
Abstract
Background
Imaging evaluation of femoroacetabular impingement (FAI) plays a major role in early diagnosis and treatment, preventing irreversible degenerative changes in hip joints.
Purpose
To investigate the anatomical parameters associated with FAI in a Chinese asymptomatic population by computed tomography (CT) and to evaluate the prevalence of the radiographic features of cam and pincer types in Chinese patients.
Material and Methods
We reviewed the CT images of 470 hips in 235 Chinese patients who underwent abdominal and pelvic CT scans for reasons unrelated to hip symptoms at our hospital between February and October 2017. The following measurements were made on each hip joint: acetabular version angle (AV); anterior acetabular sector angle (AASA); posterior acetabular sector angle (PASA); the lateral center edge angle (LCE); the alpha angle (AA); and femoral head-neck offset (FHNO).
Results
Significant differences in all parameters were seen between men and women. Young men and elderly women showed more retroversion in our study. LCE, AA, and FHNO were all larger in men than women. The data showed 25% of female joints and 34.5% of male joints had at least one predisposing factor for FAI using measurement parameters by CT images in Chinese asymptomatic patients, and the prevalence of pincer lesion (19.1%) was larger than cam lesion (9.1%).
Conclusion
Morphological features associated with FAI are also present in Chinese asymptomatic patients. The threshold values for abnormal parameters should be reconsidered based on gender, age, and other factors in order to improve the accuracy of diagnosis.
Introduction
Femoroacetabular impingement (FAI) has been found to cause adult hip pain and progressive degenerative changes leading to early osteoarthritis (OA) of the hips (1–4). It is defined as an impingement due to abnormal contact during hip motion between the proximal femur and rim of the acetabulum which leads to hip labral and cartilage injuries. Three types of FAI have been described: (i) cam impingement (deformities of the femoral head-neck junction); (ii) pincer impingement (overcoverage of the acetabulum); and (iii) mixed impingement (a combination of cam-type and pincer-type) (5,6).
To support the clinical diagnosis of FAI, many imaging parameters have been suggested and used clinically for its diagnosis. Imaging evaluation of FAI plays a major role in early diagnosis and treatment, preventing irreversible degenerative changes in hip joints (7). At present, most data related to FAI have been obtained from studies of Caucasians in Western countries, reporting a relatively high prevalence of FAI-related morphologic features (8–11). Little is known about the true prevalence of morphological features associated with FAI in Asians, especially Chinese populations. Therefore, the aim of the present study was to investigate the anatomical parameters associated with FAI in a Chinese asymptomatic population by high-resolution reconstructed multislice computed tomography (CT) images, and to determine the prevalence of the radiographic features of cam and pincer types in Chinese patients.
Material and Methods
Our institutional research review board approved the study and the requirement for patient consent was waived.
Study population
We reviewed the CT images of 470 hips in 235 Chinese patients (113 men, 122 women; age range = 19–64 years) who underwent abdominal and pelvic CT scans for reasons unrelated to hip symptoms at our hospital between February and October 2017. The inclusion criteria were as follows: the whole pelvis and both hip joints were involved; no hip symptom and CT signs of OA; age ≥18 years; and no history of hip disease such as congenital hip dysplasia, slipped capital femoral epiphysis, hip fracture, surgery, and any arthropathy.
CT examination and image reconstruction
All CT scans were performed using a 16-, 64-, or 256-multidetector CT (MDCT) scanner (Brilliance 16, Brilliance 64, or Brilliance iCT, respectively; SIEMENS or GE or Philips Healthcare) and multiplanar reconstructions were generated with a bone algorithm. The following measurements were made on each hip joint: acetabular version angle (AV); anterior acetabular sector angle (AASA) and posterior acetabular sector angle (PASA); the lateral center edge angle (LCE); the alpha angle (AA); and femoral head-neck offset (FHNO). To avoid the effect of pelvic tilt on the measurement and improve the accuracy, it is necessary to correct pelvic tilt in the sagittal plane. The position of the pelvis was standardized using the anterior pelvic plane (Fig. 1) (12–14). AV, AASA, and PASA were all assessed in the axial scanning image after correction for pelvic tilt (13,15,16). The AV was measured in three different axial slices at intervals of 30°: AV1 in the 1 o’clock position (the superior margin of the femoral head); AV2 in the 2 o’clock position (the level between the other two slices); and AV3 in the 3 o’clock position (center of the femoral head) (Fig. 2a and 2b). The AASA and PASA were evaluated in the 3 o’clock position (Fig. 2c). LCE was measured on transparent 3-dimensional pelvis model (11,17) (Fig. 3). The AA and FHNO were measured in the oblique axial plane through the center of the femoral neck (11,18) (Fig. 4). A pincer lesion was defined as AV being negative in any slice (19) and/or LCE > 40° (20). A cam lesion was defined as an alpha angle > 55° (20) and/or a femoral head-neck offset < 8 mm (18).

