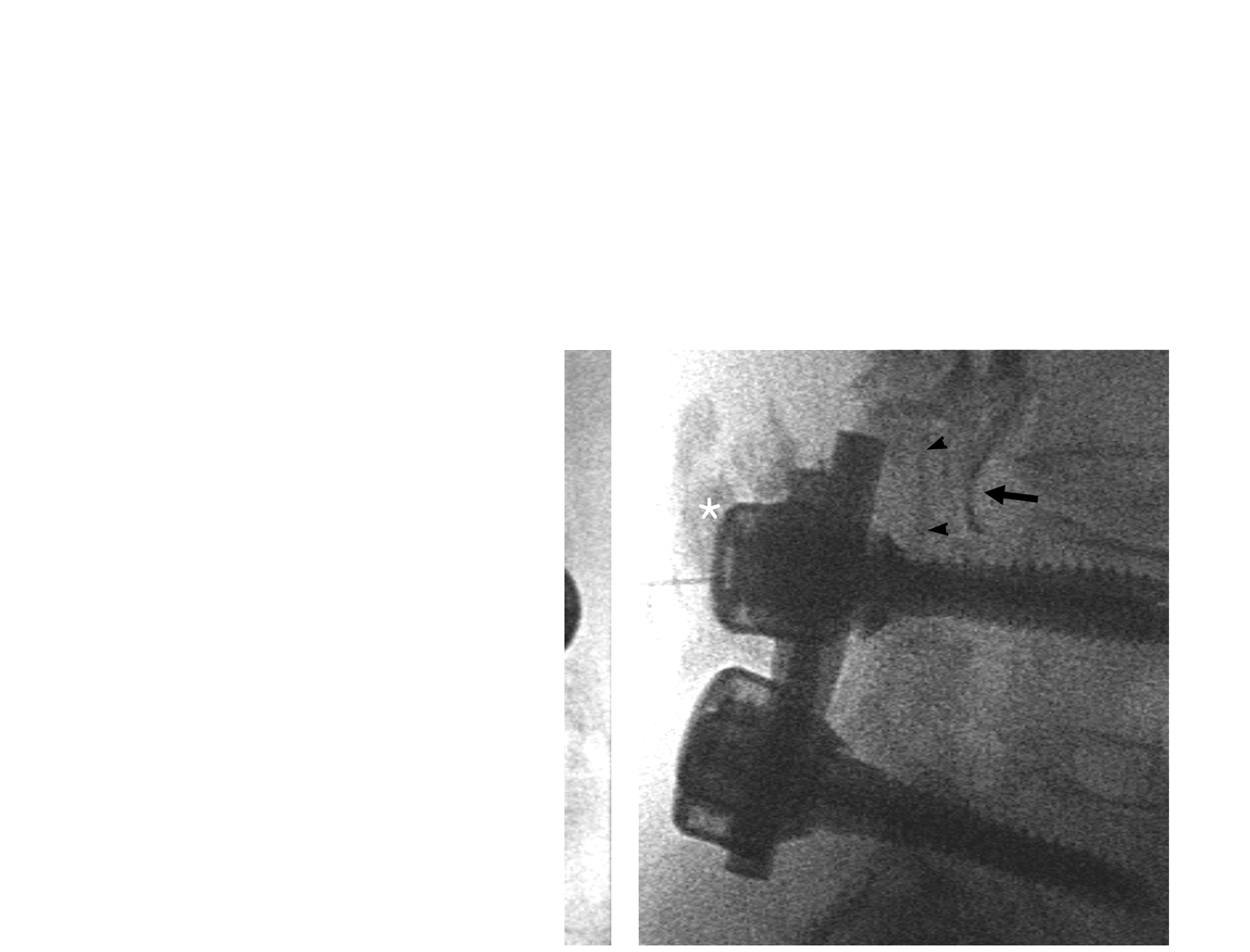
One-level bilateral facet joint injection at L3/4 in an 88-year-old man. On the final AP (a) and lateral (b) projections of the left L3/4 facet joint injection, there is not only a central spread but also a foraminal spread with typical nerve root filling along the inferomedial border of the pedicle in the neural foramen (arrows, a) and an extraforaminal extension. Foraminal spread is observed at the left L3/4 and L2/3 neural foramen, which is the same or above the level of the corresponding facet arthrogram (arrowheads) and therefore is recorded as the above spread. Distribution of the central spread is recorded as unilateral (not crossing the spinous process on the AP projection), dorsal and ventral (tubular-shaped contrast material spreading between the spinolaminar line and the posterior longitudinal ligament on the lateral projection), and cephalad (above the ring-shaped facet arthrogram) spread. The type of epidural spread pattern is unilateral, central, and foraminal. Paravertebral soft-tissue leakage in which the contrast material was flocculated at an unexpected location is accompanied by epidural spread; the injection is performed adjacent to the L4-5 posterior fusion level. LFJI, lumbar facet joint injection; AP, anteroposterior.
