
Abstract
Background
Fluorodeoxyglucose positron emission tomography (FDG-PET)/computed tomography (CT) and diffusion-weighted magnetic resonance imaging (DWI or DW-MRI) are tools for the diagnosis of pancreatic cancer. However, comparison of their diagnostic performance remains unknown.
Purpose
To indirectly compare the diagnostic value of DWI and FDG-PET/CT in the detection of pancreatic cancer.
Material and Methods
A literature search of PubMed, Embase, and Cochrane Library electronic databases for articles published through May 2018 yielded 875 articles. For the meta-analysis, we included 26 studies evaluating the efficacy of DWI and FDG-PET/CT for determining pancreatic cancer with a total of 1377 patients. QUADAS (Quality Assessment of Diagnostic Accuracy Studies) was used to assess the study quality. Sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and the area under the receiver operating characteristic curves (AUC) with their 95% confidence intervals were calculated for each individual study.
Results
There were no significant differences between DWI and FDG-PET/CT for sensitivity, specificity, PLR, NLR, or DOR, while DWI AUC was higher than that of FDG-PET/CT for the detection of pancreatic cancer.
Conclusion
The diagnostic value of both DWI and FDG-PET/CT were comparable and, hence, both techniques seem to be equally useful tools for the diagnosis of pancreatic cancer.
Introduction
Pancreatic cancer is the fourth leading cause of cancer mortality in Western countries and accounts for 12.5 per 100,000 population annually, with an annual death rate of 10.9 per 100,000 (1,2). Nearly 15% of patients are in stage I or II (resectable), 35% are in stage III (locally advanced), and 50% are in stage IV (metastatic) pancreatic cancer at the time of diagnosis (3). The survival rate of patients with pancreatic cancer is poor, with <5% surviving to one year (4). One reason for the poor survival rate might be that pancreatic cancer is difficult to detect in its early stages, and most cancers found in patients are already at a metastatic stage at the time of diagnosis (5). The symptoms that present in a clinical setting include weight loss, jaundice, malabsorption, pain, dyspepsia, and nausea, but there are also many patients without clinical symptoms or early warning signs; therefore, a more effective diagnostic tool must be explored for early detection of this cancer.
The diagnostic tools for pancreatic cancer are computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic or laparoscopic ultrasonography; however, the best of these procedures remains controversial (6). Fluorodeoxyglucose positron emission tomography (FDG-PET) has shown good diagnostic results for differentiating malignant from benign lesions but lacks accurate anatomical data when used alone (7–9); therefore, a combination of FDG-PET and CT are widely used and could provide anatomical and spatial information with functional images (10). In addition, evidence has indicated that diffusion-weighted MRI (DWI) is promising for detecting pancreatic cancer based on pancreatic imaging (11). Although DWI and FDG-PET/CT are used for the early assessment of pancreatic cancer, the diagnostic results of these two methods needed to be demonstrated; therefore, we conducted this systematic review and meta-analysis to quantitatively evaluate the diagnostic performance of DWI and FDG-PET/CT for the early detection of pancreatic cancer. In addition, an indirect comparison between DWI and FDG-PET/CT for their diagnostic performance was calculated.
Material and Methods
Data sources, search strategy, and selection criteria
This systematic review and meta-analysis was performed in accordance with PRISMA 2009 guidelines (12). Studies published in English that investigated the diagnostic performance of DWI or FDG-PET/CT for the early detection of pancreatic cancer was eligible for inclusion in this quantitative analysis without restricted publication status. PubMed, Embase, and Cochrane Library electronic databases were searched for articles published through May 2018. Search terms used in our study were [“PET/CT” OR “PET-CT” OR “positron emission tomography/computed tomography” OR “positron emission tomography-computed tomography” OR (“weighted imaging” AND “diffusion”)] AND (“pancreas” OR “pancreatic”) AND (“neoplasm” OR “tumor” OR “cancer” OR “carcinoma”) AND (“sensitivity” OR “specificity” OR “diagnosis” OR “detection” OR “accuracy”). Manual searches of the reference lists from the eligible articles and relevant reviews were also conducted to select any additional potential articles.