The anterior pelvic plane was the reference plane involving the bilateral anterior superior iliac spines and the top of the pubis symphysis. The axial scanning line was perpendicular to the anterior pelvic plane. The angle between the scanning line and the horizontal line is the corrective angle of the pelvis.
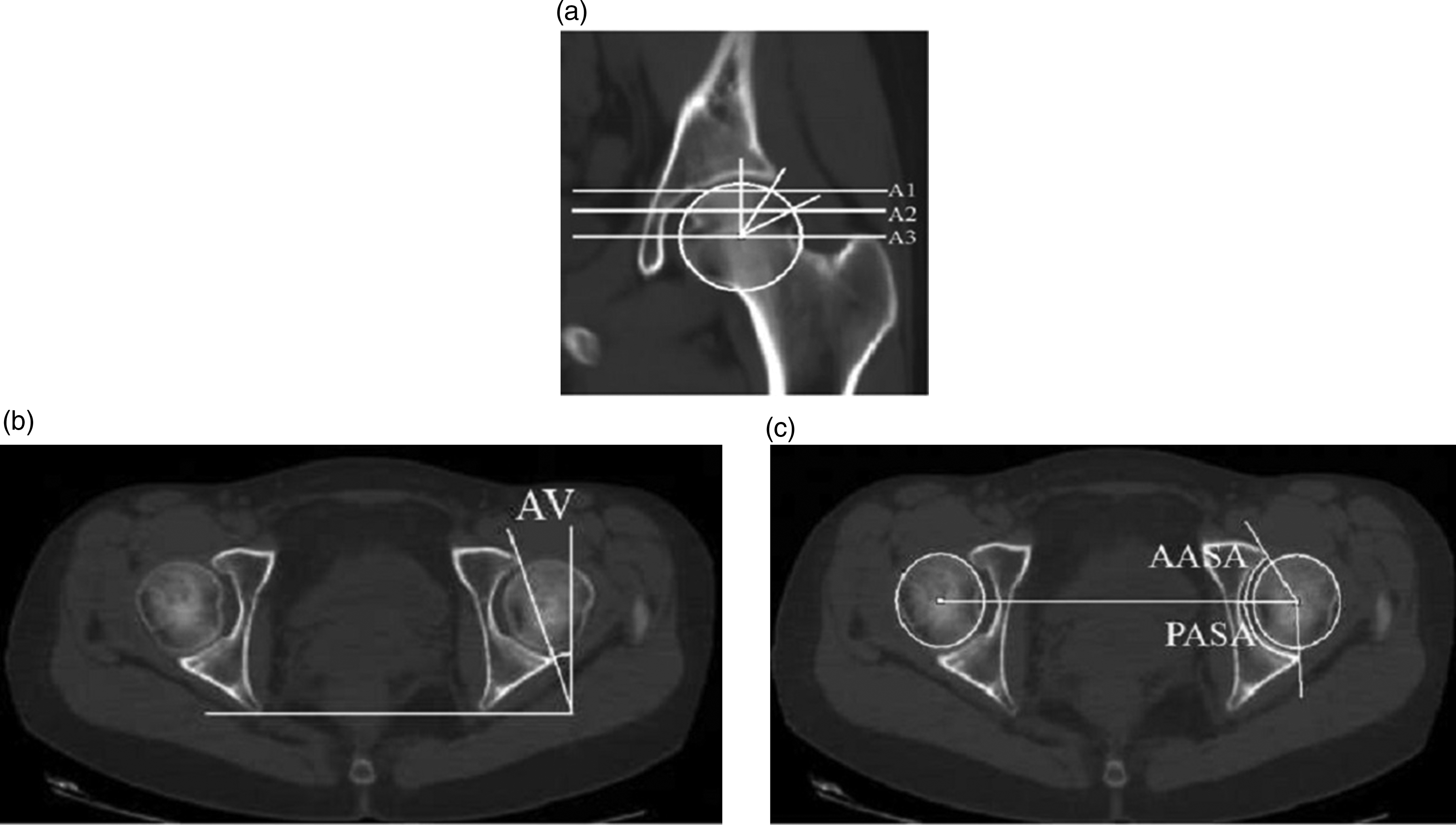
(a) Reference plane for measuring the acetabular version angle. Each line represents one of the three slices. Slices A1, A2, and A3 are axial slices in the 1 o’clock, 2 o’clock, and 3 o’clock positions. (b) The acetabular version angle measurement in axial slice of A3. It was measured as the angle between the line joining the anterior and posterior edges of the acetabulum and the line perpendicular to the line joining the posterior edges of both acetabula. (c) Measurements of the anterior acetabular sector angle (AASA) and the posterior acetabular sector angle (PASA). They were made by a line connecting the center of the bilateral femoral head and lines from the center of the femoral heads to the anterior and posterior margins of the acetabulum in the 3 o’clock position.

