
Abstract
Background
Hybrid SPECT/CT systems allow the shortening of lead time for investigation of cancer patients, since a complementary CT for radiological characterization of focally increased isotope uptake of unclear origin in bone scintigraphy can be performed simultaneously. The use of low-dose CT (sub-mSv CT) reduces radiation dose compared to standard-dose CT and facilitates the application of complementary CT.
Purpose
To test the feasibility of sub-mSv CT for the characterization of non-specific findings in the bone scintigraphy of oncological patients.
Material and Methods
Nineteen oncological patients with a total of 50 findings of unclear origin on bone scintigraphy which required further correlation with morphologic data were included in the study. Each patient underwent two CT scan series consecutively: one low-dose CT and one standard-dose CT. The CT studies were randomized and each finding was rated by four blinded experienced radiologists. A shift in ratings between standard-dose and low-dose images were assessed using the Stuart–Maxwell chi-squared test. Inter-observer agreement and intra-observer agreement was assessed using Light’s kappa and Cohen’s kappa, respectively.
Results
The mean effective dose of low-dose CT scans was 0.8 mSv compared to 4.2 mSv for the standard-dose CT scans. No statistically significant shift in ratings was observed (P = 0.62). There was no statistically significant difference in the inter-observer agreements: the values for the standard-dose and low-dose groups were 0.68 (95% confidence interval [CI] 0.57–0.79) and 0.60 (95% CI 0.47–0.72), respectively.
Conclusion
These results indicate that sub-mSv CT for characterization of non-specific findings in bone scintigraphy of oncological patients is feasible.
Keywords
Introduction
Bone scintigraphy is a standard examination in the diagnosis of skeletal metastases in different types of tumors, mostly prostate cancer and breast cancer. The rationale behind this method is that the majority of bone metastases are accompanied by an osteoblastic reaction which can be seen as a focally increased tracer uptake (1). However, as elevated osteoblastic activity also occurs in benign conditions such as fractures and degenerative diseases, scintigraphy findings are not always easy to characterize via bone scan alone (1). For this reason, a complementary radiological assessment with radiographs, computed tomography (CT), or magnetic resonance imaging (MRI) (1,2) is required. Hybrid imaging with a single photon-computed tomography (SPECT)/CT allows a complete investigation of patients in one examination, thereby reducing the time of the bone metastases assessment.
The effective dose of bone scintigraphy performed according to European guidelines is approximately 3 mSv (3). Supplementary standard diagnostic CT with a scan length of 50 cm typically results in additional effective doses of about 7–11 mSv (4). Considering that the reason for complementary examination in bone scintigraphy is skeletal changes, which are usually well visible on CT scans, a low-dose CT examination might be sufficient for these purposes (5).
There are several studies available in diagnostic radiology evaluating whether the reduction of radiation doses can provide similar image quality in skeletal studies (6–9) and in other organs (10,11). To our knowledge, there are two studies that evaluated the utility of low-dose CT in association with bone scintigraphy, though none of these studies consisted of strictly oncological patients (12,13). The first study (12) found that a final diagnosis was reached in only 59% of cases with low-dose CT protocol (2 mSv). However, no comparison with the standard-dose protocol was performed and image quality in present SPECT/CTs have improved radically (most notably multiplanar) since 2007 when it was published. The second study (13) found an improvement in bone image quality with a low-dose protocol (1.8 mSv) in combination with a medium smooth filter. However, that study assessed image quality while varying several parameters including dose (reduced radiation dose by itself can only decrease image quality). The aim of this study is to use the same (optimized) parameters for both groups and compare the diagnostic outcome between the standard-dose and a low-dose (sub-mSv) protocol, under the hypothesis that low-dose (sub-mSv) CT for characterization of nonspecific findings in bone scintigraphy of oncological patients is feasible.
Material and Methods
Study design
During the period of May to December 2015, all oncological patients, mostly patients with prostate cancer, that were referred to our department for bone scintigraphy with 99mTc-HDP were screened for the study. The inclusion criteria were: patients aged > 60 years with two or more focal uptakes in the lower spine and/or pelvis, which, after assessment of bone scintigraphy, was considered to be of unclear origin and required further radiological examination, and who agreed to volunteer in the study. Nineteen patients (15 men, 4 women) with a total of 50 uptakes were recruited (mean ± SD for age and body mass index [BMI] were 74 ± 10 years and 25 ± 4 kg/m2, respectively). The study was approved by the Regional Ethical Board (2015/581-31/4) and local Radiation Protection Committee (2.2 K0721-201, 1037891). All patients signed an informed consent.