Two independent reviewers were involved in the literature search and study selection process; a standard flow chart was followed. A group discussion was conducted to resolve any inconsistencies in reviewer results until a consensus was reached. The inclusion criteria of our meta-analysis were as follows: (i) all patients who were at risk for pancreatic cancer; (ii) patients received DWI or FDG-PET/CT to diagnose pancreatic cancer; (iii) a biopsy was performed; (iv) studies had to have reported both true and false positives, true and false negatives, or results that could be transformed into these data; and (v) an irrespective prospective or retrospective design. Duplication or irrelevant studies were excluded.
Data collection and quality assessment
The data collected in this meta-analysis were first author’s surname, year of publication, study design, country, sample size, mean age, percent male, mean size of lesion, diagnostic methods, gold standard, true and false positives, and true and false negatives. For studies that reported the same population more than once, the most recent was selected for final analysis. The study quality was assessed using QUADAS (Quality Assessment of Diagnostic Accuracy Studies), a comprehensive and partially validated tool for evaluating the quality of diagnostic accuracy studies in meta-analysis (13). QUADAS was based on 14 items with each indicating yes, no, or unclear. Two independent reviewers collected the data and conducted the quality assessment; any disagreement was adjudicated by the corresponding author in reference to the original articles.
Statistical analyses
The true-positive, false-positive, false-negative, and true-negative results were used to calculate the sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and the area under the receiver operating characteristic (ROC) curves (AUC) with their 95% confidence intervals (CIs) for each individual study. The bivariate generalized linear mixed model and the random-effects model were used to calculate the pooled summary sensitivity, specificity, PLR, NLR, and DOR (14). In addition, the summary AUC was calculated using a hierarchical regression (15). Heterogeneity across the included studies was calculated using I-square and Q statistics; I-square ≥50.0% or P value <0.10 were regarded as significant heterogeneity (16,17). Subgroup analyses for DOR of DWI and FDG-PET/CT were conducted based on study design, country, sample size, mean age, percent male, and mean size of the lesion. The ratio of DWI to FDG-PET/CT or subgroups was also calculated (18). Publication bias for DWI and FDG-PET/CT was calculated using funnel plots and Deeks’ asymmetry tests (19). P values were two-sided and P values <0.05 were considered statistically significant for pooled diagnostic parameters. The meta-analysis was performed using STATA v. 10.0 (Stata Corporation, College Station, TX, USA).
Results
Literature search
The initial search of electronic databases produced 875 articles, comprising 546 in PubMed, 278 in Embase, and 51 in The Cochrane Library. In total 836 of these studies were excluded because of duplications and irrelevant topics. Thirty-nine studies were further evaluated; 13 of these were excluded because of insufficient data (n = 7), another diagnostic tool was used on the patients (n = 5), or the study was not published in English (n = 1). Ultimately, 26 studies were selected for the final quantitative analysis (20–45). A manual search of the references of the 26 studies did not yield any new or eligible studies. The results of the study selection process are presented in Fig. 1; the general characteristics of the included studies and patients are shown in Table 1.

Flow diagram representing the study selection process.
Baseline characteristics of the included studies and patients.

CT, computed tomography; DWI, diffusion-weighted magnetic resonance imaging; NA, not available; PC, pancreatic cancer; PET, positron emission tomography.
Study characteristics
Twenty-six studies comprising 1377 participants were included in the final analysis, of which 11 were prospective and the remaining 15 retrospective studies. Fourteen studies investigated the diagnostic performance of DWI; the remaining 12 studies evaluated the diagnostic performance of FDG-PET/CT. The included studies were published between 2004 and 2017 and 12–126 patients were included in each study. Twelve studies were conducted in Eastern countries and the remaining 14 studies were conducted in Western countries. The age of the included patients was in the range of 47.0–69.0 years, the ratio of males was in the range of 44.0%–81.3%, and the size of lesions was in the range of 12.0–51.0 mm. Study quality was assessed using QUADAS, and the results are shown in Supplemental Table 1.