Lateral center edge angle measurement. The angle was made between the line joining the lateral edge of acetabulum and the center of the femoral head and the vertical line that is perpendicular to the horizontal line joining the ischial tuberosities.

(a) Reference plane for measuring alpha angle and femoral head-neck offset. (b) Alpha angle measurement. The angle was measured between the line crossing the center of the femoral neck and the line joining the center of the femoral head and the point where the radius femoral head exceeds the circle. (c) Femoral head-neck offset measurement. It was the distance between lines a and b in the oblique axial plane. Line a is parallel to the anterior cortex of the femoral head, while line b is parallel to the anterior aspect of the femoral neck cortex. Line a and b are both parallel to the line c crossing the center of the femoral neck.
Statistical analysis
All data were computed using SPSS software, version 20.0 (SPSS Inc., Chicago, IL, USA). The one-sample Kolmogorov–Smirnov test was used to test whether data samples were normally distributed. Differences between sexes and age groups were compared using Student’s t-test. One-way analysis of variance (ANOVA) with a Scheffé post hoc test was used to determine the significance of differences among three groups. Statistical differences were considered significant if the P value was <0.05. The reliability of the radiographic analysis was assessed by determining the inter- and intra-observer reproducibility in 30 randomly selected patients.
Results
In total, 470 hip joints of 235 patients (122 women, 113 men; age range = 19–64 years; mean age = 37.7 ± 10.5 years) were assessed for the parameters associated with FAI.
The value of each parameter in all patients
The mean AV was 9.7° ± 8.8° in the 1 o’clock position, 19.4° ± 7.4° in the 2 o’clock position, and 19.3° ± 5.1° in the 3 o’clock position. The mean AASA was 59.4° ± 6.6° and the mean PASA was 96.8° ± 7.5°. The mean LCE was 32.5° ± 5.1°. The mean AA was 44.8° ± 5.9° and the mean FHNO was 9.6 ± 1.2 mm. Table 1 showed the value of each parameter in all patients on gender. Significant differences in all parameters were seen between men and women. Women showed significantly more anteversion than men in all three positions (P < 0.05). Men had more anterior acetabular coverage than women in the 3 o’clock position, while women had significantly more posterior wall coverage. The LCE, AA, and FHNO were all larger in men than in women. The AV increased as the slice neared the femoral head except the AV3 decreased compared with the AV2 in women, but there was no significant difference between AV2 and AV3 in men and women (Fig. 5). This study did a statistical analysis of 95% reference intervals of each quantitative morphometric parameter (Table 2).
Descriptive values of each parameter on gender.