The central spread was further divided into subgroups according to the distribution of contrast material on three coordinate axes, relative to the corresponding facet arthrogram. Unilateral (Fig. 2a) and bilateral spread (Fig. 1b) depended on the contrast material crossing the spinous process on the AP projection. Dorsal spread was defined as a cresentic contrast pattern spreading superiorly and inferiorly, just anterior to the spinolaminar line (Fig. 1c), and ventral spread as extension of the contrast material along the posterior longitudinal ligament or abutting the posterior aspect of the vertebral body on the lateral projection (Fig. 2b). Cephalad or caudad spread was deemed to have occurred when an upward or downward contrast flow was identified superiorly or inferiorly to the boundary of the facet arthrogram on the final projections (Figs. 1b, 1c, 2a, and 2b). Foraminal spread was divided into above and below spread on the vertical axis when it was observed above or below the facet arthrogram (Fig. 2a). The patterns of ES were expressed as a combination of foraminal spread and central spread (unilateral or bilateral) by the increasing order of the extent: unilateral foraminal only; unilateral central only; unilateral central and foraminal; bilateral central only; and bilateral central and foraminal.
In addition, the other leakages were recorded when showing paravertebral soft-tissue leakage or abnormal communication (horizontal or vertical communications). The presence of spondylolisthesis at the level of LFJI and whether the LFJI was performed just above or below the posterior fusion level were also evaluated based on the fluoroscopic images (Fig. 2).
Statistical analysis
Potential predictors of ES were analyzed for statistical significance using the chi-squared test, Fisher’s exact test, or a t-test. Patient age, sex, and other factors associated with the procedure (injection level, total injectate volume, spondylolisthesis, adjacency of posterior fusion level, and other leakage) were analyzed using relative risk (RR) ratio. We also examined the ES pattern with regard to laterality, the injection method used, and the operator to exclude technical factors. P values < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 21.0 software (IBM Corp., Armonk, NY, USA).
Results
Patient demographics
In total, 100 patients underwent 200 LFJI procedures during the study period. One patient was excluded because both LFJI procedures failed and eight injections were excluded because of targeting failure, leaving data for 99 patients and 192 procedures available for analysis. The LFJIs were mostly performed via L4/5 (104 of 200 cases; see Table 2). The numbers enrolled in the two different total injectate volume groups were approximately equal. Spondylolisthesis was identified in 67 (33.5%) cases and the adjacency of the posterior fusion level was identified in 15 (7.5%) cases. Of the 192 cases of intra-articular LFJI, other leakage was observed in 109 (56.8%) cases.
Description of procedural details.