DWI
Fourteen studies reported the diagnostic performance of DWI for detecting pancreatic cancer. The summaries for DWI sensitivity and specificity are shown in Fig. 2 at 0.93 (95% CI - 0.84–0.97) and 0.86 (95% CI = 0.75–0.92), respectively. In addition, the pooled PLR and NLR are provided in Fig. 3, with an effect of 6.53 (95% CI = 3.53–12.09) and 0.08 (95% CI = 0.03–0.20), respectively. DOR of DWI for diagnosing pancreatic cancer was 44.07 (95% CI = 15.92–122.00; Fig. 4). Finally, the summary area under the DWI ROC for detecting pancreatic cancer was 0.95 (95% CI = 0.93–0.97; Fig. S1).

Summary sensitivity and specificity for diffusion-weighted imaging.

Summary positive likelihood ratio and negative likelihood ratio for diffusion-weighted imaging.

Summary diagnostic odds ratio for diffusion-weighted imaging.
FDG-PET/CT
Twelve studies reported the diagnostic performance of FDG-PET/CT for detecting pancreatic cancer. The summaries for the sensitivity and specificity of FDG-PET/CT are shown in Fig. S2, with parameters of 0.88 (95% CI = 0.83–0.91) and 0.78 (95% CI = 0.66–0.87), respectively. In addition, pooled PLR and NLR are provided in Fig. S3, with effect estimates of 4.07 (95% CI = 2.53–6.53), and 0.16 (95% CI = 0.11–0.21), respectively. DOR of FDG-PET/CT for diagnosing pancreatic cancer was 20.65 (95% CI = 12.39–34.41; Fig. S4). Finally, the summary area under the FDG-PET/CT ROC for detecting pancreatic cancer was 0.91 (0.91; 95% CI = 0.88–0.93; Fig. S5).
Indirect comparison of diagnostic performance between DWI and FDG-PET/CT
The ratio of the DWI to FDG-PET/CT diagnostic parameters was calculated. Overall, there were no significant differences between DWI and FDG-PET/CT for sensitivity (DWI to FDG-PET/CT: 1.06; 95% CI = 0.97–1.15; P = 0.205), specificity (DWI to FDG-PET/CT = 1.10; 95% CI = 0.93–1.31; P = 0.265), PLR (DWI to FDG-PET/CT: 1.60; 95% CI = 0.74–3.49; P = 0.233), NLR (ratio between DWI and FDG-PET/CT: 0.50; 95% CI = 0.18–1.36; P = 0.175), and DOR (DWI to FDG-PET/CT: 2.13; 95% CI = 0.68–6.67; P = 0.192). Moreover, when diagnosing pancreatic cancer, DWI was associated with higher AUC than FDG-PET/CT (DWI to FDG-PET/CT: 1.04; 95% CI = 1.01–1.08; P = 0.015).
Subgroup analyses
Subgroup analyses for DOR of DWI and FDG-PET/CT are provided in Table 2. DOR of DWI was higher than that of FDG-PET/CT in Eastern countries (DWI to FDG-PET/CT: 4.83; 95% CI = 1.00–23.35). Furthermore, DOR was lower when the mean size of the lesion was ≥30 mm in patients who received DWI compared to that when the mean size of the lesion was <30 mm (DWI to FDG-PET/CT: 0.09; 95% CI = 0.01–0.91). No other significant differences between DWI and FDG-PET/CT or predefined subgroups were observed.
Subgroup analysis for diagnostic odds ratios.