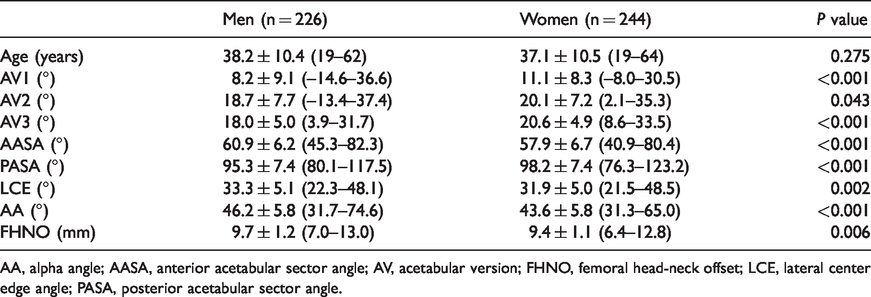
AA, alpha angle; AASA, anterior acetabular sector angle; AV, acetabular version; FHNO, femoral head-neck offset; LCE, lateral center edge angle; PASA, posterior acetabular sector angle.

The means of acetabular anteversion angles in men and women. The 95% confidence intervals are shown by the error bars.
95% reference intervals of each quantitative morphometric parameter.
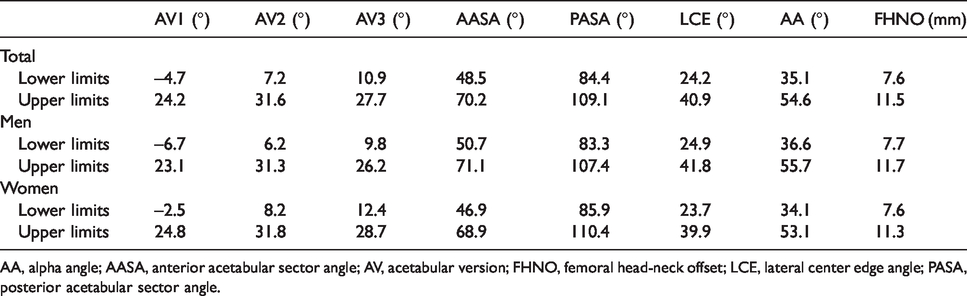
AA, alpha angle; AASA, anterior acetabular sector angle; AV, acetabular version; FHNO, femoral head-neck offset; LCE, lateral center edge angle; PASA, posterior acetabular sector angle.
Jihang et al. (21) thought FAI was frequently in young adults (age range = 18–40 years), so we divided men and women into two groups by age respectively (the “young” group as patients aged <40 years and the “elderly” group as those aged ≥40 years). Statistically significant differences in all parameters except AASA, LCE, and AA were seen between the age groups in men, and significant differences in AV1, AV2, AV3, and AASA were seen between the age groups in women. We found young men and elderly women showed more retroversion. We also divided the patients into two groups (the normal group as AV ≥0° and the abnormal group as AV < 0°). The normal group’s mean AASA and PASA were 60.2° ± 6.1°, 96.7° ± 7.0° in men and 57.3° ± 6.5°, 98.9° ± 7.2° in women, respectively. The abnormal group’s mean AASA and PASA was 64.3° ± 5.9°, 89.0° ± 5.7° in men and 63.2° ± 6.6°, 91.2° ± 6.3° in women, respectively. The abnormal group showed more anterior acetabular coverage and less posterior wall coverage in either men or women (P ≤ 0.002).
The prevalence of the radiographic features with FAI
Of the 470 patients included in our analysis, a negative acetabular anteversion angle (<0°) in any slice was found in 40/226 male hip joints and 24/244 female hip joints; an abnormal center-edge angle (>40°) was found in 21/226 male hip joints and 17/244 female hip joints. An abnormal alpha angle (>55°) was found in 21/226 male hip joints and 11/244 female hip joints, and an abnormal femur head-neck offset (<8 mm) was found in 19/226 male hip joints and 21/244 female hip joints. At least one of those abnormal parameters was found in 78/226 (34.5%) male hip joints and 61/244 (20.5%) female hip joints (Table 3).
Prevalence of radiologic features associated with femoroacetabular impingement.
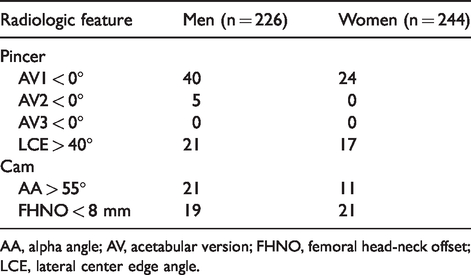
AA, alpha angle; AV, acetabular version; FHNO, femoral head-neck offset; LCE, lateral center edge angle.