The study protocol consisted of whole-body bone scintigraphy, directly followed by standard-dose CT and (without repositioning) an additional scan series with the low-dose CT (Fig. 1).
(a) Increased uptake in one area of the lower thoracic spine, in the lumbar spine, and in the pelvis. (b) Low-dose CT that shows metastasis and (c) Standard-dose CT. CT, computed tomography.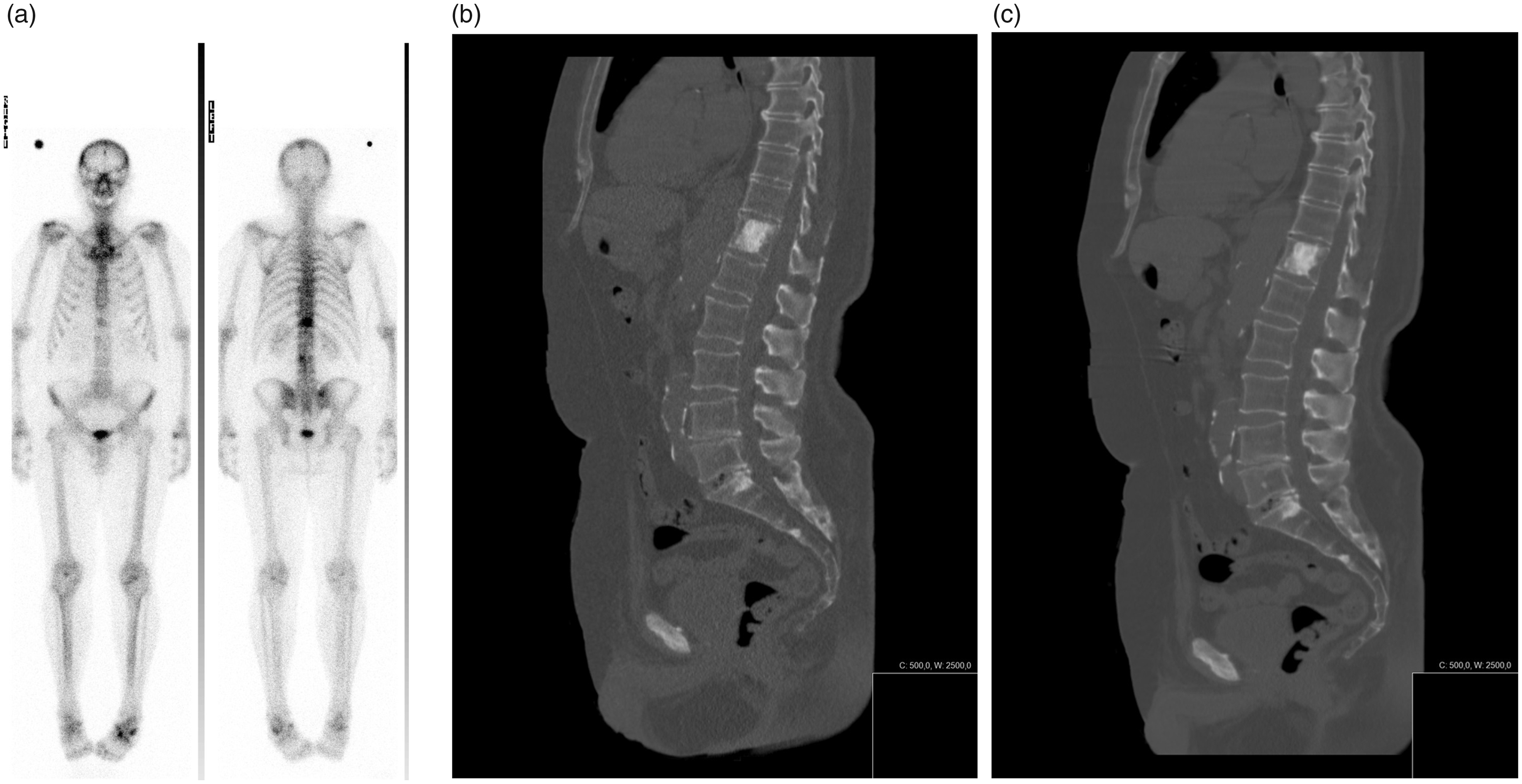
Scan protocols
All examinations were performed on a Siemens Emotion 16-slice SPECT-CT (Siemens, Forchheim, Germany). The whole-body bone scintigraphy was performed according to European Guidelines (3). The CT scan parameters and level of dose reduction was based on pilot phantom tests (Rando phantom (14), with a human skeleton) performed previously at the department. Side-by-side comparison of phantom scan images with different combinations of mAs was performed by radiologists to decide the dose level for the low-dose group.