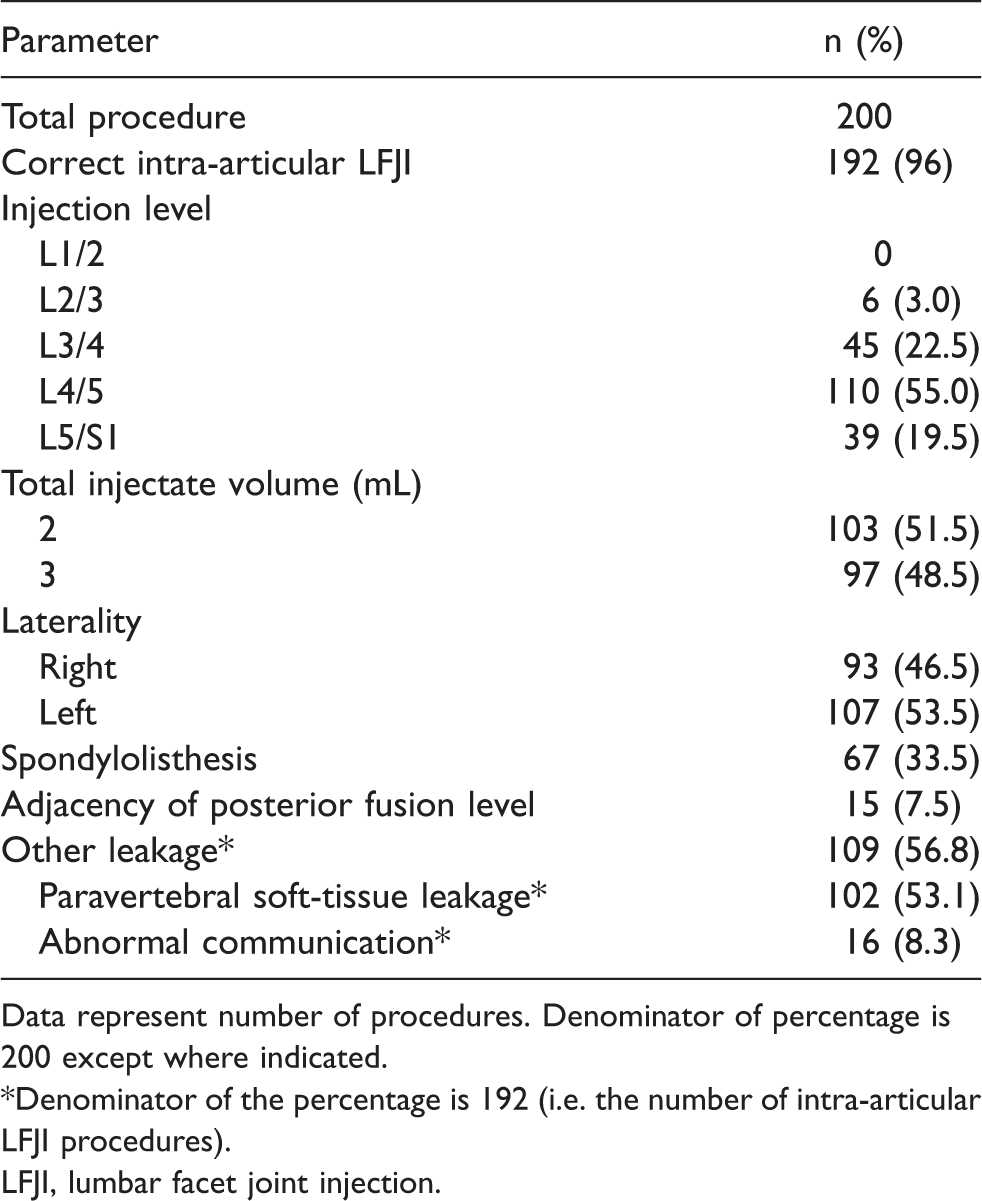
Data represent number of procedures. Denominator of percentage is 200 except where indicated.
*Denominator of the percentage is 192 (i.e. the number of intra-articular LFJI procedures).
LFJI, lumbar facet joint injection.
Incidence and contrast pattern of ES
The overall incidence of the ES patterns in the LFJI is shown in Table 3. The incidence of ES during LFJI was 64.6% (n = 64) in 99 patients and 49.5% (n = 95) in 192 procedures. Among the 95 procedures with ES, central spread occurred in 91 (95.8%) cases, foraminal spread in 35 (36.8%) cases, and ventral spread in 56 (58.9%) cases. Unilateral (70/95, 73.7%), dorsal (88/95, 92.6%), and cephalad (92.6%) distributions were identified in most cases of ES. Ventral and caudad distributions were usually accompanied by their counterparts, although three cases of ventral distribution only and two cases of caudad distribution only were observed. Foraminal spread above invariably occurred in all cases of foraminal spread. The unilateral central only type was most commonly identified, followed by unilateral central and foraminal, bilateral central only, bilateral central and foraminal, and unilateral foraminal only. Foraminal spread was usually combined with central spread except in four cases where the spread was foraminal only.