Intra- and inter-observer variabilities
There was a good correlation between the two radiologists with regard to the measurements of all parameters (Table 4).
Reliability of all radiographic parameters.
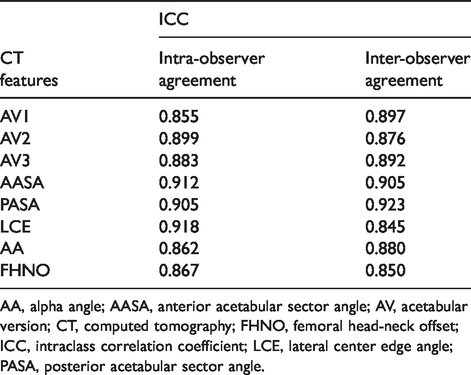
AA, alpha angle; AASA, anterior acetabular sector angle; AV, acetabular version; CT, computed tomography; FHNO, femoral head-neck offset; ICC, intraclass correlation coefficient; LCE, lateral center edge angle; PASA, posterior acetabular sector angle.
Discussion
We reviewed 470 CT scans of Chinese hips to perform a detailed investigation of the radiographic parameters associated with FAI and determine the prevalence of the cam and pincer types of FAI in Chinese asymptomatic hips. In contrast to conventional radiography and MRI, multislice CT has the advantage of the feasibility of multiplanar reformats that can show the bone contour and morphology clearly with thin-section reformats (21,22).
In this study, six quantitative parameters associated with FAI morphology were evaluated and we used reformatted CT axial images to calculate the AVs which estimated the degree of anterior wall overcoverage. The acetabular version measurement in two-dimensional (2D) CT by the femoral head clock-face positions was seldom used in previous studies. This measurement was given a simpler method to evaluate the value of the acetabular anteversion angle than three-dimensional (3D) CT scans that have been put into practice in daily work in our hospital. We found that men showed significantly more retroversion than women in all three positions, which was consistent with a previous report by Tannenbaum et al. (23). Of the three positions measured, 64 hips in the 1 o’clock and only five hips in the 2 o’clock positions showed acetabular retroversion (< 0°), which is because this location is involved with FAI pathology due to anterosuperior overcoverage of the femoral head (14,23,24). Besides, statistically significant differences in acetabular anteversion were seen between the age groups that young men and elderly women showed more retroversion in our study. A number of studies have described acetabular retroversion by crossover sign on conventional radiography which may be overestimated (25). In other studies, acetabular retroversion was diagnosed by the acetabular anteversion angle < 15° that was measured at a level where the acetabular cup was at its deepest (13,21). However, in our study, we estimated the AV measurements in three different clock-face positions by gender and age groups instead of one uniform threshold to determine acetabular retroversion and we found the significant differences of AVs in different groups. Therefore, the threshold value for an abnormal AV should be reconsidered based on gender, age, and the location where it is measured. We also divided the patients into the normal and abnormal groups; the abnormal group (AV < 0°) showed more anterior acetabular coverage and less posterior wall coverage in either men or women. That means AASA and PASA, which also evaluated the extent of acetabular overcoverage, were correlated with the AV that the AASA was positive correlated with the AV while the PASA was negative correlated with the AV. At present, the threshold values of abnormal AASA and PASA have not been made to evaluate the pincer deformity of FAI. LCE, which estimated coxa profunda, was another parameter that determined the pincer impingement. The LCE was larger in men than women, but the angle was relatively lower than previous reports (7,11,21,26).
We used AA and FHNO to determine the cam impingement; men showed lager AA and FHNO than women in our study population, which was consistent with previous studies (10,21,27). The alpha angle is frequently used to assess cam impingement caused by femoral head asphericity and diminished femoral head–neck offset, and we considered an alpha angle > 55° abnormal, but this cut-off has not yet been firmly established in the current literature. Several authors (7,8,17,26) evaluated cam deformity by measuring AA in both the oblique axial plane and the radial plane and similarly found that the AA in the radial position revealed more abnormalities than in the oblique axial plane. Measuring only the AA in the oblique axial plane in our study may overestimate the prevalence of the cam impingement. Sutter et al. (28) stated that the alpha angle did not help to differentiate accurately between volunteers and patients with FAI who have cam-type deformities, and suggested that an increase of the alpha angle threshold in the range of 55°–60° may reduce false-positive results. A study by Lepage-Saucier et al. (7) also suggested that the alpha angle was not an appropriate parameter to define cam-type morphotype.