Both CT protocols were identical except the quality reference mAs, which were reduced from 89 in the standard-dose protocol to 17 in the low-dose protocol (Table 1). A medium smooth reconstruction kernel (B31) was used to reduce image noise while still being deemed to have enough resolution for the imaging task. According to the quality assurance test of the department, this kernel has a resolution of approximately 6.5–8.2 lp/cm (as measured by the 10% and 2% modulation transfer function, using the manufacturer phantom and built-in software), which is probably enough for viewing skeletal details of size roughly ≥1.5 mm.
Scan parameters for the two groups.
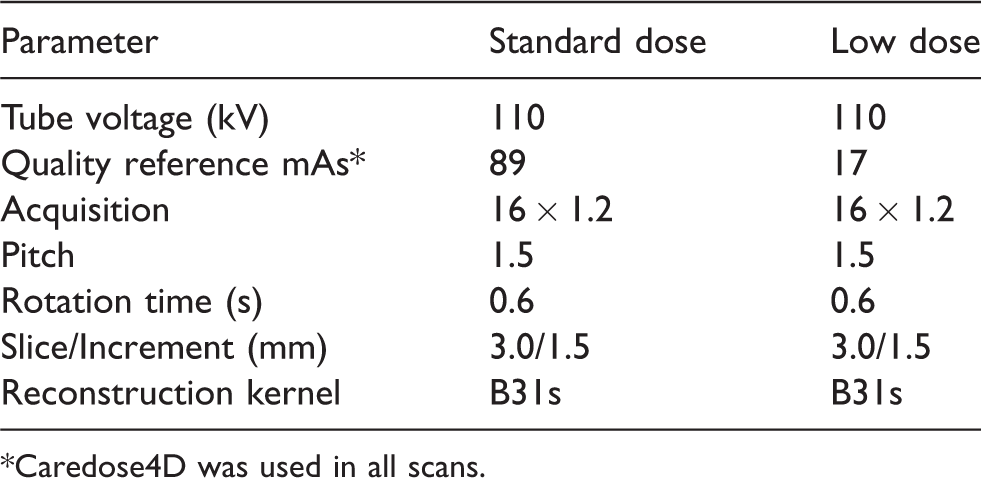
*Caredose4D was used in all scans.
Radiation dose
Mean effective mAs, CTDIvol, and dose-length product for each scan series were taken from the patient protocols. Estimates of the effective dose were performed using a conversion factor of 0.015 mSv/mGycm (15).
Image readings
Two sets of images consisting of bone scintigraphy paired with either low-dose or standard-dose CT were prepared. The images were anonymized and randomly divided into two lists for reading, so that both lists contained either the standard-dose or low-dose examination of each patient in random order. Before the readings, one of the readers viewed all bone scintigraphy images and defined two or three positions (average = 2.6) of focal tracer uptake in the lower spine and/or pelvis for each patient. These predefined uptake findings were later read by four experienced radiologists (one of them an expert in musculoskeletal radiology) and rated (1 = benign lesion, 2 = malignant lesion, 3 = no finding, 4 = do not know). Two of the readers first rated the findings in the first list and later rated the second list, while the other two readers began with the second list. A minimum of one month between rating the two lists was allowed, to minimize a probable remaining impression from the reading of the images in the first session.
Main outcome measures
The main outcome test was shift in ratings (1 = benign lesion, 2 = malignant lesion, 3 = no finding, 4 = do not know) when using the low-dose images compared to the standard-dose images. In addition, the inter-observer agreement when using the standard-dose images was compared to the inter-observer agreement when using the low-dose images. Lastly, the intra-observer agreement (i.e. each reader’s agreement with him/herself when using the standard-dose and low-dose of the same patient) was calculated.
Statistical analysis
To test for a shift in ratings, a Stuart-Maxwell chi-squared test for marginal homogeneity was performed, using the software MH Program v. 1.2 (16). The inter-observer agreement was assessed and compared by using the Light’s kappa (mean value of Cohen’s kappa values for all readers) with bootstrapped 95% confidence intervals (CI), calculated in the psy- and boot library in the statistical software R v. 3.4.4 (R Foundation for Statistical Computing, Vienna, Austria). To test the difference between the Light’s kappa values, a distribution of differences was generated through bootstrapping by subtracting each bootstrapped low-dose Light’s kappa value from the standard-dose kappa value. If the 95% CI of the difference distribution did not overlap zero, this was considered significant. Intra-observer agreements were quantified as the Cohen’s kappa using the psy-library in R.