Epidural spread patterns in LFJI.

Data represent numbers of procedures. The denominator of the percentage is 192 (i.e. the number of intra-articular LFJI).
*Contrast pattern on the level relative to the corresponding facet arthrogram was evaluated in cases of foraminal spread.
†Contrast pattern in the frontal axis (unilateral or bilateral), sagittal axis (dorsal or ventral), and vertical axis (cephalad or caudad) was evaluated in cases of central spread.
LFJI, lumbar facet joint injection.
Potential predictors of ES
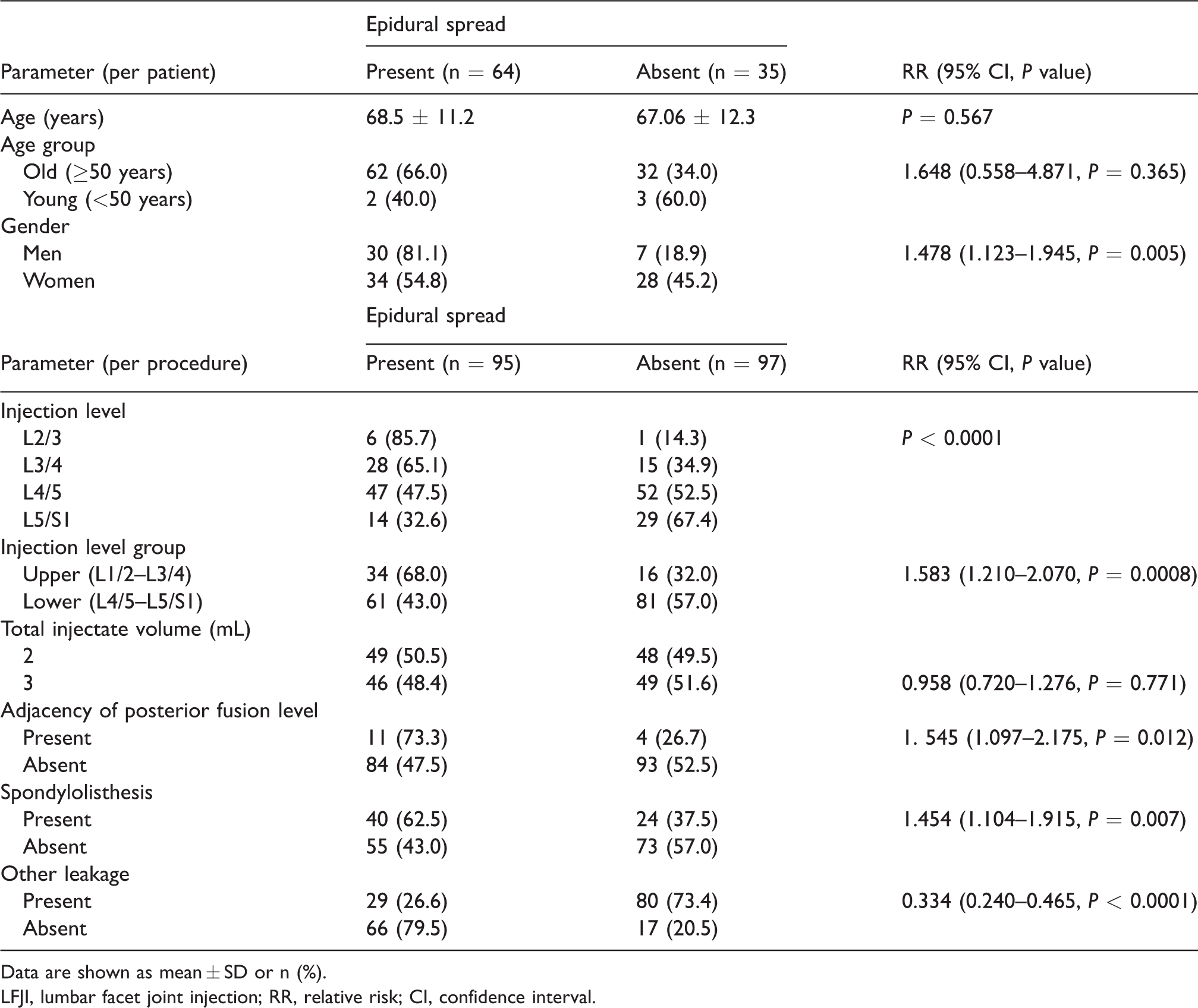
No difference in the rate of ES was found with regard to laterality (P = 0.658), the injection method used (P = 0.673), or the operator (P = 0.868). As shown in Table 4, ES occurred more frequently (RR = 1.478, P = 0.005) in men (81.1%) than in women (54.8%). The incidence of ES increased significantly in the caudocephalic direction (L2/3 = 85.7%, L3/4 = 65.1%, L4/5 = 47.5%, L5/S1 = 32. 6%) and was higher in cases with spondylolisthesis (62.5%, RR = 1.454, P = 0.007) and adjacency of posterior fusion level (RR = 1.545, P = 0.012). The older age group had a higher ES rate than the younger age group, but the difference was not statistically significant (RR = 1.648, P = 0.365). ES occurred with similar frequency in the groups that received 2 mL (50.5%) or 3 mL (48.4%) of total injectate volume (RR = 0.958, P = 0.771). Other leakage was strongly associated with ES (RR = 0.334, P < 0.0001), but there was a somewhat exclusive and inverse relationship in that most cases (146/192, 76.0%) were classified as either other leakage only or ES only.
Potential predictors of epidural spread in LFJI.
Data are shown as mean ± SD or n (%).
LFJI, lumbar facet joint injection; RR, relative risk; CI, confidence interval.