This study provided 95% reference intervals for each parameter associated with FAI in a Chinese asymptomatic population. Some parameters were consistent with the normal range of parameters reported in previous studies, such as the LCE angle and the alpha angle. Most studies diagnosed hip dysplasia by estimating AASA and PASA values. Ito et al. (29) calculated the abnormal range of AASA and PASA by acetabular dysplasia and concluded that hip dysplasia was defined as AASA < 50° and/or PASA > 90°. The overall reference ranges of AASA and PASA in this study were approximately 48°–70° and 80°–109°, respectively. These data suggested that some patients in the selected population may also have hip dysplasia. Therefore, patients with hip dysplasia may have morphological changes in the hip under the influence of some factors and may also be secondary to FAI.
Our study demonstrated that 25% of female joints and 34.5% of male joints had at least one predisposing factor for FAI using measurement parameters by high-resolution reconstructed multislice CT images in Chinese asymptomatic patients; the prevalence of pincer lesion (19.1%) was larger than cam lesion (9.1%) in our study. However, the overall prevalence was lower than previously reported. For instance, Mineta et al. (13) found that 37.4% of all patients had pincer-type deformity and 45.3% had cam-type deformity, and 65.6% of all hips had at least one parameter that predisposes to FAI in asymptomatic Japanese patients. Chakraverty et al. (8) reported that 66% (66/100 hips) had at least one abnormal parameter (71.7% in men, 57.5% in women) associated with FAI in young asymptomatic patients in the UK. Another study (11) demonstrated that 31% of female joints (33% of female participants) and 48% of male joints (52% of male participants) had at least one factor for predisposing FAI in New Zealand. Teke et al. (17) found that 64.5% of the 400 joints had at least one abnormal morphological parameter associated with FAI in Turkey. At least one of the abnormal CT features was detected in 126/292 (43.2%) male hips and in 64/181 (35.4%) female hips in the Republic of Korea (21). A comparative study (30) found that the prevalence of radiographic signs associated with a risk of the development of FAI was significantly higher in white individuals than in Chinese individuals. Clearly, these findings were suggested that even asymptomatic patients had the potential risk of developing FAI. The prevalence of Chinese patients with FAI was relatively lower than that of other countries, possibly because of exercise mode, the setting posture, or the pelvis difference itself in different countries or because the diagnostic criteria using parameters of FAI in different articles was different. In these asymptomatic populations, there were more pincer-type abnormal parameters than cam-type, which may due to the smaller and relatively limited extent of acetabular and articular cartilage damage in pincer-type (31), so people may not feel joint pain during normal activities. While there was premature contact between the femur and the acetabular rim in cam-type, which wore the labrum and cartilage earlier, the pain symptoms appeared relatively early. The higher pincer incidence could also be related to coxa profunda morphology which has been considered an indicator of acetabular overcoverage (6). Many studies (3,4,6,32,33) have confirmed that acetabular overcoverage and femoral head asphericity contributed to the development of hip OA. Hence, early diagnosis and treatment were very important for clinicians to prevent the labral and cartilage lesions of the hip which finally resulted in the development of OA.
The study had several limitations. First, we investigated patient population by our radiology and hospital databases without hip symptoms and other hip diseases, but we verified their asymptomatic status without reference to physical examination such as an impingement test (34). Second, we mainly examined the acetabular version and only focused on abnormal morphology of the femoral head. We did not investigate other femoral characteristics which also play important roles in FAI, including the femoral anteversion (35) and the neck-shaft angle (36). Unfortunately, we could not obtain data for femoral version because the CT imaging did not include the femoral condyles that was used to calculate this angle. Third, we did not focus on the patients’ conditions such as body mass index, daily activity level, heavy work, and pelvic posture, which may be important in the development of FAI because FAI is a morphological and dynamic syndrome.
In conclusion, morphological features associated with FAI are also present in Chinese asymptomatic patients. Radiographic features play an important role in the diagnosis of FAI. The threshold value of abnormal parameters should be reconsidered based on gender, age, and other factors in order to improve the accuracy of the diagnosis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.