Results
Nineteen patients aged > 60 years were recruited for this study. A total of 50 focally increased 99mTc-HDP-uptakes were selected for further evaluation. The uptakes were positioned in the spine (n = 29), pelvis (n = 19), and proximal femur (n = 2).
No statistically significant shift in ratings was seen for any reader between the standard-dose and low-dose studies using the Stuart–Maxwell test (Tables 2 and 3). There was no statistically significant difference in the inter-observer agreements: the Light’s kappa values for the standard-dose and low-dose group were 0.68 (95% CI = 0.57–0.79) and 0.60 (95% CI = 0.47–0.72) with a difference of 0.08 (95% CI = -0.075–0.25). The mean intra-observer agreement was 0.72 (0.77, 0.76, 0.65, and 0.68 for raters 1–4, respectively).
Summarization of all ratings for the paired standard and low-dose images for each of the four raters.
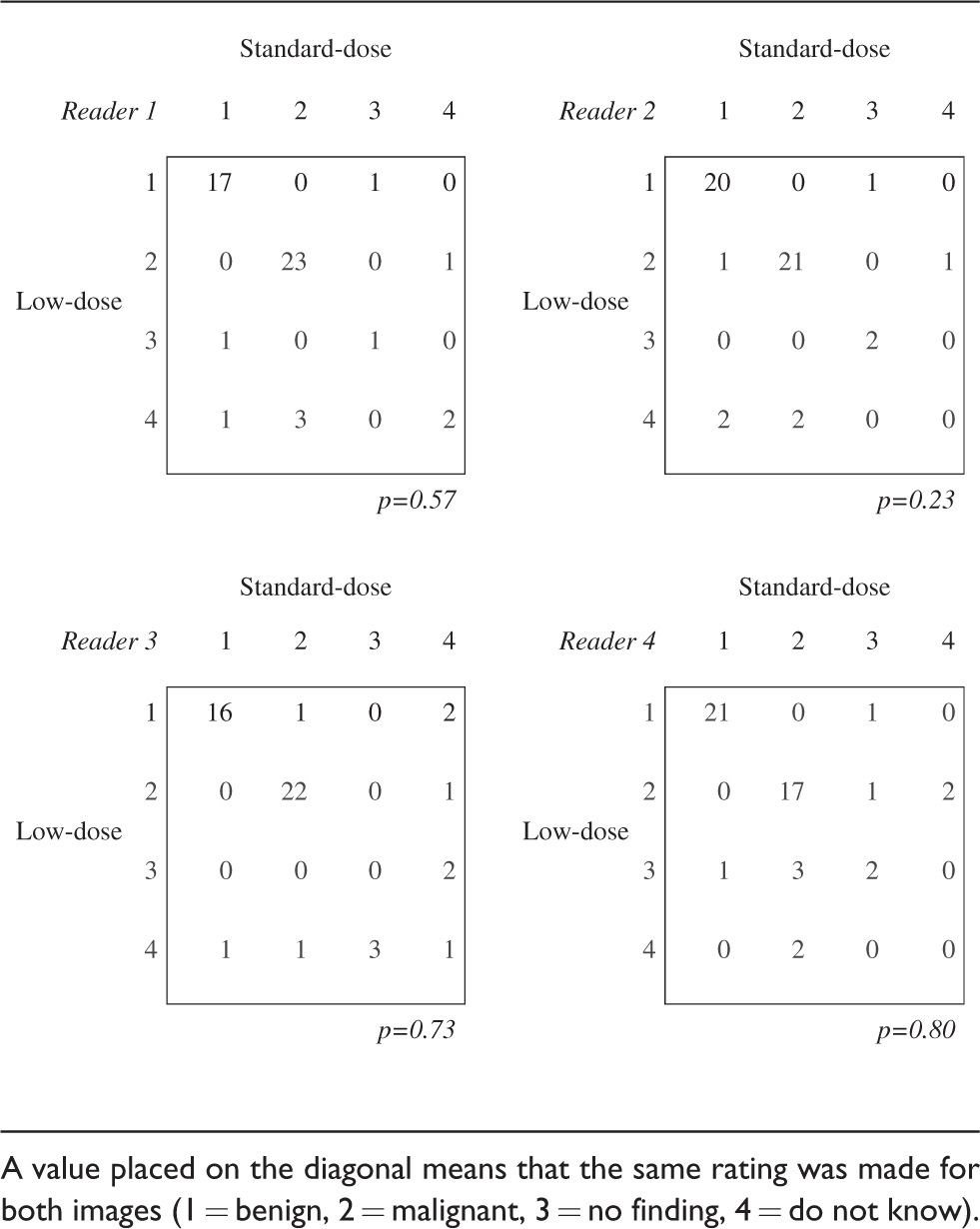
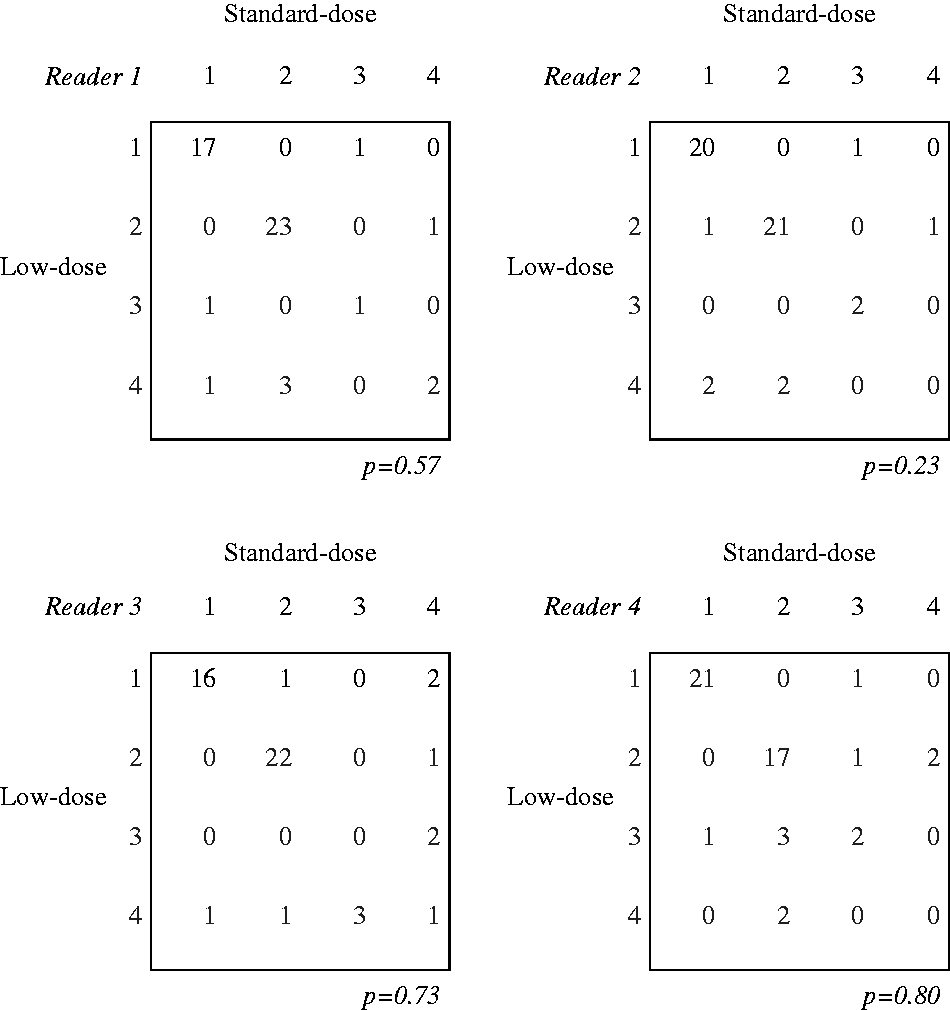
A value placed on the diagonal means that the same rating was made for both images (1 = benign, 2 = malignant, 3 = no finding, 4 = do not know).
The sum of all four readers’ ratings from Table 2.