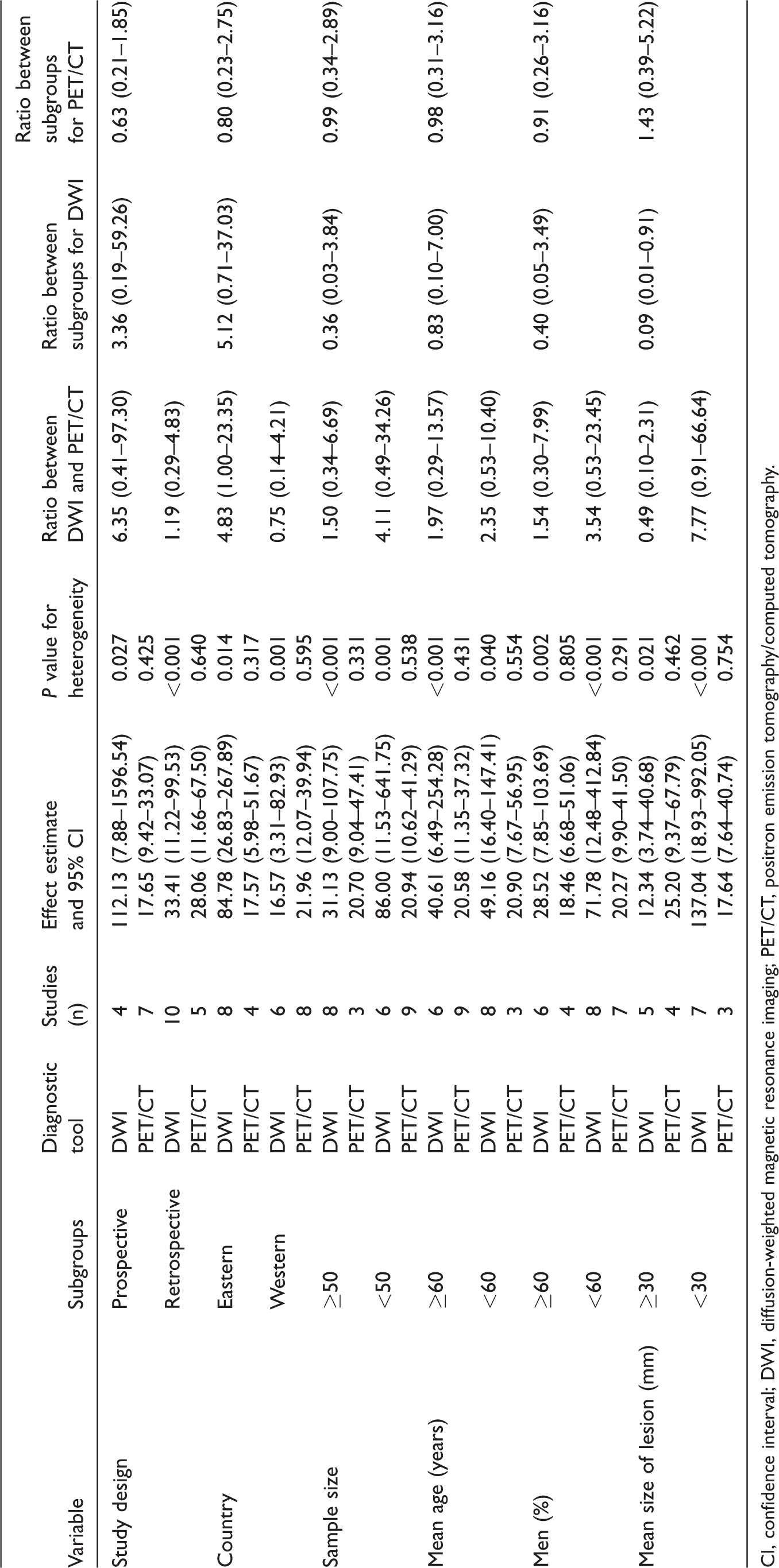
CI, confidence interval; DWI, diffusion-weighted magnetic resonance imaging; PET/CT, positron emission tomography/computed tomography.
Publication bias
Review of the funnel plots could not rule out the potential for publication bias for DWI and FDG-PET/CT (Fig. S6). The Deeks’ asymmetry tests showed no significant publication biases for DWI (P = 0.74) and FDG-PET/CT (P = 0.80).