Discussion
In this study, ES occurred in almost half (53.1%) of the LFJI procedures that were performed. These findings suggest that ES occurs in a significant number of cases during LFJI, but it may also mean that intra-articular FJI cannot completely replace epidural injection in terms of epidural access. We think it is more important that ES during the LFJI may be an alternate way to access the epidural space where direct epidural access is not feasible, such as posterior epidural space obliteration in the severe spinal stenosis, interlaminar space block due to severe degenerative change, or postoperative state such as laminectomy, because the results of this study showed the possibilities of spread of contrast/drugs to the epidural space of injected level. Other possible clinical utility of ES in the LFJI is managing lumbar radiculopathy in patients with a high risk of bleeding (who take anticoagulants). In fact, LESI is known as a very safe procedure and epidural hemorrhage related with epidural injection is a very rare, but potentially serious because neurological complications may be more severe in the presence of spinal stenosis (16–18). LFJI is safer than an epidural injection in terms of bleeding risk (particularly epidural hematoma) because the needle does not reach the epidural space. However, a case report of delayed onset epidural hematoma after FJI has been reported (19). It is necessary to investigate the safety of the ES during LFJI for epidural hemorrhage compared to the epidural injection. In practice, except in these cases, the valid use of FJI is for rupture or for injecting a facet joint synovial cyst and possibly for chronic pain related to vertebral compression fracture since medial branch RFA is not valid at the thoracic levels.