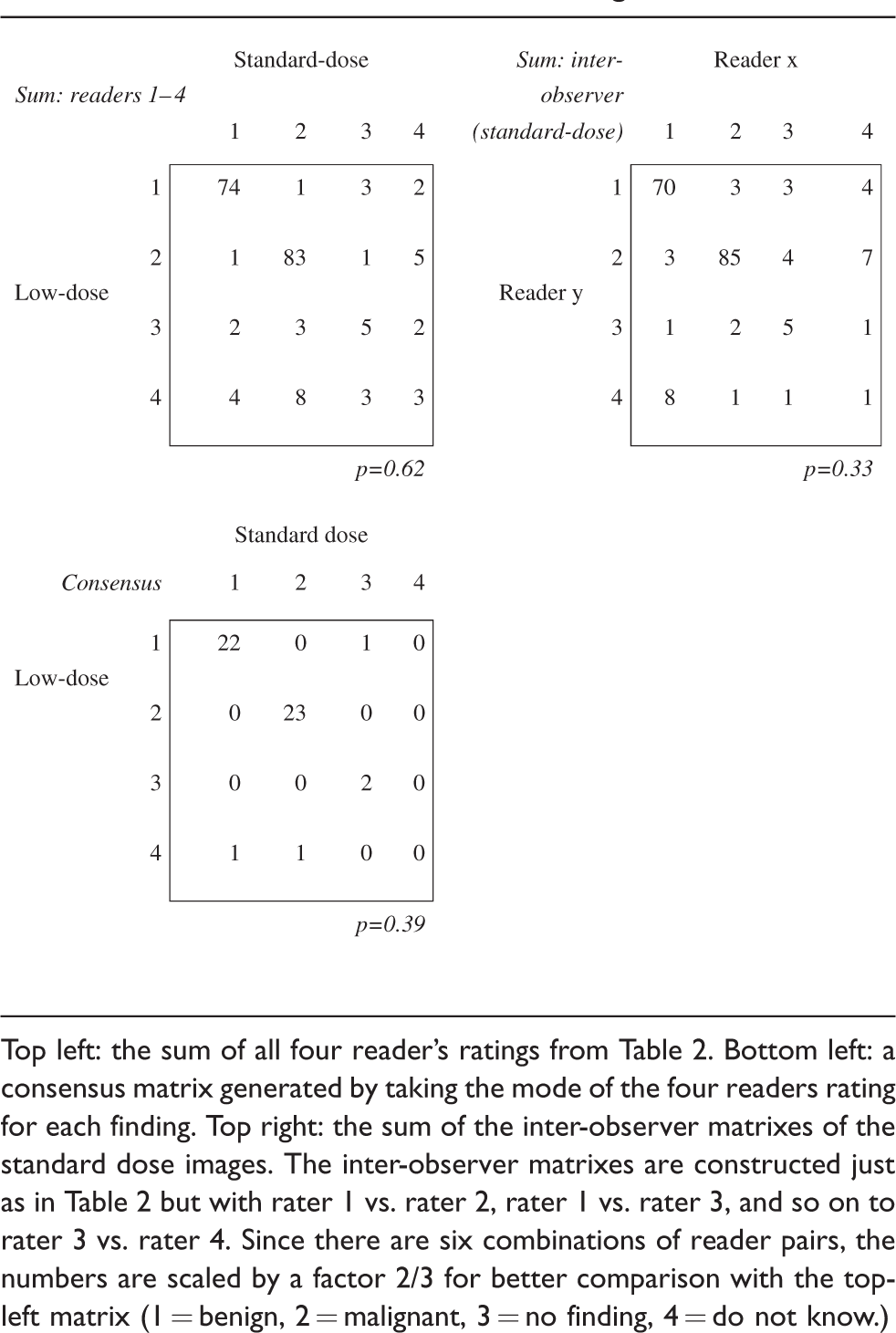
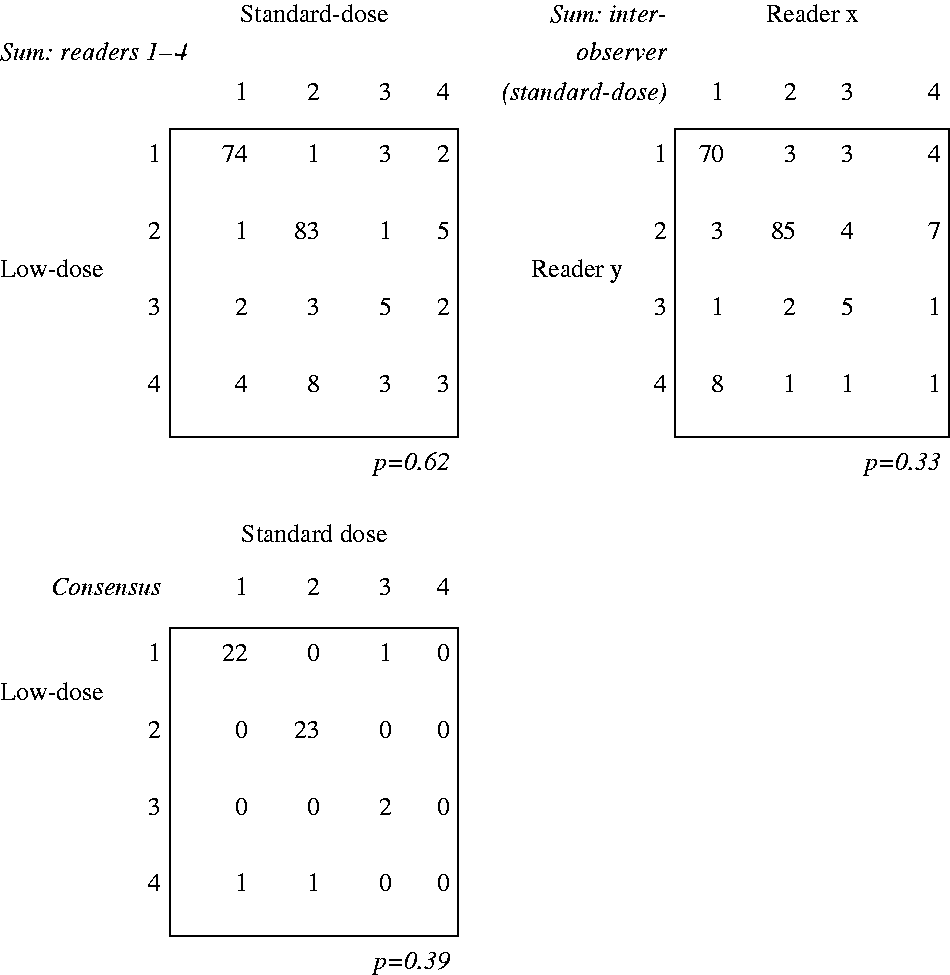
Top left: the sum of all four reader’s ratings from Table 2. Bottom left: a consensus matrix generated by taking the mode of the four readers rating for each finding. Top right: the sum of the inter-observer matrixes of the standard dose images. The inter-observer matrixes are constructed just as in Table 2 but with rater 1 vs. rater 2, rater 1 vs. rater 3, and so on to rater 3 vs. rater 4. Since there are six combinations of reader pairs, the numbers are scaled by a factor 2/3 for better comparison with the top-left matrix (1 = benign, 2 = malignant, 3 = no finding, 4 = do not know.)