Discussion
Although many studies have been published on the diagnostic performance of DWI and FDG-PET/CT for detecting pancreatic cancer, the range of diagnostic parameters vary widely; therefore, we conducted this meta-analysis to decide the diagnostic value of both DWI and FDG-PET/CT for the early detection of pancreatic cancer on a large scale. This comprehensive quantitative meta-analysis comprised 1377 patients from 26 studies with a broad range of characteristics. The results from this meta-analysis indicate that both DWI and FDG-PET/CT perform moderately in detecting pancreatic cancer. Furthermore, the AUC in DWI is significantly higher than that in FDG-PET/CT. Finally, the DOR in DWI is significantly higher than that in FDG-PET/CT in the study conducted in Eastern countries.
A previous meta-analysis was conducted based on 52 studies to demonstrate the performance of MRI, CT, PET, PET/CT, endoscopic ultrasound (EUS), and transabdominal ultrasound in diagnosing pancreatic ductal adenocarcinoma (46). This study has pointed out that the diagnostic value of MRI was associated with higher sensitivity, specificity, and diagnostic accuracy than CT and PET, but the diagnostic value of FDG-PET/CT was not illustrated. Another important meta-analysis was conducted based on 16 studies to illustrate the performance of DWI and FDG-PET/CT in diagnosing pancreatic cancer (47). This study concluded that PET/CT had higher sensitivity, whereas DWI had a higher specificity for detecting pancreatic malignancy. In addition, they have pointed out that enhanced PET/CT had a higher diagnostic value than unenhanced PET/CT; however, the statistical results of these comparisons were not calculated. Therefore, we conducted a systematic review and meta-analysis of the published studies to evaluate the performance of DWI and FDG-PET/CT for diagnosing pancreatic cancer.
Most of the included studies reported that DWI had moderate or good performance for diagnosing pancreatic cancer; however, three of the studies suggested no diagnostic significance for DWI. The study conducted by Caramella et al. (23) indicated that DWI had high sensitivity (0.94), but lower specificity (0.17). Sandrasegaran et al. (31) suggested that the apparent diffusion coefficient from DWI was a useful index for deciding the malignant potential of intraductal papillary mucinous neoplasm, while DWI was not a useful tool in differentiating malignant from benign lesions. Robertis et al. (36) indicated that a DWI having a lower sensitivity and a higher specificity has clinical value for detecting liver metastases but was associated with lower performance for diagnosing pancreatic cancer. This lower performance was the result of different types of pancreatic cancer and the mean size of the lesions; the diagnostic value of DWI was suitable for patients with specific characteristics.
Most studies included in this meta-analysis showed moderate performance of FDG-PET/CT for diagnosing pancreatic cancer. One study indicated that diagnostic performance of FDG-PET/MR was similar to that of PET/CT for assessing the resectability and staging of pancreatic tumors preoperatively (41); however, in this study based on a small patient cohort, PET/MRI showed higher sensitivity than PET/CT when depicting regional lymph node metastasis. Furthermore, the baseline characteristics of the patients included in the study and the expertise of the radiologist could have affected the diagnostic performance of FDG-PET/CT.
Subgroup analyses indicated that DWI had higher DOR than FDG-PET/CT when the study was conducted in Eastern countries, which might be because of the varying prevalence of pancreatic cancer, the cancer type, and variations in the mean size of the lesions in different countries. In addition, the diagnostic performance of DWI if the mean size of the lesions was <30 mm was higher than that with lesions ≥30 mm; however, a broad 95% CI of the diagnostic parameters caused the variable ratios between DWI and FDG-PET/CT or subgroups. Therefore, we provided a relative result and a synthetic and comprehensive review.
DWI is routinely used in clinical imaging as an adjunct MRI technique for tumor detection in different organs, staging, monitoring, and determining treatment effectiveness. The DWI technique has been evolving over the past three decades leading to its widespread use in medical sciences; diffusion-weighted whole-body imaging with background body signal suppression and dynamic contrast-enhanced MRI have been employed for the diagnosis of various tumors, while diffusion tensor imaging has been used for assessing organs with highly organized fiber structure (48,49). Nevertheless, our aim was to compare the diagnostic value of DWI (irrespective of the technology-specificity) and FDG-PET/CT on a very broad perspective. While it can be taken as a shortcoming that the present study discounts very specific technological advancements in DWI in the studies considered, the strength of the present study lies in the fact that we have been able to rigorously evaluate several studies spanning >10 years that have used the two techniques specifically for pancreatic cancer detection.