The method of approach with regard to the target site and the consequent contrast pattern may reflect the therapeutic effect in LESI because it has been suggested that the therapeutic effect would be better if delivered closer to the site of pathology (20–24). According to our study, the contrast pattern of ES in LFJI tends to be more similar to that of the interlaminar approach than the transforaminal approach, in agreement with previous studies showing that the contrast is predominantly distributed in the dorsal epidural space rather than in the ventral epidural and foraminal spaces, and cephalad-dominant flow was observed (25–29). On an anatomic basis, there are two potential routes for ES in LFJI, i.e. an anteromedial capsule and a superior recess (12). In our daily clinical practice, we have found that ES mostly occurred because of rupture of the anteromedial capsule rather than direct extension from the superior recess on real-time fluoroscopy. This observation is consistent with the contrast pattern seen in our study because the rupture point of the anteromedial capsule is posterior to the dorsal epidural space between the spinous process and the pedicle (30,31). The level of the anteromedial capsule is the same or higher than that of the interlaminar space (30,31), which is the level of the interlaminar approach. For this reason, LFJI can be compatible with interlaminar LESI, although the overall incidence of ventral (29.2%) and foraminal (18.8%) spread during LFJI approximates that of the midline interlaminar approach. In addition, contrast material mostly flows superiorly and foraminal spread invariably occurs at least at the same level of the corresponding facet joints (e.g. no lower than the L4/5 neural foramen in the case of L4/5 LFJI). Therefore, we recommend that the injection level for LFJI should be at the same level as the targeting neural foramen. As mentioned above, ES mainly occurred through the anteromedial capsule, which is replaced by ligamentum flavum (32) and we postulated that the integrity of the ligamentum flavum, as well as facet arthrosis, is an important factor for ES in LFJI. The facet joint is a crucial component in the stability of the lumbar spine, so laxity and degeneration of the ligamentum flavum is strongly associated with segmental instability in facet joint degeneration (33,34). This condition would make the ligamentum flavum fragile and increase the chance of rupture in LFJI.
The ideal volume of a LFJI has been reported to be 1–2 mL (35). The facet capsule can rupture and extravasation in the epidural space or the paravertebral soft tissue inevitably occurs when the injectate volume exceeds the capacity, which is >2 mL in the intra-articular LFJI (13,36). Further, Moran et al. (13) suggested that extravasation occurs in the epidural space rather than in the paravertebral tissue, which increases the possibility of ES by injecting a larger volume. In our study, extravasation occurred in most cases (91.1%), which is consistent with the former, while the incidence of ES was similar when a larger injectate volume was used (50.5% for 2 mL vs. 48.4% for 3 mL), in conflict to the latter. Therefore, we recommend that the total injectate volume should not be >2 mL when attempting to achieve ES during LFJI. Other important information for LFJI is the dose which did not permit extravasation of joint space. In our study, injections of 2 mL or 3 mL were used and an average of 50% of the patients developed ES. In general, considering a total of 1 mL of medication (triamcinolone acetonide and ropivacaine hydrochloride) is injected for LFJI, it is necessary to minimize the amount of test and push contrast to not exceed the joint capacity when the injection is performed in patients who do not require ES. It is also thought that further study of the incidence of ES in <2 mL of injection we used in this study will be needed. In this type of intra-articular FJI, it must be considered that the ES can cause damage to the anatomical structures that make up the facet joint. In fact, it is not clear how the anatomical damage by ES affects the normal joint; there is a possibility that the degeneration of the normal joint may accelerate or chronic pain can be induced due to the disruption of normal joint capsule, cartilage injury, or increased joint pressure in the process of epidural rupture. In this respect, it is thought that ES should be avoided in relatively young patients.
Our study has some limitations. First, we did not correlate ES with therapeutic outcome or clinical diagnosis; however, we used an anatomic consistency of contrast distribution as the outcome and believe that this provides objective and reasonable evidence for LFJI as an alternative to epidural injection given the suggestion that the therapeutic effect depends on the proximity of drug delivery to the site of pathology (37,38). In cases of ES during LFJI, the diagnosis is ambiguous, but efficacy might be better. Therefore, further evaluation from this study is efficacy difference from ES or not during LFJI. Second, we did not consider the relationship between location of the needle and the contrast pattern of ES. Third, in this study, we focused on the incidence of ES and performed only a limited analysis of the potential predictors of ES. There is a need to conduct more research on a wide range of imaging and clinical factors for ES.
In conclusion, ES occurred in about half the number of LFJIs in this study and showed a contrast pattern similar to that seen with the interlaminar approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.