For the 200 uptake readings (50 findings times 4 raters), a total of 13 clinically relevant changes in ratings from the standard-dose to low-dose studies were observed (Table 4). The corresponding number of changes in ratings between different readers of the standard-dose studies was also 13 (an average of 9 and 17, depending on the direction) per 199 readings.
The number of clinically relevant rating changes from the standard-dose to the low-dose images, compared to the rating changes between observers for the standard-dose images (from Table 3).

The mean effective dose of the standard-dose and low-dose group was 4.2 mSv and 0.8 mSv, respectively (Table 5).
Radiation doses for both groups.
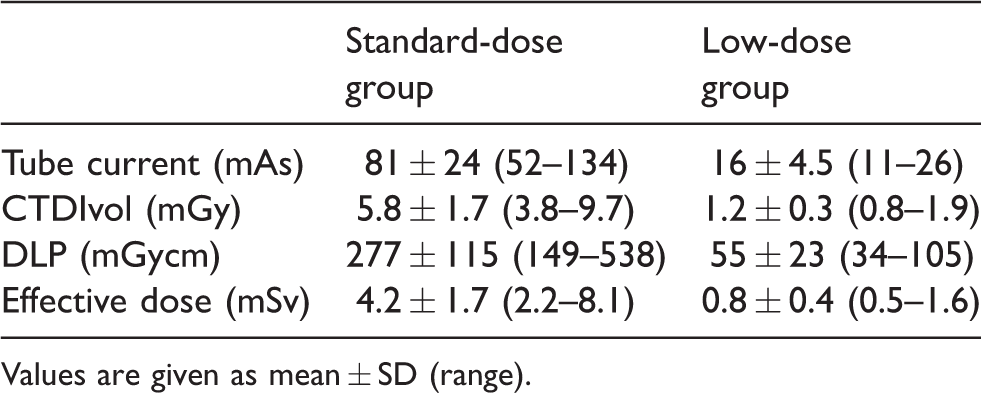
Values are given as mean ± SD (range).