In our study, 13 out of the 26 studies included did not report any b-values. Of the others, some used a combination of b-values with a maximum of 1000 s/mm2 and many used a b-value of 800 s/mm2 (30,31,33,41,42,44,45). The ranges and thresholds of apparent diffusion coefficients (ADC) values become difficult to interpret because of variability in b-values across studies. We were unable to perform a meta-analysis in the subgroup of studies since 50% of the studies did not report any b-values. While a high intensity signal with poor anatomical delineation was associated with a high b-value of 1100 s/mm2, benign and malignant pancreatic tumors could be distinguished with a b-value of 700 s/mm2 associated with ADCs; b-values of 50, 350, 400, 450, and 1100 s/mm2 were associated with imprecise ADC values and could not differentiate between benign and malignant tumors (50). A b-value of 800 s/mm2 can help to differentiate between pancreatic cancer, mass-forming focal pancreatitis, and a normal pancreas (51). Due to the lack of standardization, the choice of b-value in clinical practice is controversial (52). While a higher b-value of 1000 s/mm2 has been reported for the detection of pancreatic adenocarcinoma with a high specificity and sensitivity (21), using b-values in the range of 0–800 s/mm2 increases the sensitivity and specificity for differentiating pancreas carcinoma from healthy pancreatic tissue (30). In clinical practice for pancreatic tumor detection, the choice of b-value should be made with the aim of minimizing motion artifacts and improving the signal-to-noise ratio (53).
The strengths of this meta-analysis are as follows: (i) a large sample size with a broad range of patient characteristics could show that the study might represent a greater range of populations; (ii) stratified results for DOR in DWI and FDG-PET/CT were conducted to evaluate the diagnostic performance in specific subsets; and (iii) indirect comparisons of the diagnostic parameters between DWI and FDG-PET/CT were calculated, which could provide a relative best diagnostic tool for detecting pancreatic cancer.
The limitations of this meta-analysis should be highlighted. First, both prospective and retrospective studies were included, and selection and recall bias in retrospective case-control studies might affect the accuracy of the diagnostic performance. Second, the current study was based on published studies and publication bias is an inevitable problem. Third, the diagnostic performance of DWI and FDG-PET/CT on a specific type of pancreatic cancer was not illustrated because of the various types of pancreatic cancer. Finally, the baseline characteristics of patients were based on pooled data; individual data were not available. This restricted us to conduct stratified analyses based on patient characteristics.
In conclusion, DWI and FDG-PET/CT showed a medium performance for diagnosing pancreatic cancer, and no significant differences between DWI and FDG-PET/CT in sensitivity, specificity, PLR, NLR, and DOR were observed. Furthermore, the AUC in DWI was higher than that in FDG-PET/CT in detecting pancreatic cancer. Future large-scale prospective studies should be conducted to directly compare the performance of DWI with FDG-PET/CT in the detection of pancreatic cancer.
Supplemental Material
ACR907246 Supplemental material - Supplemental material for Diffusion-weighted MRI versus FDG-PET/CT for diagnosing pancreatic cancer: an indirect comparison meta-analysis
Supplemental material, ACR907246 Supplemental material for Diffusion-weighted MRI versus FDG-PET/CT for diagnosing pancreatic cancer: an indirect comparison meta-analysis by Renye Que, Yirong Chen, Zhihui Tao, Bingjing Ge, Miaohua Li, Zhiquan Fu and Yong Li in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support with respect to the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (No. 81573775 and 81873157), Shanghai Outstanding Academic Leader of Health System (No. XBR2013120), the Natural Science Foundation of Shanghai (No. 16ZR1433800), the budgetary Foundation of Shanghai University of Traditional Chinese Medicine (No. 18LK074), and Shanghai Sailing Program (No. 19YF1445200). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.