Discussion
To our knowledge, this is the first prospective study in nuclear medicine in which a double set of images of the same patient was used to directly compare the diagnostic results of standard-dose and low-dose CT in bone scintigraphy. This approach allows more direct comparison than what was previously provided by other studies using a retrospective design and a different cohort of patients (6–8,13). The design of the present study is aimed to test whether the low-dose CT provides sufficient image information to make the same decision as the standard CT in those areas with increased tracer uptake and not just to assess image quality as in previously published studies (10,13,17).
There was no statistically significant shift in ratings between the standard dose and low dose or between the observer agreement when using the standard-dose versus the low-dose images. Failure to reject the null hypothesis in a small sample could either mean that there is indeed no difference or that the sample was too small; hence, there is a need for a larger study.
In Table 3, we have summed up all the raters’ readings in standard dose versus low dose and, for the sake of comparison, generated an analogous for rater versus rater (inter-observer) in the standard-dose case. The matrices are very similar; the raw number of changes are almost the same, a couple more in the inter-observer matrix. This is also reflected in the fact that the intra-observer agreement (same observer looking at standard dose versus low dose) was 0.72 on average compared to the inter-observer agreement (different observer looking solely at standard dose) of 0.68. These two comparisons indicate that, based on these data, there is no reason to assume that the low-dose images introduce more changes in ratings than merely having different raters viewing the standard-dose images. In Table 3, we have also generated a consensus matrix by taking the mode of the raters. As can be seen from this matrix, there were three occasions where the consensus changed from the high-dose to the low-dose case. On these three occasions, there were only two raters who made the corresponding change in rating. It is difficult to assess the significance of these changes. In Table 4, we have made a summary of all of the clinically relevant changes in ratings when going from standard dose to low dose and compared that to the changes when going from one rater to another using only the standard-dose images (normalized as in Table 3). Table 3 indicates that the number of clinically relevant changes in ratings introduced by using the low-dose images does not seem higher than having different raters viewing the standard-dose images.
There are several limitations of our study. First, the sample size is small; 19 patients with a total of 50 findings. Second, it is unclear to what extent the findings can be considered independent. Since the 2–3 findings per patient (either standard dose or low dose) were viewed consecutively in the same image stack, “that favored treating them dependent.” However, in older patients (such as these), it is common to have benign degenerative findings in the skeleton, so the raters were actively expecting the next finding to be either malignant or benign, regardless of the previous finding, which suggests they could be considered independent (although some expectation bias is likely). With regard to image quality, the situation is a mix between independent and dependent, but the dependency is largely eliminated since the same finding is compared in the standard-dose and low-dose images. There was image quality variation within patients (from finding to finding) due to inter-slice and intra-slice variance in noise related to the sampling, longitudinal variance in patient thickness, anatomical surroundings, and anatomical noise. Meanwhile, there was image quality correlation within patients due to factors like overall patient size, centering error, etc. These factors are all identical in the standard-dose and low-dose images (except for the sampling-related variance). Third, no pre-study power calculation was performed, which limits the ability to draw conclusions when the null hypothesis is not rejected. Fourth, we did not take into consideration the image quality changes depending on the person’s BMI (6). Even though we had gathered the BMI values of our patients (average = 24.9 kg/m2; range =18–35 kg/m2), we decided not to perform such analysis because of the limited number of patients. The pilot phantom tests were performed on a phantom representing a small adult. This means that large patients could have been noisier than expected (since the automatic exposure control, Caredose 4D, by design does not maintain constant noise for large patients). Reviewing the BMI of the patients with clinically relevant rating changes indicate that there may be an overrepresentation of larger patients; however, the number of cases is too few to draw any firm conclusions.
The low-dose CT protocol resulted in dose reduction of about 80% compared to the standard-dose protocol. The dose level of the low-dose protocol in our study is comparable with radiographs’ doses (5). Such low-radiation doses may enable delegation of the decision of complementary CT in association with bone scintigraphy to the nuclear medicine technicians or radiographers after appropriate training.
In conclusion, sub-mSv CT seems feasible for morphological characterization of skeletal changes in areas with increased tracer uptake on bone scintigraphy. The results of this study could now be tested in a larger population to replace a standard-dose CT protocol with a sub-mSv-dose CT protocol as a complementary study for bone scintigraphy in daily practice in nuclear medicine departments.
Footnotes
Acknowledgements
The authors thank Annie Bjäreback for her contribution in planning and the preparation of images for review. They would also like to thank Bertil Leidner for sharing his knowledge and expertise in the CT protocols.
Declaration of conflicting interests
The author(s) declared no potential conflict of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.